Frontiers of Robotic Gastroscopy: A Comprehensive Review of Robotic Gastroscopes and Technologies

 ,
,  , ,
, ,  ,
,  ,
,  and
and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:Simple Summary
Abstract
1. Introduction
2. Commercially Available Gastroscopes: Conventional Instruments and Robotic Platforms
2.1. Diagnosis of UGI Malignant and Non-Malignant Lesions with Conventional Gastroscopes
2.2. Gastric Capsule Endoscopes
2.2.1. UGI Motility-Actuated Capsule Gastroscopes
2.2.2. Externally Actuated Capsule Gastroscopes
3. Research-Oriented Robotic Gastroscopes: Innovative Smart Devices for Upper-GI Tract
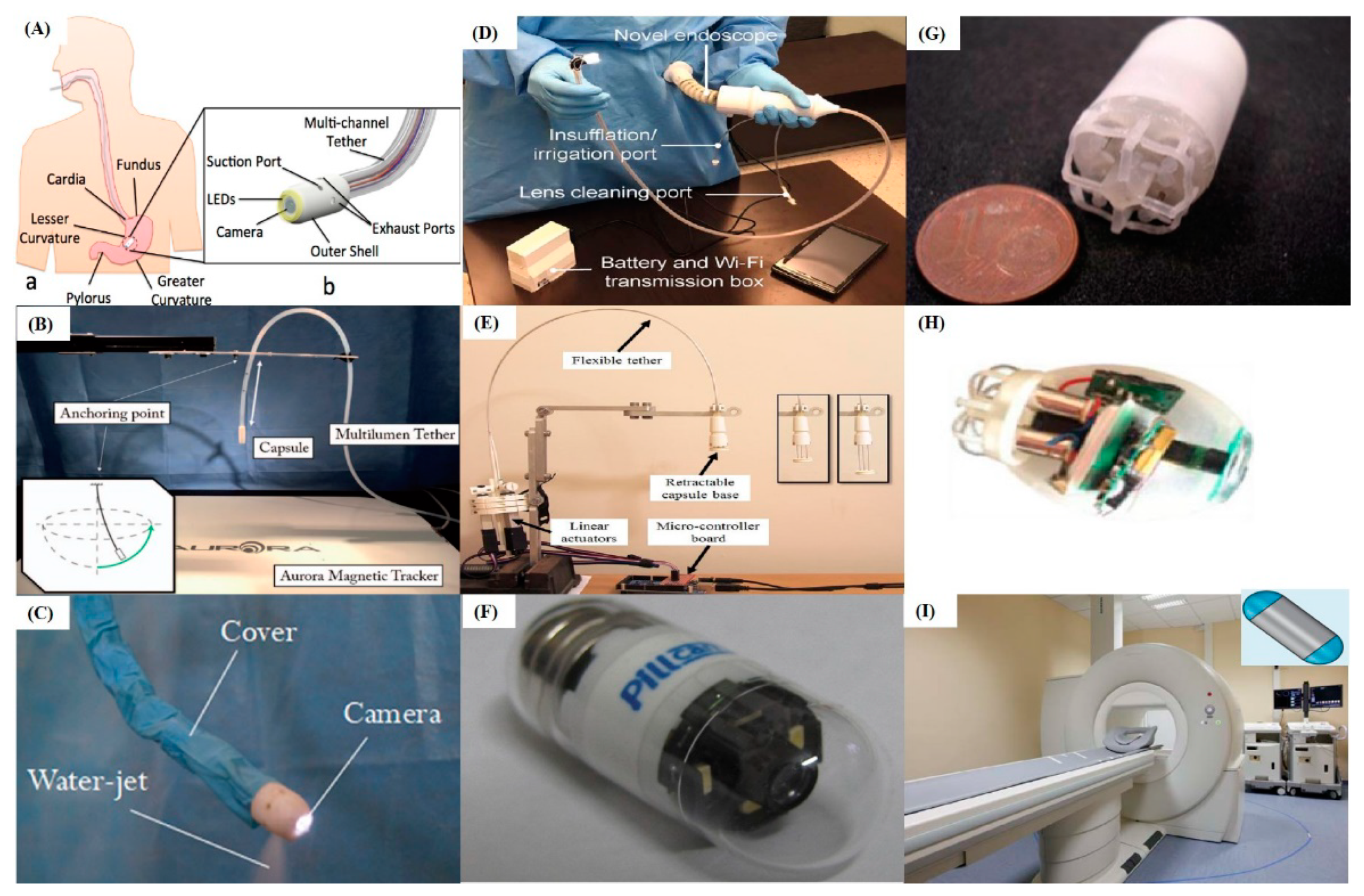
3.1. Tethered Capsule-Like Gastroscopes
3.2. Wireless Capsule Gastroscopes
4. Novel Flexible Robots for UGI Surgery
4.1. Gastric Surgery
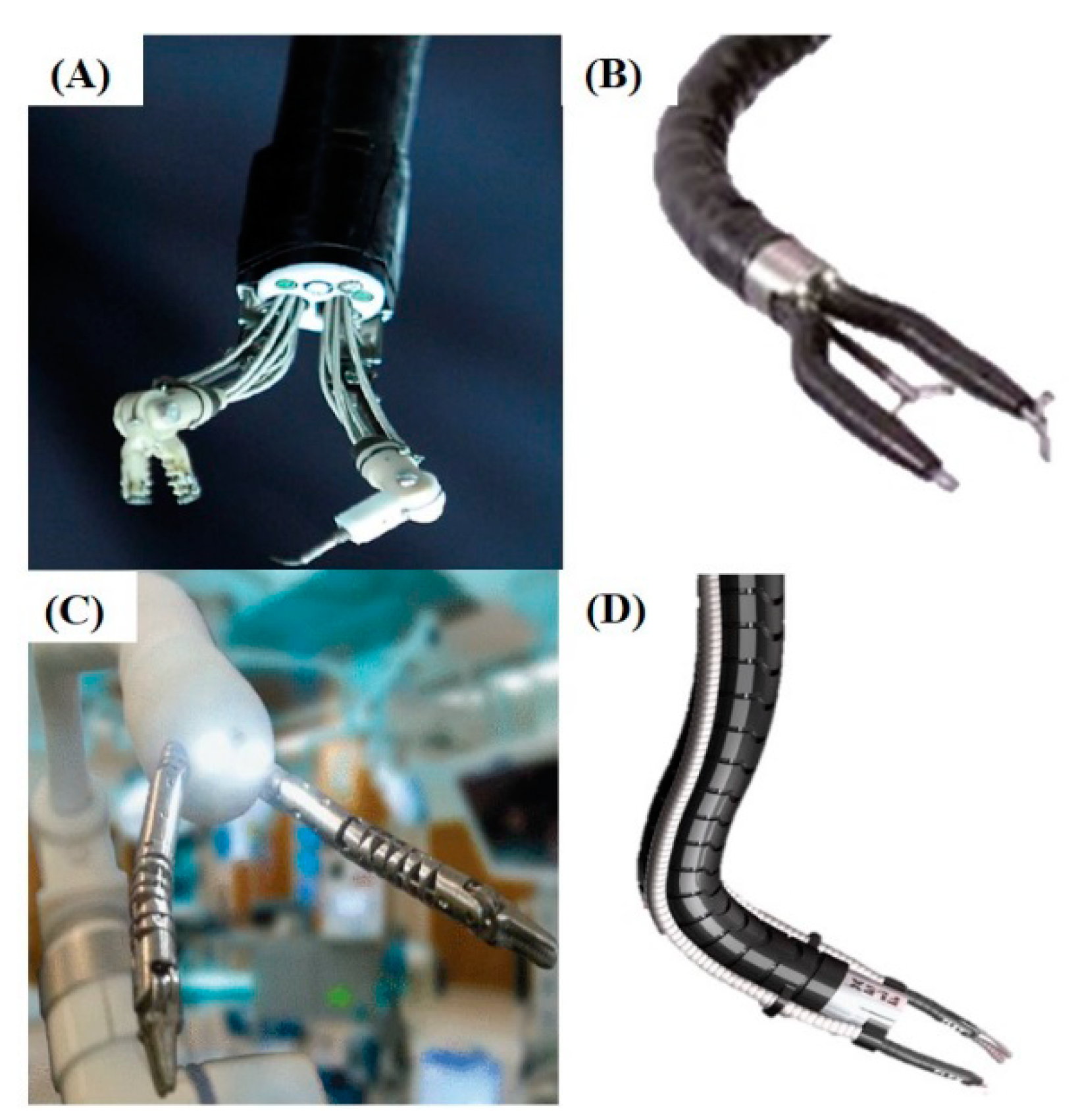
4.2. Novel Flexible Surgical Robots
5. Artificial Intelligence in Gastroscopy
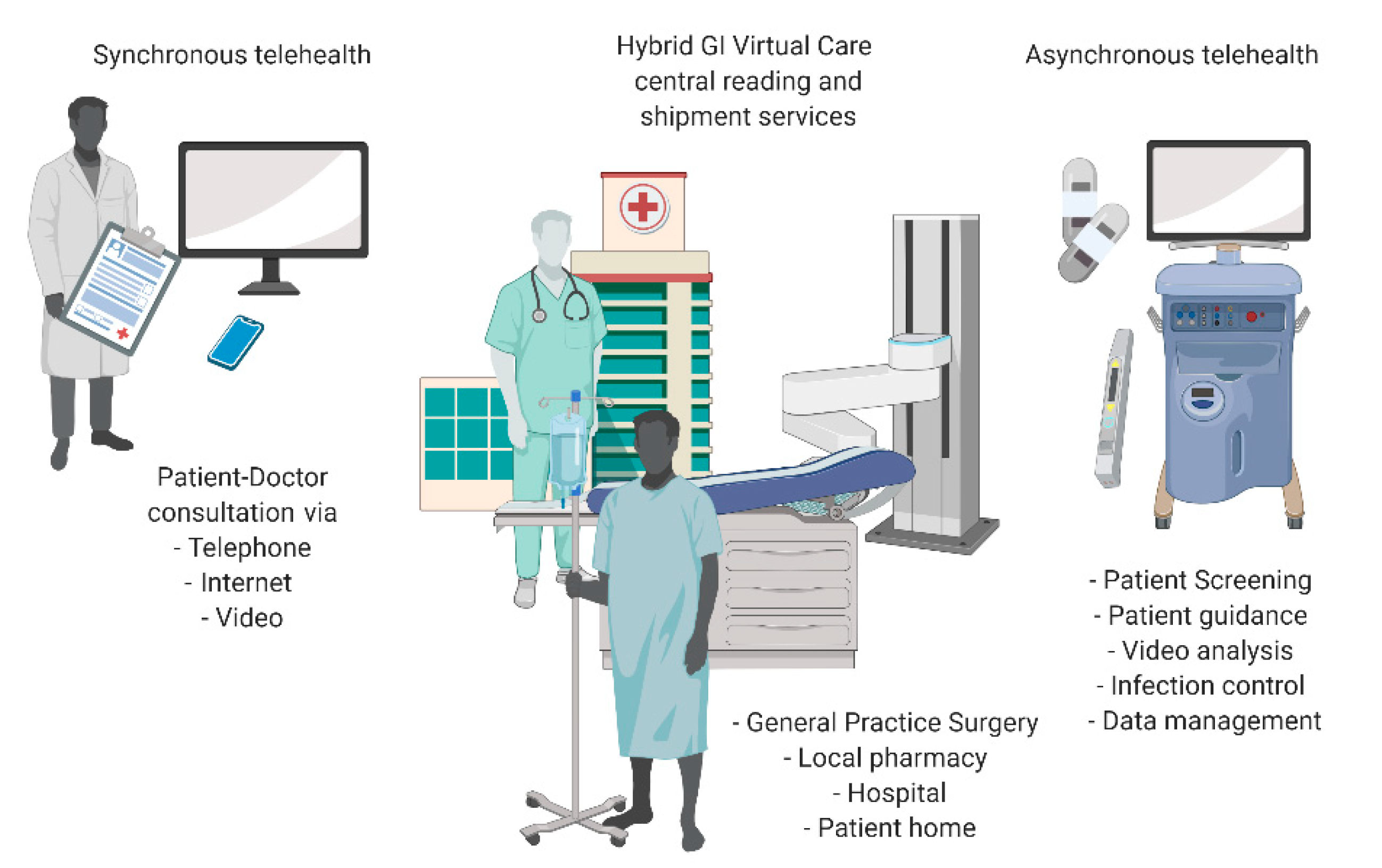
6. Endoscopy Services in the COVID-19 Era: Call for Innovation
7. Conclusions and Discussions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| AI | Artificial Intelligence |
| CAD | Computer-Aided Diagnostics |
| CNNs | Convolutional Neural Networks |
| COVID-19 | COronaVIrus Disease 19 |
| ESD | Endoscopic Submucosal Dissection |
| FPS | Frame Per Second |
| IoT | Internet of Things |
| LED | Light Emitting Diode |
| NOTES | Natural Orifice Transluminal Endoscopic Surgery |
| POEM | Per-Oral Endoscopic Myotomy |
| SARS-CoV-2 | Severe Acute Respiratory Syndrome-CoronaVirus-2 |
| UGI | Upper GastroIntestinal |
| WCE | Wireless Capsule Endoscope |
References
- Arnold, M.; Abnet, C.C.; Neale, R.E.; Vignat, J.; Giovannucci, E.L.; McGlynn, K.A.; Bray, F. Global Burden of 5 Major Types Of Gastrointestinal Cancer. Gastroenterology 2020. [Google Scholar] [CrossRef] [PubMed]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Etemadi, A.; Safiri, S.; Sepanlou, S.G.; Ikuta, K.; Bisignano, C.; Shakeri, R.; Amani, M.; Fitzmaurice, C.; Nixon, M.R.; Abbasi, N.; et al. The global, regional, and national burden of stomach cancer in 195 countries, 1990–2017: A systematic analysis for the Global Burden of Disease study 2017. Lancet Gastroenterol. Hepatol. 2020, 5, 42–54. [Google Scholar] [CrossRef] [Green Version]
- Coleman, H.G.; Xie, S.H.; Lagergren, J. The Epidemiology of Esophageal Adenocarcinoma. Gastroenterology 2018, 154, 390–405. [Google Scholar] [CrossRef] [PubMed]
- Choi, I.; Kim, C.; Lee, J.; Kim, Y.; Kook, M.C.; Park, B.; Joo, J. Undefined Family History of Gastric Cancer and Helicobacter pylori Treatment. Mass Med. Soc 2020, 382, 427–436. [Google Scholar] [CrossRef]
- Rawla, P.; Barsouk, A. Epidemiology of gastric cancer: Global trends, risk factors and prevention. Prz. Gastroenterol. 2019, 14, 26. [Google Scholar] [CrossRef]
