Evaluation of Vascular Patterns Using Contact Endoscopy and Narrow-Band Imaging (CE-NBI) for the Diagnosis of Vocal Fold Malignancy

 , , , ,
, , , ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Reported Prevalence of PVC-Positive Lesions in Different Groups of Histological Diagnoses
3.2. Association of the Detection of PVC to Different Groups of Histological Diagnoses
3.3. Sensitivity, Specificity, and Positive and Negative Predictive Values in the Diagnosis of Malignant and Premalignant Laryngeal Lesions
3.4. Interobserver Agreement in the Identification of PVC in NBI-CE
4. Discussion
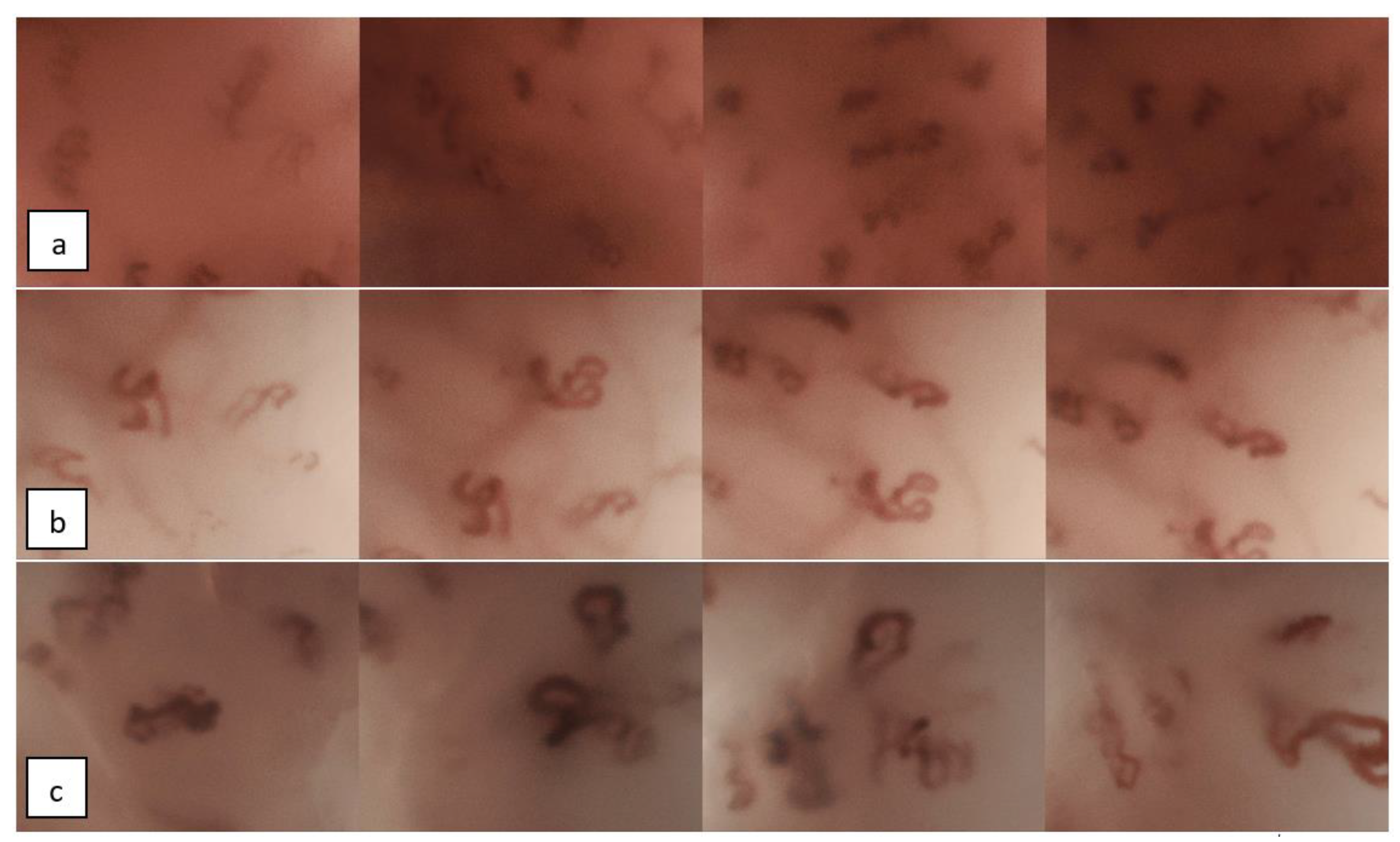
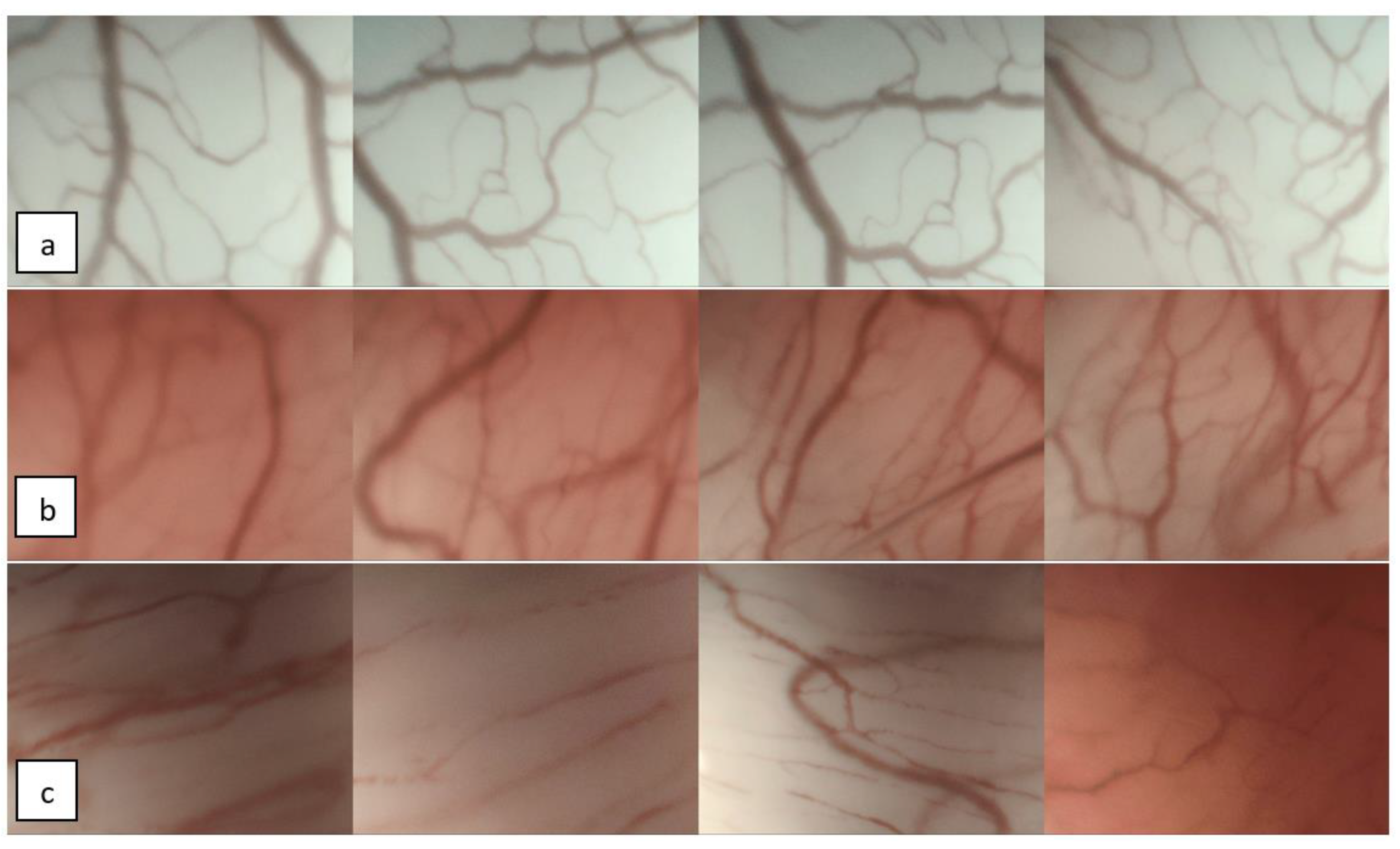
4.1. Endoscopic Evaluation of Vascular Patterns of the Vocal Folds
4.2. ELS Classification for Vascular Changes of the Vocal Folds
4.3. Key Findings of the Present Study in Relation to Previous Research
4.4. Implications and Suggestions for Future Research
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Watanabe, A.; Taniguchi, M.; Tsujie, H.; Hosokawa, M.; Fujita, M.; Sasaki, S. The value of narrow band imaging endoscope for early head and neck cancers. Otolaryngol. Head Neck Surg. 2008, 138, 446–451. [Google Scholar] [CrossRef]
- Piazza, C.; Cocco, D.; de Benedetto, L.; Del Bon, F.; Nicolai, P.; Peretti, G. Narrow band imaging and high definition television in the assessment of laryngeal cancer: A prospective study on 279 patients. Eur. Arch. Otorhinolaryngol. 2010, 267, 409–414. [Google Scholar] [CrossRef] [PubMed]
- Tjon Pian Gi, R.E.A.; Halmos, G.B.; van Hemel, B.M.; van den Heuvel, E.R.; van der Laan, B.F.A.M.; Plaat, B.E.C.; Dikkers, F.G. Narrow band imaging is a new technique in visualization of recurrent respiratory papillomatosis. Laryngoscope 2012, 122, 1826–1830. [Google Scholar] [CrossRef] [PubMed]
- Ni, X.-G.; He, S.; Xu, Z.-G.; Gao, L.; Lu, N.; Yuan, Z.; Lai, S.-Q.; Zhang, Y.-M.; Yi, J.-L.; Wang, X.-L.; et al. Endoscopic diagnosis of laryngeal cancer and precancerous lesions by narrow band imaging. J. Laryngol. Otol. 2011, 125, 288–296. [Google Scholar] [CrossRef] [PubMed]
