EBV+ and MSI Gastric Cancers Harbor High PD-L1/PD-1 Expression and High CD8+ Intratumoral Lymphocytes

 ,
, 
Abstract
:1. Introduction
2. Results
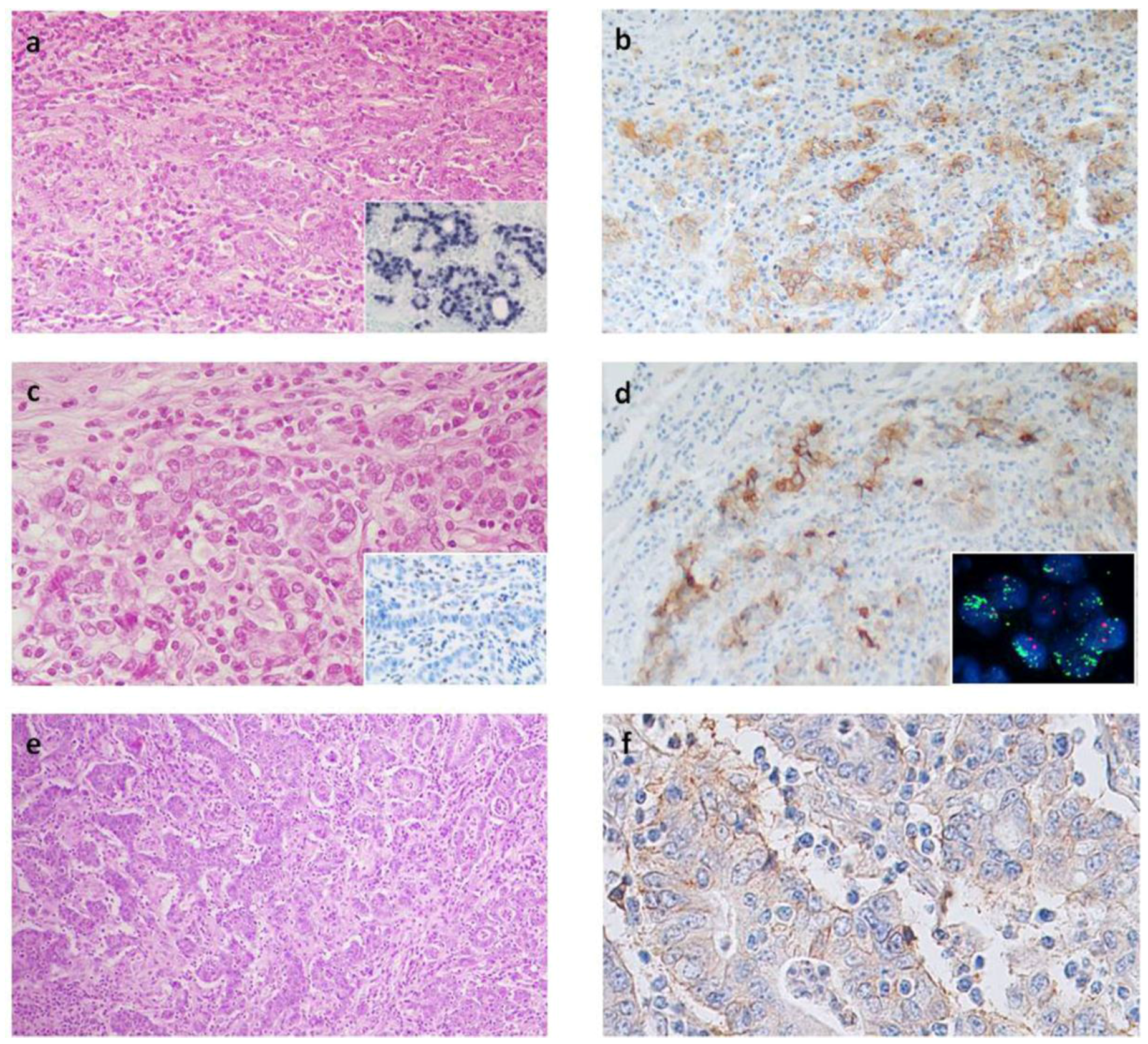
2.1. PD-L1 Expression
2.2. CD8+ Lymphocytes
2.3. PD-1+ Intraepithelial Lymphocytes
2.4. FISH Results
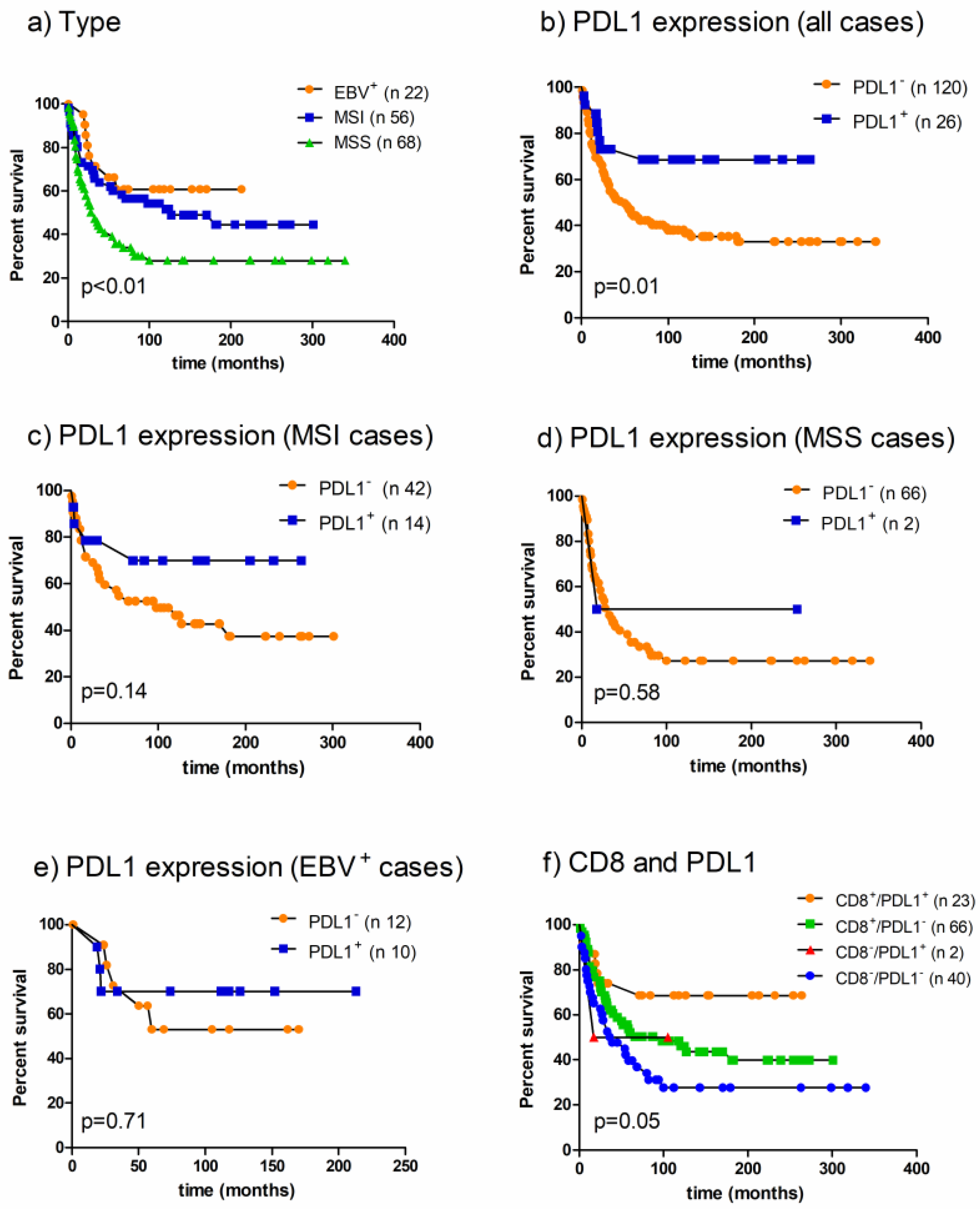
2.5. Survival Analysis
3. Discussion
4. Materials and Methods
4.1. Patients and Samples
4.2. Immunohistochemical Study
4.3. Fluorescence In Situ Hybridization (FISH) Analysis
4.4. Statistical Analysis
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| EBV | Epstein Barr Virus |
| MSI | Microsatellite instability |
| MSS | Microsatellite stable |
| TILs | tumor Infiltrating Lymphocytes |
References
- The Cancer Genome Atlas Research Network. Comprehensive molecular characterization of gastric adenocarcinoma. Nature 2014, 513, 202–209. [Google Scholar] [Green Version]
- Cristescu, R.; Lee, J.; Nebozhyn, M.; Kim, K.-M.; Ting, J.C.; Wong, S.S.; Liu, J.; Yue, Y.G.; Wang, J.; Yu, K.; et al. Molecular analysis of gastric cancer identifies subtypes associated with distinct clinical outcomes. Nat. Med. 2015, 21, 449–456. [Google Scholar] [CrossRef] [PubMed]
- Merelli, B.; Massi, D.; Cattaneo, L.; Mandalà, M. Targeting the PD1/PD-L1 axis in melanoma: Biological rationale, clinical challenges and opportunities. Crit. Rev. Oncol. Hematol. 2014, 89, 140–165. [Google Scholar] [CrossRef] [PubMed]
- Mandai, M.; Hamanishi, J.; Abiko, K.; Matsumura, N.; Baba, T.; Konishi, I. Dual faces of IFNγ in cancer progression: A role of PD-L1 induction in the determination of pro- and antitumor immunity. Clin. Cancer Res. 2016, 22, 2329–2334. [Google Scholar] [CrossRef] [PubMed]
- Böger, C.; Behrens, H.-M.; Mathiak, M.; Krüger, S.; Kalthoff, H.; Röcken, C. PD-L1 is an independent prognostic predictor in gastric cancer of Western patients. Oncotarget 2016, 7, 24269–24283. [Google Scholar] [CrossRef] [PubMed]
- Ock, C.-Y.; Keam, B.; Kim, S.; Lee, J.-S.; Kim, M.; Kim, T.M.; Jeon, Y.K.; Kim, D.-W.; Chung, D.H.; Heo, D.S. Pan-cancer immunogenomic perspective on the tumor microenvironment based on PD-L1 and CD8 T-cell infiltration. Clin. Cancer Res. 2016, 22, 2261–2270. [Google Scholar] [CrossRef] [PubMed]
