Lower Extremity Lymphedema in Gynecologic Cancer Patients: Propensity Score Matching Analysis of External Beam Radiation versus Brachytherapy

 ,
,  and
and
Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
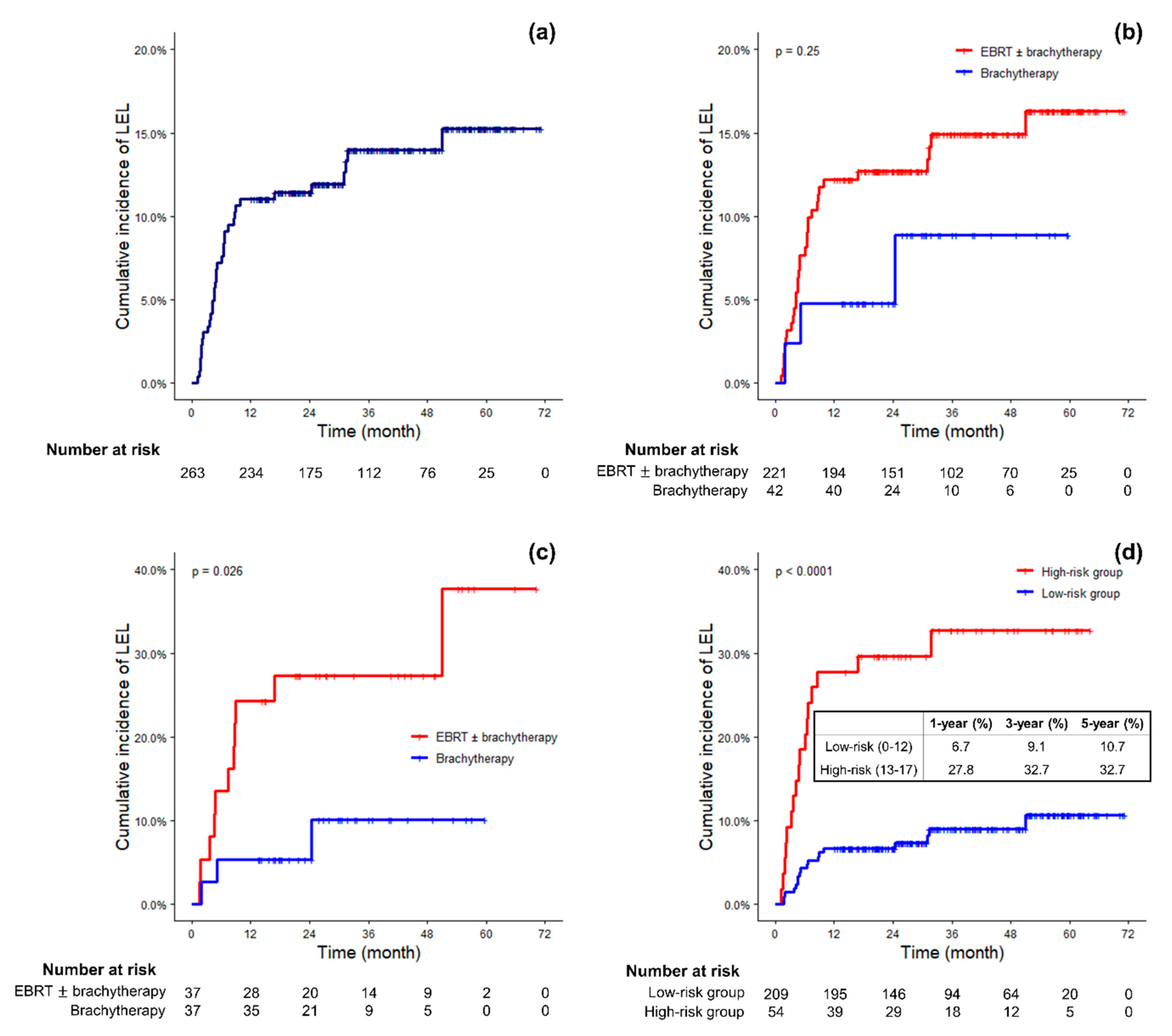
2.2. Overall Incidence of LEL
2.3. Risk Factors Associated with LEL
2.4. Risk Scores and Risk Groups of LEL Based on the Risk Factors
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Treatment
4.3. Diagnosis of LEL
4.4. Statistical Analysis
4.5. Ethics Statement
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Rowlands, I.J.; Beesley, V.L.; Janda, M.; Hayes, S.C.; Obermair, A.; Quinn, M.A.; Brand, A.; Leung, Y.; McQuire, L.; Webb, P.M. Quality of life of women with lower limb swelling or lymphedema 3–5 years following endometrial cancer. Gynecol. Oncol. 2014, 133, 314–318. [Google Scholar] [CrossRef] [PubMed]
- Greimel, E.R.; Vlasic, K.K.; Waldenstrom, A.C.; Duric, V.M.; Jensen, P.T.; Singer, S.; Chie, W.; Nordin, A.; Radisic, V.B.; Wydra, D. The European Organization for Research and Treatment of Cancer (EORTC) Quality-of-Life questionnaire cervical cancer module: EORTC QLQ-CX24. Cancer 2006, 107, 1812–1822. [Google Scholar] [CrossRef] [PubMed]
- Mendivil, A.A.; Rettenmaier, M.A.; Abaid, L.N.; Brown, J.V.; Micha, J.P.; Lopez, K.L.; Goldstein, B.H. Lower-extremity lymphedema following management for endometrial and cervical cancer. Surg. Oncol. 2016, 25, 200–204. [Google Scholar] [CrossRef] [PubMed]
- Yost, K.J.; Cheville, A.L.; Al-Hilli, M.M.; Mariani, A.; Barrette, B.A.; McGree, M.E.; Weaver, A.L.; Dowdy, S.C. Lymphedema after surgery for endometrial cancer: Prevalence, risk factors, and quality of life. Obstet. Gynecol. 2014, 124, 307–315. [Google Scholar] [CrossRef] [PubMed]
- Casley-Smith, J.R. Alterations of Untreated Lymphedema and It Grade Over Time. Lymphology 1995, 28, 174–185. [Google Scholar] [PubMed]
- Eby, C.S.; Brennan, M.J.; Fine, G. Lymphangiosarcoma: A Lethal Complication of Chronic Lymphedema: Report of Two Cases and Review of the Literature. Arch. Surg. 1967, 94, 223–230. [Google Scholar] [CrossRef]
- Huey, G.R.; Stehman, F.B.; Roth, L.M.; Ehrlich, C.E. Lymphangiosarcoma of the edematous thigh after radiation therapy for carcinoma of the vulva. Gynecol. Oncol. 1985, 20, 394–401. [Google Scholar] [CrossRef]
- Park, H.J.; Kim, H.J.; Wu, H.-G.; Kim, H.; Ha, S.W.; Kang, S.-B.; Song, Y.-S.; Park, N.-H.; Kim, J.-W. The influence of adjuvant radiotherapy on patterns of failure and survivals in uterine carcinosarcoma. Radiat. Oncol. J. 2011, 29, 228–235. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.; Suh, D.H.; Yang, E.J.; Lim, M.C.; Choi, J.Y.; Kim, K.; No, J.H.; Kim, Y.-B. Identifying risk factors for occult lower extremity lymphedema using computed tomography in patients undergoing lymphadenectomy for gynecologic cancers. Gynecol. Oncol. 2017, 144, 153–158. [Google Scholar] [CrossRef]