- Puxeddu, R.; Sionis, S.; Gerosa, C.; Carta, F. Enhanced contact endoscopy for the detection of neoangiogenesis in tumors of the larynx and hypopharynx. Laryngoscope 2015, 125, 1600–1606. [Google Scholar] [CrossRef]
- Arens, C.; Piazza, C.; Andrea, M.; Dikkers, F.G.; Tjon Pian Gi, R.E.A.; Voigt-Zimmermann, S.; Peretti, G. Proposal for a descriptive guideline of vascular changes in lesions of the vocal folds by the committee on endoscopic laryngeal imaging of the European Laryngological Society. Eur. Arch. Otorhinolaryngol. 2016, 273, 1207–1214. [Google Scholar] [CrossRef]
- Mehlum, C.S.; Rosenberg, T.; Dyrvig, A.-K.; Groentved, A.M.; Kjaergaard, T.; Godballe, C. Can the Ni classification of vessels predict neoplasia? A systematic review and meta-analysis. Laryngoscope 2018, 128, 168–176. [Google Scholar] [CrossRef]
- Šifrer, R.; Rijken, J.A.; Leemans, C.R.; Eerenstein, S.E.J.; van Weert, S.; Hendrickx, J.-J.; Bloemena, E.; Heuveling, D.A.; Rinkel, R.N.P.M. Evaluation of vascular features of vocal cords proposed by the European Laryngological Society. Eur. Arch. Otorhinolaryngol. 2018, 275, 147–151. [Google Scholar] [CrossRef] [Green Version]
- Andrea, M.; Dias, O.; Santos, A. Contact endoscopy during microlaryngeal surgery: A new technique for endoscopic examination of the larynx. Ann. Otol. Rhinol. Laryngol. 1995, 104, 333–339. [Google Scholar] [CrossRef]
- Arens, C.; Voigt-Zimmermann, S. Kontaktendoskopie der Stimmlippen in Kombination mit Narrow-Band-Imaging (Kompaktendoskopie). Laryngorhinootologie 2015, 94, 150–152. [Google Scholar] [CrossRef]
- Piazza, C.; Del Bon, F.; Peretti, G.; Nicolai, P. Narrow band imaging in endoscopic evaluation of the larynx. Curr. Opin. Otolaryngol. Head Neck Surg. 2012, 20, 472–476. [Google Scholar] [CrossRef] [PubMed]
- Lukes, P.; Zabrodsky, M.; Lukesova, E.; Chovanec, M.; Astl, J.; Betka, J.A.; Plzak, J. The role of NBI HDTV magnifying endoscopy in the prehistologic diagnosis of laryngeal papillomatosis and spinocellular cancer. Biomed Res. Int. 2014, 2014. [Google Scholar] [CrossRef] [PubMed]