- Arnal, M.J.D.; Arenas, Á.F.; Arbeloa, Á.L. Esophageal cancer: Risk factors, screening and endoscopic treatment in Western and Eastern countries. World J. Gastroenterol. WJG 2015, 21, 7933. [Google Scholar] [CrossRef]
- Libânio, D.; Dinis-Ribeiro, M. Gastroscopy and gastric cancer–related mortality: Time to change recommendations regarding screening? Gastrointest. Endosc. 2018, 87, 128–130. [Google Scholar] [CrossRef]
- Yoshida, N.; Doyama, H.; Yano, T.; Horimatsu, T.; Uedo, N.; Yamamoto, Y.; Kakushima, N.; Kanzaki, H.; Hori, S.; Yao, K.; et al. Early gastric cancer detection in high-risk patients: A multicentre randomised controlled trial on the effect of second-generation narrow band imaging. Gut 2020. [Google Scholar] [CrossRef]
- Chiu, P.; Sano, Y.; Uedo, N.; Singh, R.; Ng, E.; Aang, T.; Chiu, H.; Ho, S.-H.; Banerjee, R.; Tanaka, S.; et al. Utility of a standardized training program for endoscopic diagnosis of early gastrointestinal neoplasia. Endosc. Int. Open 2019, 7, E452–E458. [Google Scholar] [CrossRef] [Green Version]
- Xiao, H.F.; Yan, S.P.; Chen, Y.F.; Shi, Z.; Zou, Y.H.; Zhu, S.L.; Xu, K.K.; Song, T.; Liao, X.Z. Community-based upper gastrointestinal cancer screening in a randomized controlled trial: Baseline results in a non-high-incidence area. Cancer Prev. Res. 2020, 13, 317–327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Menon, S.; Trudgill, N. How commonly is upper gastrointestinal cancer missed at endoscopy? A meta-analysis. Endosc. Int. Open 2014, 2, E46–E50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pimenta-Melo, A.R.; Monteiro-Soares, M.; Libânio, D.; Dinis-Ribeiro, M. Missing rate for gastric cancer during upper gastrointestinal endoscopy: A systematic review and meta-analysis. Eur. J. Gastroenterol. Hepatol. 2016, 28, 1041–1049. [Google Scholar] [CrossRef] [PubMed]
- Beg, S.; Ragunath, K.; Wyman, A.; Banks, M.; Trudgill, N.; Pritchard, M.D.; Riley, S.; Anderson, J.; Griffiths, H.; Bhandari, P.; et al. Quality standards in upper gastrointestinal endoscopy: A position statement of the British Society of Gastroenterology (BSG) and Association of Upper Gastrointestinal Surgeons of Great Britain and Ireland (AUGIS). Gut 2017, 66, 1886–1899. [Google Scholar] [CrossRef] [Green Version]
- Fanelli, R.D.; Fanelli, S.M. Intraoperative endoscopy: An important skill for general surgeons. Gastrointest. Endosc. 2018, 20, 166–171. [Google Scholar] [CrossRef]
- Yung, D.E.; Banfi, T.; Ciuti, G.; Arezzo, A.; Dario, P.; Koulaouzidis, A. Musculoskeletal injuries in gastrointestinal endoscopists: A systematic review. Expert Rev. Gastroenterol. Hepatol. 2017, 11, 939–947. [Google Scholar] [CrossRef]