- Kim, J.H.; Choi, J.H.; Ki, E.Y.; Lee, S.J.; Yoon, J.H.; Lee, K.H.; Park, T.C.; Park, J.S.; Bae, S.N.; Hur, S.Y. Incidence and risk factors of lower-extremity lymphedema after radical surgery with or without adjuvant radiotherapy in patients with FIGO stage I to stage IIA cervical cancer. Int. J. Gynecol. Cancer 2012, 22, 686–691. [Google Scholar] [CrossRef]
- Bae, H.S.; Lim, M.C.; Lee, J.S.; Lee, Y.; Nam, B.H.; Seo, S.-S.; Kang, S.; Chung, S.H.; Kim, J.-Y.; Park, S.-Y. Postoperative Lower Extremity Edema in Patients with Primary Endometrial Cancer. Ann. Surg. Oncol. 2016, 23, 186–195. [Google Scholar] [CrossRef] [PubMed]
- Kuroda, K.; Yamamoto, Y.; Yanagisawa, M.; Kawata, A.; Akiba, N.; Suzuki, K.; Naritaka, K. Risk factors and a prediction model for lower limb lymphedema following lymphadenectomy in gynecologic cancer: A hospital-based retrospective cohort study. BMC Womens Health 2017, 17, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Ohba, Y.; Todo, Y.; Kobayashi, N.; Kaneuchi, M.; Watari, H.; Takeda, M.; Sudo, S.; Kudo, M.; Kato, H.; Sakuragi, N. Risk factors for lower-limb lymphedema after surgery for cervical cancer. Int. J. Clin. Oncol. 2011, 16, 238–243. [Google Scholar] [CrossRef] [PubMed]
- Beesley, V.L.; Rowlands, I.J.; Hayes, S.C.; Janda, M.; O’Rourke, P.; Marquart, L.; Quinn, M.A.; Spurdle, A.B.; Obermair, A.; Brand, A.; et al. Incidence, risk factors and estimates of a woman’s risk of developing secondary lower limb lymphedema and lymphedema-specific supportive care needs in women treated for endometrial cancer. Gynecol. Oncol. 2015, 136, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Karabuga, H.; Gultekin, M.; Tulunay, G.; Yuce, K.; Ayhan, A.; Yuce, D.; Yildiz, F. Assessing the quality of life in patients with endometrial cancer treated with adjuvant radiotherapy. Int. J. Gynecol. Cancer 2015, 25, 1526–1533. [Google Scholar] [CrossRef]
- Hopp, E.E.; Osborne, J.L.; Schneider, D.K.; Bojar, C.J.; Uyar, D.S. A prospective pilot study on the incidence of post-operative lymphedema in women with endometrial cancer. Gynecol. Oncol. Rep. 2016, 15, 25–28. [Google Scholar] [CrossRef] [PubMed]
- Deura, I.; Shimada, M.; Hirashita, K.; Sugimura, M.; Sato, S.; Sato, S.; Oishi, T.; Itamochi, H.; Harada, T.; Kigawa, J. Incidence and risk factors for lower limb lymphedema after gynecologic cancer surgery with initiation of periodic complex decongestive physiotherapy. Int. J. Clin. Oncol. 2015, 20, 556–560. [Google Scholar] [CrossRef]
