Mu Opioid Receptor 1 (MOR-1) Expression in Colorectal Cancer and Oncological Long-Term Outcomes: A Five-Year Retrospective Longitudinal Cohort Study

 , ,
, ,
Abstract
:
1. Introduction
2. Results
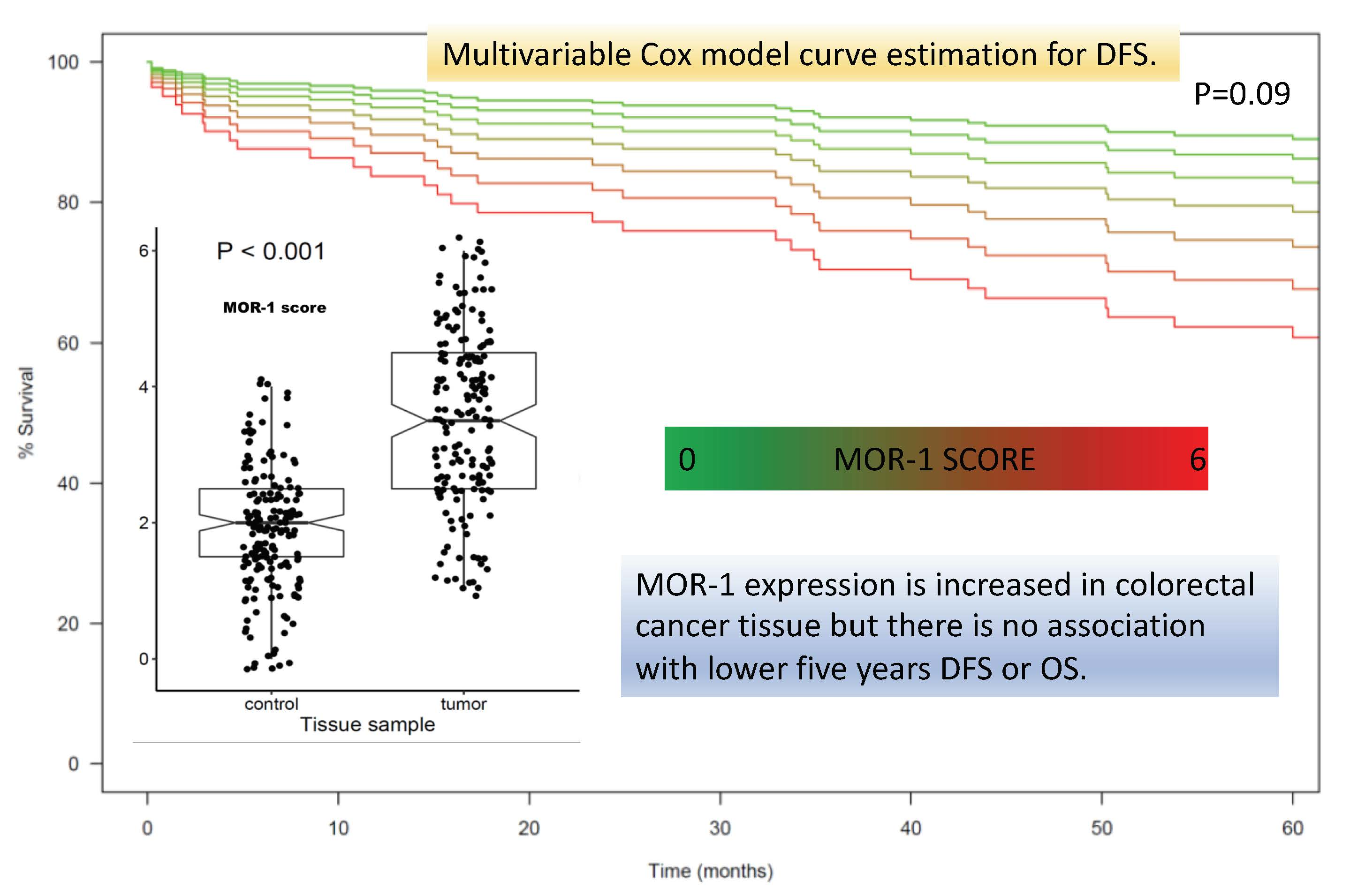
2.1. Expression of MOR-1
2.2. Association between MOR Expression and Long-Term Outcomes
2.3. Association between MOR-1 Expression and Postoperative Complications
3. Discussion
4. Materials and Methods
4.1. Study Population
4.2. Primary Outcome
4.3. Secondary Outcomes
4.4. Definitions
4.5. Data Collected
4.6. Sample Size Calculation
4.7. Analysis Plan
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Appendix A
Standard Operating Procedure (SOP) Immunohistochemical Analysis

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Positivity Percentage | Staining Intensity | |||
|---|---|---|---|---|
| No Staining | Weak | Moderate | Strong | |
| Negative (< 5%) | 0 | 1 | 2 | 3 |
| Sporadic (5%–25%) | 0 | 2 | 3 | 4 |
| Focal (25%–50%) | 0 | 3 | 4 | 5 |
| Diffuse (> 50%) | 0 | 4 | 5 | 6 |

References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sullivan, R.; Alatise, O.I.; Anderson, B.O.; Audisio, R.; Autier, P.; Aggarwal, A.; Balch, C.; Brennan, M.F.; Dare, A.; D’Cruz, A.; et al. Global cancer surgery: Delivering safe, affordable, and timely cancer surgery. Lancet Oncol. 2015, 16, 1193–1224. [Google Scholar] [CrossRef]
- Snyder, G.L.; Greenberg, S. Effect of anaesthetic technique and other perioperative factors on cancer recurrence. Br. J. Anaesth. 2010, 105, 106–115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Behrenbruch, C.; Shembrey, C.; Paquet-Fifield, S.; Mølck, C.; Cho, H.J.; Michael, M.; Thomson, B.N.J.; Heriot, A.G.; Hollande, F. Surgical stress response and promotion of metastasis in colorectal cancer: A complex and heterogeneous process. Clin. Exp. Metastasis 2018, 35, 333–345. [Google Scholar] [CrossRef]
- Chen, D.T.; Pan, J.H.; Chen, Y.H.; Xing, W.; Yan, Y.; Yuan, Y.F.; Zeng, W.A. The mu-opioid receptor is a molecular marker for poor prognosis in hepatocellular carcinoma and represents a potential therapeutic target. Br. J. Anaesth. 2019, 122, e157–e167. [Google Scholar] [CrossRef]
- Hiller, J.G.; Perry, N.J.; Poulogiannis, G.; Riedel, B.; Sloan, E.K. Perioperative events influence cancer recurrence risk after surgery. Nat. Rev. Clin. Oncol. 2018, 15, 205–218. [Google Scholar] [CrossRef]
- Byrne, K.; Levins, K.J.; Buggy, D.J. Can anesthetic-analgesic technique during primary cancer surgery affect recurrence or metastasis? Can. J. Anesth. 2016, 63, 184–192. [Google Scholar] [CrossRef]
- Missair, A.; Cata, J.P.; Votta-Velis, G.; Johnson, M.; Borgeat, A.; Tiouririne, M.; Gottumukkala, V.; Buggy, D.; Vallejo, R.; Marrero, E.B.; et al. Impact of perioperative pain management on cancer recurrence: An ASRA/ESRA special article. Reg. Anesth. Pain Med. 2019, 44, 13–28. [Google Scholar] [CrossRef] [PubMed]
