Causes for Frequent Pathogenic BRCA1 Variants Include Low Penetrance in Fertile Ages, Recurrent De-Novo Mutations and Genetic Drift


Abstract
:1. Introduction
2. Material and Methods
2.1. Patients and ethics
2.2. Material and Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Tharmaratnam, K.; Hagen, A.I.; Moller, P. MRI screening of women with hereditary predisposition to breast cancer: Diagnostic performance and survival analysis. Breast Cancer Res. Treat. 2014, 148, 687–688. [Google Scholar] [CrossRef] [PubMed]
- Finch, A.P.; Lubinski, J.; Moller, P.; Singer, C.F.; Karlan, B.; Senter, L.; Rosen, B.; Maehle, L.; Ghadirian, P.; Cybulski, C.; et al. Impact of oophorectomy on cancer incidence and mortality in women with a BRCA1 or BRCA2 mutation. J. Clin. Oncol. 2014, 32, 1547–1553. [Google Scholar] [CrossRef] [PubMed]
- Borg, A.; Dorum, A.; Heimdal, K.; Maehle, L.; Hovig, E.; Moller, P. BRCA1 1675delA and 1135insA account for one third of Norwegian familial breast-ovarian cancer and are associated with later disease onset than less frequent mutations. Dis. Mark. 1999, 15, 79–84. [Google Scholar] [CrossRef]
- Moller, P.; Maehle, L.; Engebretsen, L.F.; Ludvigsen, T.; Jonsrud, C.; Apold, J.; Vabo, A.; Clark, N. High penetrances of BRCA1 and BRCA2 mutations confirmed in a prospective series. Hered. Cancer Clin. Pract. 