- Ryan, M.; Stainton, M.C.; Slaytor, E.K.; Jaconelli, C.; Watts, S.; Mackenzie, P. Aetiology and prevalence of lower limb lymphoedema following treatment for gynaecological cancer. Aust. New Zeal. J. Obstet. Gynaecol. 2003, 43, 148–151. [Google Scholar] [CrossRef] [PubMed]
- Mitra, D.; Catalano, P.J.; Cimbak, N.; Damato, A.L.; Muto, M.G.; Viswanathan, A.N. The risk of lymphedema after postoperative radiation therapy in endometrial cancer. J. Gynecol. Oncol. 2016, 27, 1–11. [Google Scholar] [CrossRef]
- Todo, Y.; Yamazaki, H.; Takeshita, S.; Ohba, Y.; Sudo, S.; Minobe, S.; Okamoto, K.; Kato, H. Close relationship between removal of circumflex iliac nodes to distal external iliac nodes and postoperative lower-extremity lymphedema in uterine corpus malignant tumors. Gynecol. Oncol. 2015, 139, 160–164. [Google Scholar] [CrossRef]
- Barnett, J.C.; Havrilesky, L.J.; Bondurant, A.E.; Fleming, N.D.; Lee, P.S.; Secord, A.A.; Berchuck, A.; Valea, F.A. Adverse events associated with laparoscopy vs. laparotomy in the treatment of endometrial cancer. Am. J. Obstet. Gynecol. 2011, 205, e1–e143. [Google Scholar]
- Kuoppala, T.; Tomás, E.; Heinonen, P.K. Clinical outcome and complications of laparoscopic surgery compared with traditional surgery in women with endometrial cancer. Arch. Gynecol. Obstet. 2004, 270, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Atlan, D.; Touboul, E.; Deniaud-Alexandre, E.; Lefranc, J.-P.; Antoine, J.-M.; Jannet, D.; Lhuillier, P.; Uzan, M.; Huart, J.; Genestie, C.; et al. Operable Stages IB and II cervical carcinomas: A retrospective study comparing preoperative uterovaginal brachytherapy and postoperative radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2002, 54, 780–793. [Google Scholar] [CrossRef]
- Nout, R.A.; Putter, H.; Jürgenliemk-Schulz, I.M.; Jobsen, J.J.; Lutgens, L.C.H.W.; Van Der Steen-Banasik, E.M.; Mens, J.W.M.; Slot, A.; Stenfert Kroese, M.C.; Nijman, H.W.; et al. Five-year quality of life of endometrial cancer patients treated in the randomised Post Operative Radiation Therapy in Endometrial Cancer (PORTEC-2) trial and comparison with norm data. Eur. J. Cancer 2012, 48, 1638–1648. [Google Scholar] [CrossRef]
- Kumar, V.J.; Nin, C.Y.; Kuei, L.Y.; Tan, K.H.S.; Yeo, R.; Lam, P.Y.K. Survival and disease relapse in surgical stage I endometrioid adenocarcinoma of the uterus after adjuvant vaginal vault brachytherapy. Int. J. Gynecol. Cancer 2010, 20, 564–569. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Entire Cohort (Before Matching) | p | Matched Cohort (After Matching) | p | ||