- Kawazoe, A.; Kuwata, T.; Kuboki, Y.; Shitara, K.; Nagatsuma, A.K.; Aizawa, M.; Yoshino, T.; Doi, T.; Ohtsu, A.; Ochiai, A. Clinopathological features of programmed death ligand 1 expression with tumor-infiltrating lymphocyte, mismatch repair, and Epstein-Barr virus status in a large cohort of gastric cancer patients. Gastric Cancer 2017, 20, 407–415. [Google Scholar] [CrossRef] [PubMed]
- Derks, S.; Liao, X.; Chiaravalli, A.M.; Xu, X.; Camargo, M.C.; Solcia, E.; Sessa, F.; Fleitas, T.; Freeman, G.J.; Rodig, S.J.; et al. Abundant PD-L1 expression in Epstein-Barr virus-infected gastric cancers. Oncotarget 2016, 7, 32925–32932. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Lai, Y.; Sun, L.; Zhang, X.; Liu, R.; Feng, G.; Zhou, L.; Jia, L.; Huang, X.; Kang, Q.; et al. PD-L1 expression is associated with massive lymphocyte infiltration and histology in gastric cancer. Hum. Pathol. 2016, 55, 182–189. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Qiu, M.; Jin, Y.; Ji, J.; Li, B.; Wang, X.; Yan, S.; Xu, R.; Yang, D. Programmed cell death ligand 1 (PD-L1) expression on gastric cancer and its relationship with clinicopathologic factors. Int. J. Clin. Exp. Pathol. 2015, 8, 11084–11091. [Google Scholar] [PubMed]
- Chang, H.; Jung, W.Y.; Kang, Y.; Lee, H.; Kim, A.; Kim, H.K.; Shin, B.K.; Kim, B.H. Programmed death-ligand 1 expression in gastric adenocarcinoma is a poor prognostic factor in a high CD8+ tumor infiltrating lymphocytes group. Oncotarget 2016, 7, 80426–80434. [Google Scholar] [CrossRef] [PubMed]
- Eto, S.; Yoshikawa, K.; Nishi, M.; Higashijima, J.; Tokunaga, T.; Nakao, T.; Kashihara, H.; Takasu, C.; Iwata, T.; Shimada, M. Programmed cell death protein 1 expression is an independent prognostic factor in gastric cancer after curative resection. Gastric Cancer 2016, 19, 466–471. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Dong, Y.; Liu, H.; Wang, Y.; Zhao, S.; Xuan, Q.; Wang, Y.; Zhang, Q. The clinicopathological and prognostic significance of PD-L1 expression in gastric cancer: A meta-analysis of 10 studies with 1901 patients. Sci. Rep. 2016, 6, 37933. [Google Scholar] [CrossRef] [PubMed]
