Angiogenesis in Pancreatic Cancer: Pre-Clinical and Clinical Studies




Abstract
:1. Introduction
2. Angiogenesis in Pancreatic Cancer
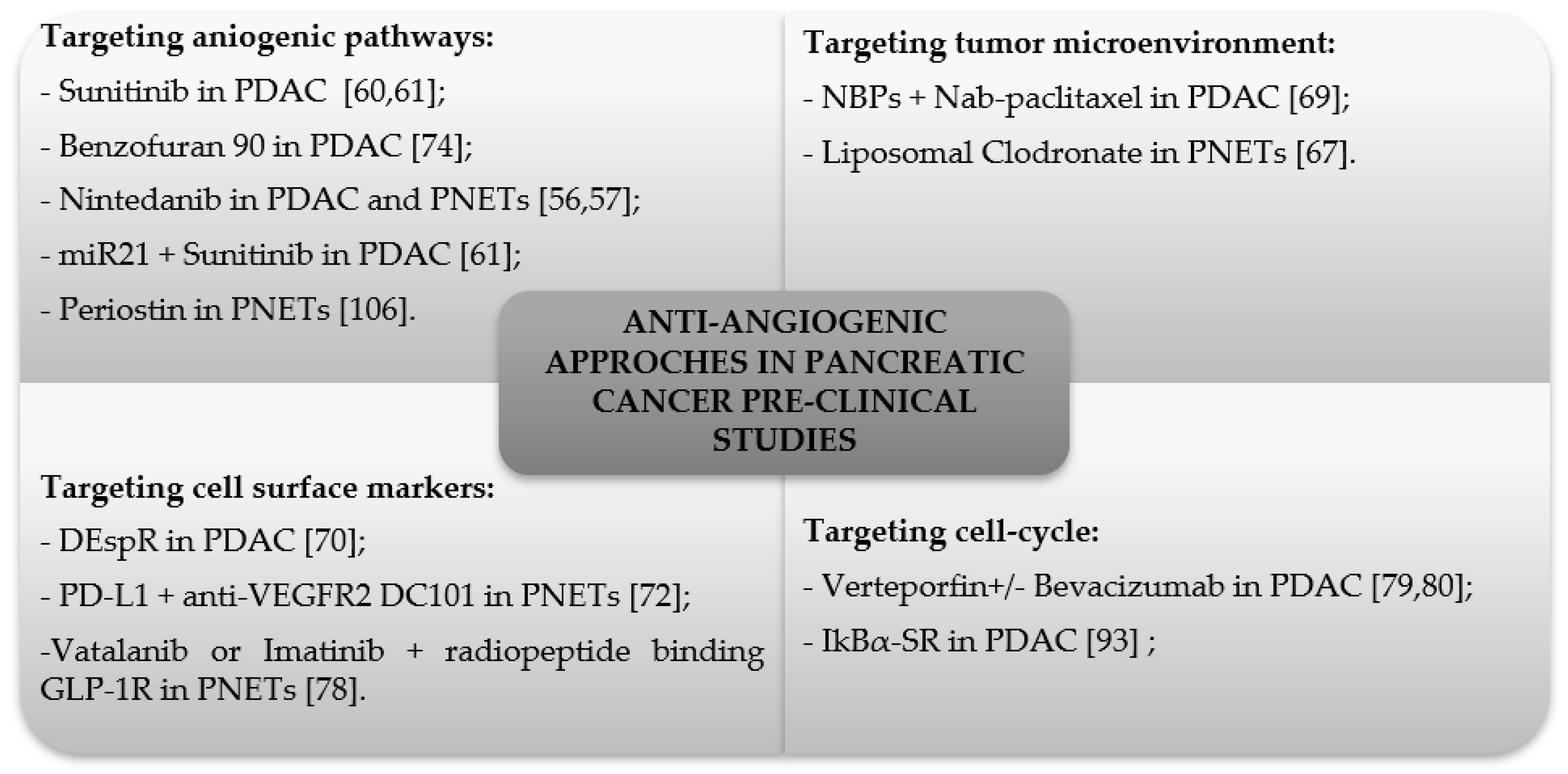
3. Anti-Angiogenic Inhibitors in Pre-Clinical Studies
4. Anti-Angiogenic Inhibitors in Clinical Studies
5. Concluding Remarks
Author Contributions
Funding
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: Globocan estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Bosetti, C.; Rosato, V.; Li, D.; Silverman, D.; Petersen, G.M.; Bracci, P.M.; Neale, R.E.; Muscat, J.; Anderson, K.; Gallinger, S.; et al. Diabetes, antidiabetic medications, and pancreatic cancer risk: An analysis from the international pancreatic cancer case-control consortium. Ann. Oncol. 2014, 25, 2065–2072. [Google Scholar] [CrossRef] [PubMed]
- Raimondi, S.; Lowenfels, A.B.; Morselli-Labate, A.M.; Maisonneuve, P.; Pezzilli, R. Pancreatic cancer in chronic pancreatitis; aetiology, incidence, and early detection. Best Pract. Res. Clin. Gastroenterol. 2010, 24, 349–358. [Google Scholar] [CrossRef]
- Schulte, A.; Pandeya, N.; Fawcett, J.; Fritschi, L.; Klein, K.; Risch, H.A.; Webb, P.M.; Whiteman, D.C.; Neale, R.E. Association between family cancer history and risk of pancreatic cancer. Cancer Epidemiol. 2016, 45, 145–150. [Google Scholar] [CrossRef] [PubMed]
- Yuan, C.; Morales-Oyarvide, V.; Babic, A.; Clish, C.B.; Kraft, P.; Bao, Y.; Qian, Z.R.; Rubinson, D.A.; Ng, K.; Giovannucci, E.L.; et al. Cigarette smoking and pancreatic cancer survival. J. Clin. Oncol. 2017, 35, 1822–1828. [Google Scholar] [CrossRef]
- Chen, W. WHO Classification of Tumors. Available online: http://www.pathologyoutlines.com/topic/pancreaswho.html (accessed on 21 January 2019).
