Acute Skin Damage and Late Radiation-Induced Fibrosis and Inflammation in Murine Ears after High-Dose Irradiation

 ,
, 

Abstract
:1. Introduction
2. Results
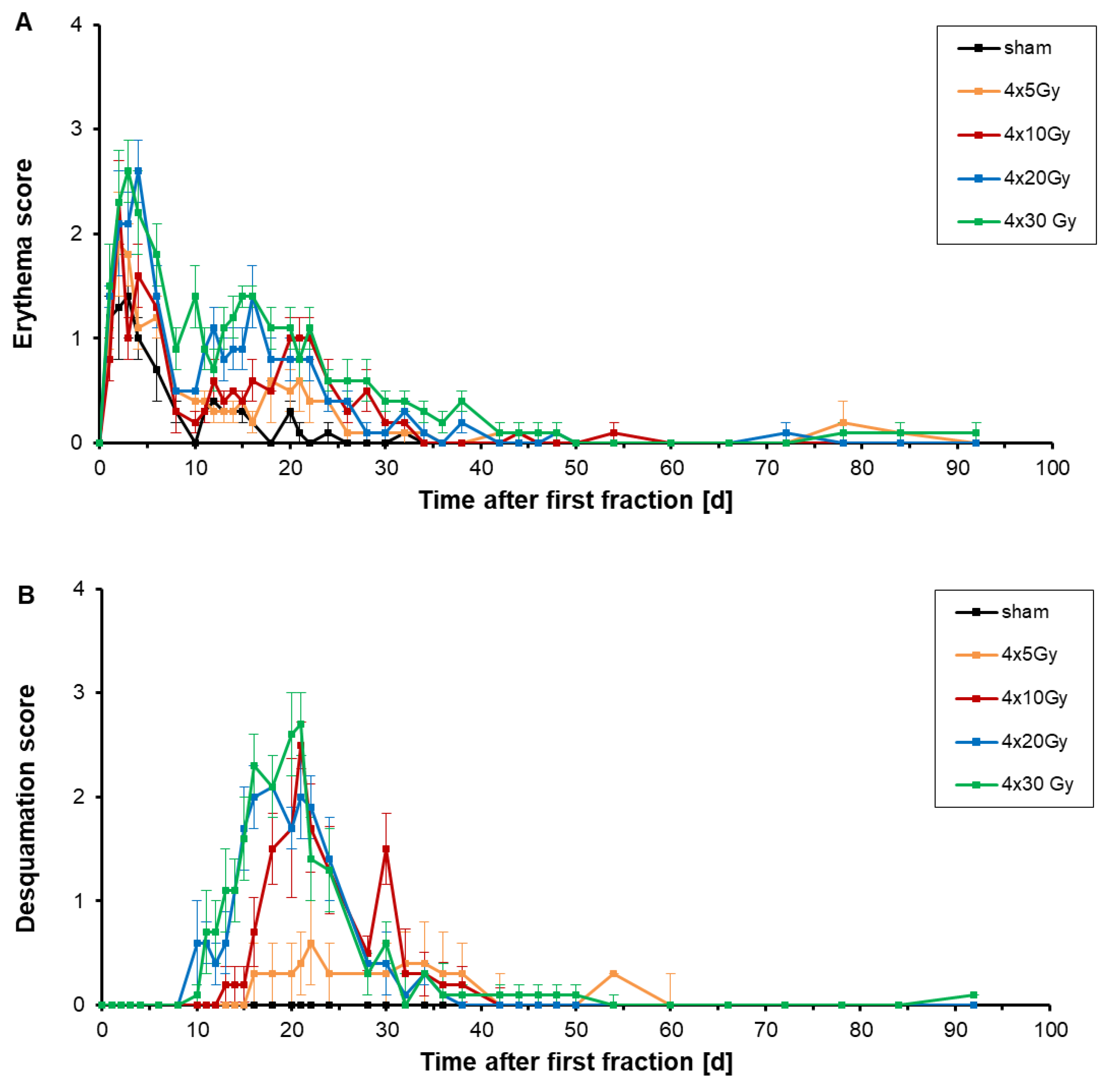
2.1. Analysis of Erythema and Desquamation
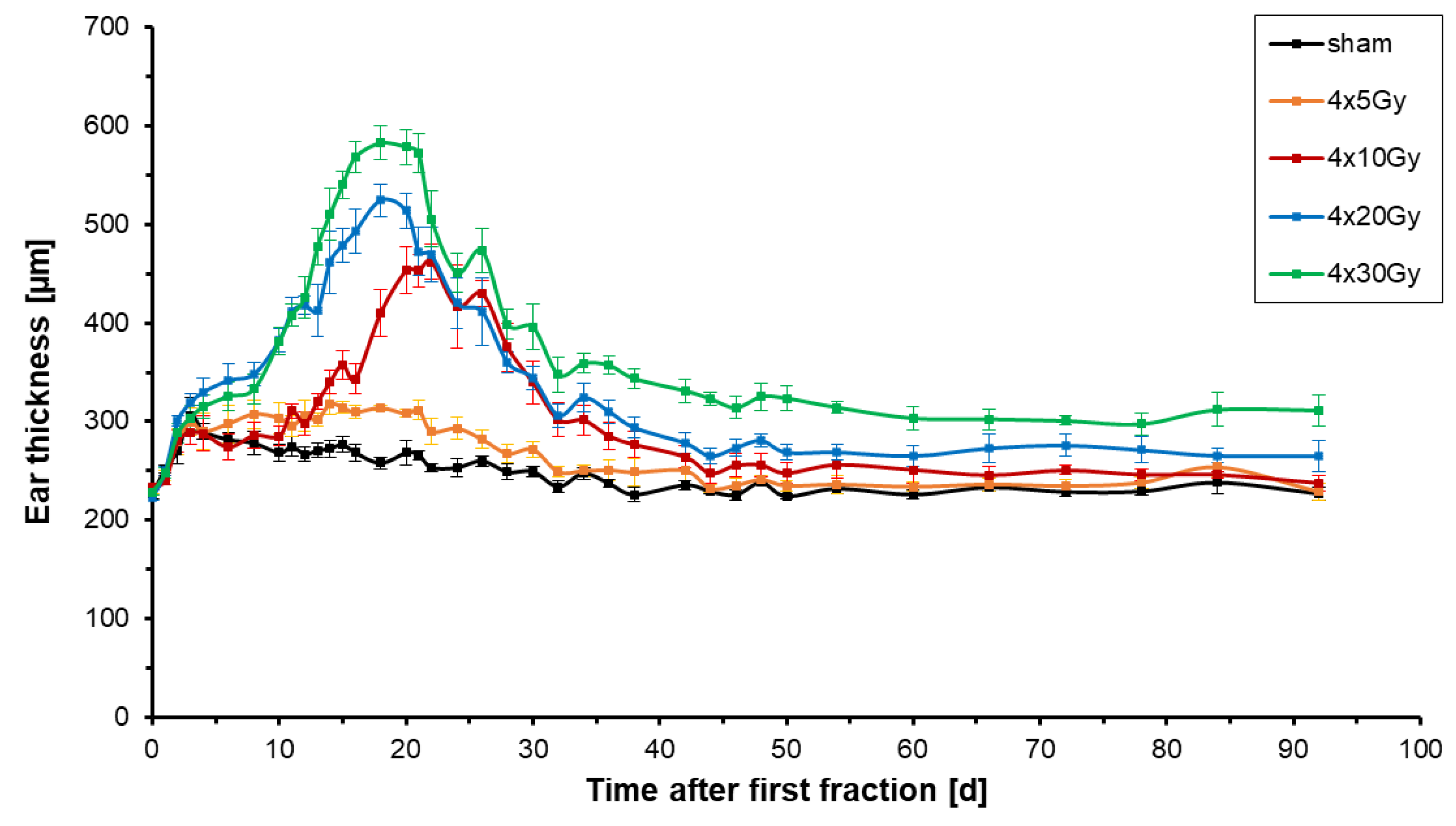
2.2. Analysis of Ear Thickness
2.3. Dose-Dependency of the Maximum Ear Thickness, the Maximum Erythema and Desquamation Score
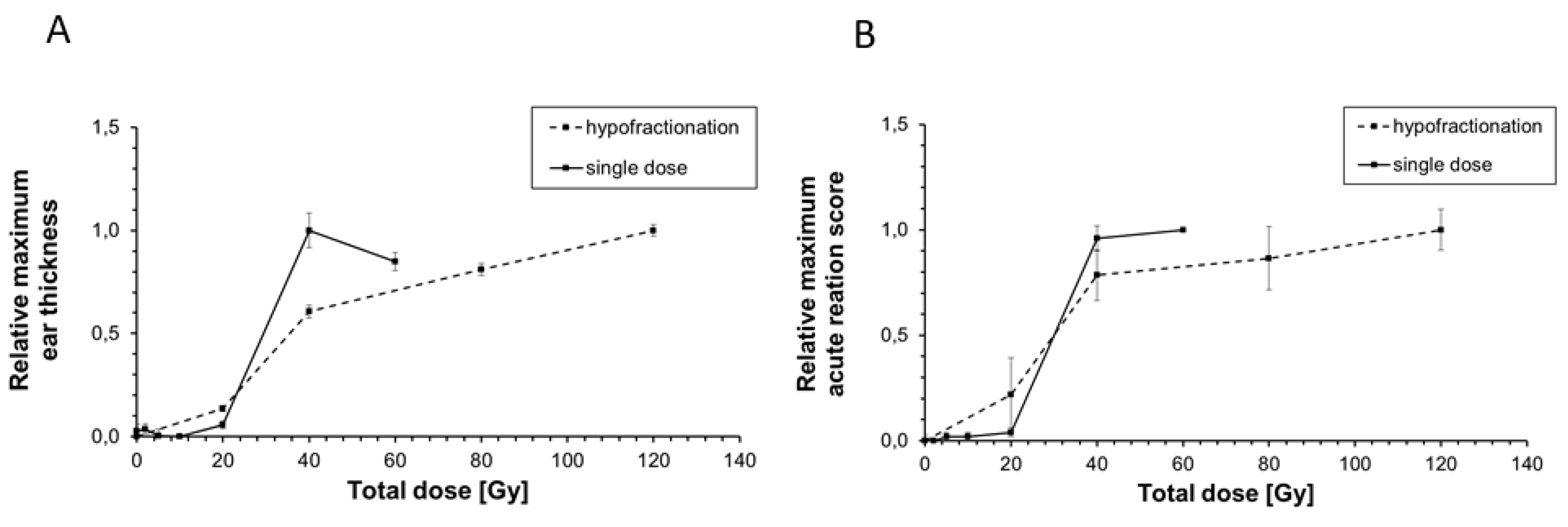
2.4. Comparison of the Maximum Acute Reaction Score and the Maximum Ear Thickness between Hypofractionated and Single X-ray Dose Irradiation
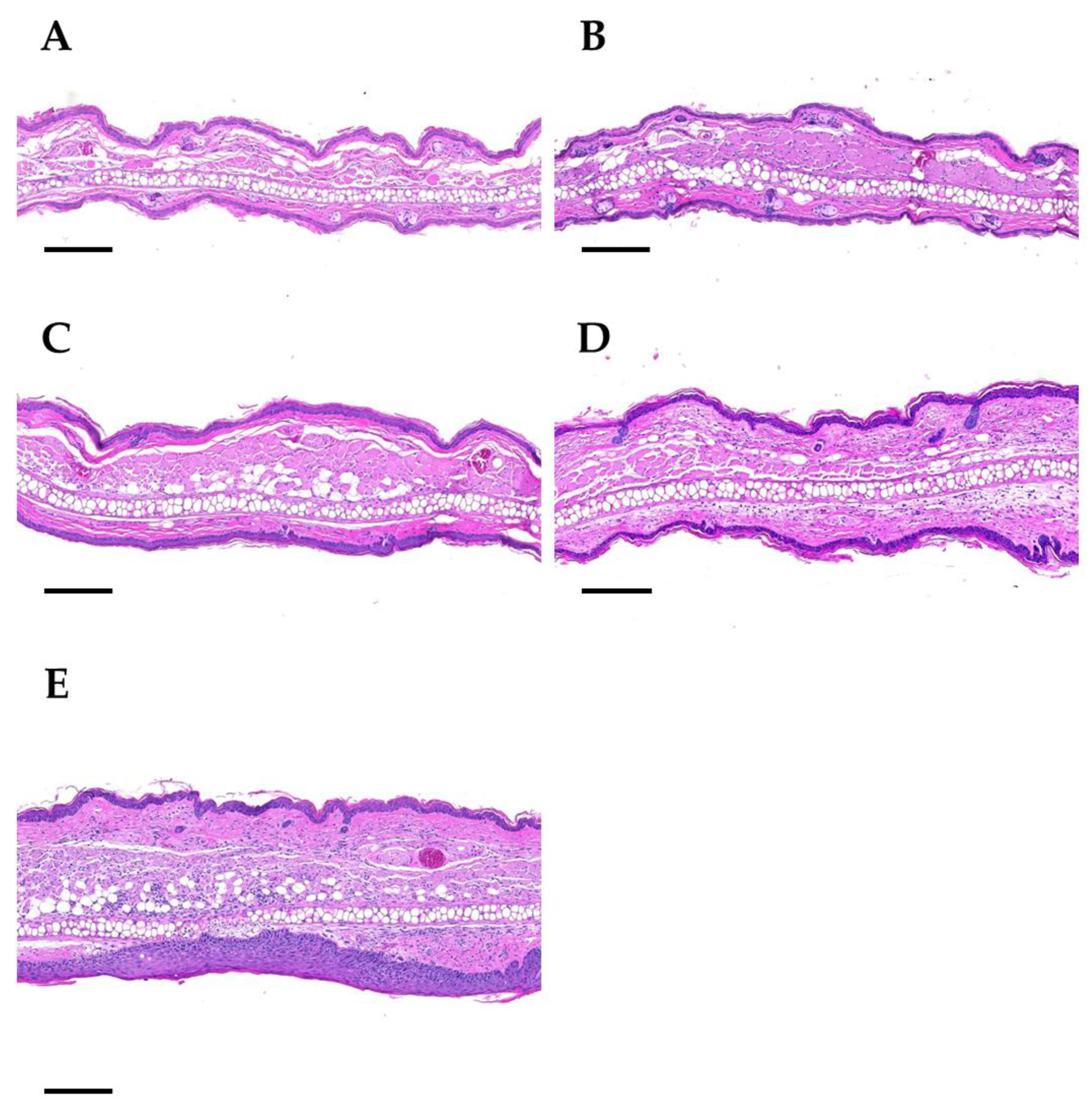
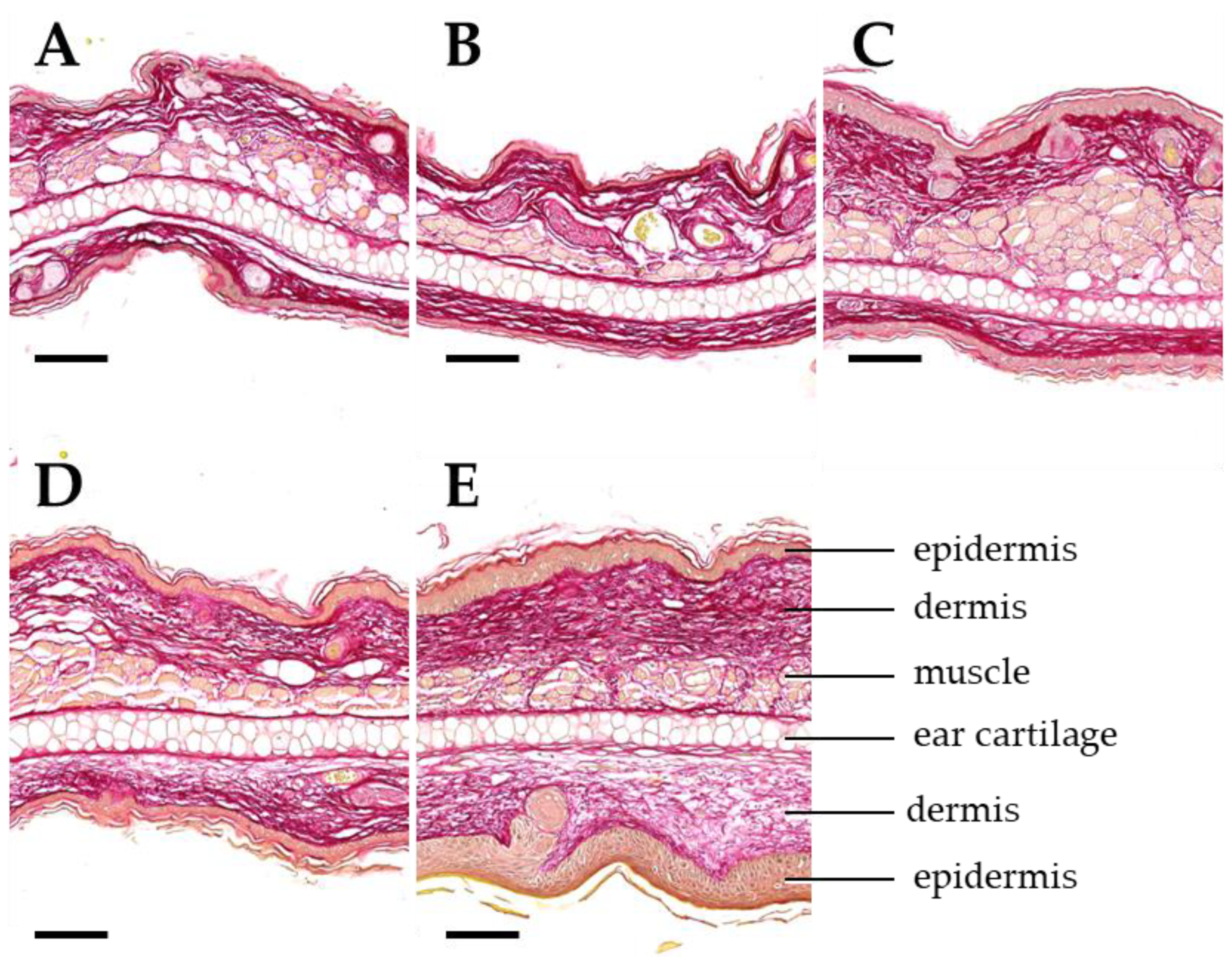
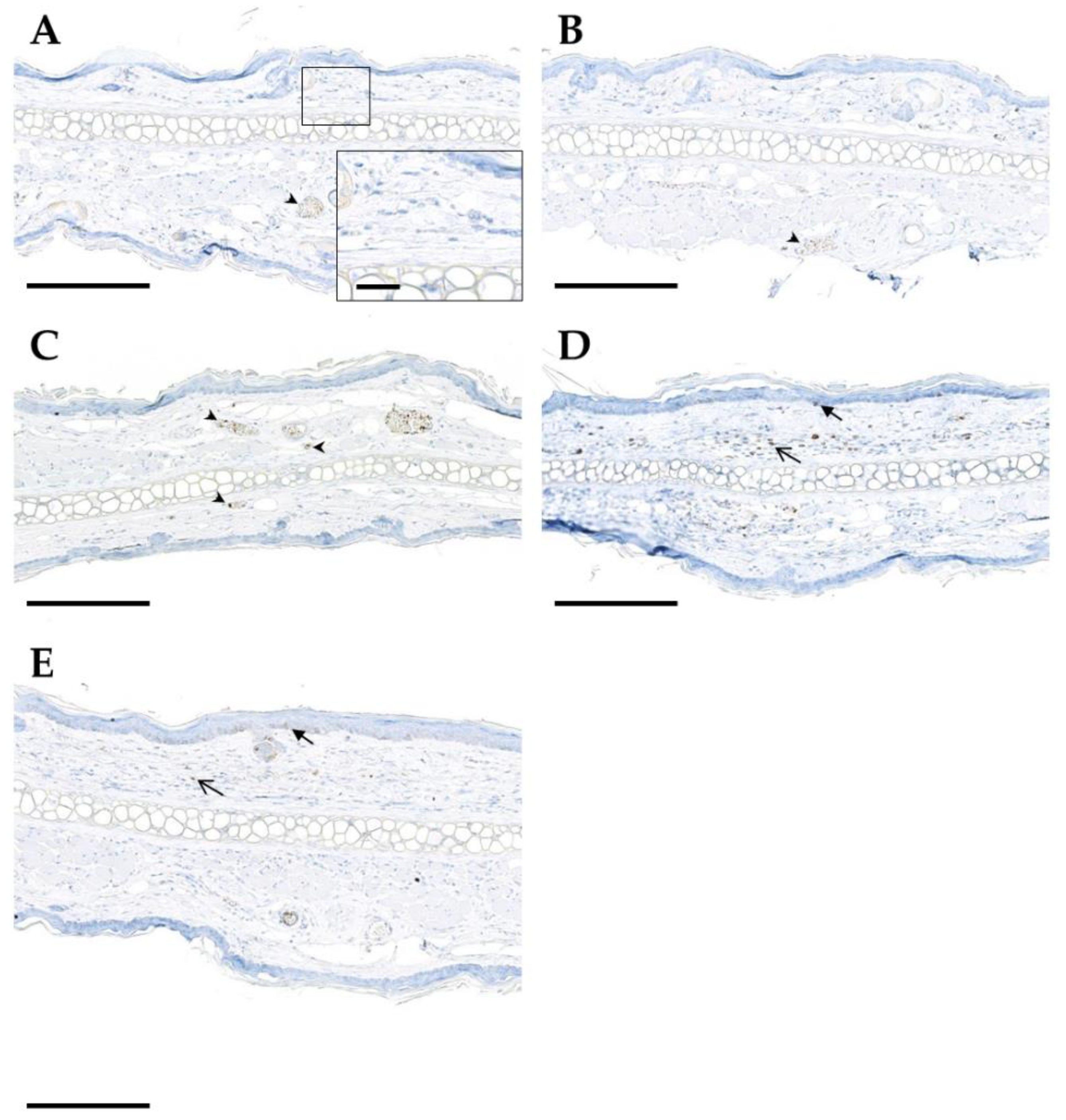
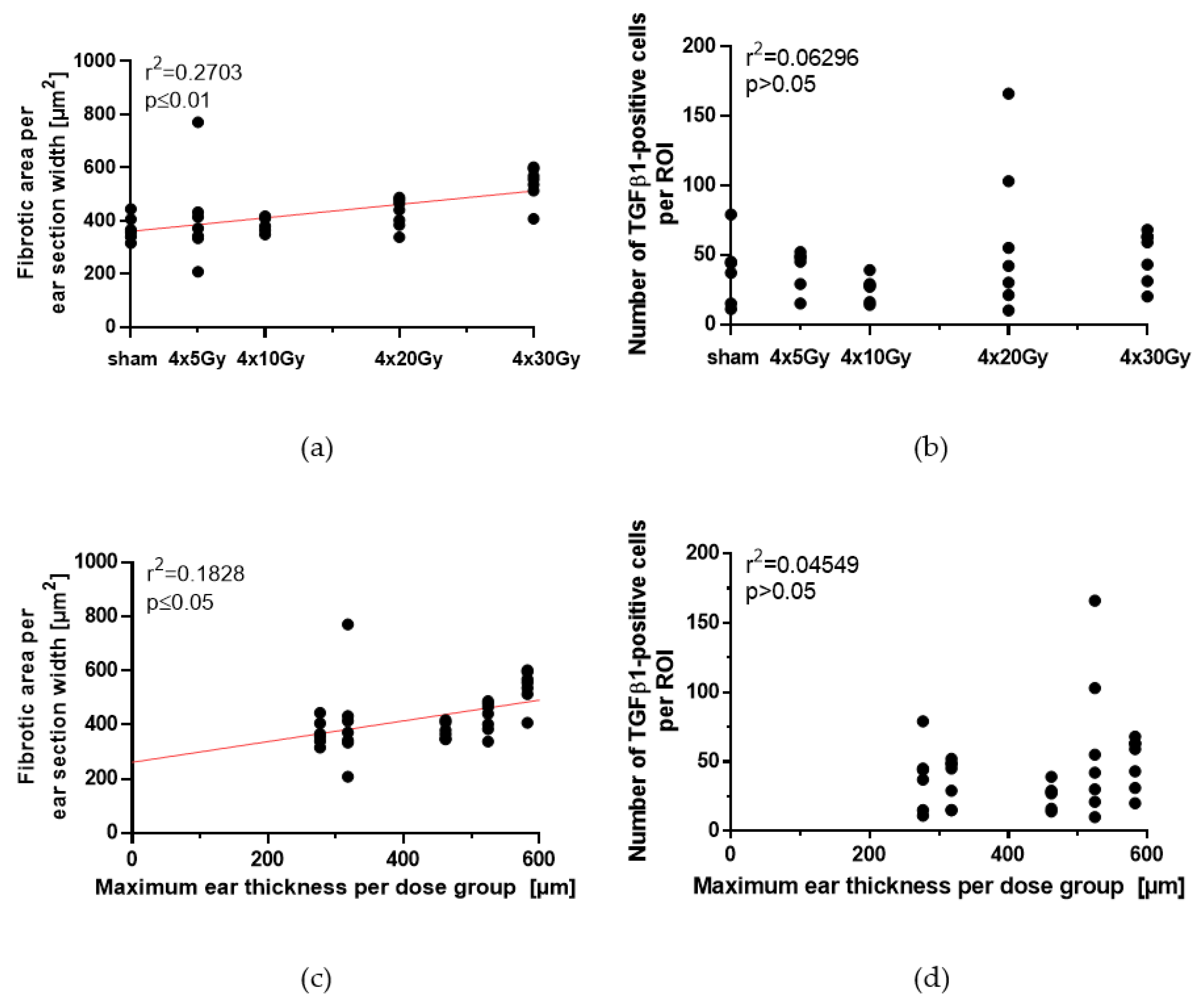
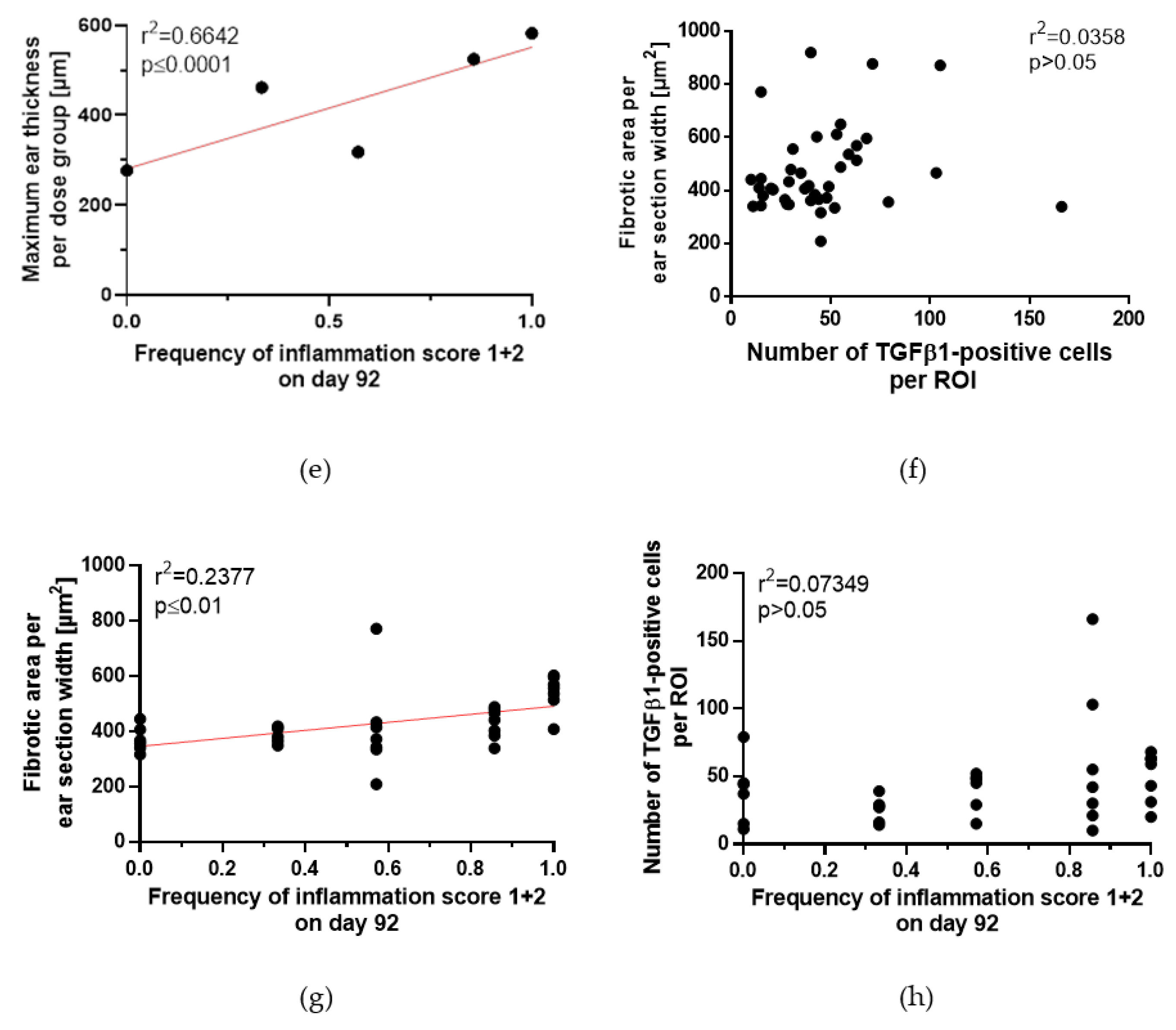
2.5. Histopathological Analyses of Irradiated Ears
2.6. Correlation of Acute and Late Side Effects after Hypofractionation
3. Discussion
4. Material and Methods
4.1. Ear Irradiation
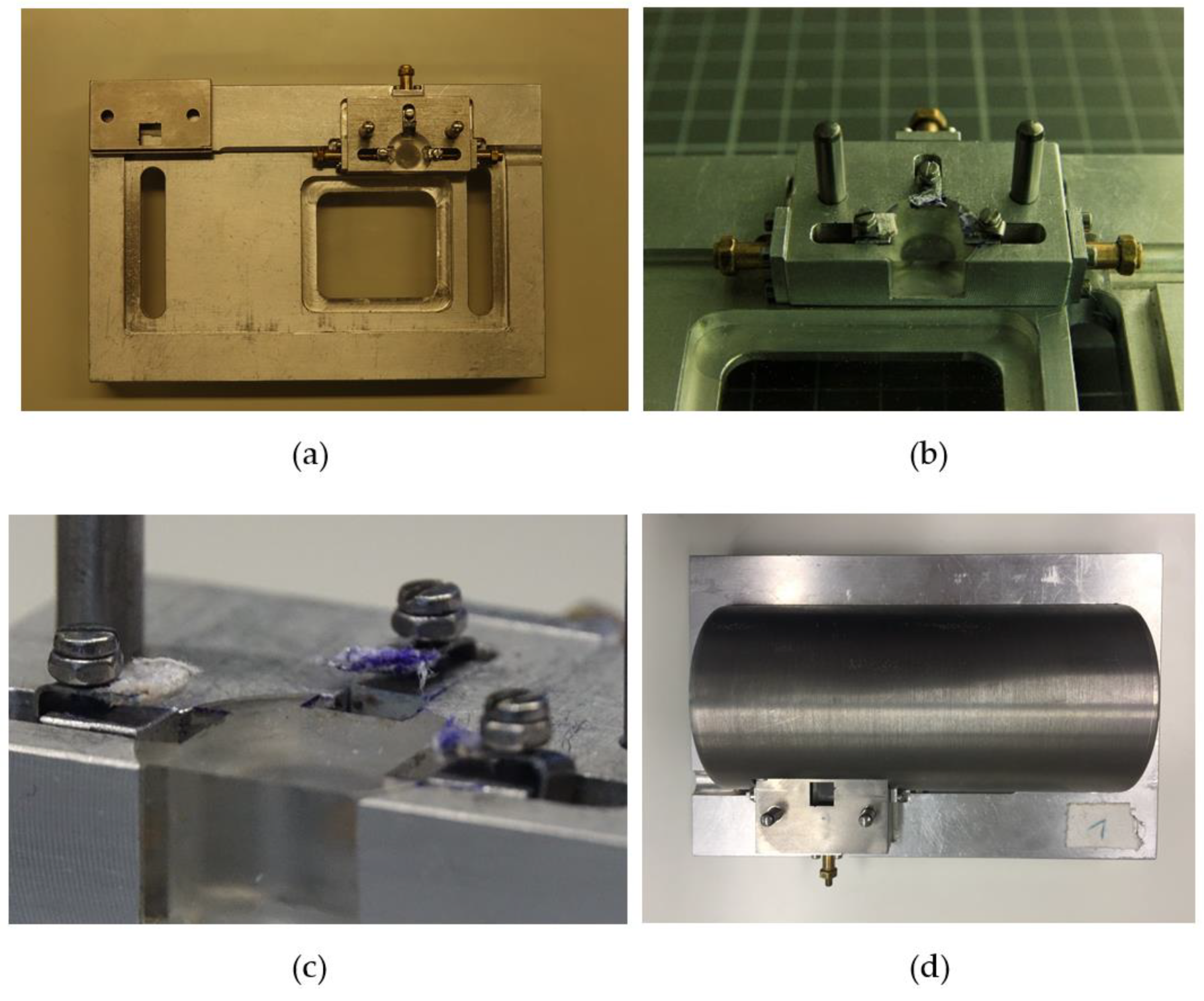
4.2. Ear Positioning and Accuracy
4.3. Scoring of Acute Side Effect: Erythema, Desquamation and Ear Swelling
4.4. Histopathological Analysis of Skin Toxicities on Day 92
4.5. Statistical Analyis
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bentzen, S.M. Preventing or reducing late side effects of radiation therapy: Radiobiology meets molecular pathology. Nat. Rev. Cancer 2006, 6, 702–713. [Google Scholar] [CrossRef] [PubMed]