- Chiaravalli, A.M.; Klersy, C.; Vanoli, A.; Ferretti, A.; Capella, C.; Solcia, E. Histotype-based prognostic classification of gastric cancer. World J. Gastroenterol. 2012, 18, 896–904. [Google Scholar] [CrossRef] [PubMed]
- Chiaravalli, A.M.; Feltri, M.; Bertolini, V.; Bagnoli, E.; Furlan, D.; Cerutti, R.; Novario, R.; Capella, C. Intratumour T cells, their activation status and survival in gastric carcinomas characterised for micro satellite instability and Epstein-Barr virus infection. Virchows Arch. 2006, 448, 334–353. [Google Scholar] [CrossRef] [PubMed]
- Park, J.J.; Omiya, R.; Matsumura, Y.; Sakoda, Y.; Kuramasu, A.; Augustine, M.M.; Yao, S.; Tsushima, F.; Narazaki, H.; Anand, S.; et al. B7-H1/CD80 interaction is required for the induction and maintenance of peripheral T-cell tolerance. Blood 2010, 116, 1291–1298. [Google Scholar] [CrossRef] [PubMed]
- Butte, M.J.; Keir, M.E.; Phamduy, T.B.; Sharpe, A.H.; Freeman, G.J. Programmed death-1 ligand 1 interacts specifically with the B7-1 costimulatory molecule to inhibit T cell responses. Immunity 2007, 27, 111–122. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.; Zhu, Y.; Jiang, J.; Zhao, J.; Zhang, X.G.; Xu, N. Immunohistochemical localization of programmed death-1 ligand-1 (PD-L1) in gastric carcinoma and its clinical significance. Acta Histochem. 2006, 108, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Ma, C.; Patel, K.; Singhi, A.D.; Ren, B.; Zhu, B.; Shaikh, F.; Sun, W. Programmed Death-Ligand 1 Expression Is Common in Gastric Cancer Associated With Epstein-Barr Virus or Microsatellite Instability. Am. J. Surg. Pathol. 2016, 40, 1496–1506. [Google Scholar] [CrossRef] [PubMed]
- Thompson, E.D.; Zahurak, M.; Murphy, A.; Cornish, T.; Cuka, N.; Abdelfatah, E.; Yang, S.; Duncan, M.; Ahuja, N.; Taube, J.M.; et al. Patterns of PD-L1 expression and CD8 T cell infiltration in gastric adenocarcinomas and associated immune stroma. Gut 2017, 66, 794–801. [Google Scholar] [CrossRef] [PubMed]