- Ciuti, G.; Skonieczna-Żydecka, K.; Marlicz, W.; Iacovacci, V.; Liu, H.; Stoyanov, D.; Arezzo, A.; Chiurazzi, M.; Toth, E.; Thorlacius, H.; et al. Frontiers of Robotic Colonoscopy: A Comprehensive Review of Robotic Colonoscopes and Technologies. J. Clin. Med. 2020, 9, 1648. [Google Scholar] [CrossRef]
- Boškoski, I.; Costamagna, G. Endoscopy robotics: Current and future applications. Dig. Endosc. 2019, 31, 119–124. [Google Scholar] [CrossRef] [Green Version]
- Gelijns, A.C.; Halm, E.A. The Diffusion of New Technology: Costs and Benefits to Health Care. In The Changing Economics of Medical Technology; National Academies Press (US): Washington, DC, USA, 1991. [Google Scholar]
- Lee, H.D.; Chung, H.; Kwak, Y.; Choi, J.; Lee, A.; Kim, J.L.; Cho, S.J.; Kim, S.G. Endoscopic Submucosal Dissection Versus Surgery for Superficial Esophageal Squamous Cell Carcinoma: A Propensity Score-Matched Survival Analysis. Clin. Transl. Gastroenterol. 2020, 11, 00193. [Google Scholar] [CrossRef]
- Hatta, W.; Gotoda, T.; Oyama, T.; Kawata, N.; Takahashi, A.; Yoshifuku, Y.; Hoteya, S.; Nakagawa, M.; Hirano, M.; Esaki, M.; et al. A Scoring System to Stratify Curability after Endoscopic Submucosal Dissection for Early Gastric Cancer: “eCura system”. Am. J. Gastroenterol. 2017, 112. [Google Scholar] [CrossRef]
- Fujiya, K.; Takizawa, K.; Tokunaga, M.; Kawata, N.; Hikage, M.; Makuuchi, R.; Tanizawa, Y.; Bando, E.; Kawamura, T.; Tanaka, M.; et al. The value of diagnostic endoscopic submucosal dissection for patients with clinical submucosal invasive early gastric cancer. Gastric Cancer 2018, 21, 124–132. [Google Scholar] [CrossRef] [Green Version]
- Białek, A.; Pertkiewicz, J.; Karpińska, K.; Marlicz, W.; Bielicki, D.; Starzyńska, T. Treatment of large colorectal neoplasms by endoscopic submucosal dissection: A European single-center study. Eur. J. Gastroenterol. Hepatol. 2014, 26, 607–615. [Google Scholar] [CrossRef] [PubMed]
- Hepatology, H.Y. Endoscopic submucosal dissection—Current success and future directions. Nat. Rev. Gastroenterol. Hepatol. 2012, 9, 519–529. [Google Scholar]
- Zhao, J.; Feng, B.; Zheng, M.H.; Xu, K. Surgical robots for SPL and NOTES: A review. Minim. Invasive Ther. Allied Technol. 2015, 24, 8–17. [Google Scholar] [CrossRef] [PubMed]
- Aguiluz Cornejo, G.; Jelen, N.; Gangemi, A. Robot-Assisted Revisional Surgery of Gastric Greater Curvature Plication to Roux-en-Y Gastric Bypass. Obes. Surg. 2019, 29, 1434–1435. [Google Scholar] [CrossRef]
- Ciuti, G.; Caliò, R.; Camboni, D.; Neri, L.; Bianchi, F.; Arezzo, A.; Koulaouzidis, A.; Schostek, S.; Stoyanov, D.; Oddo, C.M.; et al. Frontiers of robotic endoscopic capsules: A review. J. Micro-Bio Robot. 2016, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yeung, B.P.M.; Chiu, P.W.Y. Application of robotics in gastrointestinal endoscopy: A review. World J. Gastroenterol. 2016, 22, 1811–1825. [Google Scholar] [CrossRef]