2010, 8, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moller, P.; Maehle, L.; Vabo, A.; Clark, N.; Sun, P.; Narod, S.A. Age-specific incidence rates for breast cancer in carriers of BRCA1 mutations from Norway. Clin. Genet. 2013, 83, 88–91. [Google Scholar] [CrossRef] [PubMed]
- Moller, P.; Hagen, A.I.; Apold, J.; Maehle, L.; Clark, N.; Fiane, B.; Lovslett, K.; Hovig, E.; Vabo, A. Genetic epidemiology of BRCA mutations--family history detects less than 50% of the mutation carriers. Eur. J. Cancer 2007, 43, 1713–1717. [Google Scholar] [CrossRef] [PubMed]
- Heimdal, K.; Maehle, L.; Apold, J.; Pedersen, J.C.; Moller, P. The Norwegian founder mutations in BRCA1: High penetrance confirmed in an incident cancer series and differences observed in the risk of ovarian cancer. Eur. J. Cancer 2003, 39, 2205–2213. [Google Scholar] [CrossRef]
- Rudkin, T.M.; Hamel, N.; Galvez, M.; Hogervorst, F.; Gille, J.J.; Moller, P.; Apold, J.; Foulkes, W.D. The frequent BRCA1 mutation 1135insA has multiple origins: A haplotype study in different populations. BMC Med. Genet. 2006, 7, 15. [Google Scholar] [CrossRef] [PubMed]
- Moller, P.; Seppala, T.T.; Bernstein, I.; Holinski-Feder, E.; Sala, P.; Gareth Evans, D.; Lindblom, A.; Macrae, F.; Blanco, I.; Sijmons, R.H.; et al. Cancer risk and survival in path_MMR carriers by gene and gender up to 75 years of age: A report from the Prospective Lynch Syndrome Database. Gut 2018, 67, 1306–1316. [Google Scholar] [CrossRef] [PubMed]
