Clinical Evaluation of CA72-4 for Screening Gastric Cancer in a Healthy Population: A Multicenter Retrospective Study

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
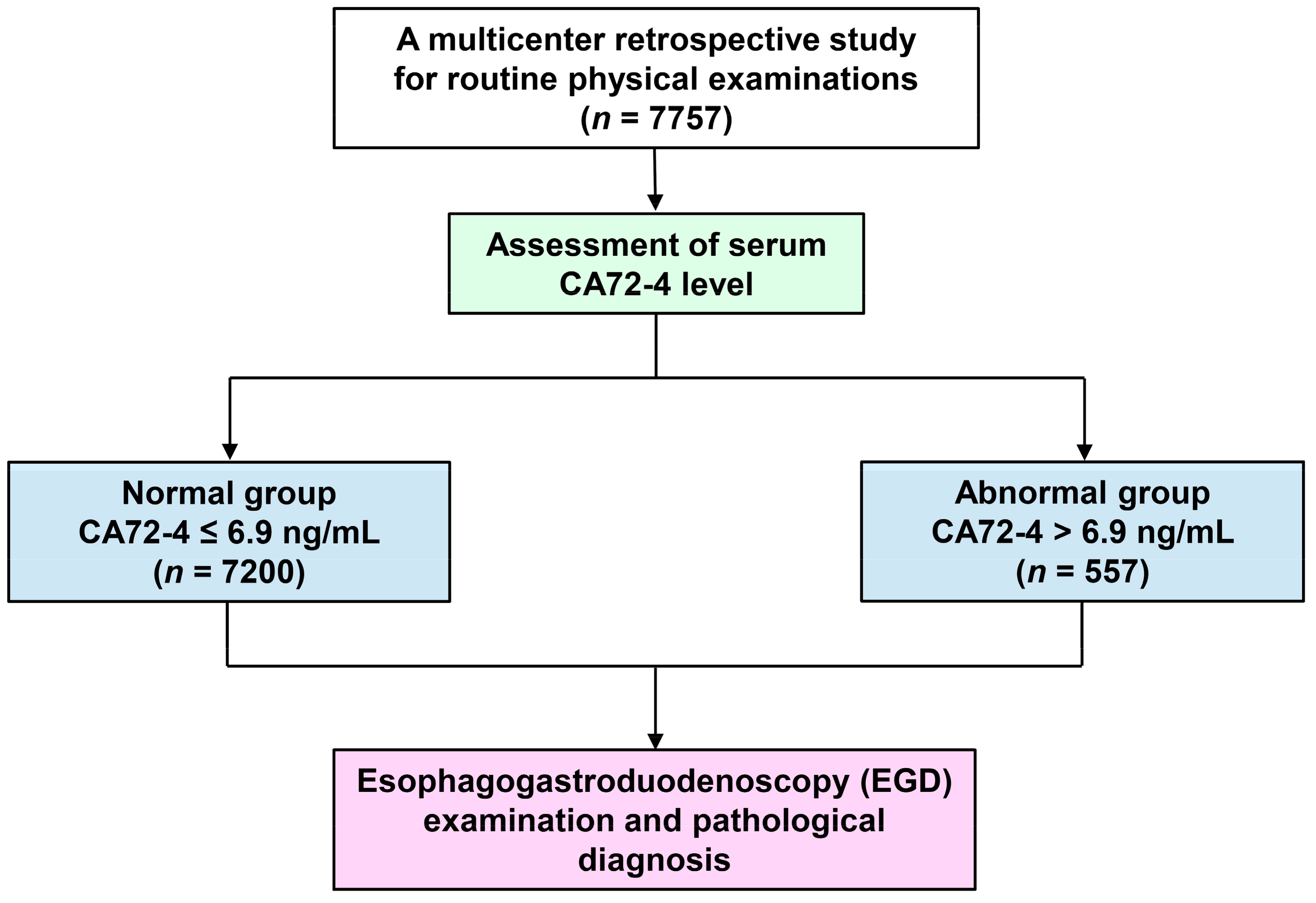
2.1. Study Design and Population Collection
2.2. Analysis of Serum Tumor Markers
2.3. Evaluation of EGD
2.4. Statistical Analysis
3. Results
3.1. Demographic Characteristics of the Study Population
3.2. Measuring Serum CA72-4 in Healthy Population
3.3. Association between Serum CA72-4 and EGD Findings
3.4. Association between CA72-4 Serum Level and GC
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Laversanne, M.; Brewster, D.H.; Gombe Mbalawa, C.; Kohler, B.; Pineros, M.; Steliarova-Foucher, E.; Swaminathan, R.; Antoni, S.; et al. Cancer Incidence in Five Continents: Inclusion criteria, highlights from Volume X and the global status of cancer registration. Int. J. Cancer 2015, 137, 2060–2071. [Google Scholar] [CrossRef] [PubMed]
- Sitarz, R.; Skierucha, M.; Mielko, J.; Offerhaus, G.J.A.; Maciejewski, R.; Polkowski, W.P. Gastric cancer: Epidemiology, prevention, classification, and treatment. Cancer Manag. Res. 2018, 10, 239–248. [Google Scholar] [CrossRef] [PubMed]
- Bickenbach, K.; Strong, V.E. Comparisons of Gastric Cancer Treatments: East vs. West. J. Gastric Cancer 2012, 12, 55–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dan, Y.Y.; So, J.B.; Yeoh, K.G. Endoscopic screening for gastric cancer. Clin. Gastroenterol. Hepatol. 2006, 4, 709–716. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.H.; Oh, S.J.; Oh, C.A.; Choi, M.G.; Noh, J.H.; Sohn, T.S.; Bae, J.M.; Kim, S. The relationships between perioperative CEA, CA 19-9, and CA 72-4 and recurrence in gastric cancer patients after curative radical gastrectomy. J. Surg. Oncol. 2011, 104, 585–591. [Google Scholar] [CrossRef]
- Shimada, H.; Noie, T.; Ohashi, M.; Oba, K.; Takahashi, Y. Clinical significance of serum tumor markers for gastric cancer: A systematic review of literature by the Task Force of the Japanese Gastric Cancer Association. Gastric Cancer 2014, 17, 26–33. [Google Scholar] [CrossRef]
- Colcher, D.; Hand, P.H.; Nuti, M.; Schlom, J. A spectrum of monoclonal antibodies reactive with human mammary tumor cells. Proc. Natl. Acad. Sci. USA 1981, 78, 3199–3203. [Google Scholar] [CrossRef]
- Mariampillai, A.I.; Cruz, J.P.D.; Suh, J.; Sivapiragasam, A.; Nevins, K.; Hindenburg, A.A. Cancer Antigen 72-4 for the Monitoring of Advanced Tumors of the Gastrointestinal Tract, Lung, Breast and Ovaries. Anticancer Res. 2017, 37, 3649–3656. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marshall, B. Helicobacter pylori: 20 years on. Clin. Med. 2002, 2, 147–152. [Google Scholar] [CrossRef]
- Rehena, Z.; Ghosh, C.K.; Afroz, F.; Alam, M.B.; Ferdousi, S.; Mahmuduzzaman, M.; Sultana, T.; Ahmed, A.N. Comparison of Serum CA72-4 and CEA Levels in Patient with Endoscopically Suspected Gastric Carcinoma. Mymensingh Med. J. 2015, 24, 542–549. [Google Scholar] [PubMed]
- Liang, Y.; Wang, W.; Fang, C.; Raj, S.S.; Hu, W.M.; Li, Q.W.; Zhou, Z.W. Clinical significance and diagnostic value of serum CEA, CA19-9 and CA72-4 in patients with gastric cancer. Oncotarget 2016, 7, 49565–49573. [Google Scholar] [CrossRef]
- Goral, V.; Yesilbagdan, H.; Kaplan, A.; Sit, D. Evaluation of CA 72-4 as a new tumor marker in patients with gastric cancer. Hepatogastroenterology 2007, 54, 1272–1275. [Google Scholar]
- Ucar, E.; Semerci, E.; Ustun, H.; Yetim, T.; Huzmeli, C.; Gullu, M. Prognostic value of preoperative CEA, CA 19-9, CA 72-4, and AFP levels in gastric cancer. Adv. Ther. 2008, 25, 1075–1084. [Google Scholar] [CrossRef]
- Gaspar, M.J.; Arribas, I.; Coca, M.C.; Diez-Alonso, M. Prognostic value of carcinoembryonic antigen, CA 19-9 and CA 72-4 in gastric carcinoma. Tumour. Biol. 2001, 22, 318–322. [Google Scholar] [CrossRef]
- Aloe, S.; D’Alessandro, R.; Spila, A.; Ferroni, P.; Basili, S.; Palmirotta, R.; Carlini, M.; Graziano, F.; Mancini, R.; Mariotti, S.; et al. Prognostic value of serum and tumor tissue CA 72-4 content in gastric cancer. Int. J. Biol. Markers 2003, 18, 21–27. [Google Scholar] [CrossRef]
- Ikeguchi, M.; Katano, K.; Saitou, H.; Tsujitani, S.; Maeta, M.; Kaibara, N. Pre-operative serum levels of CA72-4 in patients with gastric adenocarcinoma. Hepatogastroenterology 1997, 44, 866–871. [Google Scholar] [PubMed]
- Hamazoe, R.; Maeta, M.; Matsui, T.; Shibata, S.; Shiota, S.; Kaibara, N. CA72-4 compared with carcinoembryonic antigen as a tumour marker for gastric cancer. Eur. J. Cancer 1992, 28A, 1351–1354. [Google Scholar] [CrossRef]
- Chen, X.Z.; Zhang, W.K.; Yang, K.; Wang, L.L.; Liu, J.; Wang, L.; Hu, J.K.; Zhang, B.; Chen, Z.X.; Chen, J.P.; et al. Correlation between serum CA72-4 and gastric cancer: Multiple analyses based on Chinese population. Mol. Biol. Rep. 2012, 39, 9031–9039. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.; Zheng, W. An Alternative Method for Screening Gastric Cancer Based on Serum Levels of CEA, CA19-9, and CA72-4. J. Gastrointest. Cancer 2018, 49, 57–62. [Google Scholar] [CrossRef]
- Lee, J.C.; Lee, S.Y.; Kim, C.Y.; Yang, D.H. Clinical utility of tumor marker cutoff ratio and a combination scoring system of preoperative carcinoembryonic antigen, carbohydrate antigen 19-9, carbohydrate antigen 72-4 levels in gastric cancer. J. Korean Surg. Soc. 2013, 85, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Jing, J.X.; Wang, Y.; Xu, X.Q.; Sun, T.; Tian, B.G.; Du, L.L.; Zhao, X.W.; Han, C.Z. Tumor markers for diagnosis, monitoring of recurrence and prognosis in patients with upper gastrointestinal tract cancer. Asian Pac. J. Cancer Prev. 2014, 15, 10267–10272. [Google Scholar] [CrossRef]
- Parkin, D.M. The global health burden of infection-associated cancers in the year 2002. Int. J. Cancer 2006, 118, 3030–3044. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiariotti, L.; Angrisano, T.; Keller, S.; Florio, E.; Affinito, O.; Pallante, P.; Perrino, C.; Pero, R.; Lembo, F. Epigenetic modifications induced by Helicobacter pylori infection through a direct microbe-gastric epithelial cells cross-talk. Med. Microbiol. Immunol. 2013, 202, 327–337. [Google Scholar] [CrossRef] [PubMed]
- Taiwan’s Leading Causes of Death in 2016 (Last updated by 19 June, 2017). Available online: https://www.mohw.gov.tw/cp-3425-33347-2.html (accessed on 26 April 2019).
- Hong, J.; Tsai, Y.; Novick, D.; Hsiao, F.C.; Cheng, R.; Chen, J.S. The economic burden of advanced gastric cancer in Taiwan. BMC Health Serv. Res. 2017, 17, 663. [Google Scholar] [CrossRef]
- Menon, S.; Trudgill, N. How commonly is upper gastrointestinal cancer missed at endoscopy? A meta-analysis. Endosc. Int. Open 2014, 2, E46–E50. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Parameter | Number (%) |
|---|---|
| Total population | 7757 |
| Age (mean ± SD) | 45.6 ± 11.1 |
| Gender | |
| Male, n (%) | 4704 (60.6%) |
| Female, n (%) | 3053 (39.4%) |
| Total number | 7757 |
| Smoking history | |
| Yes, n (%) | 1668 (21.9%) |
| No, n (%) | 5950 (78.1%) |
| Total number | 7618 |
| BMI † (mean ± SD), kg/m2 | 23.8 ± 3.6 |
| H. pylori infection | |
| Positive, n (%) | 1611 (21.1%) |
| Negative, n (%) | 6030 (78.9%) |
| Total number | 7641 |
| CA72-4 (mean ± SD), ng/mL | 2.8 ± 3.9 |
| Total number | 7757 |
| CA19-9 (mean ± SD), U/mL | 10.3 ± 8.3 |
| Total number CA19-9 positive, n (%) | 5989 52 (0.87%) |
| CEA (mean ± SD), ng/mL | 1.7 ± 1.2 |
| Total number CEA positive, n (%) | 7703 181 (2.35%) |
| Variable | High CA72-4 Level (n = 557) | Normal CA72-4 Level (n = 7200) | p-Value † |
|---|---|---|---|
| Age (years ± SD) | 46.8 ± 12.2 | 45.5 ± 11.0 | 0.007 |
| Male, n (%) | 346 (62.1%) | 4358 (60.5%) | 0.459 |
| Smoking history, % | 22.2% | 21.9% | 0.848 |
| BMI (mean ± SD), kg/m2 | 24.0 ± 3.6 | 23.8 ± 3.6 | 0.394 |
| H. pylori infection, % | 27.5% | 20.6% | <0.001 |
| CA72-4 (mean ± SD), ng/mL | 14.2 ± 7.1 | 2.0 ± 1.3 | <0.001 |
| CA19-9 (mean ± SD), U/mL | 10.1 ± 8.9 | 10.3 ± 8.3 | 0.744 |
| CEA (mean ± SD), ng/mL | 2.0 ± 1.2 | 1.7 ± 1.2 | <0.001 |
| Variable ‡ | Multiple Analysis † | ||
|---|---|---|---|
| p-Value ¶ | OR | (95% CI) | |
| Age (Years) | 0.014 | 1.01 | 1.00–1.02 |
| Male | 0.476 | 1.07 | 0.89–1.29 |
| Smoking history | 0.911 | 0.99 | 0.80–1.22 |
| BMI (kg/m2) | 0.515 | 1.01 | 0.98–1.03 |
| H. pylori infection | <0.001 | 1.44 | 1.19–1.76 |
| EGD Finding | High CA72-4 Level (n = 557) | Normal CA72-4 Level (n = 7200) | p-Value † |
|---|---|---|---|
| Normal | 214 (38.4%) | 3454 (48%) | |
| Reflux esophagitis | 143 (25.7%) | 1870 (26%) | 0.877 |
| Gastric ulcer | 53 (9.5%) | 328 (4.6%) | <0.001 |
| Gastric polyps | 83 (14.9%) | 776 (10.8%) | 0.003 |
| Gastric erosions | 74 (13.3%) | 792 (11%) | 0.099 |
| Atrophic gastritis | 57 (10.2%) | 566 (7.9%) | 0.047 |
| Gastric submucosal tumor | 23 (4.1%) | 291 (4.0%) | 0.920 |
| Esophageal cancer | 0 (0%) | 2 (0.03%) | 0.694 |
| Gastric cancer | 1 (0.18%) | 2 (0.03%) | 0.079 |
| Outcome of EGD Finding | Univariate † | Multivariate ‡ | ||
|---|---|---|---|---|
| OR | 95% CI | Adjusted OR | Adjusted 95% CI | |
| Reflux esophagitis | 0.99 | 0.81–1.20 | 0.98 | 0.80–1.20 |
| Gastric ulcer | 2.20 | 1.63–2.99 *** | 2.11 | 1.56–2.86 *** |
| Gastric polyps | 1.45 | 1.14–1.85 ** | 1.42 | 1.11–1.81 ** |
| Gastric erosions | 1.24 | 0.96–1.60 | 1.13 | 0.87–1.47 |
| Atrophic gastritis | 1.34 | 1.00–1.78* | 1.27 | 0.95–1.69 |
| Gastric submucosal tumor | 1.02 | 0.66–1.58 | 0.98 | 0.63–1.51 |
| Gastric cancer | 6.47 | 0.59–71.5 | 4.54 | 0.37–56.32 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hu, P.-J.; Chen, M.-Y.; Wu, M.-S.; Lin, Y.-C.; Shih, P.-H.; Lai, C.-H.; Lin, H.-J. Clinical Evaluation of CA72-4 for Screening Gastric Cancer in a Healthy Population: A Multicenter Retrospective Study. Cancers 2019, 11, 733. https://doi.org/10.3390/cancers11050733
Hu P-J, Chen M-Y, Wu M-S, Lin Y-C, Shih P-H, Lai C-H, Lin H-J. Clinical Evaluation of CA72-4 for Screening Gastric Cancer in a Healthy Population: A Multicenter Retrospective Study. Cancers. 2019; 11(5):733. https://doi.org/10.3390/cancers11050733
Chicago/Turabian StyleHu, Ping-Jen, Ming-Yao Chen, Ming-Shun Wu, Ying-Chin Lin, Ping-Hsiao Shih, Chih-Ho Lai, and Hwai-Jeng Lin. 2019. "Clinical Evaluation of CA72-4 for Screening Gastric Cancer in a Healthy Population: A Multicenter Retrospective Study" Cancers 11, no. 5: 733. https://doi.org/10.3390/cancers11050733
APA StyleHu, P.-J., Chen, M.-Y., Wu, M.-S., Lin, Y.-C., Shih, P.-H., Lai, C.-H., & Lin, H.-J. (2019). Clinical Evaluation of CA72-4 for Screening Gastric Cancer in a Healthy Population: A Multicenter Retrospective Study. Cancers, 11(5), 733. https://doi.org/10.3390/cancers11050733