- Banks, M.; Graham, D.; Jansen, M.; Gotoda, T.; Coda, S.; Di Pietro, M.; Uedo, N.; Bhandari, P.; Pritchard, D.M.; Kuipers, E.J.; et al. British Society of Gastroenterology guidelines on the diagnosis and management of patients at risk of gastric adenocarcinoma. Gut 2019, 68, 1545–1575. [Google Scholar] [CrossRef] [Green Version]
- Januszewicz, W.; Kaminski, M.F. Quality indicators in diagnostic upper gastrointestinal endoscopy. Therap. Adv. Gastroenterol. 2020, 13. [Google Scholar] [CrossRef]
- Olympus Olympus GIF-N180. Available online: https://aamedicalstore.com/products/olympus-gif-n180-evis-exera%E2%84%A2-ii-video-gastroscope (accessed on 30 January 2020).
- Bisschops, R.; Areia, M.; Coron, E.; Dobru, D.; Kaskas, B.; Kuvaev, R.; Pech, O.; Ragunath, K.; Weusten, B.; Familiari, P.; et al. Performance measures for upper gastrointestinal endoscopy: A European Society of Gastrointestinal Endoscopy (ESGE) Quality Improvement Initiative. Mário Dinis-Ribeiro 2016, 11, 843–864. [Google Scholar] [CrossRef] [Green Version]
- Park, W.G.; Shaheen, N.J.; Cohen, J.; Pike, I.M.; Adler, D.G.; Inadomi, J.M.; Laine, L.A.; Lieb, J.G.; Rizk, M.K.; Sawhney, M.S.; et al. Quality indicators for EGD. Am. J. Gastroenterol. 2015, 110, 60–71. [Google Scholar] [CrossRef] [PubMed]
- Wai, P.; Chiu, Y.; Uedo, N.; Singh, R.; Gotoda, T.; Kwok, E.; Ng, W.; Yao, K.; Leong Ang, T.; Ho, S.H.; et al. An Asian consensus on standards of diagnostic upper endoscopy for neoplasia. Gut 2019, 68, 186–197. [Google Scholar] [CrossRef] [Green Version]
- Eisen, G.M. Pillcam ESO: A Primer. Tech. Gastrointest. Endosc. 2006, 8, 154–159. [Google Scholar] [CrossRef]
- PillCam ESO2. Available online: http://www.medwow.com/med/camera-pill/given-imaging/pillcam-eso-2/66528.model-spec (accessed on 20 May 2020).
- Medtronic PillCam. Available online: https://www.pillcamcrohnscapsule.eu/product-overview.html (accessed on 1 June 2020).
- Beg, S.; Card, T.; Warburton, S.; Rahman, I.; Wilkes, E.; White, J.; Ragunath, K. Diagnosis of Barrett’s esophagus and esophageal varices using a magnetically assisted capsule endoscopy system. Gastrointest. Endosc. 2020, 91, 773–781. [Google Scholar] [CrossRef] [PubMed]
- Liao, Z.; Duan, X.D.; Xin, L.; Bo, L.M.; Wang, X.H.; Xiao, G.H.; Hu, L.H.; Zhuang, S.L.; Li, Z.S. Feasibility and safety of magnetic-controlled capsule endoscopy system in examination of human stomach: A pilot study in healthy volunteers. J. Interv. Gastroenterol. 2012, 2, 155–160. [Google Scholar] [CrossRef] [Green Version]
- Chongqing Jinshan Science & Technology OMOM Capsule Endoscopy Platform. Available online: http://www.jinshangroup.com/en/solutions/omomhd.html (accessed on 20 April 2020).