- Wall, T.; Sherwin, A.; Ma, D.; Buggy, D.J. Influence of perioperative anaesthetic and analgesic interventions on oncological outcomes: A narrative review. Br. J. Anaesth. 2019, 123, 135–150. [Google Scholar] [CrossRef] [PubMed]
- Carlson, C.L. Effectiveness of the World Health Organization cancer pain relief guidelines: An integrative review. J. Pain Res. 2016, 9, 515–534. [Google Scholar] [CrossRef] [Green Version]
- Sekandarzad, M.W.; Van Zundert, A.A.J.; Lirk, P.B.; Doornebal, C.W.; Hollmann, M.W. Perioperative anesthesia care and tumor progression. Anesth. Analg. 2017, 124, 1697–1708. [Google Scholar] [CrossRef] [PubMed]
- Singleton, P.A.; Moss, J.; Karp, D.D.; Atkins, J.T.; Janku, F. The mu opioid receptor: A new target for cancer therapy? Cancer 2015, 121, 2681–2688. [Google Scholar] [CrossRef] [PubMed]
- Connolly, C.; Buggy, D.J. Opioids and tumour metastasis: Does the choice of the anesthetic-analgesic technique influence outcome after cancer surgery? Curr. Opin. Anaesthesiol. 2016, 29, 468–474. [Google Scholar] [CrossRef] [PubMed]
- Lennon, F.E.; Moss, J.; Singleton, P.A. The μ-Opioid Receptor in Cancer Progression—Is There a Direct Effect? Anesthesiology 2012, 116, 940–945. [Google Scholar] [CrossRef] [Green Version]
- Janku, F.; Johnson, L.K.; Karp, D.D.; Atkins, J.T.; Singleton, P.A.; Moss, J. Treatment with methylnaltrexone is associated with increased survival in patients with advanced cancer. Ann. Oncol. 2016, 27, 2032–2038. [Google Scholar] [CrossRef]
- Singleton, P.A.; Mirzapoiazova, T.; Hasina, R.; Salgia, R.; Moss, J. Increased μ-opioid receptor expression in metastatic lung cancer. Br. J. Anaesth. 2014, 113, 103–108. [Google Scholar] [CrossRef] [Green Version]
- Levins, K.J.; Prendeville, S.; Conlon, S.; Buggy, D.J. The effect of anesthetic technique on µ-opioid receptor expression and immune cell infiltration in breast cancer. Br. J. Anesth. 2018, 32, 792–796. [Google Scholar] [CrossRef] [Green Version]
- Zylla, D.; Gourley, B.L.; Vang, D.; Jackson, S.; Boatman, S.; Lindgren, B.; Kuskowski, M.A.; Le, C.; Gupta, K.; Gupta, P. Opioid requirement, opioid receptor expression, and clinical outcomes in patients with advanced prostate cancer. Cancer 2013, 119, 4103–4110. [Google Scholar] [CrossRef]
- Yao, Y.; Yao, R.; Zhuang, L.; Qi, W.; Lv, J.; Zhou, F.; Qiu, W.S.; Yue, L. MOR1 Expression in Gastric Cancer: A Biomarker Associated With Poor Outcome. Clin. Transl. Sci. 2015, 8, 137–142. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.F.; Xu, Q.X.; Liao, L.D.; Xu, X.E.; Wu, J.Y.; Wu, Z.Y.; Shen, J.H.; Li, E.M.; Xu, L.Y. Association of mu-opioid receptor expression with lymph node metastasis in esophageal squamous cell carcinoma. Dis. Esophagus 2015, 28, 196–203. [Google Scholar] [CrossRef]
