Establishment of an Endoscopy-Guided Minimally Invasive Orthotopic Mouse Model of Colorectal Cancer

Abstract
:Simple Summary
Abstract
1. Introduction
2. Results
2.1. Learning Curve for Successful Cell Injection
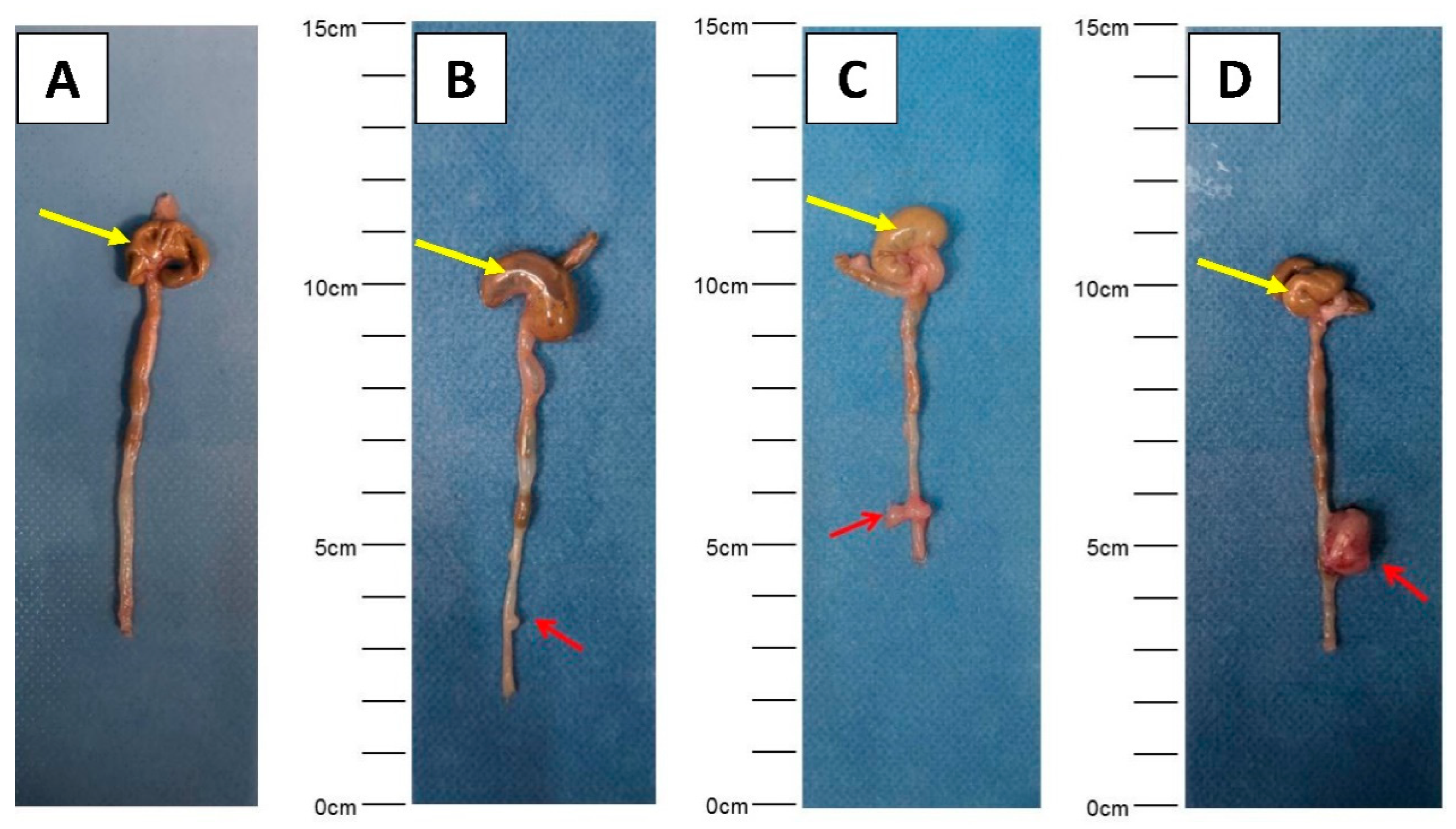
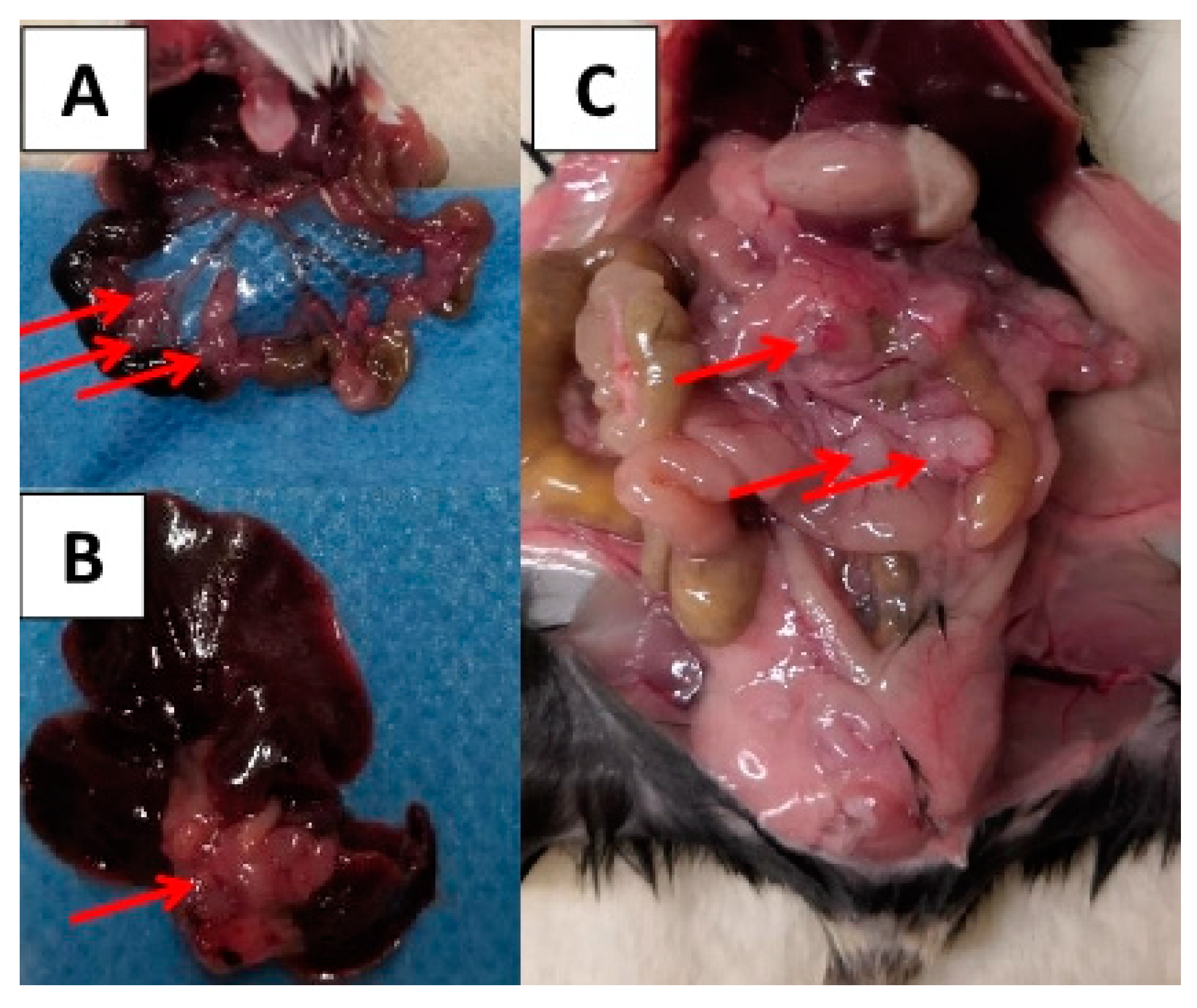
2.2. Local Tumor Growth