- Lai, H.S.; Wang, X.K.; Cai, J.Q.; Zhao, X.M.; Han, Z.L.; Zhang, J.; Chen, Z.Y.; Lin, Z.Z.; Zhou, P.H.; Hu, B.; et al. Standing-type magnetically guided capsule endoscopy versus gastroscopy for gastric examination: Multicenter blinded comparative trial. Dig. Endosc. 2019. [Google Scholar] [CrossRef] [Green Version]
- Rahman, I.; Pioche, M.; Shim, C.S.; Lee, S.P.; Sung, I.K.; Saurin, J.C.; Patel, P. Magnetic-assisted capsule endoscopy in the upper GI tract by using a novel navigation system (with video). Gastrointest. Endosc. 2016, 83, 889–895. [Google Scholar] [CrossRef]
- Hale, M.F.; Rahman, I.; Drew, K.; Sidhu, R.; Riley, S.A.; Patel, P.; McAlindon, M.E. Magnetically steerable gastric capsule endoscopy is equivalent to flexible endoscopy in the detection of markers in an excised porcine stomach model: Results of a randomized trial. Endoscopy 2015, 96. [Google Scholar] [CrossRef]
- Liao, Z.; Hou, X.; Lin-Hu, E.Q.; Sheng, J.Q.; Ge, Z.Z.; Jiang, B.; Hou, X.H.; Liu, J.Y.; Li, Z.; Huang, Q.Y.; et al. Accuracy of Magnetically Controlled Capsule Endoscopy, Compared With Conventional Gastroscopy, in Detection of Gastric Diseases. Clin. Gastroenterol. Hepatol. 2016, 14, 1266–1273. [Google Scholar] [CrossRef] [Green Version]
- Liao, Z.; Zou, W.; Li, Z.S. Clinical application of magnetically controlled capsule gastroscopy in gastric disease diagnosis: Recent advances. Sci. China Life Sci. 2018, 61, 1304–1309. [Google Scholar] [CrossRef]
- Ching, H.L.; Hale, M.F.; Sidhu, R.; McAlindon, M.E. PTH-050 Robot magnet-controlled upper gi capsule endoscopy using the ankon navicam ® system: First reported experience outside china. Gut 2017, 66, A1–A288. [Google Scholar] [CrossRef]
- Caprara, R.; Obstein, K.L.; Scozzarro, G.; Di Natali, C.; Beccani, M.; Morgan, D.R.; Valdastri, P. A platform for gastric cancer screening in low- and middle-income countries. IEEE Trans. Biomed. Eng. 2015, 62, 1324–1332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campisano, F.; Gramuglia, F.; Dawson, I.R.; Lyne, C.T.; Izmaylov, M.L.; Misra, S.; De Momi, E.; Morgan, D.R.; Obstein, K.L.; Valdastri, P. Gastric cancer screening in low-income countries: System design, fabrication, and analysis for an ultralow-cost endoscopy procedure. IEEE Robot. Autom. Mag. 2017, 24, 73–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yin, L.; Wang, S.; Zuo, S. Water-jet outer sheath with braided shape memory polymer tubes for upper gastrointestinal tract screening. Int. J. Med. Robot. Comput. Assist. Surg. 2018, 14, e1944. [Google Scholar] [CrossRef] [PubMed]
- Garbin, N.; Mamunes, A.P.; Sohn, D.; Hawkins, R.W.; Valdastri, P.; Obstein, K.L. Evaluation of a novel low-cost disposable endoscope for visual assessment of the esophagus and stomach in an ex-vivo phantom model. Endosc. Int. Open 2019, 7, E1175–E1183. [Google Scholar] [CrossRef] [Green Version]
- Ye, X.; Cabibihan, J.-J.; Yoon, W.J. Design and verification of a flexible device for steering a tethered capsule endoscope in the stomach. In Proceedings of the 2017 14th International Conference on Ubiquitous Robots and Ambient Intelligence (URAI), Jeju, Korea, 28 June–1 July 2017; pp. 550–555. [Google Scholar]
- Swain, P.; Toor, A.; Volke, F.; Keller, J.; Gerber, J.; Rabinovitz, E.; Rothstein, R.I. Remote magnetic manipulation of a wireless capsule endoscope in the esophagus and stomach of humans (with videos). Gastrointest. Endosc. 2010, 71, 1290–1293. [Google Scholar] [CrossRef]
- Tortora, G.; Valdastri, P.; Susilo, E.; Menciassi, A.; Dario, P.; Rieber, F.; Schurr, M.O. Propeller-based wireless device for active capsular endoscopy in the gastric district. Minim. Invasive Ther. Allied Technol. 2009, 18, 280–290. [Google Scholar] [CrossRef]
- De Falco, I.; Tortora, G.; Dario, P.; Menciassi, A. An integrated system for wireless capsule endoscopy in a liquid-distended stomach. IEEE Trans. Biomed. Eng. 2014, 61, 794–804. [Google Scholar] [CrossRef]
- Rey, J.F.; Ogata, H.; Hosoe, N.; Ohtsuka, K.; Ogata, N.; Ikeda, K.; Aihara, H.; Pangtay, I.; Hibi, T.; Kudo, S.; et al. Feasibility of stomach exploration with a guided capsule endoscope. Endoscopy 2010, 42, 541–545. [Google Scholar] [CrossRef]
- Keller, J.; Fibbe, C.; Volke, F.; Gerber, J.; Mosse, A.C.; Reimann-Zawadzki, M.; Rabinovitz, E.; Layer, P.; Schmitt, D.; Andresen, V.; et al. Inspection of the human stomach using remote-controlled capsule endoscopy: A feasibility study in healthy volunteers (with videos). Gastrointest. Endosc. 2011, 73, 22–28. [Google Scholar] [CrossRef]
- Rey, J.F.; Ogata, H.; Hosoe, N.; Ohtsuka, K.; Ogata, N.; Ikeda, K.; Aihara, H.; Pangtay, I.; Hibi, T.; Kudo, S.E.; et al. Blinded nonrandomized comparative study of gastric examination with a magnetically guided capsule endoscope and standard videoendoscope. Gastrointest. Endosc. 2012, 75, 373–381. [Google Scholar] [CrossRef]