- Gale, N.; Hille, J.; Jordan, R.C.; Nadal, A.; Williams, M.D. Regarding Laryngeal precursor lesions: Interrater and intrarater reliability of histopathological assessment. Laryngoscope 2019, 129, E91–E92. [Google Scholar] [CrossRef] [PubMed]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davaris, N.; Voigt-Zimmermann, S.; Roessner, A.; Arens, C. “Narrow band imaging” zur Beurteilung laryngealer Schleimhautläsionen. HNO 2017, 65, 527–542. [Google Scholar] [CrossRef]
- Zwakenberg, M.A.; Dikkers, F.G.; Wedman, J.; Halmos, G.B.; van der Laan, B.F.A.M.; Plaat, B.E.C. Narrow band imaging improves observer reliability in evaluation of upper aerodigestive tract lesions. Laryngoscope 2016, 126, 2276–2281. [Google Scholar] [CrossRef]
- Davaris, N.; Voigt-Zimmermann, S.; Kropf, S.; Arens, C. Flexible transnasal endoscopy with white light or narrow band imaging for the diagnosis of laryngeal malignancy: Diagnostic value, observer variability and influence of previous laryngeal surgery. Eur. Arch. Otorhinolaryngol. 2019, 276, 459–466. [Google Scholar] [CrossRef] [Green Version]
- Mehlum, C.S.; Kjaergaard, T.; Grøntved, Å.M.; Lyhne, N.M.; Jørkov, A.P.S.; Homøe, P.; Tvedskov, J.F.; Bork, K.H.; Möller, S.; Jørgensen, G.; et al. Value of pre- and intraoperative diagnostic methods in suspected glottic neoplasia. Eur. Arch. Otorhinolaryngol. 2019. [Google Scholar] [CrossRef]
- Mannelli, G.; Cecconi, L.; Gallo, O. Laryngeal preneoplastic lesions and cancer: Challenging diagnosis. Qualitative literature review and meta-analysis. Crit. Rev. Oncol. Hematol. 2016, 106, 64–90. [Google Scholar] [CrossRef]
- Sun, C.; Han, X.; Li, X.; Zhang, Y.; Du, X. Diagnostic Performance of Narrow Band Imaging for Laryngeal Cancer: A Systematic Review and Meta-analysis. Otolaryngol. Head Neck Surg. 2017, 156, 589–597. [Google Scholar] [CrossRef]
- Rzepakowska, A.; Żurek, M.; Grzybowski, J.; Pihowicz, P.; Górnicka, B.; Osuch-Wójcikiewicz, E.; Niemczyk, K. Correlation of narrow band imaging vascular patterns with immunohistological microvessel density in vocal fold lesions. Braz. J. Otorhinolaryngol. 2019. [Google Scholar] [CrossRef] [PubMed]
- Hosono, H.; Katada, C.; Okamoto, T.; Ichinoe, M.; Sakamoto, Y.; Matsuba, H.; Kano, K.; Ishido, K.; Tanabe, S.; Koizumi, W.; et al. Usefulness of narrow band imaging with magnifying endoscopy for the differential diagnosis of cancerous and noncancerous laryngeal lesions. Head Neck 2019, 41, 2555–2560. [Google Scholar] [CrossRef] [PubMed]