|---|---|---|---|---|---|---|
| Brachytherapy | EBRT ± Brachytherapy | Brachytherapy | EBRT ± Brachytherapy | |||
| (n = 42) | (n = 221) | (n = 37) | (n = 37) | |||
| Age (years) | 0.007 * | 0.804* | ||||
| < 55 | 11 (26.2%) | 111 (50.2%) | 11 (29.7%) | 13 (35.1%) | ||
| ≥ 55 | 31 (73.8%) | 110 (49.8%) | 26 (70.3%) | 24 (64.9%) | ||
| Preoperative BMI (kg/m2) | 0.698 † | 1.000 * | ||||
| < 25 | 24 (57.1%) | 131 (59.3%) | 24 (64.9%) | 23 (62.2%) | ||
| ≥ 25 | 18 (42.9%) | 84 (38.0%) | 13 (35.1%) | 14 (37.8%) | ||
| Unknown | 0 (0.0%) | 6 (2.7%) | 0 (0.0%) | 0 (0.0%) | ||
| Hypertension | 19 (45.2%) | 54 (24.4%) | 0.010 * | 15 (40.5%) | 7 (18.9%) | 0.075 * |
| Diabetes mellitus | 8 (19.0%) | 22 (10.0%) | 0.151 * | 6 (16.2%) | 4 (10.8%) | 0.736 † |
| Chronic kidney disease | 3 (7.1%) | 3 (1.4%) | 0.054 † | 3 (8.1%) | 0 (0.0%) | 0.240 † |
| Peripheral vascular disease | 1 (2.4%) | 3 (1.4%) | 0.504 † | 1 (2.7%) | 2 (5.4%) | 1.000 † |
| Lower extremity surgery history | 5 (11.9%) | 15 (6.8%) | 0.407 * | 4 (10.8%) | 2 (5.4%) | 0.674 † |
| Origin of cancer | <0.001 † | 0.007 † | ||||
| Cervix | 5 (11.9%) | 121 (54.8%) | 4 (10.8%) | 15 (40.5%) | ||
| Endometrium | 37 (88.1%) | 88 (39.8%) | 33 (89.2%) | 22 (59.5%) | ||
| Uterine sarcoma | 0 (0.0%) | 7 (3.2%) | 0 (0.0%) | 0 (0.0%) | ||
| Double/Triple primary | 0 (0.0%) | 5 (2.3%) | 0 (0.0%) | 0 (0.0%) | ||
| FIGO stage (2009) | 0.002 † | 1.000† | ||||
| I–II | 42 (100.0%) | 178 (80.5%) | 37 (100.0%) | 36 (97.3%) | ||
| III | 0 (0.0%) | 39 (17.7%) | 0 (0.0%) | 0 (0.0%) | ||
| Unknown | 0 (0.0%) | 4 (1.8%) | 0 (0.0%) | 1 (2.7%) | ||
| Lymph node metastasis | 0 (0.0%) | 74 (33.5%) | <0.001 † | 37 (100.0%) | 34 (91.9%) | 0.240 † |
| Surgical approach | 0.001 * | 0.754 † | ||||
| Open | 5 (11.9%) | 87 (39.4%) | 5 (13.5%) | 5 (13.5%) | ||
| Laparoscopy | 37 (88.1%) | 133 (60.2%) | 32 (86.5%) | 31 (83.8%) | ||
| Vaginal | 0 (0.0%) | 1 (0.5%) | 0 (0.0%) | 1 (2.7%) | ||
| Number of pelvic LNs harvested | 0.376 * | 1.000 * | ||||
| ≤ 30 | 36 (85.7%) | 173 (78.3%) | 31 (83.8%) | 32 (86.5%) | ||
| > 30 | 6 (14.3%) | 48 (21.7%) | 6 (16.2%) | 5 (13.5%) | ||
| PALND | 14 (33.3%) | 71 (32.1%) | 1.000 * | 14 (37.8%) | 15 (40.5%) | 1.000 * |
| Adjuvant chemotherapy | 2 (4.8%) | 151 (68.3%) | <0.001 † | 2 (5.4%) | 2 (5.4%) | 1.000 † |
| Variable | Univariate | Multivariate | ||
|---|---|---|---|---|
| HR (95% CI) | p * | HR (95% CI) | p * | |
| Age ≥ 55 years | 1.207 (0.617–2.358) | 0.581 | ||
| Preoperative BMI ≥ 25 kg/m2 | 0.636 (0.306–1.325) | 0.227 | ||
| Hypertension | 0.774 (0.352–1.705) | 0.525 | ||
| Diabetes mellitus | 0.223 (0.301–1.630) | 0.139 | ||
| History of lower extremity surgery | 0.346 (0.047–2.529) | 0.346 | ||