- Kuchenbaecker, K.B.; Hopper, J.L.; Barnes, D.R.; Phillips, K.A.; Mooij, T.M.; Roos-Blom, M.J.; Jervis, S.; van Leeuwen, F.E.; Milne, R.L.; Andrieu, N.; et al. Risks of Breast, Ovarian, and Contralateral Breast Cancer for BRCA1 and BRCA2. JAMA 2017, 317, 2402–2416. [Google Scholar] [CrossRef] [PubMed]
- Moller, P.; Heimdal, K.; Apold, J.; Fredriksen, A.; Borg, A.; Hovig, E.; Hagen, A.; Hagen, B.; Pedersen, J.C.; Maehle, L.; et al. Genetic epidemiology of BRCA1 mutations in Norway. Eur. J. Cancer 2001, 37, 2428–2434. [Google Scholar] [CrossRef]
- Jorgensen, K.J.; Gotzsche, P.C.; Kalager, M.; Zahl, P.H. Breast Cancer Screening in Denmark. Ann. Intern. Med. 2017, 167, 524. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Cancer Type | Path_BRCA1 Variant | 25yrs | 25ca | AIR25 (95%CI) | 30yrs | 30ca | AIR30 (95%CI) | 35yrs | 35ca | AIR35 (95%CI) | 40yrs | 40ca | AIR40 (95%CI) | 45yrs | 45ca | AIR45 (95%CI) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ovarian cancer | Frequent | 48 | 0 | 0 | 161 | 0 | 0 | 173 | 1 | 0.0058 | 115 | 5 | 0.0435 | 33 | 1 | 0.0303 |
| Infrequent | 36 | 0 | 0 | 100 | 0 | 0 | 107 | 0 | 0 | 80 | 1 | 0.0125 | 28 | 2 | 0.0714 | |