- Tirado, C.A.; Shabsovich, D.S.; Ji, J.; Dawson, D. Pancreatic tumors: An overview. Atlas Genet. Cytogenet. Oncol. Haematol. 2014, 18, 125–132. [Google Scholar] [CrossRef]
- Kamisawa, T.; Wood, L.D.; Itoi, T.; Takaori, K. Pancreatic cancer. Lancet 2016, 388, 73–85. [Google Scholar] [CrossRef]
- Ferrone, C.R.; Brennan, M.F.; Gonen, M.; Coit, D.G.; Fong, Y.; Chung, S.; Tang, L.; Klimstra, D.; Allen, P.J. Pancreatic adenocarcinoma: The actual 5-year survivors. J. Gastrointest. Surg. 2008, 12, 701–706. [Google Scholar] [CrossRef]
- O’Reilly, E.M. Adjuvant therapy for pancreas adenocarcinoma: Where are we going? Expert Rev. Anticancer Ther. 2011, 11, 173–177. [Google Scholar] [CrossRef]
- Regine, W.F.; Winter, K.A.; Abrams, R.A.; Safran, H.; Hoffman, J.P.; Konski, A.; Benson, A.B.; Macdonald, J.S.; Kudrimoti, M.R.; Fromm, M.L.; et al. Fluorouracil vs. gemcitabine chemotherapy before and after fluorouracil-based chemoradiation following resection of pancreatic adenocarcinoma: A randomized controlled trial. JAMA 2008, 299, 1019–1026. [Google Scholar] [CrossRef]
- Paulson, A.S.; Tran Cao, H.S.; Tempero, M.A.; Lowy, A.M. Therapeutic advances in pancreatic cancer. Gastroenterology 2013, 144, 1316–1326. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Asa, S.L.; Dey, C.; Kennecke, H.; Laidley, D.; Law, C.; Asmis, T.; Chan, D.; Ezzat, S.; Goodwin, R.; et al. Diagnosis and management of gastrointestinal neuroendocrine tumors: An evidence-based canadian consensus. Cancer Treat. Rev. 2016, 47, 32–45. [Google Scholar] [CrossRef] [PubMed]
- Fendrich, V.; Waldmann, J.; Bartsch, D.K.; Langer, P. Surgical management of pancreatic endocrine tumors. Nat. Rev. Clin. Oncol. 2009, 6, 419–428. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.J.; Choi, D.W.; Choi, S.H.; Heo, J.S.; Park, H.J.; Choi, K.K.; Jang, K.T.; Sung, J.Y. Surgical strategies for non-functioning pancreatic neuroendocrine tumours. Br. J. Surg. 2012, 99, 1562–1568. [Google Scholar] [CrossRef]
- Kulke, M.H.; Bendell, J.; Kvols, L.; Picus, J.; Pommier, R.; Yao, J. Evolving diagnostic and treatment strategies for pancreatic neuroendocrine tumors. J. Hematol. Oncol. 2011, 4, 29. [Google Scholar] [CrossRef] [PubMed]
- Tomassetti, P.; Campana, D.; Piscitelli, L.; Casadei, R.; Santini, D.; Nori, F.; Morselli-Labate, A.M.; Pezzilli, R.; Corinaldesi, R. Endocrine pancreatic tumors: Factors correlated with survival. Ann. Oncol. 2005, 16, 1806–1810. [Google Scholar] [CrossRef] [PubMed]
- Kondo, N.I.; Ikeda, Y. Practical management and treatment of pancreatic neuroendocrine tumors. Gland Surg. 2014, 3, 276–283. [Google Scholar]
- Folkman, J. Tumor angiogenesis: Therapeutic implications. N. Engl. J. Med. 1971, 285, 1182–1186. [Google Scholar] [PubMed]
- Annese, T.; Tamma, R.; Ruggieri, S.; Ribatti, D. Erythropoietin in tumor angiogenesis. Exp. Cell Res. 2019, 374, 266–273. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Xu, H.X.; Wu, C.T.; Wang, W.Q.; Jin, W.; Gao, H.L.; Li, H.; Zhang, S.R.; Xu, J.Z.; Qi, Z.H.; et al. Angiogenesis in pancreatic cancer: Current research status and clinical implications. Angiogenesis 2019, 22, 15–36. [Google Scholar] [CrossRef] [PubMed]
- Franco, M.; Paez-Ribes, M.; Cortez, E.; Casanovas, O.; Pietras, K. Use of a mouse model of pancreatic neuroendocrine tumors to find pericyte biomarkers of resistance to anti-angiogenic therapy. Horm. Metab. Res. Horm. Stoffwechs. Horm. Metab. 2011, 43, 884–889. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Zhu, D.M.; Zhou, X.G.; Yin, N.; Zhang, Y.; Zhang, Z.X.; Li, D.C.; Zhou, J. Hif-2alpha promotes the formation of vasculogenic mimicry in pancreatic cancer by regulating the binding of twist1 to the ve-cadherin promoter. Oncotarget 2017, 8, 47801–47815. [Google Scholar] [PubMed]
- Li, A.; Cheng, X.J.; Moro, A.; Singh, R.K.; Hines, O.J.; Eibl, G. Cxcr2-dependent endothelial progenitor cell mobilization in pancreatic cancer growth. Transl. Oncol. 2011, 4, 20–28. [Google Scholar] [CrossRef] [PubMed]
- Maity, G.; Mehta, S.; Haque, I.; Dhar, K.; Sarkar, S.; Banerjee, S.K.; Banerjee, S. Pancreatic tumor cell secreted ccn1/cyr61 promotes endothelial cell migration and aberrant neovascularization. Sci. Rep. 2014, 4, 4995. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, K.; Sasajima, J.; Mizukami, Y.; Sugiyama, Y.; Yamazaki, M.; Fujii, R.; Kawamoto, T.; Koizumi, K.; Sato, K.; Fujiya, M.; et al. Hedgehog promotes neovascularization in pancreatic cancers by regulating ang-1 and igf-1 expression in bone-marrow derived pro-angiogenic cells. PLoS ONE 2010, 5, e8824. [Google Scholar] [CrossRef]
- Vizio, B.; Biasi, F.; Scirelli, T.; Novarino, A.; Prati, A.; Ciuffreda, L.; Montrucchio, G.; Poli, G.; Bellone, G. Pancreatic-carcinoma-cell-derived pro-angiogenic factors can induce endothelial-cell differentiation of a subset of circulating cd34+ progenitors. J. Transl. Med. 2013, 11, 314. [Google Scholar] [CrossRef]
- Vizio, B.; Novarino, A.; Giacobino, A.; Cristiano, C.; Prati, A.; Brondino, G.; Ciuffreda, L.; Bellone, G. Pilot study to relate clinical outcome in pancreatic carcinoma and angiogenic plasma factors/circulating mature/progenitor endothelial cells: Preliminary results. Cancer Sci. 2010, 101, 2448–2454. [Google Scholar] [CrossRef]
- Barau, A.; Ruiz-Sauri, A.; Valencia, G.; Gomez-Mateo Mdel, C.; Sabater, L.; Ferrandez, A.; Llombart-Bosch, A. High microvessel density in pancreatic ductal adenocarcinoma is associated with high grade. Virchows Arch. Int. J. Pathol. 2013, 462, 541–546. [Google Scholar] [CrossRef]
- Van der Zee, J.A.; van Eijck, C.H.; Hop, W.C.; van Dekken, H.; Dicheva, B.M.; Seynhaeve, A.L.; Koning, G.A.; Eggermont, A.M.; ten Hagen, T.L. Angiogenesis: A prognostic determinant in pancreatic cancer? Eur. J. Cancer 2011, 47, 2576–2584. [Google Scholar] [CrossRef]