- Kósa, G.; Jakab, P.; Székely, G.; Hata, N. MRI driven magnetic microswimmers. Biomed. Microdevices 2012, 14, 165–178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arkenbout, E.A.; Henselmans, P.W.J.; Jelínek, F.; Breedveld, P. A state of the art review and categorization of multi-branched instruments for NOTES and SILS. Surg. Endosc. 2015, 29, 1281–1296. [Google Scholar] [CrossRef]
- Shaikh, S.N. Natural orifice translumenal surgery: Flexible platform review. World J. Gastrointest. Surg. 2010, 2, 210. [Google Scholar] [CrossRef] [PubMed]
- Akintoye, E.; Obaitan, I.; Muthusamy, A.; Akanbi, O.; Olusunmade, M.; Levine, D. Endoscopic submucosal dissection of gastric tumors: A systematic review and meta-analysis. World J. Gastrointest. Endosc. 2016, 8, 517. [Google Scholar] [CrossRef] [PubMed]
- Hedjoudje, A.; Abu Dayyeh, B.K.; Cheskin, L.J.; Adam, A.; Neto, M.G.; Badurdeen, D.; Morales, J.G.; Sartoretto, A.; Nava, G.L.; Vargas, E.; et al. Efficacy and Safety of Endoscopic Sleeve Gastroplasty: A Systematic Review and Meta-Analysis. Clin. Gastroenterol. Hepatol. 2019. [Google Scholar] [CrossRef] [PubMed]
- Fayad, L.; Adam, A.; Schweitzer, M.; Cheskin, L.J.; Ajayi, T.; Dunlap, M.; Badurdeen, D.S.; Hill, C.; Paranji, N.; Lalezari, S.; et al. Endoscopic sleeve gastroplasty versus laparoscopic sleeve gastrectomy: A case-matched study. Gastrointest. Endosc. 2019, 89, 782–788. [Google Scholar] [CrossRef]
- Park, C.H.; Jung, D.H.; Kim, D.H.; Lim, C.H.; Moon, H.S.; Park, J.H.; Jung, H.K.; Hong, S.J.; Choi, S.C.; Lee, O.Y. Comparative efficacy of per-oral endoscopic myotomy and Heller myotomy in patients with achalasia: A meta-analysis. Gastrointest. Endosc. 2019, 90, 546.e3–558.e3. [Google Scholar] [CrossRef]
- Daoud, D.C.; Suter, N.; Durand, M.; Bouin, M.; Faulques, B.; Von Renteln, D. Comparing outcomes for endoscopic submucosal dissection between Eastern and Western countries: A systematic review and meta-analysis. World J. Gastroenterol. 2018, 24, 2518–2536. [Google Scholar] [CrossRef]
- Kume, K. Flexible robotic endoscopy: Current and original devices. Comput. Assist. Surg. 2016, 21, 150–159. [Google Scholar] [CrossRef]
- Phee, S.J.; Reddy, N.; Chiu, P.W.Y.; Rebala, P.; Rao, G.V.; Wang, Z.; Sun, Z.; Wong, J.Y.Y.; Ho, K.Y. Robot-Assisted Endoscopic Submucosal Dissection Is Effective in Treating Patients With Early-Stage Gastric Neoplasia. Clin. Gastroenterol. Hepatol. 2012, 10, 1117–1121. [Google Scholar] [CrossRef] [PubMed]
- Seah, T.E.T.; Do, T.N.; Takeshita, N.; Ho, K.Y.; Phee, S.J. Flexible Robotic Endoscopy Systems and the Future Ahead. In Diagnostic and Therapeutic Procedures in Gastroenterology; Humana Press: Cham, Switzerland, 2018; pp. 521–536. [Google Scholar]
- Patel, N.; Darzi, A.; Teare, J. The endoscopy evolution: ‘the superscope era.’. Frontline Gastroenterol. 2015, 6, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Berthet-Rayne, P.; Leibrandt, K.; Kim, K.; Seneci, C.A.; Shang, J.; Yang, G.Z. Rolling-Joint Design Optimization for Tendon Driven Snake-Like Surgical Robots. IEEE Int. Conf. Intell. Robot. Syst. 2018, 4964–4971. [Google Scholar] [CrossRef]
- Seneci, C.A.; Shang, J.; Leibrandt, K.; Vitiello, V.; Patel, N.; Darzi, A.; Teare, J.; Yang, G.Z. Design and evaluation of a novel flexible robot for transluminal and endoluminal surgery. In Proceedings of the IEEE International Conference on Intelligent Robots and Systems, Chicago, IL, USA, 14–18 September 2014; pp. 1314–1321. [Google Scholar]
- Mandapathil, M.; Duvvuri, U.; Güldner, C.; Teymoortash, A.; Lawson, G.; Werner, J.A. Transoral surgery for oropharyngeal tumors using the Medrobotics® Flex® System—A case report. Int. J. Surg. Case Rep. 2015, 10, 173–175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fuchs, K.H.; Breithaupt, W. Transgastric small bowel resection with the new multitasking platform EndoSAMURAITM for natural orifice transluminal endoscopic surgery. Surg. Endosc. 2012, 26, 2281–2287. [Google Scholar] [CrossRef] [PubMed]
- Rothstein, R.I.; Swanstrom, L.L. Use of the Direct Drive Endoscopic System (DDES) for In-Vivo Mucosal Resection in a Porcine Model. Gastrointest. Endosc. 2008, 67, AB146. [Google Scholar] [CrossRef]
- Johnson, P.J.; Serrano, C.M.R.; Castro, M.; Kuenzler, R.; Choset, H.; Tully, S.; Duvvuri, U. Demonstration of transoral surgery in cadaveric specimens with the medrobotics flex system. Laryngoscope 2013, 123, 1168–1172. [Google Scholar] [CrossRef]
- Mori, Y.; Kudo, S.E.; Mohmed, H.E.N.; Misawa, M.; Ogata, N.; Itoh, H.; Oda, M.; Mori, K. Artificial intelligence and upper gastrointestinal endoscopy: Current status and future perspective. Dig. Endosc. 2019, 31, 378–388. [Google Scholar] [CrossRef] [Green Version]