| Breast cancer | Frequent | 165 | 1 | 0.006 (0–0.034) | 463 | 0 | 0 (0–0.008) | 414 | 8 | 0.019 (0.008–0.038) | 219 | 4 | 0.018 (0.005–0.047) | 80 | 2 | 0.025 (0.003–0.090) |
| Infrequent | 134 | 1 | 0.008 (0–0.041) | 299 | 3 | 0.010 (0.002–0.029) | 297 | 10 | 0.034 (0.016–0.062) | 173 | 6 | 0.034 (0.013–0.076) | 95 | 3 | 0.032 (0.006–0.093) |
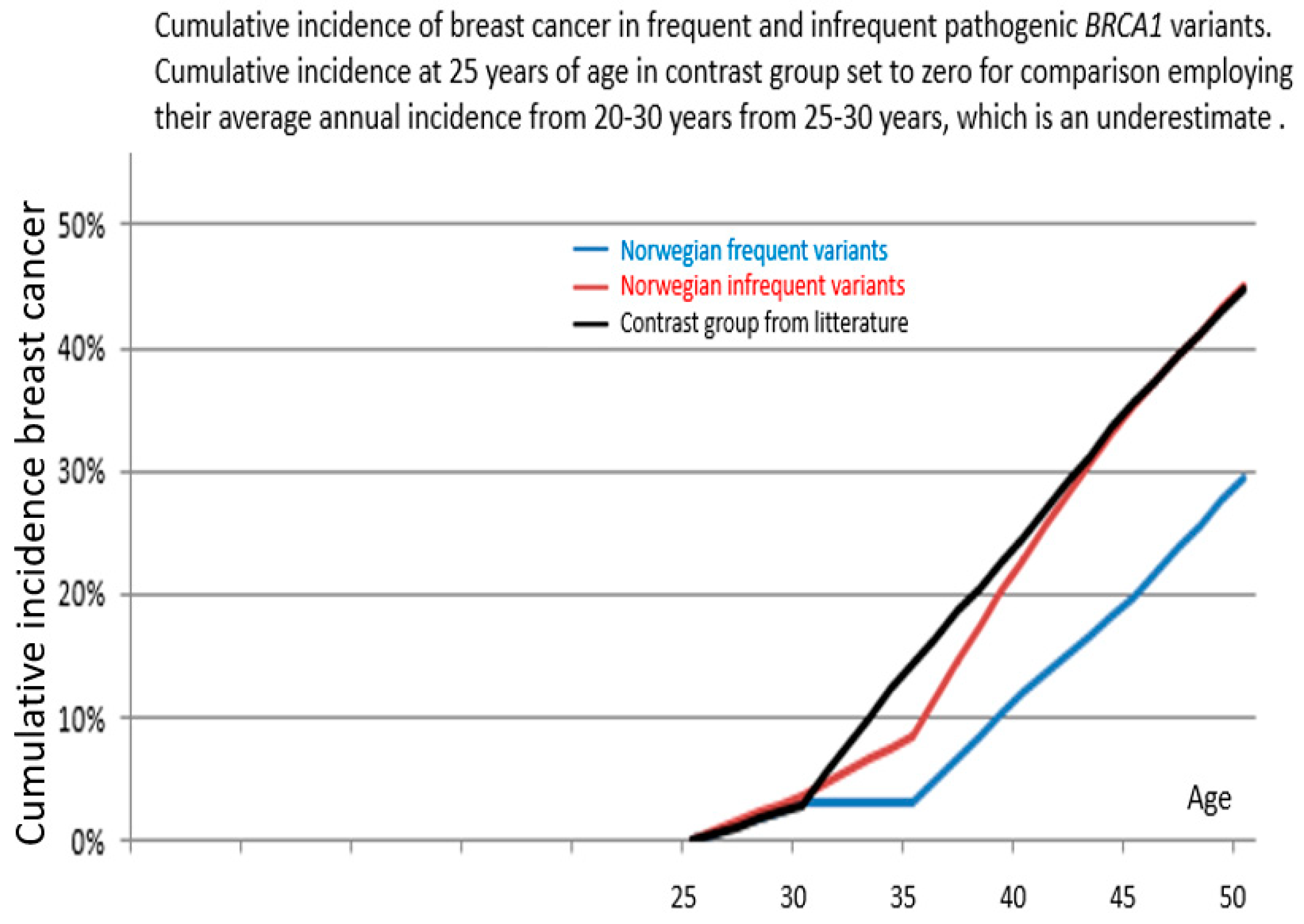
| Path_BRCA1 Variant | From 25 Years of Age to | Cumulative Incidence | 95% Confidence Interval | p-Value Versus Infrequent | p-Value Versus Kuchenbaeker et al. |
|---|---|---|---|---|---|
| Frequent | 40 years | 12% | 4–20% | 0.05 | 0.0001 |
| 45 years | 20% | 10–30% | 0.02 | 0.0001 | |
| 50 years | 29% | 14–45% * | 0.09 * | 0.01 * | |
| Infrequent | 40 years | 23% | 12–34% | ||
| 45 years | 35% | 22–48% | |||
| 50 years | 45% | 30–60% * | |||
| Kuchenbaeker et al. | 40 years | 24% | 21–28% | ||
| 45 years | 35% | 32–39% | |||
| 50 years | 45% | 41–49% |
| BRCA1 Variant | Number of Carriers |
|---|---|
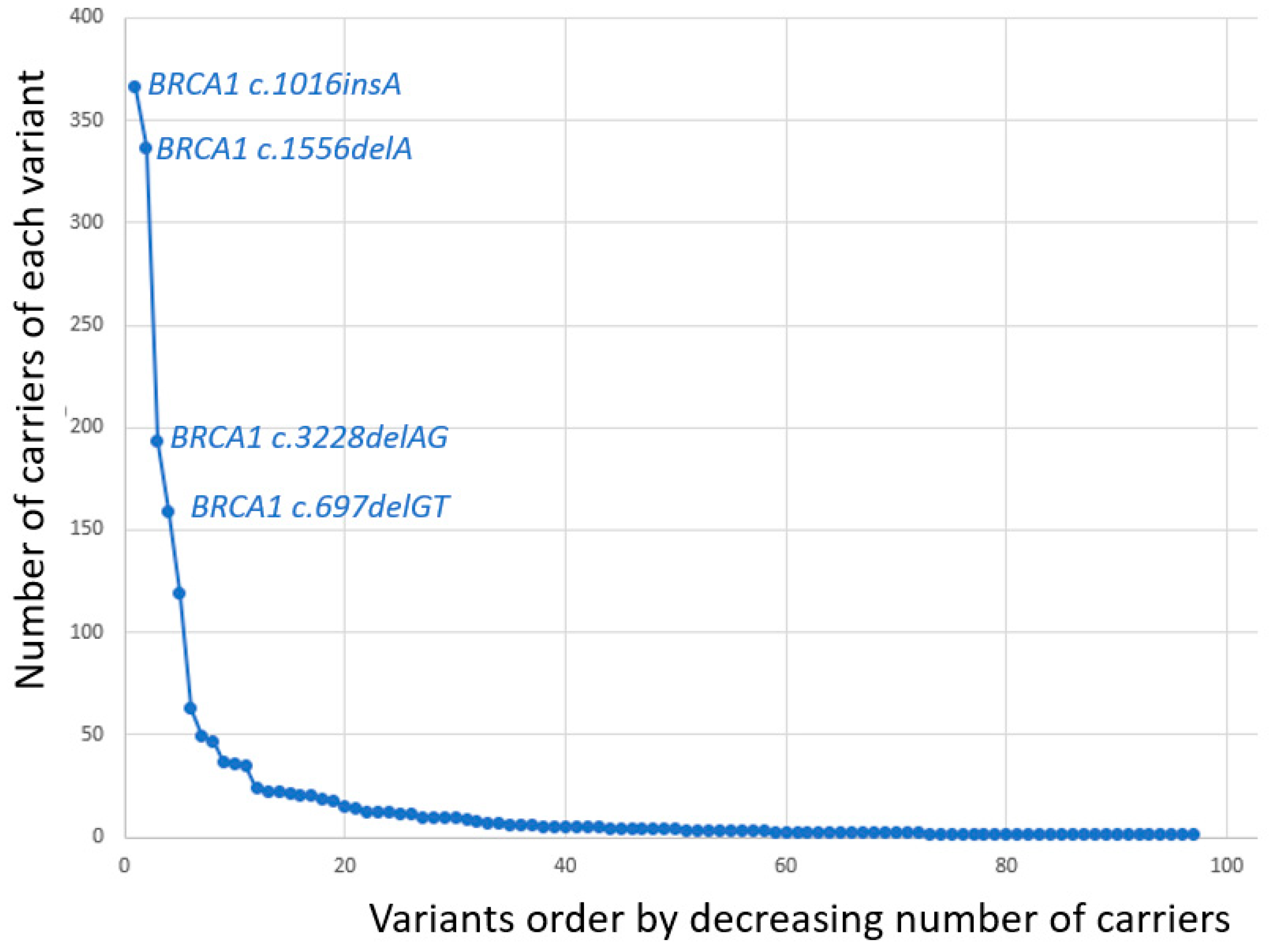
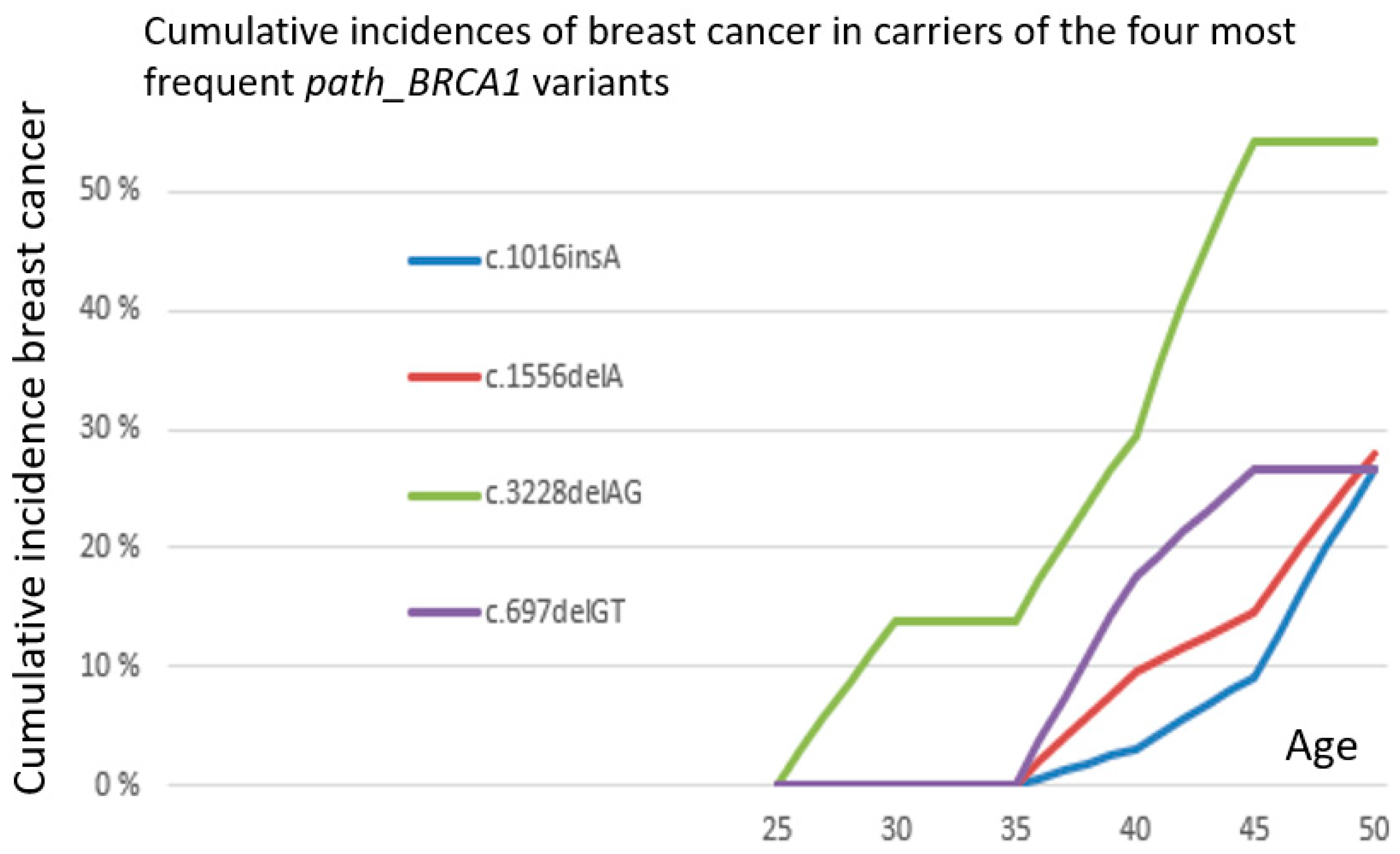
| c.1016dupA | 366 |
| c.1556delA | 337 |
| c.3228_3229delAG | 193 |
| c.697_698delGT | 159 |
| c.3178G>T | 119 |
| c.4745delA | 63 |
| c.1A>G | 49 |
| c.2351_2357delCGTTACT | 47 |
| c.5075-2A>C | 37 |
| c.3084_3094delTAATAACATTA | 36 |
| c.5047G>T | 35 |
| del exon 8–13 | 24 |
| c.3607C>T | 22 |