- Nylund, G.; Pettersson, A.; Bengtsson, C.; Khorram-Manesh, A.; Nordgren, S.; Delbro, D.S. Functional expression of μ-opioid receptors in the human colon cancer cell line, HT-29, and their localization in human colon. Dig. Dis. Sci. 2008, 53, 461–466. [Google Scholar] [CrossRef] [PubMed]
- Diaz-Cambronero, O.; Mazzinari, G.; Cata, J.P. Perioperative opioids and colorectal cancer recurrence: A systematic review of the literature. Pain Manag. 2018, 8, 353–361. [Google Scholar] [CrossRef] [PubMed]
- Dorcaratto, D.; Mazzinari, G.; Fernandez, M.; Muñoz, E.; Garcés-Albir, M.; Ortega, J.; Sabater, L. Impact of Postoperative Complications on Survival and Recurrence After Resection of Colorectal Liver Metastases: Systematic Review and Meta-analysis. Ann. Surg. 2019, 270, 1018–1027. [Google Scholar] [CrossRef] [PubMed]
- Sinn, H.P.; Schneeweiss, A.; Keller, M.; Schlombs, K.; Laible, M.; Seitz, J.; Lakis, S.; Veltrup, E.; Altevogt, P.; Eidt, S.; et al. Comparison of immunohistochemistry with PCR for assessment of ER, PR, and Ki-67 and prediction of pathological complete response in breast cancer. BMC Cancer 2017, 17, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Zhu, G.J.; Xu, C.W.; Fang, M.Y.; Zhang, Y.P.; Li, Y. Detection of Her-2/neu expression in gastric cancer: Quantitative PCR versus immunohistochemistry. Exp. Ther. Med. 2014, 8, 1501–1507. [Google Scholar] [CrossRef]
- Shabalina, S.A.; Zaykin, D.V.; Gris, P.; Ogurtsov, A.Y.; Gauthier, J.; Shibata, K.; Tchivileva, I.E.; Belfer, I.; Mishra, B.; Kiselycznyk, C.; et al. Expansion of the human μ-opioid receptor gene architecture: Novel functional variants. Hum. Mol. Genet. 2009, 18, 1037–1051. [Google Scholar] [CrossRef]
- Fukuda, K.; Hayashida, M.; Ide, S.; Saita, N.; Kokita, Y.; Kasai, S.; Nishizawa, D.; Ogai, Y.; Hasegawa, J.; Nagashima, M.; et al. Association between OPRM1 gene polymorphisms and fentanyl sensitivity in patients undergoing painful cosmetic surgery. Pain 2009, 147, 194–201. [Google Scholar] [CrossRef]
- Bortsov, A.V.; Millikan, R.C.; Belfer, I.; Boortz-Marx, R.L.; Arora, H.; McLean, S.A. μ-Opioid receptor gene A118G polymorphism predicts survival in patients with breast cancer. Anesthesiology 2012, 116, 896–902. [Google Scholar] [CrossRef] [Green Version]
- Xu, X.; Mao, B.; Wu, L.; Liu, L.; Rui, J.; Chen, G. A118G Polymorphism in μ-Opioid Receptor Gene and Interactions with Smoking and Drinking on Risk of Oesophageal Squamous Cell Carcinoma. J. Clin. Lab. Anal. 2017, 31, e22018. [Google Scholar] [CrossRef] [Green Version]
- Oh, T.K.; Kim, K.; Jheon, S.H.; Do, S.H.; Hwang, J.W.; Jeon, Y.T.; Kim, K.; Song, I.A. Long-Term Oncologic Outcomes, Opioid Use, and Complications after Esophageal Cancer Surgery. J. Clin. Med. 2018, 7, 33. [Google Scholar] [CrossRef] [Green Version]