- Mimura, K.; The, J.L.; Okayama, H.; Shiraishi, K.; Kua, L.F.; Koh, V.; Smoot, D.T.; Ashktorab, H.; Oike, T.; Suzuki, Y.; et al. PD-L1 expression is mainly regulated by interferon gamma associated with JAK-STAT pathway in gastric cancer. Cancer Sci. 2018, 109, 43–53. [Google Scholar] [CrossRef] [PubMed]
- Clavé, S.; Pijuan, L.; Casadevall, D.; Taus, Á.; Gimeno, J.; Hernández-Llodrà, S.; Rodríguez-Rivera, M.; Lorenzo, M.; Menéndez, S.; Albanell, J.; et al. CD274 (PDL1) and JAK2 genomic amplifications in pulmonary squamous-cell and adenocarcinoma patients. Histopathology 2018, 72, 259–269. [Google Scholar] [CrossRef] [PubMed]
- Lauren, P. The two histological main type of gastric carcinoma: Diffuse and so-called intestinal-type carcinoma. Acta Pathol. Microbiol. Scand. 1965, 64, 31–49. [Google Scholar] [CrossRef] [PubMed]
- Sobin, L.H.; Gospodarowicz, M.; Wittekind, C. TNM Classification of Malignant Tumours, 7th ed.; Wiley-Blackwell Eds.: Hoboken, NJ, USA, 2009. [Google Scholar]
- Hastings, R.J.; Bown, N.; Tibiletti, M.G.; Debiec-Rychter, M.; Vanni, R.; Espinet, B.; van Roy, N.; Roberts, P.; van den Berg-de-Ruiter, E.; Bernheim, A.; et al. Tumour Best Practice meeting; Eurogentest. Guidelines for cytogenetic investigations in tumours. Eur. J. Hum. Genet. 2016, 24, 6–13. [Google Scholar] [CrossRef] [PubMed]
- Simons, A.; Shaffer, L.G.; Hastings, R.J. Cytogenetic Nomenclature: Changes in the ISCN 2013 Compared to the 2009 Edition. Cytogenet. Genome Res. 2013, 141, 1–6. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Feature | Total Cases | EBV+ Cases | MSI Cases | MSS/EBV− Cases | ||||
|---|---|---|---|---|---|---|---|---|
| Total | PD-L1+ | TOT | PD-L1+ | TOT | PD-L1+ | TOT | PD-L1+ | |
| Number of cases | 169 | 31 (18) | 33 | 15 (46) *** | 59 | 14 (24) *** | 77 | 2 (3) *** |
| Male | 103 (61) | 18 (58) | 24 (73) | 11 (73) | 26 (44) | 5 (36) | 53 (69) | 2 (100) |
| Female | 66 (39) | 13 (42) | 9 (27) | 4 (27) | 33 (56) | 9 (64) | 24 (31) | 0 |
| Mean age years (range) | 67 (36–90) | 68 (51–84) | 66 (36–86) | 66 (51–86) | 71 (49–90) | 72 (51–84) | 63 (38–84) | 61 (52–70) |
| ≥67 years | 91 (54) | 19 (61) **** | 17 (52) | 9 (60) | 40 (68) | 9 (64) | 34 (44) | 1 (50) |
| <67 years | 78 (46) | 12 (39) **** | 16 (49) | 6 (40) | 19 (32) | 5 (36) | 43 (56) | 1 (50) |
| Tumor location | ||||||||
| Cardias | 9 (5) | 3 (10) | 4(12) | 3 (20) | 1 (2) | 0 | 4 (5) | 0 |
| Body/fundus | 38 (22) | 8 (26) | 14 (43) | 6 (40) | 8 (13) | 2 (14) | 16 (21) | 0 |
| Antrum | 105 (62) | 16 (51) | 6 (18) | 2 (13) | 50 (85) | 12 (86) | 49 (64) | 2 (100) |
| Stump | 11 (7) | 3 (10) | 8 (24) | 3 (20) | 0 | 0 | 3 (4) | 0 |
| Others | 6 (4) | 1 (3) | 1 (3) | 1 (7) | 0 | 0 | 5 (6) | 0 |
| Mean diameter mm (range) | 52 (0–190) | 60 (0–130) | 52 (0–130) | 52 (23–130) | 61 (0–120) | 61 (0–120) | 45 (0–190) | 47 (43–50) |
| ≥52 mm | 61 (36) | 18 (58) *** | 13 (39) | 9 (60) | 32 (54) | 9 (64) | 16 (21) | 0 |
| <52 mm | 108 (64) | 13 (42) *** | 20 (61) | 6 (40) | 27 (46) | 5 (36) | 61 (79) | 2 (100) |
| Lauren classification | ||||||||
| Intestinal | 118 (70) | 26 (84) | 26 (79) | 12 (80) | 48 (81) | 12 (86) | 44(57) | 2 (100) |
| Diffuse | 21 (12) | 1 (3) | 0 | 0 | 3 (5) | 1 (7) | 18 (23) | 0 |
| Indeterminate | 30 (18) | 4 (13) | 7 (21) | 3 (20) | 8 (14) | 1 (7) | 15 (20) | 0 |
| Grading | ||||||||
| G1 | 10 (6) | 1 (3) | 3 (9) | 1 (7) | 3 (5) | 0 | 4 (5) | 0 |
| G2 | 59 (35) | 7 (23) | 14 (42) | 6 (40) | 16 (27) | 0 | 29 (38) | 1 (50) |
| G3 | 87 (51) | 22 (71) * | 15 (46) | 7 (46) | 38 (64) | 14 (100) | 34 (44) | 1 (50) |
| Not defined | 13 (8) | 1 (3) | 1 (3) | 1 (7) | 2 (4) | 0 | 10 (13) | 0 |
| Histotype-based prognostic classification | ||||||||
| Grade 1-low grade | ||||||||
| Muconodular | 1 (1) | 0 | 0 | 0 | 1 (2) | 0 | 0 | 0 |
| WD tubular | 3 (2) | 0 | 0 | 0 | 1 (2) | 0 | 2 (3) | 0 |
| DD low grade | 1 (1) | 0 | 0 | 0 | 0 | 0 | 1 (1) | 0 |
| HLR | 77 (45) | 28 (90) *** | 33 (100) | 15 (100) | 37 (63) | 12 (86) | 7 (9) | 1 (50) |
| Grade 2-Intermediate grade | ||||||||
| Ordinary cohesive | 58 (34) | 2 (7) | 0 | 0 | 16 (27) | 1 (7) | 42 (55) | 1 (50) |
| Ordinary diffuse | 18 (10) | 0 | 0 | 0 | 0 | 0 | 18 (23) | 0 |
| Ordinary mucinous | 3 (2) | 0 | 0 | 0 | 1 (2) | 0 | 2 (3) | 0 |