| dup exon 13 | 22 |
| c.3048_3052dupTGAGA | 21 |
| c.3331_3334delCAAG | 20 |
| c.5266dupC | 20 |
| del exon 22 | 19 |
| c.1072delC | 18 |
| c.5511G>A | 15 |
| c.1450G>T | 14 |
| c.3319G>T | 14 |
| c.2869C>T | 13 |
| c.5513T>G | 12 |
| c.66dupA | 12 |
| del exon 3-16 | 12 |
| c.2475delC | 11 |
| c.3966delA | 11 |
| c.1058G>A | 10 |
| c.2591C>G | 10 |
| c.4065_4068delTCAA | 9 |
| c.5407-25T>A | 8 |
| c.1292dupT | 7 |
| c.2558ins356 | 7 |
| c.3874delT | 6 |
| c.457_458ins21 | 6 |
| c.5251C>T | 6 |
| c.68_69delAG | 6 |
| c.1687C>T | 5 |
| c.3710delT | 5 |
| c.5503C>T | 5 |
| c.5534delA | 5 |
| c.794_795delCT | 5 |
| del exon 1–13 | 5 |
| c.4689C>G | 5 |
| c.115T>G | 4 |
| c.2989_2990dupAA | 4 |
| c.4035delA | 4 |
| c.4300delA | 4 |
| c.5213G>A | 4 |
| c.3770_3771delAG | 3 |
| c.4612C>T | 3 |
| c.5153G>C | 3 |
| c.848T>A | 3 |
| del exon 1–3 | 3 |
| c.1287delA | 2 |
| c.1695dupG | 2 |
| c.2389G>T | 2 |
| c.2438dupG | 2 |
| c.2681_2682delAA | 2 |
| c.3477_3479delAAAinsC | 2 |
| c.3700_3704delGTAAA | 2 |
| c.3835delG | 2 |
| c.386delG | 2 |
| c.4932_4933dupAA | 2 |
| c.4972delA | 2 |
| c.65T>C | 2 |
| del exon 18–24 | 2 |
| del exon 5–7 | 2 |
| c.1059G>A | 1 |
| c.130T>A | 1 |
| c.140G>T | 1 |
| c.1674dupA | 1 |
| c.1961dupA | 1 |
| c.2185G>T | 1 |
| c.241C>T | 1 |
| c.2722G>T | 1 |
| c.2727_2730delTCAA | 1 |
| c.3005delA | 1 |