| Endometrial cancer | 1.590 (0.814–3.109) | 0.175 | ||
| Lymph node metastasis | 1.167 (0.572–2.383) | 0.672 | ||
| Advanced FIGO stage | 1.217 (0.505–2.933) | 0.661 | ||
| Laparoscopic surgery | 2.034 (0.923–4.482) | 0.078 | 2.548 (1.131–5.740) | 0.024 |
| Number of pelvic LNs harvested > 30 | 2.106 (1.048–4.233) | 0.037 | 2.246 (1.093–4.616) | 0.028 |
| PALND | 2.391 (1.232–4.641) | 0.010 | 2.305 (1.180–4.502) | 0.014 |
| EBRT ± Brachytherapy | 1.969 (0.602–6.439) | 0.262 | ||
| Adjuvant chemotherapy | 0.744 (0.383–1.444) | 0.382 | ||
| Variable | HR * | Coefficient * | Risk Score |
|---|---|---|---|
| Laparoscopic surgery | 2.738 | 1.007 | +5 |
| Number of pelvic LNs harvested > 30 | 2.137 | 0.759 | +4 |
| PALND | 2.291 | 0.829 | +4 |
| EBRT ± Brachytherapy | 2.258 | 0.814 | +4 |
| Risk Score | n | % | 1-Year (%) | 3-Year (%) | 5-Year (%) |
|---|---|---|---|---|---|
| 0 | 2 | 0.8 | 0.0 | 0.0 | 0.0 |
| 4 | 48 | 18.3 | 2.1 | 5.1 | 5.1 |
| 5 | 21 | 8.0 | 0.0 | 8.3 | 8.3 |
| 8 | 29 | 11.0 | 10.3 | 14.8 | 14.8 |
| 9 | 95 | 36.1 | 8.4 | 8.4 | 13.0 |
| 12 | 14 | 5.3 | 14.3 | 14.3 | 14.3 |
| 13 | 45 | 17.1 | 26.7 | 32.5 | 32.5 |
| 17 | 9 | 3.4 | 33.3 | 33.3 | 33.3 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, W.I.; Kang, H.-C.; Wu, H.-G.; Kim, H.J.; Jeon, S.H.; Lee, M.; Kim, H.S.; Chung, H.H.; Kim, J.W.; Park, N.H.; et al. Lower Extremity Lymphedema in Gynecologic Cancer Patients: Propensity Score Matching Analysis of External Beam Radiation versus Brachytherapy. Cancers 2019, 11, 1471. https://doi.org/10.3390/cancers11101471
Chang WI, Kang H-C, Wu H-G, Kim HJ, Jeon SH, Lee M, Kim HS, Chung HH, Kim JW, Park NH, et al. Lower Extremity Lymphedema in Gynecologic Cancer Patients: Propensity Score Matching Analysis of External Beam Radiation versus Brachytherapy. Cancers. 2019; 11(10):1471. https://doi.org/10.3390/cancers11101471
Chicago/Turabian StyleChang, Won Ick, Hyun-Cheol Kang, Hong-Gyun Wu, Hak Jae Kim, Seung Hyuck Jeon, Maria Lee, Hee Seung Kim, Hyun Hoon Chung, Jae Weon Kim, Noh Hyun Park, and et al. 2019. "Lower Extremity Lymphedema in Gynecologic Cancer Patients: Propensity Score Matching Analysis of External Beam Radiation versus Brachytherapy" Cancers 11, no. 10: 1471. https://doi.org/10.3390/cancers11101471
APA StyleChang, W. I., Kang, H. -C., Wu, H. -G., Kim, H. J., Jeon, S. H., Lee, M., Kim, H. S., Chung, H. H., Kim, J. W., Park, N. H., Song, Y. S., & Seo, K. -S. (2019). Lower Extremity Lymphedema in Gynecologic Cancer Patients: Propensity Score Matching Analysis of External Beam Radiation versus Brachytherapy. Cancers, 11(10), 1471. https://doi.org/10.3390/cancers11101471