PD1/PD-L1 Expression in Blastic Plasmacytoid Dendritic Cell Neoplasm

 ,
,  ,
, 



Abstract
:1. Introduction
2. Results
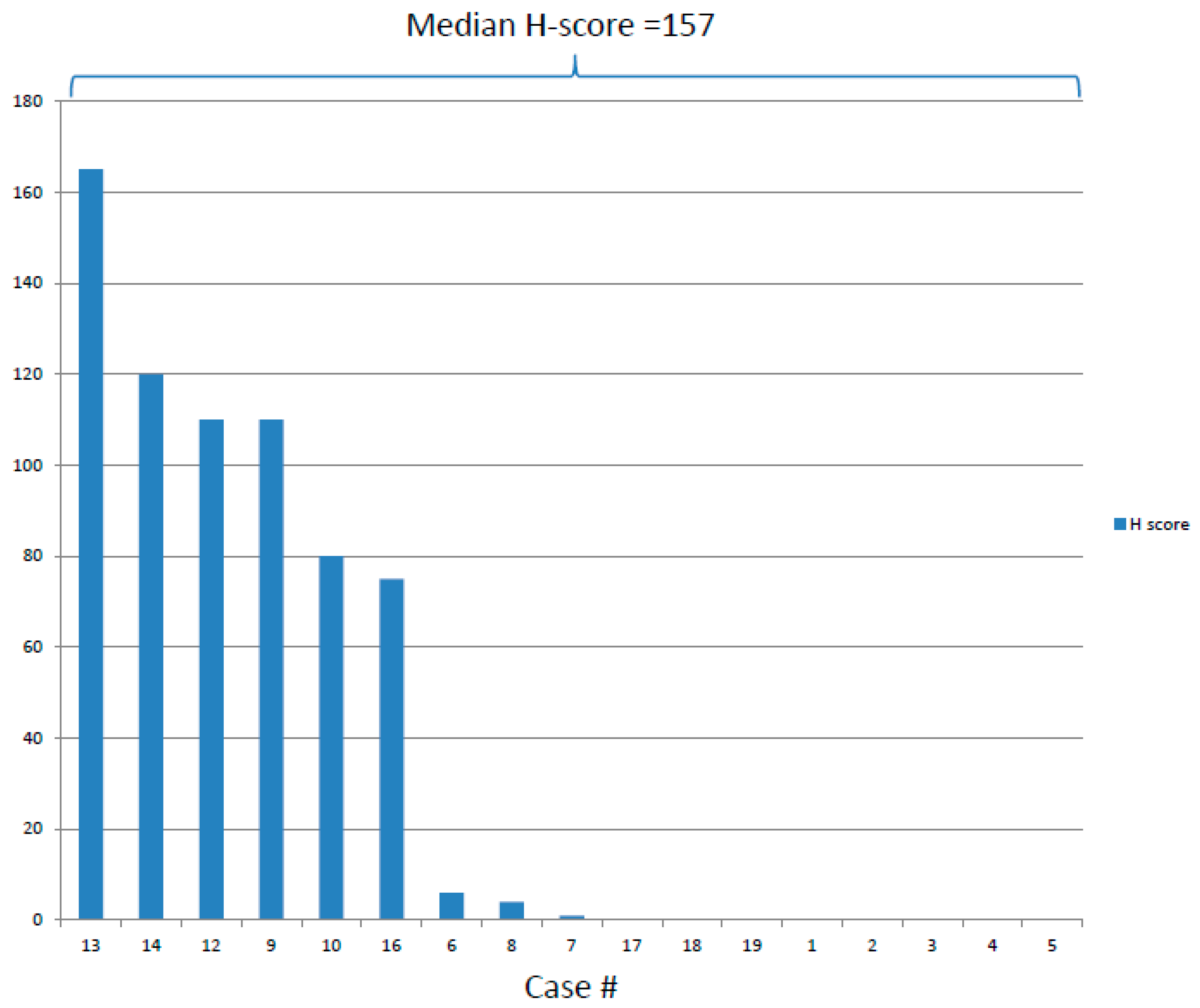
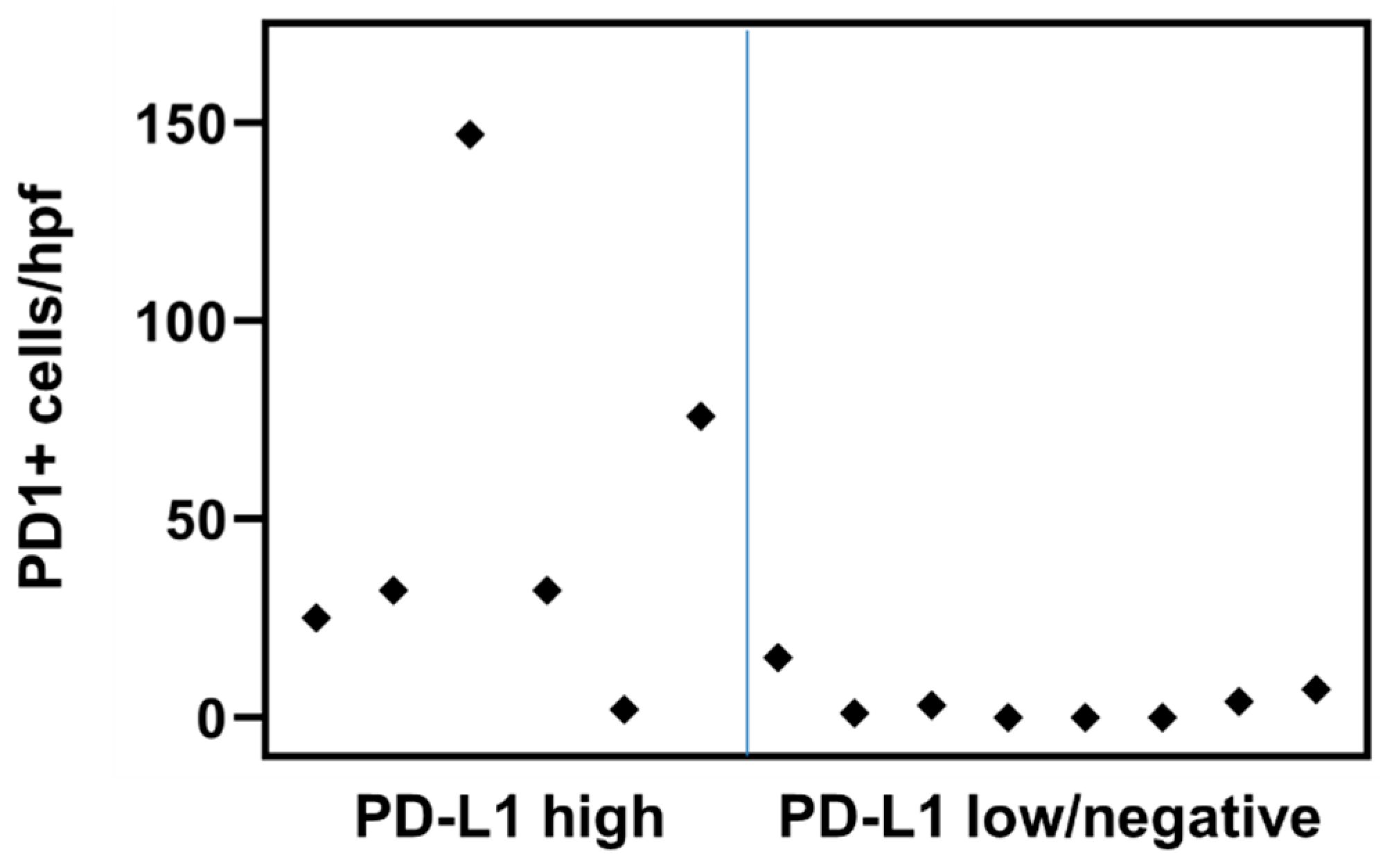
2.1. PD-L1 and PD1 Expression by Immunohistochemistry
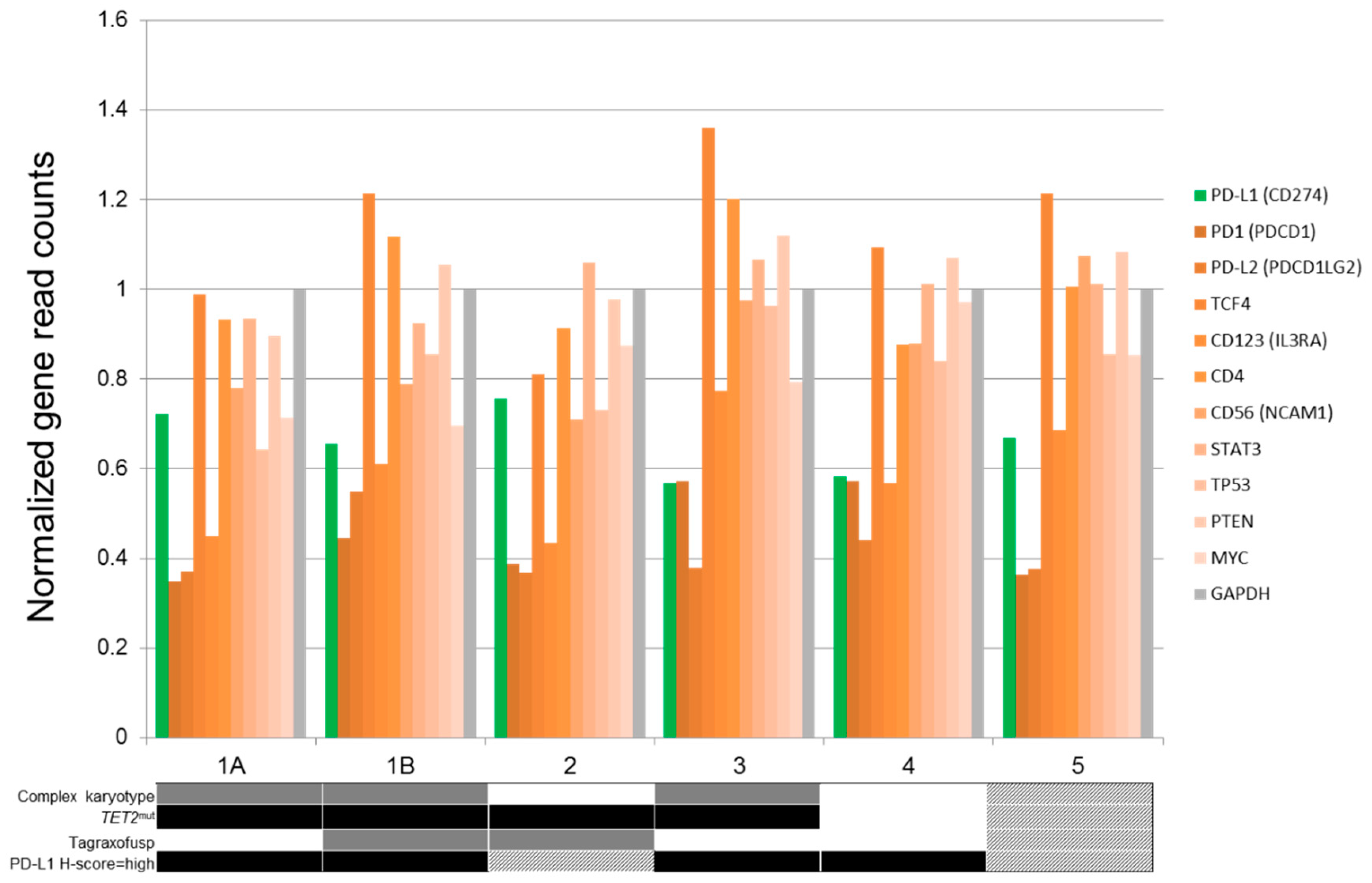
2.2. PD-L1 and PD1 Expression by RNAseq
2.3. Clinical and Molecular Correlates of PDL1 Expression
3. Discussion
4. Materials and Methods
4.1. Patient Group
4.2. Evaluation of PD1 and PD-L1 Expression by Immunohistochemistry
4.3. Molecular Analysis
4.4. Whole-Transcriptome RNA Sequencing
4.5. Conventional Cytogenetics
4.6. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Facchetti, F.; Ungari, M.; Marocolo, D.; Lonardi, S.; Vermi, W. Blastic Plasmacytoid Dendritic Cell Neoplasm. Curr. Hematol. Malig. Rep. 2018, 13, 477–483. [Google Scholar] [CrossRef]
- Guru Murthy, G.S.; Pemmaraju, N.; Atallah, E. Epidemiology and survival of blastic plasmacytoid dendritic cell neoplasm. Leuk. Res. 2018, 73, 21–23. [Google Scholar] [CrossRef] [PubMed]
- Kharfan-Dabaja, M.A.; Al Malki, M.M.; Deotare, U.; Raj, R.V.; El-Jurdi, N.; Majhail, N.; Cherry, M.A.; Bashir, Q.; Darrah, J.; Nishihori, T.; et al. Haematopoietic cell transplantation for blastic plasmacytoid dendritic cell neoplasm: A North American multicentre collaborative study. Br. J. Haematol. 2017, 179, 781–789. [Google Scholar] [CrossRef]
- Pemmaraju, N.; Lane, A.A.; Sweet, K.L.; Stein, A.S.; Vasu, S.; Blum, W.; Rizzieri, D.A.; Wang, E.S.; Duvic, M.; Sloan, J.M.; et al. Tagraxofusp in Blastic Plasmacytoid Dendritic-Cell Neoplasm. N. Engl. J. Med. 2019, 380, 1628–1637. [Google Scholar] [CrossRef]
- Keenan, T.E.; Burke, K.P.; Van Allen, E.M. Genomic correlates of response to immune checkpoint blockade. Nat. Med. 2019, 25, 389–402. [Google Scholar] [CrossRef] [PubMed]