| Grade 3-High grade | ||||||||
| Anaplastic | 5 (3) | 1 (3) | 0 | 0 | 1 (2) | 1 (7) | 4 (5) | 0 |
| Mucinous invasive | 3 (2) | 0 | 0 | 0 | 2 (3) | 0 | 1 (1) | 0 |
| TNM Stage | ||||||||
| I | 21 (12) | 6 (19) * | 11 (33) | 5 (33) | 5 (8) | 1 (7) | 5 (7) | 0 |
| II | 65 (39) | 16 (52) * | 9 (27) | 5 (33) | 31 (53) | 10 (71) | 25 (32) | 1 (55) |
| III | 72 (43) | 8 (26) | 13 (40) | 5 (33) | 20 (34) | 3 (22) | 39 (51) | 0 |
| IV | 9 (5) | 1 (3) | 0 | 0 | 2 (3) | 0 | 7 (9) | 1 (55) |
| No stage | 2 (1) | 0 | 0 | 0 | 1 (2) | 0 | 1 (1) | 0 |
| pT | ||||||||
| T1a/b | 7 (4) | 4 (13) ** | 7 (21) | 4 (27) | 0 | 0 | 0 | 0 |
| T2 | 25 (15) | 4 (13) ** | 6 (18) | 2 (13) | 7 (12) | 2 (14) | 12 (16) | 0 |
| T3 | 93 (55) | 20 (64) | 17 (52) | 8 (53) | 39 (66) | 11 (79) | 37 (48) | 1 (50) |
| T4a/b | 44 (26) | 3 (10) | 3 (9) | 1 (7) | 13 (22) | 1 (7) | 28 (36) | 1 (50) |
| pN | ||||||||
| N0 | 59 (35) | 14 (45) | 15 (46) | 6 (40) | 27 (47) | 7 (50) | 17 (22) | 1 (50) |
| N1-3 | 108 (65) | 17 (55) | 18 (54) | 9 (60) | 31 (53) | 7 (50) | 59 (77) | 1 (50) |
| CD8+ TILs > 9.5 | 107 (69) | 29 (93) *** | 33 (100) | 15 (100) | 42 (71) | 12 (86) | 32 (51) | 2 (100) |
| CD8+ TILs ≤ 9.5 | 48 (31) | 2 (7) | 0 | 0 | 17 (29) | 2 (14) | 31 (49) | 0 |
| Feature | Total | EBV+ Cases | MSI Cases | MSS/EBV− Cases | p |
|---|---|---|---|---|---|
| N. of cases | 169 | 33 | 59 | 77 | |
| PD-1+ cases | 137 (81%) | 30 (91%) | 51 (86%) | 56 (73%) | * |
| PD-1+ TILs Mean (range) | 7 (0–74.6) | 17.5 (0–74.6) | 7 (0–35.3) | 3.1 (0–26.7) | *** |
| CD8+ TILs Mean (range) | 28.9 (0–167.1) | 64.2 (14.4–167.1) | 23.1 (0–69.2) | 15.8 (0–94.4) | * |
| PDL1+ TC cases | 31 (18%) | 15 (46%) | 14 (24%) | 2 (3%) | *** |
| PDL1+ TC Mean % ^ (range) | 25 (1–90) | 33 (1–90) | 18 (1–40) | 17.5 (15–20) | ** |
| PDL1+ IC cases | 72 (42%) | 31 (94%) | 22 (37%) | 19 (25%) | *** |
| PDL1+ TI | 31/72 (43%) | 18/31 (58%) | 12/22 (54%) | 1/19 (5%) | *** |
| PDL1+ IM | 41/72 (57) | 13/31 (42%) | 10/22 (46%) | 18/19 (95%) |
| Variable | p-Value | HR | 95% CI |
|---|---|---|---|
| Intestinal type vs. others | 0.0025 | 0.5156 | 0.3143–0.8457 |