- Prasanna, A.; Ahmed, M.M.; Mohiuddin, M.; Coleman, C.N. Exploiting sensitization windows of opportunity in hyper and hypo-fractionated radiation therapy. J. Thorac. Dis. 2014, 6, 287–302. [Google Scholar] [CrossRef]
- Baskar, R.; Lee, K.A.; Yeo, R.; Yeoh, K.W. Cancer and radiation therapy: Current advances and future directions. Int. J. Med. Sci. 2012, 9, 193–199. [Google Scholar] [CrossRef]
- Hall, S.; Rudrawar, S.; Zunk, M.; Bernaitis, N.; Arora, D.; McDermott, C.M.; Anoopkumar-Dukie, S. Protection against Radiotherapy-Induced Toxicity. Antioxidants 2016, 5, 22. [Google Scholar] [CrossRef]
- Hymes, S.R.; Strom, E.A.; Fife, C. Radiation dermatitis: Clinical presentation, pathophysiology, and treatment 2006. J. Am. Acad. Dermatol. 2006, 54, 28–46. [Google Scholar] [CrossRef] [PubMed]
- Sprung, C.N.; Forrester, H.B.; Siva, S.; Martin, O.A. Immunological markers that predict radiation toxicity. Cancer Lett. 2015, 368, 191–197. [Google Scholar] [CrossRef]
- Jacobson, L.K.; Johnson, M.B.; Dedhia, R.D.; Niknam-Bienia, S.; Wong, A.K. Impaired wound healing after radiation therapy: A systematic review of pathogenesis and treatment. JPRAS 2017, 13, 92–105. [Google Scholar] [CrossRef]
- Martin, M.T.; Vulin, A.; Hendry, J.H. Human epidermal stem cells: Role in adverse skin reactions and carcinogenesis from radiation. Mutat. Res. 2016, 770, 349–368. [Google Scholar] [CrossRef] [PubMed]
- Singh, M.; Alavi, A.; Wong, R.; Akita, S. Radiodermatitis: A Review of Our Current Understanding. Am. J. Clin. Dermatol. 2016, 17, 277–292. [Google Scholar] [CrossRef]
- Joiner, M.; Van der Kogel, A. Basic Clinical Radiobiology, 4th ed.; Hodder Education: London, UK, 2009; pp. 1–391. ISBN 978-0340929667. [Google Scholar]
- Mendelsohn, F.A.; Divino, C.M.; Reis, E.D.; Kerstein, M.D. Wound Care After Radiation Therapy. Adv. Skin Wound Care 2002, 15, 216–224. [Google Scholar] [CrossRef] [PubMed]
- Hegedus, F.; Mathew, L.M.; Schwartz, R.A. Radiation dermatitis: An overview. Int. J. Dermatol. 2017, 56, 909–914. [Google Scholar] [CrossRef]
- Sivan, V.; Vozenin-Brotons, M.-C.; Tricaud, Y.; Lefaix, J.-L.; Cosset, J.-M.; Dubray, B.; Martin, M.T. Altered proliferation and differentiation of human epidermis in cases of skin fibrosis after radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2002, 53, 385–393. [Google Scholar] [CrossRef]
- Ryan, J.L. Ionizing radiation: The good, the bad, and the ugly. J. Investig. Dermatol. 2012, 132, 985–993. [Google Scholar] [CrossRef]
- Straub, J.M.; New, J.; Hamilton, C.D.; Lominska, C.; Shnayder, Y.; Thomas, S.M. Radiation-induced fibrosis: Mechanisms and implications for therapy. J. Cancer Res. Clin. Oncol. 2015, 141, 1985–1994. [Google Scholar] [CrossRef]
- Okunieff, P.; Xu, J.; Hu, D.; Liu, W.; Zhang, L.; Morrow, G.; Pentland, A.; Ryan, J.L.; Ding, I. Curcumin protects against radiation-induced acute and chronic cutaneous toxicity in mice and decreases mRNA expression of inflammatory and fibrogenic cytokines. Int. J. Radiat. Oncol. Biol. Phys. 2006, 65, 890–898. [Google Scholar] [CrossRef]
- Mancini, M.; Sonis, S. Mechanisms of cellular fibrosis associated with cancer regimen-related toxicities. Front. Pharmacol. 2014, 5. [Google Scholar] [CrossRef] [PubMed]
- Wynn, T.A. Integrating mechanisms of pulmonary fibrosis. J. Exp. Med. 2011, 208, 1339–1350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ventura, J.; Lobachevsky, P.N.; Palazzolo, J.S.; Forrester, H.; Haynes, N.M.; Ivashkevich, A.; Stevenson, A.W.; Hall, C.J.; Ntargaras, A.; Kotsaris, V.; et al. Localized Synchrotron Irradiation of Mouse Skin Induces Persistent Systemic Genotoxic and Immune Responses. Cancer Res. 2017, 77, 6389–6399. [Google Scholar] [CrossRef] [Green Version]
- Gieringer, M.; Gosepath, J.; Naim, R. Radiotherapy and wound healing: Principles, management and prospects (review). Oncol. Rep. 2011, 26, 299–307. [Google Scholar] [CrossRef]
- Cox, J.D.; Stetz, J.; Pajak, T.F. Toxicity criteria of the Radiation Therapy Oncology Group (RTOG) and the European organization for research and treatment of cancer (EORTC). Int. J. Radiat. Oncol. Biol. Phys. 1995, 31, 1341–1346. [Google Scholar] [CrossRef]
- Girst, S.; Greubel, C.; Reindl, J.; Siebenwirth, C.; Zlobinskaya, O.; Walsh, D.W.; Ilicic, K.; Aichler, M.; Walch, A.; Wilkens, J.J.; et al. Proton Minibeam Radiation Therapy Reduces Side Effects in an In Vivo Mouse Ear Model. Int. J. Radiat. Oncol. Biol. Phys. 2016, 95, 234–241. [Google Scholar] [CrossRef]
- Law, M.P.; Ahier, R.G.; Field, S.B. The Response of Mouse Skin to Combined Hyperthermia and X-rays. Int. J. Radiat. Biol. Relat. Stud. Phys. Chem. Med. 1977, 32, 153–163. [Google Scholar] [CrossRef] [PubMed]
- Coggle, J.E.; Lambert, B.E.; Moores, S.R. Radiation effects in the lung. Environ. Health Perspect. 1986, 70, 261–291. [Google Scholar] [CrossRef]
- Anscher, M.S.; Kong, F.-M.; Jirtle, R.L. The relevance of transforming growth factor β1 in pulmonary injury after radiation therapy. Lung Cancer 1998, 19, 109–120. [Google Scholar] [CrossRef]
- Peach, M.S.; Showalter, T.N.; Ohri, N. Systematic Review of the Relationship between Acute and Late Gastrointestinal Toxicity after Radiotherapy for Prostate Cancer. Prostate Cancer 2015, 2015, 624736. [Google Scholar] [CrossRef]
- Dörr, W.; Hendry, J.H. Consequential late effects in normal tissues. Radiother. Oncol. 2001, 61, 223–231. [Google Scholar] [CrossRef]
- Collen, E.B.; Mayer, M.N. Acute effects of radiation treatment: Skin reactions. Can. Vet. J. 2006, 47, 931–935. [Google Scholar] [PubMed]
- Horton, J.A.; Chung, E.J.; Hudak, K.E.; Sowers, A.; Thetford, A.; White, A.O.; Mitchell, J.B.; Citrin, D.E. Inhibition of radiation-induced skin fibrosis with imatinib. Int. J. Radiat. Biol. 2013, 89, 162–170. [Google Scholar] [CrossRef]
- Panizzon, R.G.; Hanson, W.R.; Schwartz, D.E.; Malkinson, F.D. Ionizing Radiation Induces Early, Sustained Increases in Collagen Biosynthesis: A 48-Week Study in Mouse Skin and Skin Fibroblast Cultures. Radiat. Res. 1988, 116, 145–156. [Google Scholar] [CrossRef] [PubMed]
- Law, M.P. Vascular permeability and late radiation fibrosis in mouse lung. Radiat. Res. 1985, 103, 60–76. [Google Scholar] [CrossRef]
- Randall, K.; Coggle, J.E. Long-term expression of transforming growth factor TGF beta1 in mouse skin after localized beta-irradiation. Int. J. Radiat. Biol. 1996, 70, 351–360. [Google Scholar] [CrossRef] [PubMed]
- Formenti, S.C.; Demaria, S. Systemic effects of local radiotherapy. Lancet Oncol. 2009, 10, 718–726. [Google Scholar] [CrossRef] [Green Version]
- Williams, J.P.; Brown, S.L.; Georges, G.E.; Hauer-Jensen, M.; Hill, R.P.; Huser, A.K.; Kirsch, D.G.; Macvittie, T.J.; Mason, K.A.; Medhora, M.M.; et al. Animal models for medical countermeasures to radiation exposure. Radiat. Res. 2010, 173, 557–578. [Google Scholar] [CrossRef] [PubMed]
- Chaze, T.; Hornez, L.; Chambon, C.; Haddad, I.; Vinh, J.; Peyrat, J.P.; Benderitter, M.; Guipaud, O. Serum Proteome Analysis for Profiling Predictive Protein Markers Associated with the Severity of Skin Lesions Induced by Ionizing Radiation. Proteomes 2013, 1, 40–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coggle, J.E. Expression of Transforming Growth Factor-β1 in Mouse Skin During the Acute Phase of Radiation Damage. Int. J. Radiat. Biol. 1995, 68, 301–309. [Google Scholar] [CrossRef]
- Liao, W.; Hei, T.K.; Cheng, S.K. Radiation-Induced Dermatitis is Mediated by IL17-Expressing gammadelta T Cells. Radiat. Res. 2017, 187, 454–464. [Google Scholar] [CrossRef]
- Morris, G.M.; Hopewell, J.W. Changes in the cell kinetics of pig epidermis after single doses of X rays. Br. J. Radiol. 1988, 61, 205–211. [Google Scholar] [CrossRef]
- Jang, W.H.; Shim, S.; Wang, T.; Yoon, Y.; Jang, W.-S.; Myung, J.K.; Park, S.; Kim, K.H. In vivo characterization of early-stage radiation skin injury in a mouse model by two-photon microscopy. Sci. Rep. 2016, 6, 19216. [Google Scholar] [CrossRef] [Green Version]
- Yamaguchi, Y.; Yoshikawa, K. Cutaneous Wound Healing: An Update. J. Dermatol. 2001, 28, 521–534. [Google Scholar] [CrossRef]















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Dose (Gy) | Maximum Erythema Score (µm) | Time after First Fraction (d) | Maximum Desquamation Score (µm) | Time after First Fraction (d) |
|---|---|---|---|---|
| 0 (sham) | 0.4 ± 0.1 | 12 | 0.0 ± 0.0 | - |
| 4 × 5 | 0.6 ± 0.4 | 18 | 0.6 ± 0.4 | 22 |
| 4 × 10 | 1.0 ± 0.2 | 20–22 | 2.5 ± 0.2 | 21 |
| 4 × 20 | 1.4 ± 0.3 | 16 | 2.1 ± 0.3 | 18 |
| 4 × 30 | 1.4 ± 0.1 | 15–16 | 2.7 ± 0.3 | 21 |
| Dose (Gy) | Maximum of Ear Thickness (µm) | Time after First Fraction (d) |
|---|---|---|
| 0 (sham) | 276.7 ± 15.0 | 15 |
| 4 × 5 | 317.9 ± 8.2 | 14 |
| 4 × 10 | 461.9 ± 17.8 | 22 |
| 4 × 20 | 524.5 ± 16.5 | 18 |
| 4 × 30 | 582.4 ± 16.9 | 18 |
| Kind of Score | Description |
|---|---|
| Erythema Score | Erythema |
| 3 | Severe |
| 1.5 | Definite |
| 0.5 | Mild |
| 0 | No |
| Desquamation Score | Desquamation |
| 3 | Moist |
| 2 | Crust |
| 1 | Dry |
| 0 | No |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dombrowsky, A.C.; Schauer, J.; Sammer, M.; Blutke, A.; Walsh, D.W.M.; Schwarz, B.; Bartzsch, S.; Feuchtinger, A.; Reindl, J.; Combs, S.E.; et al. Acute Skin Damage and Late Radiation-Induced Fibrosis and Inflammation in Murine Ears after High-Dose Irradiation. Cancers 2019, 11, 727. https://doi.org/10.3390/cancers11050727
Dombrowsky AC, Schauer J, Sammer M, Blutke A, Walsh DWM, Schwarz B, Bartzsch S, Feuchtinger A, Reindl J, Combs SE, et al. Acute Skin Damage and Late Radiation-Induced Fibrosis and Inflammation in Murine Ears after High-Dose Irradiation. Cancers. 2019; 11(5):727. https://doi.org/10.3390/cancers11050727
Chicago/Turabian StyleDombrowsky, Annique C., Jannis Schauer, Matthias Sammer, Andreas Blutke, Dietrich W. M. Walsh, Benjamin Schwarz, Stefan Bartzsch, Annette Feuchtinger, Judith Reindl, Stephanie E. Combs, and et al. 2019. "Acute Skin Damage and Late Radiation-Induced Fibrosis and Inflammation in Murine Ears after High-Dose Irradiation" Cancers 11, no. 5: 727. https://doi.org/10.3390/cancers11050727
APA StyleDombrowsky, A. C., Schauer, J., Sammer, M., Blutke, A., Walsh, D. W. M., Schwarz, B., Bartzsch, S., Feuchtinger, A., Reindl, J., Combs, S. E., Dollinger, G., & Schmid, T. E. (2019). Acute Skin Damage and Late Radiation-Induced Fibrosis and Inflammation in Murine Ears after High-Dose Irradiation. Cancers, 11(5), 727. https://doi.org/10.3390/cancers11050727