- Wang, W.Q.; Liu, L.; Xu, H.X.; Luo, G.P.; Chen, T.; Wu, C.T.; Xu, Y.F.; Xu, J.; Liu, C.; Zhang, B.; et al. Intratumoral alpha-sma enhances the prognostic potency of cd34 associated with maintenance of microvessel integrity in hepatocellular carcinoma and pancreatic cancer. PLoS ONE 2013, 8, e71189. [Google Scholar]
- Huang, Y.; Yuan, J.; Righi, E.; Kamoun, W.S.; Ancukiewicz, M.; Nezivar, J.; Santosuosso, M.; Martin, J.D.; Martin, M.R.; Vianello, F.; et al. Vascular normalizing doses of antiangiogenic treatment reprogram the immunosuppressive tumor microenvironment and enhance immunotherapy. Proc. Natl. Acad. Sci. USA 2012, 109, 17561–17566. [Google Scholar] [CrossRef]
- Jain, R.K. Normalization of tumor vasculature: An emerging concept in antiangiogenic therapy. Science 2005, 307, 58–62. [Google Scholar] [CrossRef]
- Mpekris, F.; Baish, J.W.; Stylianopoulos, T.; Jain, R.K. Role of vascular normalization in benefit from metronomic chemotherapy. Proc. Natl. Acad. Sci. USA 2017, 114, 1994–1999. [Google Scholar] [CrossRef]
- Yapp, D.T.; Wong, M.Q.; Kyle, A.H.; Valdez, S.M.; Tso, J.; Yung, A.; Kozlowski, P.; Owen, D.A.; Buczkowski, A.K.; Chung, S.W.; et al. The differential effects of metronomic gemcitabine and antiangiogenic treatment in patient-derived xenografts of pancreatic cancer: Treatment effects on metabolism, vascular function, cell proliferation, and tumor growth. Angiogenesis 2016, 19, 229–244. [Google Scholar] [CrossRef]
- Xie, K.; Wei, D.; Huang, S. Transcriptional anti-angiogenesis therapy of human pancreatic cancer. Cytokine Growth Factor Rev. 2006, 17, 147–156. [Google Scholar] [CrossRef]
- Di Maggio, F.; Arumugam, P.; Delvecchio, F.R.; Batista, S.; Lechertier, T.; Hodivala-Dilke, K.; Kocher, H.M. Pancreatic stellate cells regulate blood vessel density in the stroma of pancreatic ductal adenocarcinoma. Pancreatol. Off. J. Int. Assoc. Pancreatol. 2016, 16, 995–1004. [Google Scholar] [CrossRef]
- Haqq, J.; Howells, L.M.; Garcea, G.; Metcalfe, M.S.; Steward, W.P.; Dennison, A.R. Pancreatic stellate cells and pancreas cancer: Current perspectives and future strategies. Eur. J. Cancer 2014, 50, 2570–2582. [Google Scholar] [CrossRef]
- Masamune, A.; Kikuta, K.; Watanabe, T.; Satoh, K.; Hirota, M.; Shimosegawa, T. Hypoxia stimulates pancreatic stellate cells to induce fibrosis and angiogenesis in pancreatic cancer. Am. J. Physiol. Gastrointest. Liver Physiol. 2008, 295, G709–G717. [Google Scholar] [CrossRef]
- Abrakov, L.V.; Astakhova, L.S.; Vatnitskaia, T.V.; Nemchin, E.; Fainshtein, I.I. State of neurosurgical information in soviet and foreign journals. Vopr. Neirokhirurgii 1976, 3, 52–58. [Google Scholar]
- Esposito, I.; Menicagli, M.; Funel, N.; Bergmann, F.; Boggi, U.; Mosca, F.; Bevilacqua, G.; Campani, D. Inflammatory cells contribute to the generation of an angiogenic phenotype in pancreatic ductal adenocarcinoma. J. Clin. Pathol. 2004, 57, 630–636. [Google Scholar] [CrossRef]
- Penny, H.L.; Sieow, J.L.; Adriani, G.; Yeap, W.H.; See Chi Ee, P.; San Luis, B.; Lee, B.; Lee, T.; Mak, S.Y.; Ho, Y.S.; et al. Warburg metabolism in tumor-conditioned macrophages promotes metastasis in human pancreatic ductal adenocarcinoma. Oncoimmunology 2016, 5, e1191731. [Google Scholar] [CrossRef]
- Kurahara, H.; Takao, S.; Kuwahata, T.; Nagai, T.; Ding, Q.; Maeda, K.; Shinchi, H.; Mataki, Y.; Maemura, K.; Matsuyama, T.; et al. Clinical significance of folate receptor beta-expressing tumor-associated macrophages in pancreatic cancer. Ann. Surg. Oncol. 2012, 19, 2264–2271. [Google Scholar] [CrossRef]
- Li, N.; Li, Y.; Li, Z.; Huang, C.; Yang, Y.; Lang, M.; Cao, J.; Jiang, W.; Xu, Y.; Dong, J.; et al. Hypoxia inducible factor 1 (hif-1) recruits macrophage to activate pancreatic stellate cells in pancreatic ductal adenocarcinoma. Int. J. Mol. Sci. 2016, 17, 799. [Google Scholar] [CrossRef]
- Whatcott, C.J.; Diep, C.H.; Jiang, P.; Watanabe, A.; LoBello, J.; Sima, C.; Hostetter, G.; Shepard, H.M.; Von Hoff, D.D.; Han, H. Desmoplasia in primary tumors and metastatic lesions of pancreatic cancer. Clin. Cancer Res. 2015, 21, 3561–3568. [Google Scholar] [CrossRef]
- Minchinton, A.I.; Tannock, I.F. Drug penetration in solid tumours. Nat. Rev. Cancer 2006, 6, 583–592. [Google Scholar] [CrossRef]
- Netti, P.A.; Berk, D.A.; Swartz, M.A.; Grodzinsky, A.J.; Jain, R.K. Role of extracellular matrix assembly in interstitial transport in solid tumors. Cancer Res. 2000, 60, 2497–2503. [Google Scholar]
- Hexige, S.; Ardito-Abraham, C.M.; Wu, Y.; Wei, Y.; Fang, Y.; Han, X.; Li, J.; Zhou, P.; Yi, Q.; Maitra, A.; et al. Identification of novel vascular projections with cellular trafficking abilities on the microvasculature of pancreatic ductal adenocarcinoma. J. Pathol. 2015, 236, 142–154. [Google Scholar]
- Casanovas, O.; Hicklin, D.J.; Bergers, G.; Hanahan, D. Drug resistance by evasion of antiangiogenic targeting of vegf signaling in late-stage pancreatic islet tumors. Cancer Cell 2005, 8, 299–309. [Google Scholar] [CrossRef]
- Terris, B.; Scoazec, J.Y.; Rubbia, L.; Bregeaud, L.; Pepper, M.S.; Ruszniewski, P.; Belghiti, J.; Flejou, J.; Degott, C. Expression of vascular endothelial growth factor in digestive neuroendocrine tumours. Histopathology 1998, 32, 133–138. [Google Scholar] [CrossRef]
- Takahashi, Y.; Akishima-Fukasawa, Y.; Kobayashi, N.; Sano, T.; Kosuge, T.; Nimura, Y.; Kanai, Y.; Hiraoka, N. Prognostic value of tumor architecture, tumor-associated vascular characteristics, and expression of angiogenic molecules in pancreatic endocrine tumors. Clin. Cancer Res. 2007, 13, 187–196. [Google Scholar] [CrossRef]
- Pavel, M.E.; Hassler, G.; Baum, U.; Hahn, E.G.; Lohmann, T.; Schuppan, D. Circulating levels of angiogenic cytokines can predict tumour progression and prognosis in neuroendocrine carcinomas. Clin. Endocrinol. 2005, 62, 434–443. [Google Scholar] [CrossRef]
- Kindler, H.L.; Ioka, T.; Richel, D.J.; Bennouna, J.; Letourneau, R.; Okusaka, T.; Funakoshi, A.; Furuse, J.; Park, Y.S.; Ohkawa, S.; et al. Axitinib plus gemcitabine versus placebo plus gemcitabine in patients with advanced pancreatic adenocarcinoma: A double-blind randomised phase 3 study. Lancet. Oncol. 2011, 12, 256–262. [Google Scholar] [CrossRef]
- Crane, C.H.; Winter, K.; Regine, W.F.; Safran, H.; Rich, T.A.; Curran, W.; Wolff, R.A.; Willett, C.G. Phase ii study of bevacizumab with concurrent capecitabine and radiation followed by maintenance gemcitabine and bevacizumab for locally advanced pancreatic cancer: Radiation therapy oncology group rtog 0411. J. Clin. Oncol. 2009, 27, 4096–4102. [Google Scholar] [CrossRef]
- Koukourakis, M.I.; Giatromanolaki, A.; Sheldon, H.; Buffa, F.M.; Kouklakis, G.; Ragoussis, I.; Sivridis, E.; Harris, A.L.; The Tumour and Angiogenesis Research Group. Phase i/ii trial of bevacizumab and radiotherapy for locally advanced inoperable colorectal cancer: Vasculature-independent radiosensitizing effect of bevacizumab. Clin. Cancer Res. 2009, 15, 7069–7076. [Google Scholar] [CrossRef]
- Awasthi, N.; Hinz, S.; Brekken, R.A.; Schwarz, M.A.; Schwarz, R.E. Nintedanib, a triple angiokinase inhibitor, enhances cytotoxic therapy response in pancreatic cancer. Cancer Lett. 2015, 358, 59–66. [Google Scholar] [CrossRef]
- Bill, R.; Fagiani, E.; Zumsteg, A.; Antoniadis, H.; Johansson, D.; Haefliger, S.; Albrecht, I.; Hilberg, F.; Christofori, G. Nintedanib is a highly effective therapeutic for neuroendocrine carcinoma of the pancreas (pnet) in the rip1tag2 transgenic mouse model. Clin. Cancer Res. 2015, 21, 4856–4867. [Google Scholar] [CrossRef]
- Faloppi, L.; Bianconi, M.; Giampieri, R.; Sobrero, A.; Labianca, R.; Ferrari, D.; Barni, S.; Aitini, E.; Zaniboni, A.; Boni, C.; et al. The value of lactate dehydrogenase serum levels as a prognostic and predictive factor for advanced pancreatic cancer patients receiving sorafenib. Oncotarget 2015, 6, 35087–35094. [Google Scholar] [CrossRef]
- Chiorean, E.G.; Schneider, B.P.; Akisik, F.M.; Perkins, S.M.; Anderson, S.; Johnson, C.S.; DeWitt, J.; Helft, P.; Clark, R.; Johnston, E.L.; et al. Phase 1 pharmacogenetic and pharmacodynamic study of sorafenib with concurrent radiation therapy and gemcitabine in locally advanced unresectable pancreatic cancer. Int. J. Radiat. Oncol. Biol. Phys. 2014, 89, 284–291. [Google Scholar] [CrossRef]
- Wegner, C.S.; Hauge, A.; Simonsen, T.G.; Gaustad, J.V.; Andersen, L.M.K.; Rofstad, E.K. Dce-mri of sunitinib-induced changes in tumor microvasculature and hypoxia: A study of pancreatic ductal adenocarcinoma xenografts. Neoplasia 2018, 20, 734–744. [Google Scholar] [CrossRef]
- Passadouro, M.; Pedroso de Lima, M.C.; Faneca, H. Microrna modulation combined with sunitinib as a novel therapeutic strategy for pancreatic cancer. Int. J. Nanomed. 2014, 9, 3203–3217. [Google Scholar]
- O’Reilly, E.M.; Niedzwiecki, D.; Hall, M.; Hollis, D.; Bekaii-Saab, T.; Pluard, T.; Douglas, K.; Abou-Alfa, G.K.; Kindler, H.L.; Schilsky, R.L.; et al. A cancer and leukemia group b phase ii study of sunitinib malate in patients with previously treated metastatic pancreatic adenocarcinoma (calgb 80603). Oncologist 2010, 15, 1310–1319. [Google Scholar] [CrossRef] [PubMed]
- Baker, C.H.; Solorzano, C.C.; Fidler, I.J. Blockade of vascular endothelial growth factor receptor and epidermal growth factor receptor signaling for therapy of metastatic human pancreatic cancer. Cancer Res. 2002, 62, 1996–2003. [Google Scholar]
- Pellat, A.; Dreyer, C.; Couffignal, C.; Walter, T.; Lombard-Bohas, C.; Niccoli, P.; Seitz, J.F.; Hentic, O.; Andre, T.; Coriat, R.; et al. Clinical and biomarker evaluations of sunitinib in patients with grade 3 digestive neuroendocrine neoplasms. Neuroendocrinology 2018, 107, 24–31. [Google Scholar] [CrossRef]
- Grande, E.; Capdevila, J.; Castellano, D.; Teule, A.; Duran, I.; Fuster, J.; Sevilla, I.; Escudero, P.; Sastre, J.; Garcia-Donas, J.; et al. Pazopanib in pretreated advanced neuroendocrine tumors: A phase ii, open-label trial of the spanish task force group for neuroendocrine tumors (getne). Ann. Oncol. 2015, 26, 1987–1993. [Google Scholar] [CrossRef]
- Bendell, J.C.; Zakari, A.; Lang, E.; Waterhouse, D.; Flora, D.; Alguire, K.; McCleod, M.; Peacock, N.; Ruehlman, P.; Lane, C.M.; et al. A phase ii study of the combination of bevacizumab, pertuzumab, and octreotide lar for patients with advanced neuroendocrine cancers. Cancer Investig. 2016, 34, 213–219. [Google Scholar] [CrossRef]
- Krug, S.; Abbassi, R.; Griesmann, H.; Sipos, B.; Wiese, D.; Rexin, P.; Blank, A.; Perren, A.; Haybaeck, J.; Huttelmaier, S.; et al. Therapeutic targeting of tumor-associated macrophages in pancreatic neuroendocrine tumors. Int. J. Cancer 2018, 143, 1806–1816. [Google Scholar] [CrossRef]
- Markert, C.L. Lactate dehydrogenase isozymes: Dissociation and recombination of subunits. Science 1963, 140, 1329–1330. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Villasana, V.; Rodriguez-Aguayo, C.; Arumugam, T.; Cruz-Monserrate, Z.; Fuentes-Mattei, E.; Deng, D.; Hwang, R.F.; Wang, H.; Ivan, C.; Garza, R.J.; et al. Bisphosphonates inhibit stellate cell activity and enhance antitumor effects of nanoparticle albumin-bound paclitaxel in pancreatic ductal adenocarcinoma. Mol. Cancer Ther. 2014, 13, 2583–2594. [Google Scholar] [CrossRef]
- Herrera, V.L.; Decano, J.L.; Tan, G.A.; Moran, A.M.; Pasion, K.A.; Matsubara, Y.; Ruiz-Opazo, N. Despr roles in tumor vasculo-angiogenesis, invasiveness, csc-survival and anoikis resistance: A ‘common receptor coordinator’ paradigm. PLoS ONE 2014, 9, e85821. [Google Scholar] [CrossRef]
- Cheng, Y.J.; Meng, C.T.; Ying, H.Y.; Zhou, J.F.; Yan, X.Y.; Gao, X.; Zhou, N.; Bai, C.M. Effect of endostar combined with chemotherapy in advanced well-differentiated pancreatic neuroendocrine tumors. Medicine 2018, 97, e12750. [Google Scholar] [CrossRef]
- Allen, E.; Jabouille, A.; Rivera, L.B.; Lodewijckx, I.; Missiaen, R.; Steri, V.; Feyen, K.; Tawney, J.; Hanahan, D.; Michael, I.P.; et al. Combined antiangiogenic and anti-pd-l1 therapy stimulates tumor immunity through hev formation. Sci. Transl. Med. 2017, 9, eaak9679. [Google Scholar] [CrossRef] [PubMed]
- Yamaue, H.; Tsunoda, T.; Tani, M.; Miyazawa, M.; Yamao, K.; Mizuno, N.; Okusaka, T.; Ueno, H.; Boku, N.; Fukutomi, A.; et al. Randomized phase ii/iii clinical trial of elpamotide for patients with advanced pancreatic cancer: Pegasus-pc study. Cancer Sci. 2015, 106, 883–890. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.L.; Yang, Y.R.; Mo, X.F.; Wei, J.L.; Zhang, X.J.; You, Q.D. Design, synthesis, and evaluation of benzofuran derivatives as novel anti-pancreatic carcinoma agents via interfering the hypoxia environment by targeting hif-1alpha pathway. Eur. J. Med. Chem. 2017, 137, 45–62. [Google Scholar] [CrossRef]
- Joka, M.; Boeck, S.; Zech, C.J.; Seufferlein, T.; Wichert, G.; Licht, T.; Krause, A.; Jauch, K.W.; Heinemann, V.; Bruns, C.J. Combination of antiangiogenic therapy using the mtor-inhibitor everolimus and low-dose chemotherapy for locally advanced and/or metastatic pancreatic cancer: A dose-finding study. Anti Cancer Drugs 2014, 25, 1095–1101. [Google Scholar] [CrossRef]
- Waters, J.A.; Matos, J.; Yip-Schneider, M.; Aguilar-Saavedra, J.R.; Crean, C.D.; Beane, J.D.; Dumas, R.P.; Suvannasankha, A.; Schmidt, C.M. Targeted nuclear factor-kappab suppression enhances gemcitabine response in human pancreatic tumor cell line murine xenografts. Surgery 2015, 158, 881–888, discussion 888–889. [Google Scholar] [CrossRef] [PubMed]
- Yao, J.C.; Guthrie, K.A.; Moran, C.; Strosberg, J.R.; Kulke, M.H.; Chan, J.A.; LoConte, N.; McWilliams, R.R.; Wolin, E.M.; Mattar, B.; et al. Phase iii prospective randomized comparison trial of depot octreotide plus interferon alfa-2b versus depot octreotide plus bevacizumab in patients with advanced carcinoid tumors: Swog s0518. J. Clin. Oncol. 2017, 35, 1695–1703. [Google Scholar] [CrossRef]
- Wicki, A.; Wild, D.; Pretre, V.; Mansi, R.; Orleth, A.; Reubi, J.C.; Rochlitz, C.; Mamot, C.; Macke, H.R.; Christofori, G. Synergism of peptide receptor-targeted auger electron radiation therapy with anti-angiogenic compounds in a mouse model of neuroendocrine tumors. Ejnmmi Res. 2014, 4, 9. [Google Scholar] [CrossRef]
- Wei, H.; Wang, F.; Wang, Y.; Li, T.; Xiu, P.; Zhong, J.; Sun, X.; Li, J. Verteporfin suppresses cell survival, angiogenesis and vasculogenic mimicry of pancreatic ductal adenocarcinoma via disrupting the yap-tead complex. Cancer Sci. 2017, 108, 478–487. [Google Scholar] [CrossRef]
- Tangutoori, S.; Spring, B.Q.; Mai, Z.; Palanisami, A.; Mensah, L.B.; Hasan, T. Simultaneous delivery of cytotoxic and biologic therapeutics using nanophotoactivatable liposomes enhances treatment efficacy in a mouse model of pancreatic cancer. Nanomed. Nanotechnol. Biol. Med. 2016, 12, 223–234. [Google Scholar] [CrossRef]
- Capozzi, M.; Von Arx, C.; De Divitiis, C.; Ottaiano, A.; Tatangelo, F.; Romano, G.M.; Tafuto, S. Antiangiogenic therapy in pancreatic neuroendocrine tumors. Anticancer Res. 2016, 36, 5025–5030. [Google Scholar] [CrossRef]
- Longo, V.; Brunetti, O.; Gnoni, A.; Cascinu, S.; Gasparini, G.; Lorusso, V.; Ribatti, D.; Silvestris, N. Angiogenesis in pancreatic ductal adenocarcinoma: A controversial issue. Oncotarget 2016, 7, 58649–58658. [Google Scholar] [CrossRef]
- Bruns, C.J.; Shrader, M.; Harbison, M.T.; Portera, C.; Solorzano, C.C.; Jauch, K.W.; Hicklin, D.J.; Radinsky, R.; Ellis, L.M. Effect of the vascular endothelial growth factor receptor-2 antibody dc101 plus gemcitabine on growth, metastasis and angiogenesis of human pancreatic cancer growing orthotopically in nude mice. Int. J. Cancer 2002, 102, 101–108. [Google Scholar] [CrossRef]
- Duan, J.X.; Jiao, H.; Kaizerman, J.; Stanton, T.; Evans, J.W.; Lan, L.; Lorente, G.; Banica, M.; Jung, D.; Wang, J.; et al. Potent and highly selective hypoxia-activated achiral phosphoramidate mustards as anticancer drugs. J. Med. Chem. 2008, 51, 2412–2420. [Google Scholar] [CrossRef]
- Jacobetz, M.A.; Chan, D.S.; Neesse, A.; Bapiro, T.E.; Cook, N.; Frese, K.K.; Feig, C.; Nakagawa, T.; Caldwell, M.E.; Zecchini, H.I.; et al. Hyaluronan impairs vascular function and drug delivery in a mouse model of pancreatic cancer. Gut 2013, 62, 112–120. [Google Scholar] [CrossRef]
- Melisi, D.; Ishiyama, S.; Sclabas, G.M.; Fleming, J.B.; Xia, Q.; Tortora, G.; Abbruzzese, J.L.; Chiao, P.J. Ly2109761, a novel transforming growth factor beta receptor type i and type ii dual inhibitor, as a therapeutic approach to suppressing pancreatic cancer metastasis. Mol. Cancer Ther. 2008, 7, 829–840. [Google Scholar] [CrossRef]
- Shimamura, T.; Royal, R.E.; Kioi, M.; Nakajima, A.; Husain, S.R.; Puri, R.K. Interleukin-4 cytotoxin therapy synergizes with gemcitabine in a mouse model of pancreatic ductal adenocarcinoma. Cancer Res. 2007, 67, 9903–9912. [Google Scholar] [CrossRef]
- Olive, K.P.; Jacobetz, M.A.; Davidson, C.J.; Gopinathan, A.; McIntyre, D.; Honess, D.; Madhu, B.; Goldgraben, M.A.; Caldwell, M.E.; Allard, D.; et al. Inhibition of hedgehog signaling enhances delivery of chemotherapy in a mouse model of pancreatic cancer. Science 2009, 324, 1457–1461. [Google Scholar] [CrossRef]
- Provenzano, P.P.; Cuevas, C.; Chang, A.E.; Goel, V.K.; Von Hoff, D.D.; Hingorani, S.R. Enzymatic targeting of the stroma ablates physical barriers to treatment of pancreatic ductal adenocarcinoma. Cancer Cell 2012, 21, 418–429. [Google Scholar] [CrossRef]
- Atwood, W.J.; Shah, K.V. Polyomaviruses Encyclopedia of Life Sciences; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2003. [Google Scholar] [CrossRef]
- Hanahan, D. Heritable formation of pancreatic beta-cell tumours in transgenic mice expressing recombinant insulin/simian virus 40 oncogenes. Nature 1985, 315, 115–122. [Google Scholar] [CrossRef]
- Christensen, J.G. A preclinical review of sunitinib, a multitargeted receptor tyrosine kinase inhibitor with anti-angiogenic and antitumour activities. Ann. Oncol. 2007, 18 (Suppl. 10), x3–x10. [Google Scholar] [CrossRef]
- Prabhu, L.; Mundade, R.; Korc, M.; Loehrer, P.J.; Lu, T. Critical role of nf-kappab in pancreatic cancer. Oncotarget 2014, 5, 10969–10975. [Google Scholar] [CrossRef] [PubMed]
- Fujimoto, K.; Hosotani, R.; Wada, M.; Lee, J.U.; Koshiba, T.; Miyamoto, Y.; Tsuji, S.; Nakajima, S.; Doi, R.; Imamura, M. Expression of two angiogenic factors, vascular endothelial growth factor and platelet-derived endothelial cell growth factor in human pancreatic cancer, and its relationship to angiogenesis. Eur. J. Cancer 1998, 34, 1439–1447. [Google Scholar] [CrossRef]
- Wagner, M.; Lopez, M.E.; Cahn, M.; Korc, M. Suppression of fibroblast growth factor receptor signaling inhibits pancreatic cancer growth in vitro and in vivo. Gastroenterology 1998, 114, 798–807. [Google Scholar] [CrossRef]
- Assifi, M.M.; Hines, O.J. Anti-angiogenic agents in pancreatic cancer: A review. Anti Cancer Agents Med. Chem. 2011, 11, 464–469. [Google Scholar] [CrossRef]
- Masamune, A.; Kikuta, K.; Watanabe, T.; Satoh, K.; Satoh, A.; Shimosegawa, T. Pancreatic stellate cells express toll-like receptors. J. Gastroenterol. 2008, 43, 352–362. [Google Scholar] [CrossRef]
- Masamune, A.; Shimosegawa, T. Signal transduction in pancreatic stellate cells. J. Gastroenterol. 2009, 44, 249–260. [Google Scholar] [CrossRef]
- Shimizu, K.; Kobayashi, M.; Tahara, J.; Shiratori, K. Cytokines and peroxisome proliferator-activated receptor gamma ligand regulate phagocytosis by pancreatic stellate cells. Gastroenterology 2005, 128, 2105–2118. [Google Scholar] [CrossRef]
- Awasthi, N.; Zhang, C.; Schwarz, A.M.; Hinz, S.; Schwarz, M.A.; Schwarz, R.E. Enhancement of nab-paclitaxel antitumor activity through addition of multitargeting antiangiogenic agents in experimental pancreatic cancer. Mol. Cancer Ther. 2014, 13, 1032–1043. [Google Scholar] [CrossRef]
- Mardin, W.A.; Mees, S.T. Micrornas: Novel diagnostic and therapeutic tools for pancreatic ductal adenocarcinoma? Ann. Surg. Oncol. 2009, 16, 3183–3189. [Google Scholar] [CrossRef]
- Hanahan, D.; Weinberg, R.A. Hallmarks of cancer: The next generation. Cell 2011, 144, 646–674. [Google Scholar] [CrossRef] [PubMed]
- Motz, G.T.; Coukos, G. The parallel lives of angiogenesis and immunosuppression: Cancer and other tales. Nat. Rev. Immunol. 2011, 11, 702–711. [Google Scholar] [CrossRef] [PubMed]
- Mahoney, K.M.; Rennert, P.D.; Freeman, G.J. Combination cancer immunotherapy and new immunomodulatory targets. Nat. Rev. Drug Discov. 2015, 14, 561–584. [Google Scholar] [CrossRef] [PubMed]
- Sharma, P.; Allison, J.P. Immune checkpoint targeting in cancer therapy: Toward combination strategies with curative potential. Cell 2015, 161, 205–214. [Google Scholar] [CrossRef]
- Keklikoglou, I.; Kadioglu, E.; Bissinger, S.; Langlois, B.; Bellotti, A.; Orend, G.; Ries, C.H.; De Palma, M. Periostin limits tumor response to vegfa inhibition. Cell Rep. 2018, 22, 2530–2540. [Google Scholar] [CrossRef] [PubMed]
- Giordano, F.J.; Johnson, R.S. Angiogenesis: The role of the microenvironment in flipping the switch. Curr. Opin. Genet. Dev. 2001, 11, 35–40. [Google Scholar] [CrossRef]
- Semenza, G.L. Hif-1: Mediator of physiological and pathophysiological responses to hypoxia. J. Appl. Physiol. 2000, 88, 1474–1480. [Google Scholar] [CrossRef] [PubMed]
- Hecht, J.R.; Trarbach, T.; Hainsworth, J.D.; Major, P.; Jager, E.; Wolff, R.A.; Lloyd-Salvant, K.; Bodoky, G.; Pendergrass, K.; Berg, W.; et al. Randomized, placebo-controlled, phase iii study of first-line oxaliplatin-based chemotherapy plus ptk787/zk 222584, an oral vascular endothelial growth factor receptor inhibitor, in patients with metastatic colorectal adenocarcinoma. J. Clin. Oncol. 2011, 29, 1997–2003. [Google Scholar] [CrossRef]
- Van Cutsem, E.; Bajetta, E.; Valle, J.; Kohne, C.H.; Hecht, J.R.; Moore, M.; Germond, C.; Berg, W.; Chen, B.L.; Jalava, T.; et al. Randomized, placebo-controlled, phase iii study of oxaliplatin, fluorouracil, and leucovorin with or without ptk787/zk 222584 in patients with previously treated metastatic colorectal adenocarcinoma. J. Clin. Oncol. 2011, 29, 2004–2010. [Google Scholar] [CrossRef] [PubMed]
- Wada, S.; Tsunoda, T.; Baba, T.; Primus, F.J.; Kuwano, H.; Shibuya, M.; Tahara, H. Rationale for antiangiogenic cancer therapy with vaccination using epitope peptides derived from human vascular endothelial growth factor receptor 2. Cancer Res. 2005, 65, 4939–4946. [Google Scholar] [CrossRef]
- Soliman, G.A. The mammalian target of rapamycin signaling network and gene regulation. Curr. Opin. Lipidol. 2005, 16, 317–323. [Google Scholar] [CrossRef]
- Plastaras, J.P.; Kim, S.H.; Liu, Y.Y.; Dicker, D.T.; Dorsey, J.F.; McDonough, J.; Cerniglia, G.; Rajendran, R.R.; Gupta, A.; Rustgi, A.K.; et al. Cell cycle dependent and schedule-dependent antitumor effects of sorafenib combined with radiation. Cancer Res. 2007, 67, 9443–9454. [Google Scholar] [CrossRef] [PubMed]
- Suen, A.W.; Galoforo, S.; Marples, B.; McGonagle, M.; Downing, L.; Martinez, A.A.; Robertson, J.M.; Wilson, G.D. Sorafenib and radiation: A promising combination in colorectal cancer. Int. J. Radiat. Oncol. Biol. Phys. 2010, 78, 213–220. [Google Scholar] [CrossRef] [PubMed]
- Kindler, H.L.; Niedzwiecki, D.; Hollis, D.; Sutherland, S.; Schrag, D.; Hurwitz, H.; Innocenti, F.; Mulcahy, M.F.; O’Reilly, E.; Wozniak, T.F.; et al. Gemcitabine plus bevacizumab compared with gemcitabine plus placebo in patients with advanced pancreatic cancer: Phase iii trial of the cancer and leukemia group b (calgb 80303). J. Clin. Oncol. 2010, 28, 3617–3622. [Google Scholar] [CrossRef]
- Pant, S.; Martin, L.K.; Geyer, S.; Wei, L.; Van Loon, K.; Sommovilla, N.; Zalupski, M.; Iyer, R.; Fogelman, D.; Ko, A.H.; et al. Treatment-related hypertension as a pharmacodynamic biomarker for the efficacy of bevacizumab in advanced pancreas cancer: A pooled analysis of 4 prospective trials of gemcitabine-based therapy with bevacizumab. Am. J. Clin. Oncol. 2016, 39, 614–618. [Google Scholar] [CrossRef]
- O’Reilly, M.S.; Boehm, T.; Shing, Y.; Fukai, N.; Vasios, G.; Lane, W.S.; Flynn, E.; Birkhead, J.R.; Olsen, B.R.; Folkman, J. Endostatin: An endogenous inhibitor of angiogenesis and tumor growth. Cell 1997, 88, 277–285. [Google Scholar] [CrossRef]
- Sasaki, T.; Fukai, N.; Mann, K.; Gohring, W.; Olsen, B.R.; Timpl, R. Structure, function and tissue forms of the c-terminal globular domain of collagen xviii containing the angiogenesis inhibitor endostatin. EMBO J. 1998, 17, 4249–4256. [Google Scholar] [CrossRef]
- Song, H.F.; Liu, X.W.; Zhang, H.N.; Zhu, B.Z.; Yuan, S.J.; Liu, S.Y.; Tang, Z.M. Pharmacokinetics of his-tag recombinant human endostatin in rhesus monkeys. Acta Pharmacol. Sin. 2005, 26, 124–128. [Google Scholar] [CrossRef] [PubMed]
- Han, B.H.; Xiu, Q.Y.; Wang, H.M.; Shen, J.; Gu, A.Q.; Luo, Y.; Bai, C.X.; Guo, S.L.; Liu, W.C.; Zhuang, Z.X.; et al. A multicenter, randomized, double-blind, placebo-controlled safety study to evaluate the clinical effects and quality of life of paclitaxel-carboplatin (PC) alone or combined with endostar for advanced non-small cell lung cancer (NSCLC). Zhonghua Zhong Liu Za Zhi Chin. J. Oncol. 2011, 33, 854–859. [Google Scholar]
- Blumenthal, G.M.; Cortazar, P.; Zhang, J.J.; Tang, S.; Sridhara, R.; Murgo, A.; Justice, R.; Pazdur, R. Fda approval summary: Sunitinib for the treatment of progressive well-differentiated locally advanced or metastatic pancreatic neuroendocrine tumors. Oncologist 2012, 17, 1108–1113. [Google Scholar] [CrossRef]
- Ahn, H.K.; Choi, J.Y.; Kim, K.M.; Kim, H.; Choi, S.H.; Park, S.H.; Park, J.O.; Lim, H.Y.; Kang, W.K.; Lee, J.; et al. Phase ii study of pazopanib monotherapy in metastatic gastroenteropancreatic neuroendocrine tumours. Br. J. Cancer 2013, 109, 1414–1419. [Google Scholar] [CrossRef]
- Jhaveri, K.; Esteva, F.J. Pertuzumab in the treatment of her2+ breast cancer. J. Natl. Compr. Cancer Netw. Jnccn 2014, 12, 591–598. [Google Scholar] [CrossRef]
- Sampedro-Nunez, M.; Luque, R.M.; Ramos-Levi, A.M.; Gahete, M.D.; Serrano-Somavilla, A.; Villa-Osaba, A.; Adrados, M.; Ibanez-Costa, A.; Martin-Perez, E.; Culler, M.D.; et al. Presence of sst5tmd4, a truncated splice variant of the somatostatin receptor subtype 5, is associated to features of increased aggressiveness in pancreatic neuroendocrine tumors. Oncotarget 2016, 7, 6593–6608. [Google Scholar] [CrossRef] [PubMed]
- Lamberts, S.W.; van der Lely, A.J.; de Herder, W.W.; Hofland, L.J. Octreotide. N. Engl. J. Med. 1996, 334, 246–254. [Google Scholar] [CrossRef]
- Caplin, M.E.; Pavel, M.; Cwikla, J.B.; Phan, A.T.; Raderer, M.; Sedlackova, E.; Cadiot, G.; Wolin, E.M.; Capdevila, J.; Wall, L.; et al. Lanreotide in metastatic enteropancreatic neuroendocrine tumors. N. Engl. J. Med. 2014, 371, 224–233. [Google Scholar] [CrossRef] [PubMed]
- Rinke, A.; Muller, H.H.; Schade-Brittinger, C.; Klose, K.J.; Barth, P.; Wied, M.; Mayer, C.; Aminossadati, B.; Pape, U.F.; Blaker, M.; et al. Placebo-controlled, double-blind, prospective, randomized study on the effect of octreotide lar in the control of tumor growth in patients with metastatic neuroendocrine midgut tumors: A report from the promid study group. J. Clin. Oncol. 2009, 27, 4656–4663. [Google Scholar] [CrossRef]
- Taylor, S.M.; Nevis, K.R.; Park, H.L.; Rogers, G.C.; Rogers, S.L.; Cook, J.G.; Bautch, V.L. Angiogenic factor signaling regulates centrosome duplication in endothelial cells of developing blood vessels. Blood 2010, 116, 3108–3117. [Google Scholar] [CrossRef]
- Winkler, F.; Kozin, S.V.; Tong, R.T.; Chae, S.S.; Booth, M.F.; Garkavtsev, I.; Xu, L.; Hicklin, D.J.; Fukumura, D.; di Tomaso, E.; et al. Kinetics of vascular normalization by vegfr2 blockade governs brain tumor response to radiation: Role of oxygenation, angiopoietin-1, and matrix metalloproteinases. Cancer Cell 2004, 6, 553–563. [Google Scholar]
- Maes, H.; Olmeda, D.; Soengas, M.S.; Agostinis, P. Vesicular trafficking mechanisms in endothelial cells as modulators of the tumor vasculature and targets of antiangiogenic therapies. FEBS J. 2016, 283, 25–38. [Google Scholar] [CrossRef]
- Van Dusseldorp, M. Health aspects of sweets and other snack foods. Ned. Tijdschr. Voor Tandheelkd. 1990, 97, 23–26. [Google Scholar]
- Nagathihalli, N.S.; Castellanos, J.A.; Shi, C.; Beesetty, Y.; Reyzer, M.L.; Caprioli, R.; Chen, X.; Walsh, A.J.; Skala, M.C.; Moses, H.L.; et al. Signal transducer and activator of transcription 3, mediated remodeling of the tumor microenvironment results in enhanced tumor drug delivery in a mouse model of pancreatic cancer. Gastroenterology 2015, 149, 1932–1943. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, J.I.; Shields, D.J.; Barillas, S.G.; Acevedo, L.M.; Murphy, E.; Huang, J.; Scheppke, L.; Stockmann, C.; Johnson, R.S.; Angle, N.; et al. A role for VEGF as a negative regulator of pericyte function and vessel maturation. Nature 2008, 456, 809–813. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Tobacco, Cigar and Pipe Use | 20–30% of pancreatic cancers are caused by smoking. |
| Overweight and obesity | |
| Diet | Higher in red and processed meats and lower in fruits and vegetables. |
| Lack of physical activity | |
| Workplace exposure to chemicals | Chemicals used in the dry cleaning and metal working industries. |
| Age | Risk goes up as people age. |
| Gender | Men. |
| Race | African Americans more likely to develop than white. |
| Blood group | People with blood groups A, AB and B have a higher risk. |
| Family history | |
| Inherited genetic syndromes | Hereditary pancreatitis, Peutz-Jeghers syndrome, Familial malignant melanoma and pancreatic cancer, Hereditary breast and ovarian cancer syndrome, Lynch syndrome, Li-Fraumeni syndrome, Familial adenomatous polyposis. |
| Type 2 Diabetes | |
| Chronic pancreatitis | |
| Cirrhosis of the liver | |
| Gastric ulcer | Helicobacter pylori related. |
| Drugs Targeting Growth Factor- and Growth Factor Receptor Inhibitors | Drug Target/Mechanism of Action | Pre-Clinical/Clinical Studies | Evaluated in PDAC/PNETs |
|---|---|---|---|
| Axitinib [53] | Selective inhibitor of VEGFR 1–3 | Clinical | PDAC |
| Bevacizumab [54,55] | Humanized anti-VEGF monoclonal antibody | Clinical | PDAC |
| Nintedanib [56,57] | Triple angiokinase inhibitor that targets VEGFR 1–3. FGFR 1–3 and PDGFRα/β | Pre-clinical | PDAC and PNETs |
| Sorafenib [58,59] | Small molecule inhibitor of Raf kinase, PDGF, VEGFR 2–3 and c-kit | Clinical | PDAC |
| Sunitinib [60,61,62,63,64] | Multitargeted tyrosine kinase inhibitor that targets VEGFR1-3, PDGFR, c-kit, RET, stem-cell factor receptor and FMS-like tyrosine kinase-3 | Pre-clinical and Clinical | PDAC and PNETs |
| Pazopanib [65] | Multitargeted tyrosine kinase inhibitor that targets VEGFR, PDGFR and c-kit | Clinical | PNETs |
| Pertuzumab [66] | Humanized anti-HER2-receptor | Clinical | PNETs |
| Drugs targeting the tumor stroma | |||
| Liposomal Clodronate [67,68] | Arrest tumor progression and angiogenesis | Pre-clinical | PNETs |
| Nitrogen-containing bisphosphonates (NBPs) [69] | Inhibit PSCs proliferation and activation, the release of MCP-1, type I collagen expression | Pre-clinical | PDAC |
| Drugs targeting cancer stem cells | |||
| DEspR [70] | DEspR-inhibition decrease angiogenesis, invasiveness, CSCs-survival and anoikis resistance | Pre-clinical | PDAC |
| Endostar [71] | Inhibit endothelial proliferation | Clinical | PNETs |
| Drugs targeting immune-cells | |||
| Anti-PD-L1 [72] | Promote lymphocyte infiltration and activity through activation of LTβR signalling | Pre-clinical | PNETs |
| Elpamotide [73] | Induce CTLs to kill VEGFR2-expressing endothelial cells | Clinical | PDAC |
| Drugs targeting other molecules or pathways | |||
| Benzofuran 90 [74] | Suppress p53-indipendent tumor cells through inhibition of HIF-1 pathway. Inhibits tumor angiogenesis downregulating Ang-2 through inhibition of YAP activity, and suppress VM downregulating MMP2, VE-cadherin and α-SMA expression | Pre-clinical | PDAC |
| Everolimus [75] | Selective inhibitor of mTOR downstream signalling | Clinical | PDAC |
| IkBα-SR [76] | Inhibit NF-κB pathway | Pre-clinical | PDAC |
| miR21 [61] | Decrease cell viability | Pre-clinical | PDAC |
| Octreotide [77] | Synthetic somatostatin analogues that inhibit hormonal secretion | Clinical | PNETs |
| Radiopeptide anti-GLP-1R [78] | Target beta-cells with radiopepetide | Pre-clinical | PNETs |
| Verteporfin [79,80] | Arrest cell-cycle and induce apoptosis targeting Hippo pathway | Pre-clinical | PDAC |
| Drug’s Name | Sample Size | Combined Regimens | Response Rate | Objective Response Rate | Overall Survival (Months) | Progression Free Survival (Months) | Median Survival Time | Didease Control Rate | Time to Progression |
|---|---|---|---|---|---|---|---|---|---|
| Sorafenib [58] | 71 | Gemcitabine plus or not Sorafenib in patients with LDH values under or above the cut-off | 10.7 vs. 5.9 | 5.2 vs. 2.7 | |||||
| Elpamotide [73] | 153 | Gemcitabine plus or not Elpamotide | No significative | 3.71 vs. 3.75 | 8.36 vs. 8.54 | 59.6% vs. 60.4% | |||
| Everolimus [75] | 27 | Everolimus in combination with escalating low-dose gemcitabine | 13% | ||||||
| Sorafenib [59] | 25 | Gemcitabine-based chemoradion therapy plus or not Sorafenib | 12.6 in evaluable patients; 11.5 in intent to treat patients; 21.6 in patients with VEGF-A -2578 AA, -1498 CC genotypes; 14.7 in patients with VEGF-A -1154 AA genotype | 10.6 in evaluable patients; 9.9 in intent to treat patients | 10.7 in evaluable and in intent to treat patients | ||||
| Bevacizumab [116] | 163 | Gemcitabine plus Bevacizumab in patient with related hypertension (B-HTN) or not | 47% vs. 16% | 13.1 vs. 8.1 | 85% vs. 59% | ||||
| Endostar [71] | 14 | Endostar and Temozolomide or Dacarbazine plus 5-fluorouracil | 46% | 33% vs. 50% in no therapy vs. prior therapy | Not reached | 12 | |||
| Sunitinib [64] | 26 | Sunitinib after different chemotherapy protocols | 58% | 6.0 | 1.4 | ||||
| Pazopanib [65] | 44 | Pazopanib | 24.1 | 9.5 | |||||
| Octreotide [77] | 427 | Octreotide vs. Octreotide plus Bevacizumab or interferon alfa-2b | 12% in Bevacizumab arm; 4% in interferon alfa-2b arm | No significative | 16.6 in Bevacizumab arm; 15.4 in interferon alfa-2b arm | ||||
| Pertuzumab [66] | 43 | Bevacizumab, Pertuzumab and Octreotide | 16% | 26.4 | 6.5 | ||||
| sst5TMD4 [124] | 42 | Study designed to focus on functional roles of somatostatin receptors |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Annese, T.; Tamma, R.; Ruggieri, S.; Ribatti, D. Angiogenesis in Pancreatic Cancer: Pre-Clinical and Clinical Studies. Cancers 2019, 11, 381. https://doi.org/10.3390/cancers11030381
Annese T, Tamma R, Ruggieri S, Ribatti D. Angiogenesis in Pancreatic Cancer: Pre-Clinical and Clinical Studies. Cancers. 2019; 11(3):381. https://doi.org/10.3390/cancers11030381
Chicago/Turabian StyleAnnese, Tiziana, Roberto Tamma, Simona Ruggieri, and Domenico Ribatti. 2019. "Angiogenesis in Pancreatic Cancer: Pre-Clinical and Clinical Studies" Cancers 11, no. 3: 381. https://doi.org/10.3390/cancers11030381
APA StyleAnnese, T., Tamma, R., Ruggieri, S., & Ribatti, D. (2019). Angiogenesis in Pancreatic Cancer: Pre-Clinical and Clinical Studies. Cancers, 11(3), 381. https://doi.org/10.3390/cancers11030381