- Arens, C.; Glanz, H.; Dreyer, T.; Malzahn, K. Compact endoscopy of the larynx. Ann. Otol. Rhinol. Laryngol. 2003, 112, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Ni, X.-G.; Zhu, J.-Q.; Zhang, Q.-Q.; Zhang, B.-G.; Wang, G.-Q. Diagnosis of vocal cord leukoplakia: The role of a novel narrow band imaging endoscopic classification. Laryngoscope 2019, 129, 429–434. [Google Scholar] [CrossRef]
- Nogués-Sabaté, A.; Aviles-Jurado, F.X.; Ruiz-Sevilla, L.; Lehrer, E.; Santamaría-Gadea, A.; Valls-Mateus, M.; Vilaseca, I. Intra and interobserver agreement of narrow band imaging for the detection of head and neck tumors. Eur. Arch. Otorhinolaryngol. 2018, 275, 2349–2354. [Google Scholar] [CrossRef]
- De Vito, A.; Meccariello, G.; Vicini, C. Narrow band imaging as screening test for early detection of laryngeal cancer: A prospective study. Clin. Otolaryngol. 2017, 42, 347–353. [Google Scholar] [CrossRef]
- Volgger, V.; Felicio, A.; Lohscheller, J.; Englhard, A.S.; Al-Muzaini, H.; Betz, C.S.; Schuster, M.E. Evaluation of the combined use of narrow band imaging and high-speed imaging to discriminate laryngeal lesions. Lasers Surg. Med. 2017, 49, 609–618. [Google Scholar] [CrossRef]
- Alagappan, M.; Brown, J.R.G.; Mori, Y.; Berzin, T.M. Artificial intelligence in gastrointestinal endoscopy: The future is almost here. World J. Gastrointest. Endosc. 2018, 10, 239–249. [Google Scholar] [CrossRef]
- Esmaeili, N.; Illanes, A.; Boese, A.; Davaris, N.; Arens, C.; Friebe, M. Novel automated vessel pattern characterization of larynx contact endoscopic video images. Int. J. Comput. Assist. Radiol. Surg. 2019, 14, 1751–1761. [Google Scholar] [CrossRef] [Green Version]
- Irem Turkmen, H.; Elif Karsligil, M.; Kocak, I. Classification of laryngeal disorders based on shape and vascular defects of vocal folds. Comput. Biol. Med. 2015, 62, 76–85. [Google Scholar] [CrossRef]
- Moccia, S.; de Momi, E.; Guarnaschelli, M.; Savazzi, M.; Laborai, A.; Guastini, L.; Peretti, G.; Mattos, L.S. Confident texture-based laryngeal tissue classification for early stage diagnosis support. J. Med. Imaging (Bellingham) 2017, 4. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Histological Diagnosis | No. of Lesions | Experienced Observers | Less-Experienced Observers |
|---|---|---|---|
| SCC 1 | 8 | 87.5% | 62.5% |
| Dysplasia | 17 | 88.2% | 70.6% |
| Papillomatosis | 11 | 100.0% | 90.9% |
| Other benign lesions | 32 | 15.6% | 21.9% |
| Experienced Observers | Less-Experienced Observers | |||
|---|---|---|---|---|
| 95%–CI 1 | 95%–CI 1 | |||
| Sensitivity | 0.955 | 0.905–1.004 | 0.727 | 0.621–0.833 |
| Specificity | 0.630 | 0.516–0.745 | 0.609 | 0.493–0.725 |
| PPV 2 | 0.553 | 0.434–0.671 | 0.471 | 0.352–0.589 |
| NPV 3 | 0.967 | 0.924–1.009 | 0.824 | 0.733–0.914 |
| Observers | Fleiss’ Kappa | 95%–CI 1 | Agreement According to [14] |
|---|---|---|---|
| Experienced | 0.920 | 0.783–1.058 | almost perfect |
| Less Experienced | 0.510 | 0.373–0.647 | moderate |
| Overall | 0.703 | 0.642–0.764 | substantial |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Davaris, N.; Lux, A.; Esmaeili, N.; Illanes, A.; Boese, A.; Friebe, M.; Arens, C. Evaluation of Vascular Patterns Using Contact Endoscopy and Narrow-Band Imaging (CE-NBI) for the Diagnosis of Vocal Fold Malignancy. Cancers 2020, 12, 248. https://doi.org/10.3390/cancers12010248
Davaris N, Lux A, Esmaeili N, Illanes A, Boese A, Friebe M, Arens C. Evaluation of Vascular Patterns Using Contact Endoscopy and Narrow-Band Imaging (CE-NBI) for the Diagnosis of Vocal Fold Malignancy. Cancers. 2020; 12(1):248. https://doi.org/10.3390/cancers12010248
Chicago/Turabian StyleDavaris, Nikolaos, Anke Lux, Nazila Esmaeili, Alfredo Illanes, Axel Boese, Michael Friebe, and Christoph Arens. 2020. "Evaluation of Vascular Patterns Using Contact Endoscopy and Narrow-Band Imaging (CE-NBI) for the Diagnosis of Vocal Fold Malignancy" Cancers 12, no. 1: 248. https://doi.org/10.3390/cancers12010248
APA StyleDavaris, N., Lux, A., Esmaeili, N., Illanes, A., Boese, A., Friebe, M., & Arens, C. (2020). Evaluation of Vascular Patterns Using Contact Endoscopy and Narrow-Band Imaging (CE-NBI) for the Diagnosis of Vocal Fold Malignancy. Cancers, 12(1), 248. https://doi.org/10.3390/cancers12010248