2.3. Lymph Node and Distant Metastasis
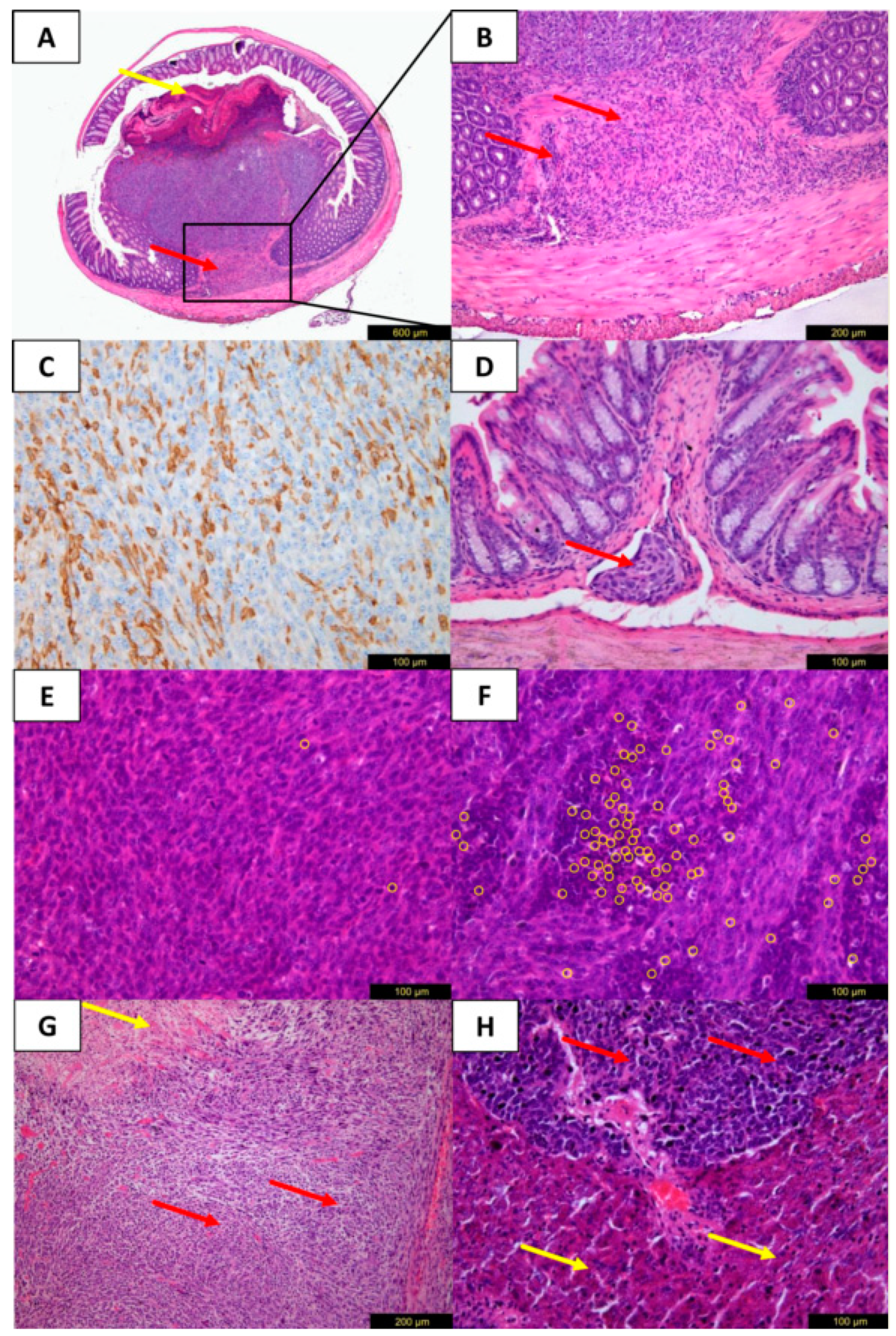
2.4. Histology and Immuno-Histochemistry
3. Discussion
4. Materials and Methods
4.1. CRC Cell Lines
4.2. Mice
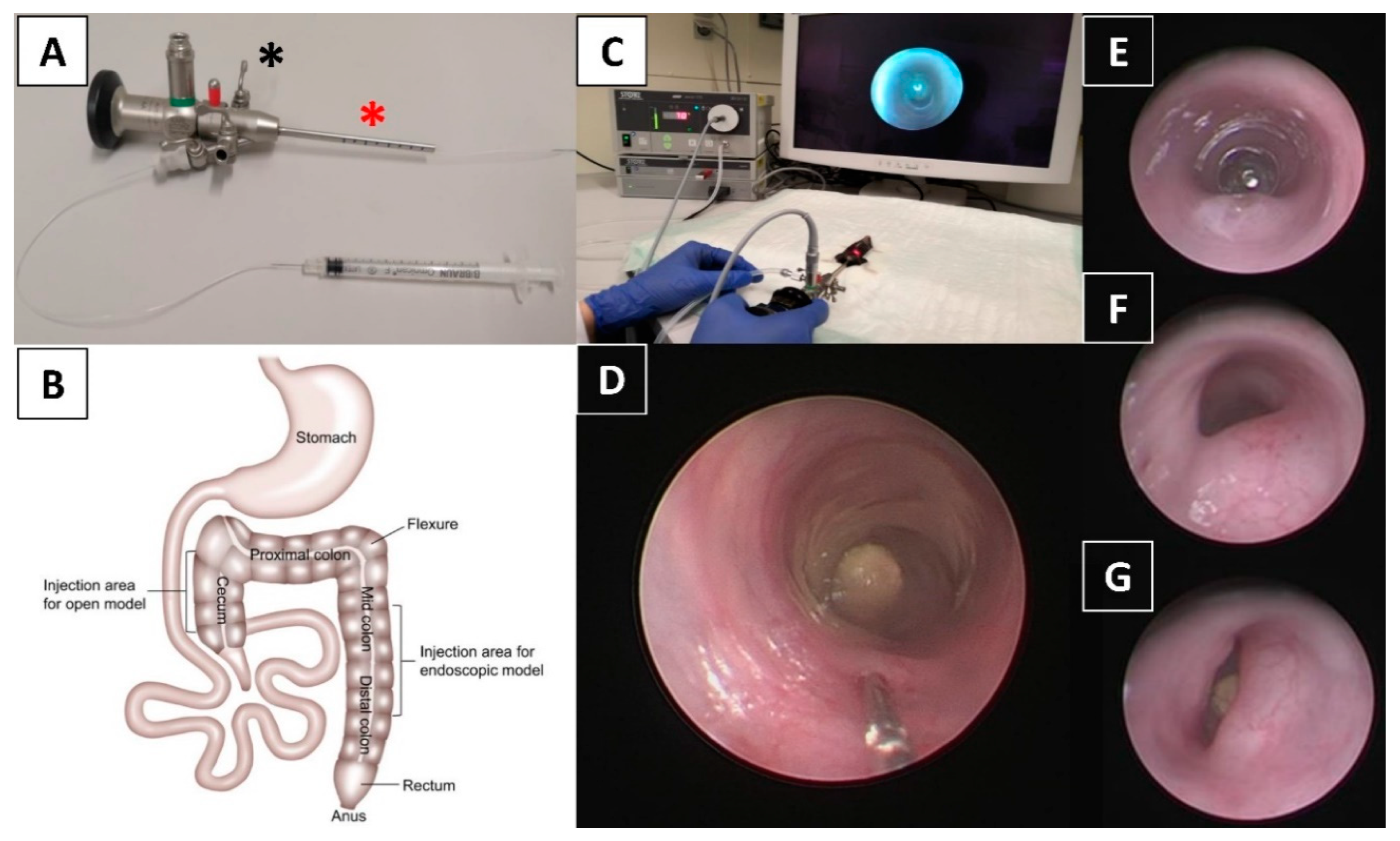
4.3. Anesthesia and Endoscopy
4.4. Endoscopy-Guided Tumor Cell Implantation
4.5. Autopsy and Tumor Assessment
4.6. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Keum, N.; Giovannucci, E. Global burden of colorectal cancer: Emerging trends, risk factors and prevention strategies. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 713–732. [Google Scholar] [CrossRef] [PubMed]
- Van der Jeught, K.; Xu, H.C.; Li, Y.J.; Lu, X.B.; Ji, G. Drug resistance and new therapies in colorectal cancer. World. J. Gastroenterol. 2018, 24, 3834–3848. [Google Scholar] [CrossRef] [PubMed]
- Clevers, H. Modeling Development and Disease with Organoids. Cell 2016, 165, 1586–1597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, R.L.; Fleet, J.C. Animal models of colorectal cancer. