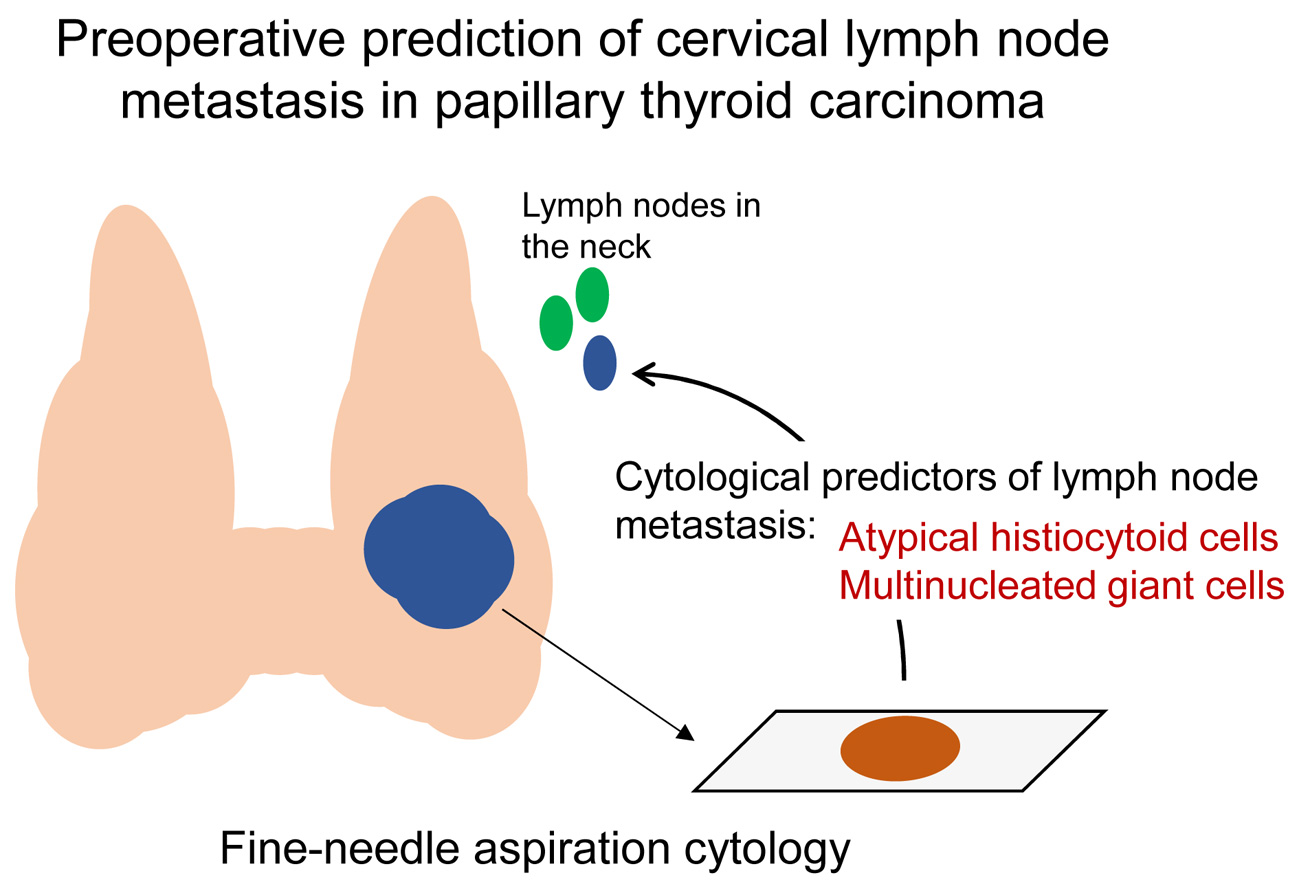
Atypical Histiocytoid Cells and Multinucleated Giant Cells in Fine-Needle Aspiration Cytology of the Thyroid Predict Lymph Node Metastasis of Papillary Thyroid Carcinoma



Abstract
:
1. Introduction
2. Results
2.1. Correlation between Clinicopathologic Features and Lymph Node Metastasis
2.2. Correlation between Cytomorphologic Features and Lymph Node Metastasis
2.3. Correlation between BRAF Mutation and Lymph Node Metastasis
2.4. Multivariate Analysis
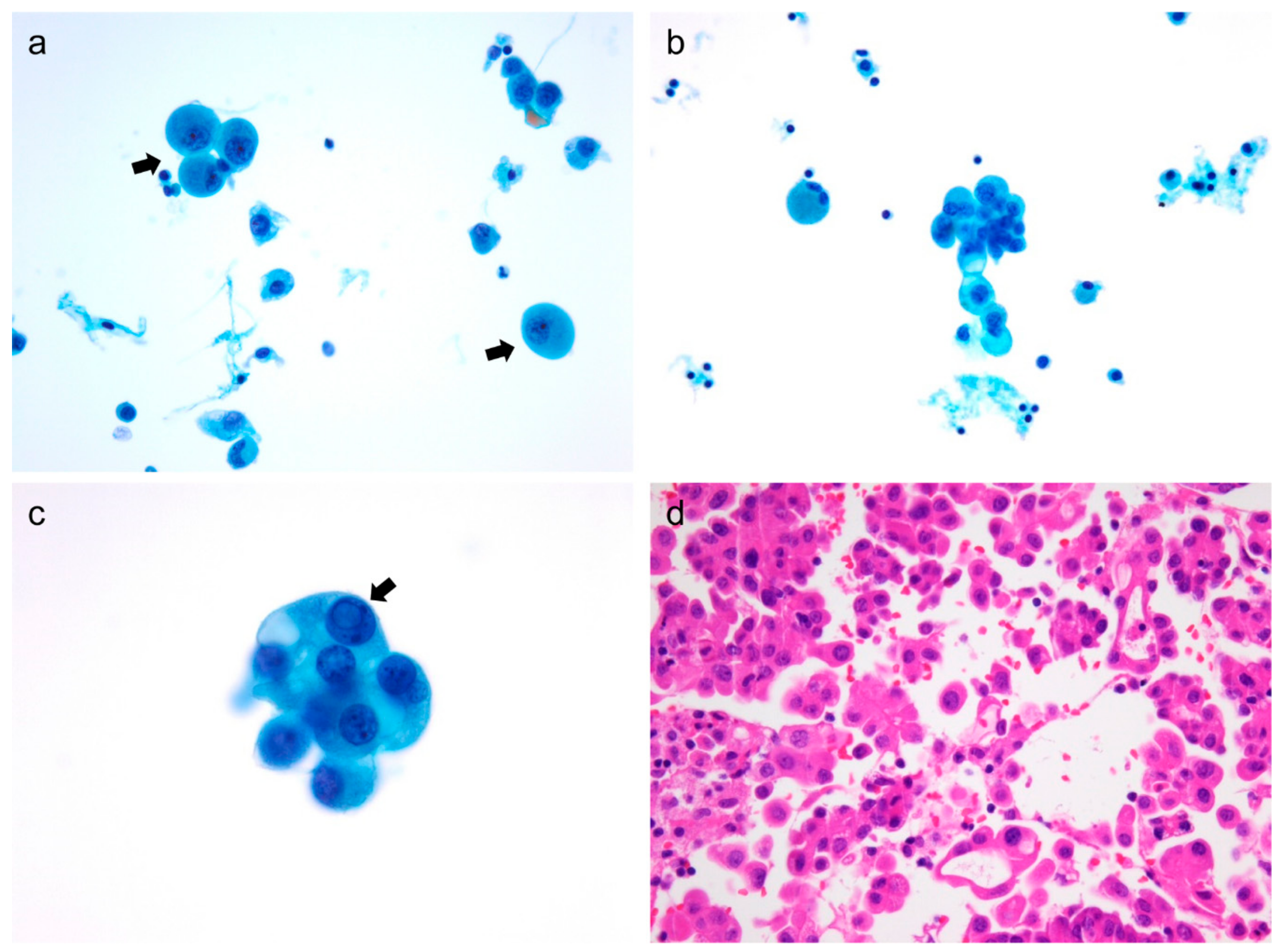
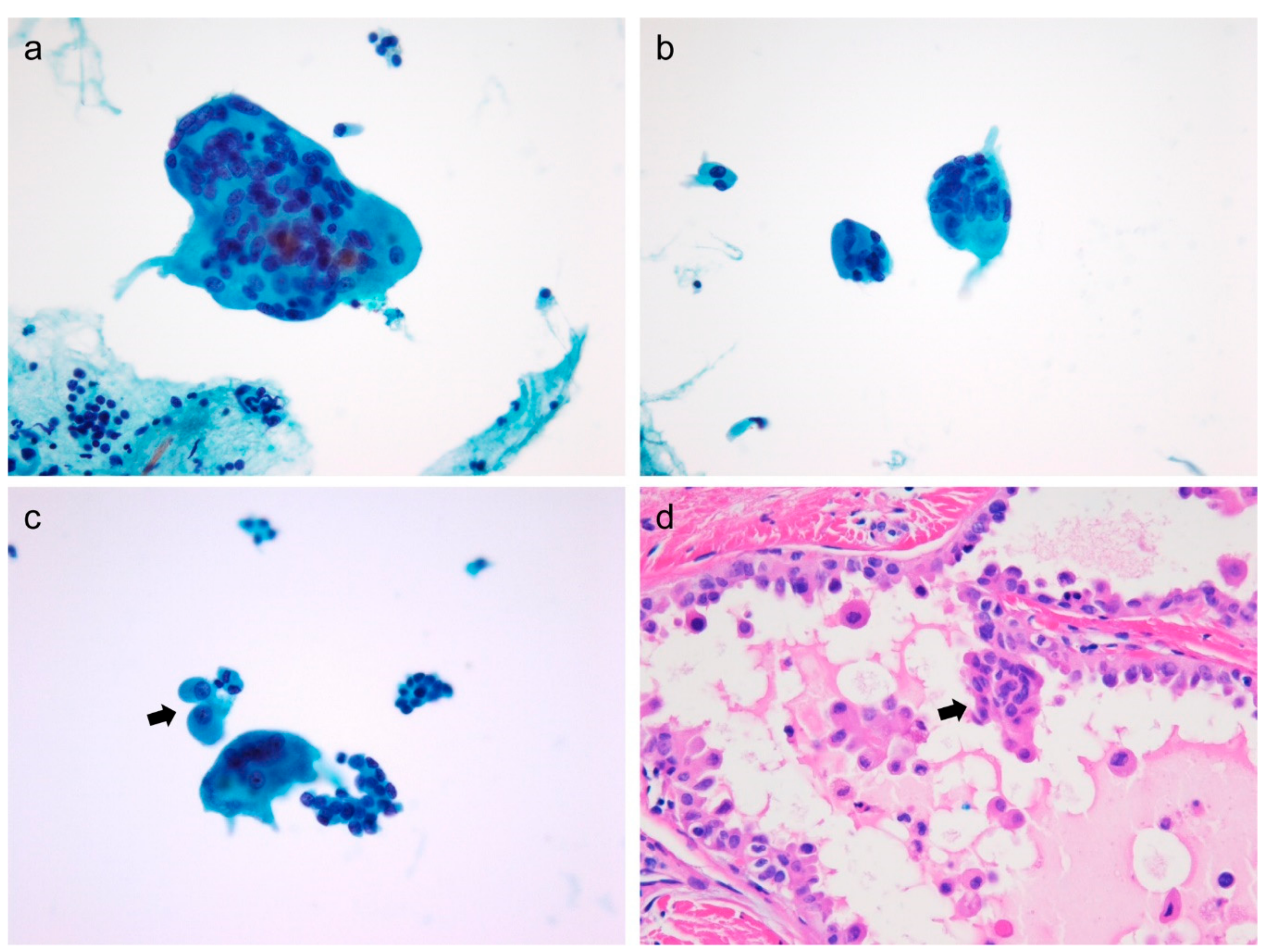
2.5. Cytomorphological Analysis of Atypical Histiocytoid Cells
2.6. Sub-Analysis of Patients with Microcarcinoma
3. Discussion
4. Materials and Methods
4.1. Patients and Clinical Samples
4.2. Cytomorphologic Evaluation
4.3. BRAF V600E Mutation Analysis
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M.; et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 2016, 26, 1–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, F.H.; Kuo, S.F.; Hsueh, C.; Chao, T.C.; Lin, J.D. Postoperative recurrence of papillary thyroid carcinoma with lymph node metastasis. J. Surg. Oncol. 2015, 112, 149–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mazzaferri, E.L.; Kloos, R.T. Clinical review 128: Current approaches to primary therapy for papillary and follicular thyroid cancer. J. Clin. Endocrinol. Metab. 2001, 86, 1447–1463. [Google Scholar] [CrossRef] [PubMed]
- Pyo, J.S.; Sohn, J.H.; Chang, K. Prognostic Role of Metastatic Lymph Node Ratio in Papillary Thyroid Carcinoma. J. Pathol. Trans. Med. 2018, 52, 331–338. [Google Scholar] [CrossRef] [PubMed]
- Das, D.K. Psammoma body: A product of dystrophic calcification or of a biologically active process that aims at limiting the growth and spread of tumor? Diagn. Cytopathol. 2009, 37, 534–541. [Google Scholar] [CrossRef] [PubMed]
- Hwang, H.S.; Orloff, L.A. Efficacy of preoperative neck ultrasound in the detection of cervical lymph node metastasis from thyroid cancer. Laryngoscope 2011, 121, 487–491. [Google Scholar] [CrossRef]
- Lee, D.W.; Ji, Y.B.; Sung, E.S.; Park, J.S.; Lee, Y.J.; Park, D.W.; Tae, K. Roles of ultrasonography and computed tomography in the surgical management of cervical lymph node metastases in papillary thyroid carcinoma. Eur. J. Surg. Oncol. 2013, 39, 191–196. [Google Scholar] [CrossRef]
- Lee, Y.J.; Kim, D.W.; Park, H.K.; Kim, D.H.; Jung, S.J.; Oh, M.; Bae, S.K. Pre-operative ultrasound diagnosis of nodal metastasis in papillary thyroid carcinoma patients according to nodal compartment. Ultrasound Med. Biol. 2015, 41, 1294–1300. [Google Scholar] [CrossRef]
- Cai, Y.F.; Wang, Q.X.; Ni, C.J.; Guo, G.L.; Li, Q.; Wang, O.C.; Wu, L.; Du, H.Y.; You, J.; Zhang, X.H. The Clinical Relevance of Psammoma Body and Hashimoto Thyroiditis in Papillary Thyroid Carcinoma: A Large Case-control Study. Medicine (Baltimore) 2015, 94, e1881. [Google Scholar] [CrossRef]
- Kim, Y.; Kim, M.H.; Jeon, S.; Kim, J.; Kim, C.; Bae, J.S.; Jung, C.K. Prognostic implication of histological features associated with EHD2 expression in papillary thyroid carcinoma. PLoS ONE 2017, 12, e0174737. [Google Scholar] [CrossRef]
- Bai, Y.; Kakudo, K.; Li, Y.; Liu, Z.; Ozaki, T.; Ito, Y.; Kihara, M.; Miyauchi, A. Subclassification of non-solid-type papillary thyroid carcinoma identification of high-risk group in common type. Cancer Sci. 2008, 99, 1908–1915. [Google Scholar] [CrossRef] [PubMed]
- Das, D.K.; Mallik, M.K.; Haji, B.E.; Ahmed, M.S.; Al-Shama’a, M.; Al-Ayadhy, B.; George, S.S.; Sathar, S.A.; Junaid, T.A. Psammoma body and its precursors in papillary thyroid carcinoma: A study by fine-needle aspiration cytology. Diagn. Cytopathol. 2004, 31, 380–386. [Google Scholar] [CrossRef]
- Pusztaszeri, M.P.; Auger, M.; Stelow, E.B.; Yang, G.C.H.; Sanchez, M.A.; LiVolsi, V.A. Papillary Thyroid Carcinoma, Variants, and Related Tumors. In The Bethesda System for Reporting Thyroid Cytopathology: Definitions, Criteria, and Explanatory Notes; Ali, S.Z., Cibas, E.S., Eds.; Springer International Publishing: Cham, Switzerland, 2018; pp. 119–156. [Google Scholar] [CrossRef]
- Lee, S.H.; Jung, C.K.; Bae, J.S.; Jung, S.L.; Choi, Y.J.; Kang, C.S. Liquid-based cytology improves preoperative diagnostic accuracy of the tall cell variant of papillary thyroid carcinoma. Diagn. Cytopathol. 2014, 42, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Renshaw, A.A. “Histiocytoid” cells in fine-needle aspirations of papillary carcinoma of the thyroid: Frequency and significance of an under-recognized cytologic pattern. Cancer 2002, 96, 240–243. [Google Scholar] [CrossRef]
- Harshan, M.; Crapanzano, J.P.; Aslan, D.L.; Vazquez, M.F.; Saqi, A. Papillary thyroid carcinoma with atypical histiocytoid cells on fine-needle aspiration. Diagn. Cytopathol. 2009, 37, 244–250. [Google Scholar] [CrossRef]
- Canepa, M.; Elsheikh, T.M.; Sabo, D.A.; Kolosiwsky, A.M.; Reynolds, J.P. Atypical Histiocytoid Cells in Metastatic Papillary Thyroid Carcinoma: An Underrecognized Cytologic Pattern. Am. J. Clin. Pathol. 2017, 148, 58–63. [Google Scholar] [CrossRef] [PubMed]
- Brooks, E.; Simmons-Arnold, L.; Naud, S.; Evans, M.F.; Elhosseiny, A. Multinucleated giant cells’ incidence, immune markers, and significance: A study of 172 cases of papillary thyroid carcinoma. Head Neck Pathol. 2009, 3, 95–99. [Google Scholar] [CrossRef]
- Lundgren, C.I.; Hall, P.; Ekbom, A.; Frisell, J.; Zedenius, J.; Dickman, P.W. Incidence and survival of Swedish patients with differentiated thyroid cancer. Int. J. Cancer 2003, 106, 569–573. [Google Scholar] [CrossRef]
- Lundgren, C.I.; Hall, P.; Dickman, P.W.; Zedenius, J. Clinically significant prognostic factors for differentiated thyroid carcinoma: A population-based, nested case-control study. Cancer 2006, 106, 524–531. [Google Scholar] [CrossRef]
- Eun, N.L.; Son, E.J.; Kim, J.A.; Gweon, H.M.; Kang, J.H.; Youk, J.H. Comparison of the diagnostic performances of ultrasonography, CT and fine needle aspiration cytology for the prediction of lymph node metastasis in patients with lymph node dissection of papillary thyroid carcinoma: A retrospective cohort study. Int. J. Surg. 2018, 51, 145–150. [Google Scholar] [CrossRef]
- Cooper, D.S.; Doherty, G.M.; Haugen, B.R.; Kloos, R.T.; Lee, S.L.; Mandel, S.J.; Mazzaferri, E.L.; McIver, B.; Pacini, F.; Schlumberger, M.; et al. Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid 2009, 19, 1167–1214. [Google Scholar] [CrossRef]
- Tsou, P.L.; Hsiao, Y.L.; Chang, T.C. Multinucleated giant cells in fine needle aspirates. Can they help differentiate papillary thyroid cancer from benign nodular goiter? Acta Cytol. 2002, 46, 823–827. [Google Scholar] [CrossRef]
- Legesse, T.; Parker, L.; Heath, J.; Staats, P.N. Distinguishing non-invasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP) from classic and invasive follicular-variant papillary thyroid carcinomas based on cytologic features. J. Am. Soc. Cytopathol. 2019, 8, 11–17. [Google Scholar] [CrossRef]
- Fadda, G.; Rossi, E.D. Liquid-Based Cytology in Fine-Needle Aspiration Biopsies of the Thyroid Gland. Acta Cytol. 2011, 55, 389–400. [Google Scholar] [CrossRef]
- Baum, J.E.; Soong, L.; Scognamiglio, T.; Margolskee, E.M.; Hoda, R.S.; Rao, R. Cytological diagnosis of papillary thyroid carcinoma with tall cells on ThinPrep liquid-based cytology. Diagn. Cytopathol. 2019, 47, 541–546. [Google Scholar] [CrossRef]
- Chong, Y.; Ji, S.J.; Kang, C.S.; Lee, E.J. Can liquid-based preparation substitute for conventional smear in thyroid fine-needle aspiration? A systematic review based on meta-analysis. Endocr. Connect. 2017, 6, 817–829. [Google Scholar] [CrossRef] [Green Version]
- Cooper, D.S.; Doherty, G.M.; Haugen, B.R.; Kloos, R.T.; Lee, S.L.; Mandel, S.J.; Mazzaferri, E.L.; McIver, B.; Sherman, S.I.; Tuttle, R.M. Management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid 2006, 16, 109–142. [Google Scholar] [CrossRef]
- Sitges-Serra, A.; Lorente, L.; Mateu, G.; Sancho, J.J. Therapy of Endocrine Disease: Central neck dissection: A step forward in the treatment of papillary thyroid cancer. Eur. J. Endocrinol. 2015, 173, R199–R206. [Google Scholar] [CrossRef]
- Zhao, H.; Li, H. Meta-analysis of ultrasound for cervical lymph nodes in papillary thyroid cancer: Diagnosis of central and lateral compartment nodal metastases. Eur. J. Radiol. 2019, 112, 14–21. [Google Scholar] [CrossRef]
- Cho, U.; Oh, W.J.; Bae, J.S.; Lee, S.; Lee, Y.S.; Park, G.S.; Lee, Y.S.; Jung, C.K. Clinicopathological features of rare BRAF mutations in Korean thyroid cancer patients. J. Korean Med. Sci. 2014, 29, 1054–1060. [Google Scholar] [CrossRef]
- Yu, F.X.; Hu, M.X.; Zhao, H.X.; Niu, L.J.; Rong, X.Y.; Li, W.H.; Zhu, Q.; Ying, J.M.; Lyu, N. Precise Detection of Gene Mutations in Fine-Needle Aspiration Specimens of the Papillary Thyroid Microcarcinoma Using Next-Generation Sequencing. Int. J. Endocrinol. 2019, 2019, 4723958. [Google Scholar] [CrossRef]
- Yang, Q.; Huo, S.; Sui, Y.; Du, Z.; Zhao, H.; Liu, Y.; Li, W.; Wan, X.; Liu, T.; Zhang, G. Mutation Status and Immunohistochemical Correlation of KRAS, NRAS, and BRAF in 260 Chinese Colorectal and Gastric Cancers. Front. Oncol. 2018, 8, 487. [Google Scholar] [CrossRef] [Green Version]
- Jennings, L.J.; Arcila, M.E.; Corless, C.; Kamel-Reid, S.; Lubin, I.M.; Pfeifer, J.; Temple-Smolkin, R.L.; Voelkerding, K.V.; Nikiforova, M.N. Guidelines for Validation of Next-Generation Sequencing-Based Oncology Panels: A Joint Consensus Recommendation of the Association for Molecular Pathology and College of American Pathologists. J. Mol. Diagn. 2017, 19, 341–365. [Google Scholar] [CrossRef]
- Jeon, S.; Kim, Y.; Jeong, Y.M.; Bae, J.S.; Jung, C.K. CCND1 Splice Variant as A Novel Diagnostic and Predictive Biomarker for Thyroid Cancer. Cancers (Basel) 2018, 10, 437. [Google Scholar] [CrossRef]
- Jung, C.K.; Kim, Y.; Jeon, S.; Jo, K.; Lee, S.; Bae, J.S. Clinical utility of EZH1 mutations in the diagnosis of follicular-patterned thyroid tumors. Hum. Pathol. 2018, 81, 9–17. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Characteristics | No. of Cases |
|---|---|
| Age (year, mean ± standard deviation) | 49.5 ± 12.8 |
| Sex | |
| Female | 172 (77.5%) |
| Male | 50 (22.5%) |
| Tumor size | |
| ≤1 cm | 164 (73.9%) |
| >1 cm | 58 (26.1%) |
| Histologic subtype | |
| Classic papillary | 165 (74.3%) |
| Classic papillary with tall cell features | 21 (9.5%) |
| Infiltrative follicular | 13 (5.9%) |
| Tall cell | 11 (5.0%) |
| Invasive encapsulated follicular | 8 (3.6%) |
| Oncocytic | 2 (0.9%) |
| Cribriform morular | 1 (0.5%) |
| Warthin-like | 1 (0.5%) |
| Multifocality | |
| Unifocal | 112 (50.5%) |
| Multifocal | 110 (49.5%) |
| Extrathyroidal extension | |
| Absent | 133 (59.9%) |
| Microscopic | 82 (36.9%) |
| Gross | 7 (3.2%) |
| pN stage | |
| pN0 | 123 (55.4%) |
| pN1a | 74 (33.3%) |
| pN1b | 25 (11.3%) |
| BRAF V600E mutation 1 | |
| Absent | 47/203 (23.2%) |
| Present | 156/203 (76.8%) |
| Variable | Cervical Lymph Node Metastasis | ||
|---|---|---|---|
| Absent (n = 123) | Present (n = 99) | p-Value | |
| Age (year, mean ± standard deviation) | 50.8 ± 12.6 | 48.0 ± 12.9 | 0.107 |
| Sex | 0.923 | ||
| Female | 95 (77.2%) | 77 (77.8%) | |
| Male | 28 (22.8%) | 22 (22.2%) | |
| Tumor size | 0.012 | ||
| ≤1 cm | 99 (80.5%) | 65 (65.7%) | |
| >1 cm | 24 (19.5%) | 34 (34.3%) | |
| Multifocality | 0.003 | ||
| Unifocal | 73 (59.3%) | 39 (39.4%) | |
| Multifocal | 50 (40.7%) | 60 (60.6%) | |
| Cellularity | 0.021 | ||
| Low | 33 (26.8%) | 14 (14.1%) | |
| Moderate/high | 90 (73.2%) | 85 (85.9%) | |
| Isolated tumor cells | 0.657 | ||
| Absent/low | 83 (67.5%) | 64 (64.6%) | |
| Moderate/high | 40 (32.5%) | 35 (35.4%) | |
| Atypical histiocytoid cells | <0.001 | ||
| Absent | 70 (56.9%) | 30 (30.3%) | |
| Present | 53 (43.1%) | 69 (69.7%) | |
| Tall cells | 0.952 | ||
| Absent/low | 104 (84.6%) | 84 (84.8%) | |
| Moderate/high | 19 (15.4%) | 15 (15.2%) | |
| Multinucleated giant cells | <0.001 | ||
| Absent/low | 117 (95.1%) | 78 (78.8%) | |
| Moderate/high | 6 (4.9%) | 21 (21.2%) | |
| Macrophages | 0.786 | ||
| Absent/low | 104 (86.4%) | 85 (85.9%) | |
| Moderate/high | 19 (15.4%) | 14 (14.1%) | |
| Psammoma bodies | 0.224 | ||
| Absent | 119 (96.7%) | 92 (92.9%) | |
| Present | 4 (3.3%) | 7 (7.1%) | |
| BRAF V600E mutation 1 | 0.054 | ||
| Wild | 31/109 (28.4%) | 16/94 (17.0%) | |
| Mutant | 78/109 (71.6%) | 78/94 (83.0%) | |
| Characteristic | Odds Ratio | 95% Confidence Interval | p-Value |
|---|---|---|---|
| Tumor size ≤1 cm vs. >1 cm | 1.425 | 0.712–2.853 | 0.318 |
| Multifocality Unifocal vs. multifocal | 2.604 | 1.441–4.705 | 0.002 |
| Cellularity Low vs. moderate/high | 1.446 | 0.680–3.077 | 0.338 |
| Atypical histiocytoid cells Absent vs. present | 2.717 | 1.468–5.029 | 0.001 |
| Multinucleated giant cells Absent/low vs. moderate/high | 3.070 | 1.109–8.497 | 0.031 |
| Variable | Atypical Histiocytoid Cells | ||
|---|---|---|---|
| Absent (n = 100) | Present (n = 122) | p-Value | |
| Cellularity | <0.001 | ||
| Low | 32 (32.0%) | 15 (12.3%) | |
| Moderate/high | 68 (68.0%) | 107 (87.7%) | |
| Isolated tumor cells | 0.002 | ||
| Absent/low | 77 (77.0%) | 70 (57.4%) | |
| Moderate/high | 23 (23.0%) | 52 (42.6%) | |
| Tall cells | <0.001 | ||
| Absent/low | 94 (94.0%) | 94 (77.0%) | |
| Moderate/high | 6 (6.0%) | 28 (23.0%) | |
| Multinucleated giant cells | <0.001 | ||
| Absent/low | 97 (97.0%) | 98 (80.3%) | |
| Moderate/high | 3 (3.0%) | 24 (19.7%) | |
| Macrophages | 0.277 | ||
| Absent/low | 88 (88.0%) | 101 (82.8%) | |
| Moderate/high | 12 (12.0%) | 21 (17.2%) | |
| Psammoma bodies | 0.352 | ||
| Absent | 97 (97.0%) | 114 (93.4%) | |
| Present | 3 (3.0%) | 8 (6.6%) | |
| BRAF V600E mutation 1 | 0.482 | ||
| Wild | 22/86 (25.6%) | 25/117 (21.4%) | |
| Mutant | 64/86 (74.4%) | 92/117 (78.6%) | |
| Variable | No. of Cases | Cervical Lymph Node Metastasis | ||
|---|---|---|---|---|
| Absent (n = 99) | Present (n = 65) | p-Value | ||
| Age (year, mean ± standard deviation) | 49.8 ± 12.5 | 50.7 ± 12.1 | 48.4 ± 13.0 | 0.255 |
| Sex | 0.525 | |||
| Male | 37 (22.6%) | 24 (24.2%) | 13 (20.0%) | |
| Female | 127 (77.4%) | 75 (75.8%) | 52 (80.0%) | |
| Multifocality | 0.080 | |||
| Unifocal | 87 (53.0%) | 58 (58.6%) | 29 (44.6%) | |
| Multifocal | 77 (47.0%) | 41 (41.4%) | 36 (55.4%) | |
| Cellularity | 0.269 | |||
| Low | 43 (26.2%) | 29 (29.3%) | 14 (21.5%) | |
| Moderate/high | 121 (73.8%) | 70 (70.7%) | 51 (78.5%) | |
| Isolated tumor cells | 0.682 | |||
| Absent/low | 114 (69.5%) | 70 (70.7%) | 44 (67.7%) | |
| Moderate/high | 50 (30.5%) | 29 (29.3%) | 21 (32.3%) | |
| Atypical histiocytoid cells | 0.005 | |||
| Absent | 80 (48.8%) | 57 (57.6%) | 23 (35.4%) | |
| Present | 84 (51.2%) | 42 (42.4%) | 42 (64.6%) | |
| Tall cells | 0.628 | |||
| Absent/low | 139 (84.8%) | 85 (85.9%) | 54 (83.1%) | |
| Moderate/high | 25 (15.2%) | 14 (14.1%) | 11 (16.9%) | |
| Multinucleated giant cells | 0.027 | |||
| Absent/low | 153 (93.3%) | 96 (97.0%) | 57 (87.7%) | |
| Moderate/high | 11 (6.7%) | 3 (3.0%) | 8 (12.3%) | |
| Macrophages | 0.628 | |||
| Absent/low | 139 (84.8%) | 85 (85.9%) | 54 (83.1%) | |
| Moderate/high | 25 (15.2%) | 14 (14.1%) | 11 (16.9%) | |
| Psammoma bodies | 0.485 | |||
| Absent | 155 (94.5%) | 95 (96.0%) | 60 (92.3%) | |
| Present | 9 (5.5%) | 4 (4.0%) | 5 (7.7%) | |
| BRAF V600E mutation 1 | 0.041 | |||
| Wild | 34 (22.8%) | 25 (28.7%) | 9 (14.5%) | |
| Mutant | 115 (77.2%) | 62 (71.3%) | 53 (85.5%) | |
| Characteristics | Odds Ratio | 95% Confidence Interval | p-Value |
|---|---|---|---|
| Multifocality Unifocal vs. multifocal | 2.415 | 1.205–4.842 | 0.013 |
| Cellularity Low vs. moderate/high | 1.134 | 0.517–2.487 | 0.754 |
| Atypical histiocytoid cells Absent vs. present | 2.761 | 1.350–5.648 | 0.005 |
| Multinucleated giant cells Absent/low vs. moderate/high | 3.703 | 0.908–15.106 | 0.068 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, J.E.; Bae, J.S.; Lim, D.-J.; Jung, S.L.; Jung, C.K. Atypical Histiocytoid Cells and Multinucleated Giant Cells in Fine-Needle Aspiration Cytology of the Thyroid Predict Lymph Node Metastasis of Papillary Thyroid Carcinoma. Cancers 2019, 11, 816. https://doi.org/10.3390/cancers11060816
Choi JE, Bae JS, Lim D-J, Jung SL, Jung CK. Atypical Histiocytoid Cells and Multinucleated Giant Cells in Fine-Needle Aspiration Cytology of the Thyroid Predict Lymph Node Metastasis of Papillary Thyroid Carcinoma. Cancers. 2019; 11(6):816. https://doi.org/10.3390/cancers11060816
Chicago/Turabian StyleChoi, Ji Eun, Ja Seong Bae, Dong-Jun Lim, So Lyung Jung, and Chan Kwon Jung. 2019. "Atypical Histiocytoid Cells and Multinucleated Giant Cells in Fine-Needle Aspiration Cytology of the Thyroid Predict Lymph Node Metastasis of Papillary Thyroid Carcinoma" Cancers 11, no. 6: 816. https://doi.org/10.3390/cancers11060816
APA StyleChoi, J. E., Bae, J. S., Lim, D. -J., Jung, S. L., & Jung, C. K. (2019). Atypical Histiocytoid Cells and Multinucleated Giant Cells in Fine-Needle Aspiration Cytology of the Thyroid Predict Lymph Node Metastasis of Papillary Thyroid Carcinoma. Cancers, 11(6), 816. https://doi.org/10.3390/cancers11060816