- Cieślińska, A.; Sienkiewicz-Szłapka, E.; Kostyra, E.; Fiedorowicz, E.; Snarska, J.; Wroński, K.; Tenderenda, M.; Jarmołowska, B.; Matysiewicz, M. μ-Opioid receptor gene (OPRM1) polymorphism in patients with breast cancer. Tumor Biol. 2015, 36, 4655–4660. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, S.; Li, Y.; Liu, X.D.; Zhao, C.X.; Yang, K.Q. Polymorphism of A118G in μ-opioid receptor gene is associated with risk of esophageal squamous cell carcinoma in a Chinese population. Int. J. Clin. Oncol. 2013, 18, 666–669. [Google Scholar] [CrossRef] [PubMed]
- Harimaya, Y.; Koizumi, K.; Andoh, T.; Nojima, H.; Kuraishi, Y.; Saiki, I. Potential ability of morphine to inhibit the adhesion, invasion and metastasis of metastatic colon 26-L5 carcinoma cells. Cancer Lett. 2002, 187, 121–127. [Google Scholar] [CrossRef]
- Min, T.J.; Park, S.H.; Ji, Y.H.; Lee, Y.S.; Kim, T.W.; Kim, J.H.; Kim, W.Y.; Park, Y.C. Morphine attenuates endothelial cell adhesion molecules induced by the supernatant of LPS-stimulated colon cancer cells. J. Korean Med. Sci. 2011, 26, 747–752. [Google Scholar] [CrossRef]
- Tegeder, I.; Geisslinger, G. Opioids as modulators of cell death and survival—Unraveling mechanisms and revealing new indications. Pharmacol. Rev. 2004, 56, 351–369. [Google Scholar] [CrossRef] [Green Version]
- Yeager, M.P.; Colacchio, T.A. Effect of Morphine on Growth of Metastatic Colon Cancer In Vivo. Arch. Surg. 1991, 126, 454–456. [Google Scholar] [CrossRef]
- Neudeck, B.L.; Loeb, J.M. Endomorphin-1 alters interleukin-8 secretion in Caco-2 cells via a receptor mediated process. Immunol. Lett. 2002, 84, 217–221. [Google Scholar] [CrossRef]
- Cata, J.P.; Keerty, V.; Keerty, D.; Feng, L.; Norman, P.H.; Gottumukkala, V.; Mehran, J.R.; Engle, M. A retrospective analysis of the effect of intraoperative opioid dose on cancer recurrence after non-small cell lung cancer resection. Cancer Med. 2014, 3, 900–908. [Google Scholar] [CrossRef]
- Du, K.N.; Feng, L.; Newhouse, A.; Mehta, J.; Lasala, J.; Mena, G.E.; Hofstetter, W.L.; Cata, J.P. Effects of intraoperative opioid use on recurrence-free and overall survival in patients with esophageal adenocarcinoma and squamous cell carcinoma. Anesth. Analg. 2018, 127, 210–216. [Google Scholar] [CrossRef]
- Wu, H.L.; Tai, Y.H.; Chang, W.K.; Chang, K.Y.; Tsou, M.Y.; Cherng, Y.G.; Cherng, Y.G.; Lin, S.P. Does postoperative morphine consumption for acute surgical pain impact oncologic outcomes after colorectal cancer resection?: A retrospective cohort study. Medicine 2019, 98, e15442. [Google Scholar] [CrossRef]
- Jammer, I.; Wickboldt, N.; Sander, M.; Smith, A.; Schultz, M.J.; Pelosi, P.; Leva, B.; Rhodes, A.; Hoeft, A.; Walder, B.; et al. Standards for definitions and use of outcome measures for clinical effectiveness research in perioperative medicine: European Perioperative Clinical Outcome (EPCO) definitions: A statement from the ESA-ESICM joint taskforce on perioperative outcome measur. Eur. J. Anaesthesiol. 2015, 32, 88–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gammaitoni, A.R.; Fine, P.; Alvarez, N.; McPherson, M.L.; Bergmark, S. Clinical application of opioid equianalgesic data. Clin. J. Pain 2003, 19, 286–297. [Google Scholar] [CrossRef] [PubMed]
- Ternès, N.; Rotolo, F.; Michiels, S. Empirical extensions of the lasso penalty to reduce the false discovery rate in high-dimensional Cox regression models. Stat. Med. 2016, 35, 2561–2573. [Google Scholar] [CrossRef] [PubMed]



| Variable | N = (174) |
|---|---|
| Age (years) | 70.5 (11.4) |
| Gender (female) | 42.0% (73) |
| Complication in the first 28 postoperative days | 18.4% (32) |
| Anesthetic agent (N = 166) | |
| Halogenated | 75.3% (125) |
| Intravenous | 20.5% (34) |
| Both | 4.2% (7) |
| Intraoperative remifentanil perfusion (N = 169) | 47.9% (81) |
| First postoperative 96 h total opioid dose | 76.43 (34.76) |
| Intraoperative epidural analgesia (Yes) | 16.1% (28) |
| Red blood cell transfusion in the first postoperative 96 h | 30.5% (53) |
| CEA value at diagnosis (N = 163) (U∙mL−1) | 2.60 [1.60–5.10] |
| Surgical duration (min) | 217.52 (88.22) |
| Preoperative total proteins (g∙dL−1) | 7.00 [6.00–7.00] |
| Preoperative Hemoglobin value (g∙dL−1) | 12.03 (2.07) |
| Number of affected lymph nodes | 0 [0–2] |
| Preoperative chemotherapy (Yes) | 10.3% (18) |
| Preoperative radiotherapy (Yes) | 9.8% (17) |
| Postoperative chemotherapy (Yes) | 50.0% (87) |
| Postoperative radiotherapy (Yes) | 1.7% (3) |
| ASA score (N = 157) | |
| 1 | 7.6% (12) |
| 2 | 54.8% (86) |
| 3 | 33.8% (53) |
| 4 | 3.8% (6) |
| HTA (Yes) | 54.6% (95) |
| Diabetes Mellitus (Yes) | 19.5% (34) |
| Reintervention Yes) | 6.3% (11) |
| Readmission (Yes) | 3.4% (6) |
| Dukes (N = 153) | |
| A | 1.3% (2) |
| B | 51.0% (78) |
| C | 46.4% (71) |
| D | 1.3% (2) |
| Cancer Staging (III) | 44.8% (78) |
| Ca 19–9 value at diagnosis (U∙mL−1) (N = 124) | 11.1 [5.3–18.5] |
| Resection margins (R+) (N = 135) | 19% (25) |
| Tumoral tissue differentiation (N = 169) | |
| Poor/Undifferentiated | 12.0% (20) |
| Moderately differentiated | 78% (132) |
| Well differentiated | 10.0% (17) |
| Outcome of interest | Complete Cases Model | Missing Data Multiple Imputation | ||||
|---|---|---|---|---|---|---|
| Disease Free Survival Model | N = 135 Events = 30 | N = 174 Events = 40 | ||||
| Hazard Ratio | Lower-Upper 95% CI | p-value | Hazard Ratio | Lower-Upper 95% CI | p-value | |
| MOR expression | 0.791 | 0.603–1.039 | 0.092 | 1.062 | 0.930–1.212 | 0.376 |
| First postoperative 96 h transfusion (yes) | 0.991 | 0.392–2.503 | 0.985 | 1.060 | 0.701–1.603 | 0.784 |
| ASA (Reference category = 1) | ||||||
| 2 | 0.707 | 0.155–3.223 | 0.654 | 0.854 | 0.427–1.710 | 0.657 |
| 3 | 0.936 | 0.195–4.481 | 0.934 | 0.994 | 0.475–2.080 | 0.986 |
| 4 | 1.322 | 0.159–11.007 | 0.796 | 0.517 | 0.129–2.069 | 0.351 |