| HLR type vs. others | <0.0001 | 2.6683 | 1.7298–4.1160 |
| Stage I/II vs. III/IV | <0.0001 | 2.9569 | 1.8946–4.6148 |
| pT2/pT3 vs. pT4 | <0.0001 | 2.6042 | 1.4849–4.5670 |
| pN0 vs. pN1/pN2/pN3 | 0.0021 | 2.2075 | 1.4088–3.4592 |
| CD8 > 9.5 cells/HPF | 0.015 | 0.5637 | 0.3358–0.9462 |
| EBV+/MSI vs. MSS/EBV− | 0.003 | 1.8981 | 1.2207–2.9513 |
| PD-L1 ≥ 5% vs. <5% | 0.012 | 0.4102 | 0.2408–0.6988 |
| Variable | Beta | SE | p-Value | Exp (Beta) | 95% CI of Exp (Beta) |
|---|---|---|---|---|---|
| Tumor stage | 0.9 | 0.2514 | 0.00035 | 2.4576 | 1.5052–4.0124 |
| CD8 > 9.5 cells/HPF | 0.55 | 0.2455 | 0.02455 | 1.7367 | 1.0760–2.8031 |
| PD-L1 ≥ 5% | 0.48 | 0.3864 | 0.2174 | 1.6105 | 0.7581–3.4211 |
| Lauren classification | 0.29 | 0.2616 | 0.2712 | 1.3335 | 0.8007–2.2208 |
| EBV presence | 0.29 | 0.4075 | 0.474 | 1.3388 | 0.6048–2.9636 |
| MSI status | 0.1 | 0.28 | 0.7271 | 1.1027 | 0.6387–1.9038 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Rosa, S.; Sahnane, N.; Tibiletti, M.G.; Magnoli, F.; Vanoli, A.; Sessa, F.; Chiaravalli, A.M. EBV+ and MSI Gastric Cancers Harbor High PD-L1/PD-1 Expression and High CD8+ Intratumoral Lymphocytes. Cancers 2018, 10, 102. https://doi.org/10.3390/cancers10040102
De Rosa S, Sahnane N, Tibiletti MG, Magnoli F, Vanoli A, Sessa F, Chiaravalli AM. EBV+ and MSI Gastric Cancers Harbor High PD-L1/PD-1 Expression and High CD8+ Intratumoral Lymphocytes. Cancers. 2018; 10(4):102. https://doi.org/10.3390/cancers10040102
Chicago/Turabian StyleDe Rosa, Simona, Nora Sahnane, Maria Grazia Tibiletti, Francesca Magnoli, Alessandro Vanoli, Fausto Sessa, and Anna Maria Chiaravalli. 2018. "EBV+ and MSI Gastric Cancers Harbor High PD-L1/PD-1 Expression and High CD8+ Intratumoral Lymphocytes" Cancers 10, no. 4: 102. https://doi.org/10.3390/cancers10040102
APA StyleDe Rosa, S., Sahnane, N., Tibiletti, M. G., Magnoli, F., Vanoli, A., Sessa, F., & Chiaravalli, A. M. (2018). EBV+ and MSI Gastric Cancers Harbor High PD-L1/PD-1 Expression and High CD8+ Intratumoral Lymphocytes. Cancers, 10(4), 102. https://doi.org/10.3390/cancers10040102