- Jin, P.; Ji, X.; Kang, W.; Li, Y.; Liu, H.; Ma, F.; Ma, S.; Hu, H.; Li, W.; Tian, Y. Artificial intelligence in gastric cancer: A systematic review. J. Cancer Res. Clin. Oncol. 2020, 146, 1–12. [Google Scholar] [CrossRef]
- Luo, H.; Xu, G.; Li, C.; He, L.; Luo, L.; Wang, Z.; Jing, B.; Deng, Y.; Jin, Y.; Li, Y.; et al. Real-time artificial intelligence for detection of upper gastrointestinal cancer by endoscopy: A multicentre, case-control, diagnostic study. Lancet Oncol. 2019, 20, 1645–1654. [Google Scholar] [CrossRef]
- Hirasawa, T.; Aoyama, K.; Tanimoto, T.; Ishihara, S.; Shichijo, S.; Ozawa, T.; Ohnishi, T.; Fujishiro, M.; Matsuo, K.; Fujisaki, J.; et al. Application of artificial intelligence using a convolutional neural network for detecting gastric cancer in endoscopic images. Gastric Cancer 2018, 21, 653–660. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Groof, A.J.; Struyvenberg, M.R.; van der Putten, J.; van der Sommen, F.; Fockens, K.N.; Curvers, W.L.; Zinger, S.; Pouw, R.E.; Coron, E.; Baldaque-Silva, F.; et al. Deep-Learning System Detects Neoplasia in Patients With Barrett’s Esophagus With Higher Accuracy Than Endoscopists in a Multistep Training and Validation Study with Benchmarking. Gastroenterology 2019, 158, 915–929. [Google Scholar] [CrossRef] [PubMed]
- Horie, Y.; Yoshio, T.; Aoyama, K.; Yoshimizu, S.; Horiuchi, Y.; Ishiyama, A.; Hirasawa, T.; Tsuchida, T.; Ozawa, T.; Ishihara, S.; et al. Diagnostic outcomes of esophageal cancer by artificial intelligence using convolutional neural networks. Gastrointest. Endosc. 2019, 89, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Quang, T.; Schwarz, R.A.; Dawsey, S.M.; Tan, M.C.; Patel, K.; Yu, X.; Wang, G.; Zhang, F.; Xu, H.; Anandasabapathy, S.; et al. A tablet-interfaced high-resolution microendoscope with automated image interpretation for real-time evaluation of esophageal squamous cell neoplasia. Gastrointest. Endosc. 2016, 84, 834–841. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guo, L.J.; Xiao, X.; Wu, C.C.; Zeng, X.; Zhang, Y.; Du, J.; Bai, S.; Xie, J.; Zhang, Z.; Li, Y.; et al. Real-time automated diagnosis of precancerous lesions and early esophageal squamous cell carcinoma using a deep learning model (with videos). Gastrointest. Endosc. 2020, 91, 41–51. [Google Scholar] [CrossRef]
- Itoh, T.; Kawahira, H.; Nakashima, H.; Yata, N. Deep learning analyzes Helicobacter pylori infection by upper gastrointestinal endoscopy images. Endosc. Int. Open 2018, 6, E139–E144. [Google Scholar] [CrossRef] [Green Version]
- Bah, A.; Saraga, E.; Armstrong, D.; Vouillamoz, D.; Dorta, G.; Duroux, P.; Weber, B.; Froehlich, F.; Blum, A.L.; Schnegg, J.F. Endoscopic Features of Helicobacter pylori-Related Gastritis. Endoscopy 1995, 27, 593–596. [Google Scholar] [CrossRef]
- Zhu, Y.; Wang, Q.C.; Xu, M.D.; Zhang, Z.; Cheng, J.; Zhong, Y.S.; Zhang, Y.Q.; Chen, W.F.; Yao, L.Q.; Zhou, P.H.; et al. Application of convolutional neural network in the diagnosis of the invasion depth of gastric cancer based on conventional endoscopy. Gastrointest. Endosc. 2019, 89, 806–815. [Google Scholar] [CrossRef]
- Zhou, T.; Han, G.; Li, B.N.; Lin, Z.; Ciaccio, E.J.; Green, P.H.; Qin, J. Quantitative analysis of patients with celiac disease by video capsule endoscopy: A deep learning method. Comput. Biol. Med. 2017, 85, 1–6. [Google Scholar] [CrossRef]
- Liedlgruber, M.; Uhl, A. Computer-aided decision support systems for endoscopy in the gastrointestinal tract: A review. IEEE Rev. Biomed. Eng. 2011, 4, 73–88. [Google Scholar] [CrossRef]
- Bretthauer, M.; Kaminski, M.F.; Løberg, M.; Zauber, A.G.; Regula, J.; Kuipers, E.J.; Hernán, M.A.; McFadden, E.; Sunde, A.; Kalager, M.; et al. Population-Based colonoscopy screening for colorectal cancer: A randomized clinical trial. JAMA Intern. Med. 2016, 176, 894–902. [Google Scholar] [CrossRef] [PubMed]
- Hamashima, C.; Ogoshi, K.; Narisawa, R.; Kishi, T.; Kato, T.; Fujita, K.; Sano, M.; Tsukioka, S. Impact of endoscopic screening on mortality reduction from gastric cancer. World J. Gastroenterol. 2015, 21, 2460–2466. [Google Scholar] [CrossRef] [PubMed]
- Mori, Y.; Kudo, S.; Misawa, M.; Saito, Y.; Ikematsu, H.; Hotta, K.; Ohtsuka, K.; Urushibara, F.; Kataoka, S.; Ogawa, Y.; et al. Real-Time Use of Artificial Intelligence in Identification of Diminutive Polyps During Colonoscopy. Ann. Intern. Med. 2018, 169, 357. [Google Scholar] [CrossRef] [PubMed]
- Parasa, S.; Wallace, M.; Bagci, U.; Antonino, M.; Berzin, T.; Byrne, M.; Celik, H.; Farahani, K.; Golding, M.; Gross, S.; et al. Proceedings from the First Global Artificial Intelligence in Gastroenterology and Endoscopy Summit. Gastrointest. Endosc. 2020. [Google Scholar] [CrossRef] [PubMed]
- National Institute of Health. Available online: https://clinicaltrials.gov/ct2/show/NCT04071678?term=endoscopy&cond=Artificial+intelligence&draw=2&rank=1 (accessed on 10 March 2020).
- Bhandari, P.; Subramaniam, S.; Bourke, M.J.; Alkandari, A.; Chiu, P.W.Y.; Brown, J.F.; Keswani, R.N.; Bisschops, R.; Hassan, C.; Raju, G.S.; et al. Recovery of endoscopy services in the era of COVID-19: Recommendations from an international Delphi consensus. Gut 2020. [Google Scholar] [CrossRef]
- Koulaouzidis, A.; Marlicz, W.; Wenzek, H.; Koulaouzidis, G.; Eliakim, R.; Toth, E. Returning to digestive endoscopy normality will be slow and must include novelty and telemedicine. Dig. Liver Dis. 2020. [Google Scholar] [CrossRef]
- Sethi, A.; Swaminath, A.; Latorre, M.; Behin, D.S.; Jodorkovsky, D.; Calo, D.; Aroniadis, O.; Mone, A.; Mendelsohn, R.B.; Sharaiha, R.Z.; et al. Donning a New Approach to the Practice of Gastroenterology: Perspectives From the COVID-19 Pandemic Epicenter. Clin. Gastroenterol. Hepatol. 2020, 18, 1673–1681. [Google Scholar] [CrossRef]
- Raphael, K.; Cerrone, S.; Sceppa, E.; Schneider, P.; Laumenede, T.; Lynch, A.; Sejpal, D.V. Improving patient safety in the endoscopy unit: Utilization of remote video auditing to improve time-out compliance. Gastrointest. Endosc. 2019, 90, 424–429. [Google Scholar] [CrossRef]
- Lees, C.W.; Regueiro, M.; Mahadevan, U. Innovation in IBD Care during the COVID-19 Pandemic: Results of a Global Telemedicine Survey by the International Organization for the Study of Inflammatory Bowel Disease. Gastroenterology 2020. [Google Scholar] [CrossRef]
- Verna, E.C.; Serper, M.; Chu, J.; Corey, K.; Fix, O.K.; Hoyt, K.; Page, K.A.; Loomba, R.; Li, M.; Everson, G.T.; et al. Clinical Research in Hepatology in the COVID-19 Pandemic and Post-Pandemic Era: Challenges and the Need for Innovation. Hepatology 2020. [Google Scholar] [CrossRef]
- Intzes, I.; Meng, H.; Cosmas, J. An Ingenious Design of a High Performance-Low Complexity Image Compressor for Wireless Capsule Endoscopy. Sensors 2020, 20, 1617. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salchak, Y.A.; Espinosa, H.G.; Thiel, D.V. Modeling the Surface Field from an Ingested Radio Transmitter with an Approximate Attenuation Model for Gastroenterology Investigations. IEEE Trans. Biomed. Eng. 2020, 67, 504–511. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Shi, Q.; Song, S.; Hu, C.; Meng, M.Q.-H. A Novel Relative Position Estimation Method for Capsule Robot Moving in Gastrointestinal Tract. Sensors 2019, 19, 2746. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koulaouzidis, G.; Charisopoulou, D.; Wojakowski, W.; Koulaouzidis, A.; Marlicz, W.; Jadczyk, T. Telemedicine in cardiology in the time of coronavirus disease 2019: A friend that everybody needs. Polish Arch. Intern. Med. 2020, 130, 559–561. [Google Scholar] [CrossRef]
- Ahad, A.; Tahir, M.; Aman Sheikh, M.; Ahmed, K.I.; Mughees, A.; Numani, A. Technologies Trend towards 5G Network for Smart Health-Care Using IoT: A Review. Sensors 2020, 20, 4047. [Google Scholar] [CrossRef]
- Li, D. 5G and intelligence medicine—How the next generation of wireless technology will reconstruct healthcare? Precis. Clin. Med. 2019, 2, 205–208. [Google Scholar] [CrossRef] [Green Version]
- Wenzek, H. Video Capsule Reporting. At ‘AI in GI—Vision 2020′ Conference. Available online: https://www.youtube.com/watch?v=Tqg23Pdi3iI (accessed on 10 May 2020).
- Alam, M.W.; Sohag, M.H.A.; Khan, A.H.; Sultana, T.; Wahid, K.A. IoT-Based intelligent capsule endoscopy system: A technical review. In Intelligent Data Analysis for Biomedical Applications: Challenges and Solutions; Elsevier: Amsterdam, The Netherlands, 2019; pp. 1–20. ISBN 9780128155530. [Google Scholar]
- Liu, N.; Huang, R.; Baldacchino, T.; Sud, A.; Sud, K.; Khadra, M.; Kim, J. Telehealth for Noncritical Patients With Chronic Diseases During the COVID-19 Pandemic. J. Med. Internet Res. 2020, 22, e19493. [Google Scholar] [CrossRef]
- Baumgart, D.C. Digital advantage in the COVID-19 response: Perspective from Canada’s largest integrated digitalized healthcare system. npj Digit. Med. 2020, 3, 1–4. [Google Scholar] [CrossRef]
- Biorender. Available online: https://biorender.com/ (accessed on 20 September 2020).




© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marlicz, W.; Ren, X.; Robertson, A.; Skonieczna-Żydecka, K.; Łoniewski, I.; Dario, P.; Wang, S.; Plevris, J.N.; Koulaouzidis, A.; Ciuti, G. Frontiers of Robotic Gastroscopy: A Comprehensive Review of Robotic Gastroscopes and Technologies. Cancers 2020, 12, 2775. https://doi.org/10.3390/cancers12102775
Marlicz W, Ren X, Robertson A, Skonieczna-Żydecka K, Łoniewski I, Dario P, Wang S, Plevris JN, Koulaouzidis A, Ciuti G. Frontiers of Robotic Gastroscopy: A Comprehensive Review of Robotic Gastroscopes and Technologies. Cancers. 2020; 12(10):2775. https://doi.org/10.3390/cancers12102775
Chicago/Turabian StyleMarlicz, Wojciech, Xuyang Ren, Alexander Robertson, Karolina Skonieczna-Żydecka, Igor Łoniewski, Paolo Dario, Shuxin Wang, John N Plevris, Anastasios Koulaouzidis, and Gastone Ciuti. 2020. "Frontiers of Robotic Gastroscopy: A Comprehensive Review of Robotic Gastroscopes and Technologies" Cancers 12, no. 10: 2775. https://doi.org/10.3390/cancers12102775
APA StyleMarlicz, W., Ren, X., Robertson, A., Skonieczna-Żydecka, K., Łoniewski, I., Dario, P., Wang, S., Plevris, J. N., Koulaouzidis, A., & Ciuti, G. (2020). Frontiers of Robotic Gastroscopy: A Comprehensive Review of Robotic Gastroscopes and Technologies. Cancers, 12(10), 2775. https://doi.org/10.3390/cancers12102775