- Zerdes, I.; Matikas, A.; Bergh, J.; Rassidakis, G.Z.; Foukakis, T. Genetic, transcriptional and post-translational regulation of the programmed death protein ligand 1 in cancer: Biology and clinical correlations. Oncogene 2018, 37, 4639–4661. [Google Scholar] [CrossRef]
- Sun, C.; Mezzadra, R.; Schumacher, T.N. Regulation and Function of the PD-L1 Checkpoint. Immunity 2018, 48, 434–452. [Google Scholar] [CrossRef] [PubMed]
- Sharpe, A.H.; Pauken, K.E. The diverse functions of the PD1 inhibitory pathway. Nat. Rev. Immunol. 2018, 18, 153–167. [Google Scholar] [CrossRef] [PubMed]
- Metcalfe, W.; Anderson, J.; Trinh, V.A.; Hwu, W.J. Anti-programmed cell death-1 (PD-1) monoclonal antibodies in treating advanced melanoma. Discov. Med. 2015, 19, 393–401. [Google Scholar] [PubMed]
- Reck, M.; Rodriguez-Abreu, D.; Robinson, A.G.; Hui, R.; Csoszi, T.; Fulop, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Pembrolizumab versus Chemotherapy for PD-L1-Positive Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2016, 375, 1823–1833. [Google Scholar] [CrossRef] [PubMed]
- Herbst, R.S.; Baas, P.; Kim, D.W.; Felip, E.; Perez-Gracia, J.L.; Han, J.Y.; Molina, J.; Kim, J.H.; Arvis, C.D.; Ahn, M.J.; et al. Pembrolizumab versus docetaxel for previously treated, PD-L1-positive, advanced non-small-cell lung cancer (KEYNOTE-010): A randomised controlled trial. Lancet 2016, 387, 1540–1550. [Google Scholar] [CrossRef]
- Borghaei, H.; Paz-Ares, L.; Horn, L.; Spigel, D.R.; Steins, M.; Ready, N.E.; Chow, L.Q.; Vokes, E.E.; Felip, E.; Holgado, E.; et al. Nivolumab versus Docetaxel in Advanced Nonsquamous Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2015, 373, 1627–1639. [Google Scholar] [CrossRef] [PubMed]
- Brahmer, J.; Reckamp, K.L.; Baas, P.; Crino, L.; Eberhardt, W.E.; Poddubskaya, E.; Antonia, S.; Pluzanski, A.; Vokes, E.E.; Holgado, E.; et al. Nivolumab versus Docetaxel in Advanced Squamous-Cell Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2015, 373, 123–135. [Google Scholar] [CrossRef] [PubMed]
- Motzer, R.J.; Escudier, B.; McDermott, D.F.; George, S.; Hammers, H.J.; Srinivas, S.; Tykodi, S.S.; Sosman, J.A.; Procopio, G.; Plimack, E.R.; et al. Nivolumab versus Everolimus in Advanced Renal-Cell Carcinoma. N. Engl. J. Med. 2015, 373, 1803–1813. [Google Scholar] [CrossRef] [PubMed]
- Ansell, S.M.; Lesokhin, A.M.; Borrello, I.; Halwani, A.; Scott, E.C.; Gutierrez, M.; Schuster, S.J.; Millenson, M.M.; Cattry, D.; Freeman, G.J.; et al. PD-1 blockade with nivolumab in relapsed or refractory Hodgkin′s lymphoma. N. Engl. J. Med. 2015, 372, 311–319. [Google Scholar] [CrossRef] [PubMed]
- Topalian, S.L.; Hodi, F.S.; Brahmer, J.R.; Gettinger, S.N.; Smith, D.C.; McDermott, D.F.; Powderly, J.D.; Carvajal, R.D.; Sosman, J.A.; Atkins, M.B.; et al. Safety, activity, and immune correlates of anti-PD-1 antibody in cancer. N. Engl. J. Med. 2012, 366, 2443–2454. [Google Scholar] [CrossRef] [PubMed]
- Lantuejoul, S.; Damotte, D.; Hofman, V.; Adam, J. Programmed death ligand 1 immunohistochemistry in non-small cell lung carcinoma. J. Thorac. Dis. 2019, 11 (Suppl. 1), S89–S101. [Google Scholar] [CrossRef] [PubMed]
- Nishino, M.; Ramaiya, N.H.; Hatabu, H.; Hodi, F.S. Monitoring immune-checkpoint blockade: Response evaluation and biomarker development. Nat. Rev. Clin. Oncol. 2017, 14, 655–668. [Google Scholar] [CrossRef] [PubMed]
- Wu, P.; Wu, D.; Li, L.; Chai, Y.; Huang, J. PD-L1 and Survival in Solid Tumors: A Meta-Analysis. PLoS ONE 2015, 10, e0131403. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Teng, F.; Kong, L.; Yu, J. PD-L1 expression in human cancers and its association with clinical outcomes. OncoTargets Ther. 2016, 9, 5023–5039. [Google Scholar] [CrossRef] [Green Version]
- Pyo, J.S.; Kang, G.; Kim, J.Y. Prognostic role of PD-L1 in malignant solid tumors: A meta-analysis. Int. J. Biol. Markers 2017, 32, e68–e74. [Google Scholar] [CrossRef]
- Gandini, S.; Massi, D.; Mandala, M. PD-L1 expression in cancer patients receiving anti PD-1/PD-L1 antibodies: A systematic review and meta-analysis. Crit. Rev. Oncol. Hematol. 2016, 100, 88–98. [Google Scholar] [CrossRef]
- Sponaas, A.M.; Moharrami, N.N.; Feyzi, E.; Standal, T.; Holth Rustad, E.; Waage, A.; Sundan, A. PDL1 Expression on Plasma and Dendritic Cells in Myeloma Bone Marrow Suggests Benefit of Targeted anti PD1-PDL1 Therapy. PLoS ONE 2015, 10, e0139867. [Google Scholar] [CrossRef] [Green Version]
- Bourque, J.; Hawiger, D. Immunomodulatory Bonds of the Partnership between Dendritic Cells and T Cells. Crit. Rev. Immunol. 2018, 38, 379–401. [Google Scholar] [CrossRef]
- Pagano, L.; Valentini, C.G.; Pulsoni, A.; Fisogni, S.; Carluccio, P.; Mannelli, F.; Lunghi, M.; Pica, G.; Onida, F.; Cattaneo, C.; et al. Blastic plasmacytoid dendritic cell neoplasm with leukemic presentation: An Italian multicenter study. Haematologica 2013, 98, 239–246. [Google Scholar] [CrossRef] [PubMed]
- Herling, M.; Teitell, M.A.; Shen, R.R.; Medeiros, L.J.; Jones, D. TCL1 expression in plasmacytoid dendritic cells (DC2s) and the related CD4+ CD56+ blastic tumors of skin. Blood 2003, 101, 5007–5009. [Google Scholar] [CrossRef] [Green Version]
- Khoury, J.D.; Medeiros, L.J.; Manning, J.T.; Sulak, L.E.; Bueso-Ramos, C.; Jones, D. CD56(+) TdT(+) blastic natural killer cell tumor of the skin: A primitive systemic malignancy related to myelomonocytic leukemia. Cancer 2002, 94, 2401–2408. [Google Scholar] [CrossRef] [PubMed]
- Leroux, D.; Mugneret, F.; Callanan, M.; Radford-Weiss, I.; Dastugue, N.; Feuillard, J.; Le Mee, F.; Plessis, G.; Talmant, P.; Gachard, N.; et al. CD4(+), CD56(+) DC2 acute leukemia is characterized by recurrent clonal chromosomal changes affecting 6 major targets: A study of 21 cases by the Groupe Francais de Cytogenetique Hematologique. Blood 2002, 99, 4154–4159. [Google Scholar] [CrossRef]
- Tsagarakis, N.J.; Kentrou, N.A.; Papadimitriou, K.A.; Pagoni, M.; Kokkini, G.; Papadaki, H.; Pappa, V.; Marinakis, T.; Anagnostopoulos, N.I.; Vadikolia, C.; et al. Acute lymphoplasmacytoid dendritic cell (DC2) leukemia: Results from the Hellenic Dendritic Cell Leukemia Study Group. Leuk. Res. 2010, 34, 438–446. [Google Scholar] [CrossRef]
- Frankel, A.E.; Woo, J.H.; Ahn, C.; Pemmaraju, N.; Medeiros, B.C.; Carraway, H.E.; Frankfurt, O.; Forman, S.J.; Yang, X.A.; Konopleva, M.; et al. Activity of SL-401, a targeted therapy directed to interleukin-3 receptor, in blastic plasmacytoid dendritic cell neoplasm patients. Blood 2014, 124, 385–392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jelinek, T.; Paiva, B.; Hajek, R. Update on PD-1/PD-L1 Inhibitors in Multiple Myeloma. Front. Immunol. 2018, 9, 2431. [Google Scholar] [CrossRef] [PubMed]
- Facchetti, F.; Petrella, T.; Pileri, S.A. Blastic plasmacytoid dendritic cell neoplasm. In WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues; Swerdlow, S.H., Campo, E., Harris, N.L., Jaffe, E.S., Pileri, S.A., Stein, H., Thiele, J., Eds.; IARC: Lyon, France, 2017; pp. 174–177. [Google Scholar]
- Alayed, K.; Patel, K.P.; Konoplev, S.; Singh, R.R.; Routbort, M.J.; Reddy, N.; Pemmaraju, N.; Zhang, L.; Shaikh, A.A.; Aladily, T.N.; et al. TET2 mutations, myelodysplastic features, and a distinct immunoprofile characterize blastic plasmacytoid dendritic cell neoplasm in the bone marrow. Am. J. Hematol. 2013, 88, 1055–1061. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khoury, J.D.; Wang, W.L.; Prieto, V.G.; Medeiros, L.J.; Kalhor, N.; Hameed, M.; Broaddus, R.; Hamilton, S.R. Validation of Immunohistochemical Assays for Integral Biomarkers in the NCI-MATCH EAY131 Clinical Trial. Clin. Cancer Res. 2018, 24, 521–531. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Singh, R.R.; Patel, K.P.; Stingo, F.; Routbort, M.; You, M.J.; Miranda, R.N.; Garcia-Manero, G.; Kantarjian, H.M.; Medeiros, L.J.; et al. BRAF kinase domain mutations are present in a subset of chronic myelomonocytic leukemia with wild-type RAS. Am. J. Hematol. 2014, 89, 499–504. [Google Scholar] [CrossRef] [PubMed]
- Khoury, J.D.; Sen, F.; Abruzzo, L.V.; Hayes, K.; Glassman, A.; Medeiros, L.J. Cytogenetic findings in blastoid mantle cell lymphoma. Hum. Pathol. 2003, 34, 1022–1029. [Google Scholar] [CrossRef]
- McGowan-Jordan, J.; Simons, A.; Schmid, M. (Eds.) ISCN 2016: An. International System for Human Cytogenomic Nomenclature (2016); S. Karger Publishing: Basel, Switzerland, 2016. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Entire Group | PD-L1 Positive | PD-L1 Negative | P-Value |
|---|---|---|---|---|
| N (%) | 28 | 10/21 (47.6) | 11/21 (52.4) | |
| Age in years, median (range) | 66.8 (22.8–86.7) | 66.2 (28.7–87) | 65.2 (38.5–84.7) | 0.860 |
| Sex, N (%) | 0.635 | |||
| Female | 6 (21.4) | 3 | 2 | |
| Male | 22 (78.6) | 7 | 9 | |
| Anatomic location at diagnosis, N (%) | 0.643 | |||
| Skin | 23 (81.2) | 9 | 9 | |
| Bone marrow | 19 (67.8) | 5 | 9 | |
| Lymph node | 8 (28.6) | 2 | 4 | |
| Peripheral blood parameters | ||||
| White blood count (× 109/L), median (range) | 5.3 (1.7–76.5) | 7.1 (2.0–76.5) | 5.1 (2.4–13.3) | 0.260 |
| Hemoglobin concentration (g/dL), median(range) | 12.2 (6.8–17.0) | 12.1 (8.7–14.6) | 13.1 (6.8–16.2) | 0.622 |
| Platelet count (× 109/L), median(range) | 147.5 (22–396) | 178 (53–396) | 183 (22–294) | 0.888 |
| Bone marrow blast percentage, median (range) | 30 (4–100) | 40 (14–70) | 47 (5–95) | 0.648 |
| Cytogenetics, N (%) * | 0.065 | |||
| Diploid | 8/19 (42.1%) | 3/5 | 1/6 | |
| Complex | 7/19 (36.8%) | 1/5 | 5/6 | |
| Mutations, present, N (%) | 1.000 | |||
| TET2 | 7/17 (41.2) | 4 | 2 | |
| ASXL1 | 2 (11.8) | 0 | 0 | |
| TET2 + ASXL1 | 6 (35.3) | 4 | 1 | |
| Other | 2 (11.8) | 0 | 0 | |
| PD1 #/high-power field, median (range) | 4.5 (0–147) | 14 (2–48) | 18 (4–66) | 0.123 |
| Tagraxofusp (SL-401) therapy, N (%) | 15/21 (71.4) | 9/15 (60) | 6/15 (40) | 0.526 |
| Stem cell therapy, N (%) | 12/20 (60) | 6/10 (60) | 6/10 (60) | 1.000 |
| Follow up duration in months, median (range) | 12 (2–66) | 14 (2–48) | 18 (4–66) | 0.621 |
| Death, N (%) | 19 (67.9) | 5/10 (50) | 9/11 (81.8) | 0.183 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aung, P.P.; Sukswai, N.; Nejati, R.; Loghavi, S.; Chen, W.; Torres-Cabala, C.A.; Yin, C.C.; Konopleva, M.; Zheng, X.; Wang, J.; et al. PD1/PD-L1 Expression in Blastic Plasmacytoid Dendritic Cell Neoplasm. Cancers 2019, 11, 695. https://doi.org/10.3390/cancers11050695
Aung PP, Sukswai N, Nejati R, Loghavi S, Chen W, Torres-Cabala CA, Yin CC, Konopleva M, Zheng X, Wang J, et al. PD1/PD-L1 Expression in Blastic Plasmacytoid Dendritic Cell Neoplasm. Cancers. 2019; 11(5):695. https://doi.org/10.3390/cancers11050695
Chicago/Turabian StyleAung, Phyu P., Narittee Sukswai, Reza Nejati, Sanam Loghavi, Weina Chen, Carlos A. Torres-Cabala, C. Cameron Yin, Marina Konopleva, Xiaofeng Zheng, Jing Wang, and et al. 2019. "PD1/PD-L1 Expression in Blastic Plasmacytoid Dendritic Cell Neoplasm" Cancers 11, no. 5: 695. https://doi.org/10.3390/cancers11050695
APA StyleAung, P. P., Sukswai, N., Nejati, R., Loghavi, S., Chen, W., Torres-Cabala, C. A., Yin, C. C., Konopleva, M., Zheng, X., Wang, J., Tang, Z., Medeiros, L. J., Prieto, V. G., Pemmaraju, N., & Khoury, J. D. (2019). PD1/PD-L1 Expression in Blastic Plasmacytoid Dendritic Cell Neoplasm. Cancers, 11(5), 695. https://doi.org/10.3390/cancers11050695