| c.3817C>T | 1 |
| c.3937C>T | 1 |
| c.5075A>C | 1 |
| c.514C>T | 1 |
| c.5212G>A | 1 |
| c.5434C>G | 1 |
| c.929delA | 1 |
| del exon 13 | 1 |
| del exon 16 | 1 |
| del exon 20–24 | 1 |
| Sum | 1914 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Møller, P.; Dominguez-Valentin, M.; Rødland, E.A.; Hovig, E. Causes for Frequent Pathogenic BRCA1 Variants Include Low Penetrance in Fertile Ages, Recurrent De-Novo Mutations and Genetic Drift. Cancers 2019, 11, 132. https://doi.org/10.3390/cancers11020132
Møller P, Dominguez-Valentin M, Rødland EA, Hovig E. Causes for Frequent Pathogenic BRCA1 Variants Include Low Penetrance in Fertile Ages, Recurrent De-Novo Mutations and Genetic Drift. Cancers. 2019; 11(2):132. https://doi.org/10.3390/cancers11020132
Chicago/Turabian StyleMøller, Pål, Mev Dominguez-Valentin, Einar Andreas Rødland, and Eivind Hovig. 2019. "Causes for Frequent Pathogenic BRCA1 Variants Include Low Penetrance in Fertile Ages, Recurrent De-Novo Mutations and Genetic Drift" Cancers 11, no. 2: 132. https://doi.org/10.3390/cancers11020132
APA StyleMøller, P., Dominguez-Valentin, M., Rødland, E. A., & Hovig, E. (2019). Causes for Frequent Pathogenic BRCA1 Variants Include Low Penetrance in Fertile Ages, Recurrent De-Novo Mutations and Genetic Drift. Cancers, 11(2), 132. https://doi.org/10.3390/cancers11020132