| Preoperative Hemoglobin (g∙dL−1) | 1.043 | 0.846–1.287 | 0.693 | 1.012 | 0.919–1.117 | 0.807 |
| Number of affected lymph nodes | 1.283 | 0.921–1.788 | 0.141 | 1.028 | 0.780–1.322 | 0.828 |
| CEA at diagnosis (U∙mL−1) | 1.811 | 1.245–2.635 | 0.002 | 1.058 | 0.877–1.28 | 0.557 |
| Age (years) | 1.010 | 0.970–1.052 | 0.638 | 1.005 | 0.987–1.022 | 0.591 |
| Overall survival model | N = 135 Events = 29 | N = 174 Events = 40 | ||||
| MOR-1 expression | 1.023 | 0.784–1.335 | 0.869 | 1.031 | 0.906–1.173 | 0.645 |
| First postoperative 96 h transfusion (yes) | 1.556 | 0.658–3.682 | 0.314 | 1.004 | 0.670–1.503 | 0.986 |
| ASA score (Reference category = 1) | ||||||
| 2 | 0.954 | 0.119–7.629 | 0.965 | 0.898 | 0.479–1.685 | 0.737 |
| 3 | 1.948 | 0.247–15.357 | 0.527 | 1.072 | 0.538–2.138 | 0.843 |
| 4 | 2.375 | 0.208–27.07 | 0.486 | 0.832 | 0.183–3.786 | 0.812 |
| Preoperative Hemoglobin (g∙dL−1) | 0.911 | 0.729–1.139 | 0.415 | 1.016 | 0.925–1.115 | 0.743 |
| Number of affected lymph nodes | 1.482 | 1.110–1.978 | 0.008 | 0.971 | 0.774–1.218 | 0.800 |
| CEA at diagnosis (U∙mL−1) | 1.485 | 1.017–2.170 | 0.041 | 1.031 | 0.859–1.24 | 0.746 |
| Age (years) | 1.031 | 0.989–1.074 | 0.147 | 1.003 | 0.986–1.020 | 0.746 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Díaz-Cambronero, O.; Mazzinari, G.; Giner, F.; Belltall, A.; Ruiz-Boluda, L.; Marqués-Marí, A.; Sánchez-Guillén, L.; Eroles, P.; Cata, J.P.; Argente-Navarro, M.P. Mu Opioid Receptor 1 (MOR-1) Expression in Colorectal Cancer and Oncological Long-Term Outcomes: A Five-Year Retrospective Longitudinal Cohort Study. Cancers 2020, 12, 134. https://doi.org/10.3390/cancers12010134
Díaz-Cambronero O, Mazzinari G, Giner F, Belltall A, Ruiz-Boluda L, Marqués-Marí A, Sánchez-Guillén L, Eroles P, Cata JP, Argente-Navarro MP. Mu Opioid Receptor 1 (MOR-1) Expression in Colorectal Cancer and Oncological Long-Term Outcomes: A Five-Year Retrospective Longitudinal Cohort Study. Cancers. 2020; 12(1):134. https://doi.org/10.3390/cancers12010134
Chicago/Turabian StyleDíaz-Cambronero, Oscar, Guido Mazzinari, Francisco Giner, Amparo Belltall, Lola Ruiz-Boluda, Anabel Marqués-Marí, Luis Sánchez-Guillén, Pilar Eroles, Juan Pablo Cata, and María Pilar Argente-Navarro. 2020. "Mu Opioid Receptor 1 (MOR-1) Expression in Colorectal Cancer and Oncological Long-Term Outcomes: A Five-Year Retrospective Longitudinal Cohort Study" Cancers 12, no. 1: 134. https://doi.org/10.3390/cancers12010134
APA StyleDíaz-Cambronero, O., Mazzinari, G., Giner, F., Belltall, A., Ruiz-Boluda, L., Marqués-Marí, A., Sánchez-Guillén, L., Eroles, P., Cata, J. P., & Argente-Navarro, M. P. (2020). Mu Opioid Receptor 1 (MOR-1) Expression in Colorectal Cancer and Oncological Long-Term Outcomes: A Five-Year Retrospective Longitudinal Cohort Study. Cancers, 12(1), 134. https://doi.org/10.3390/cancers12010134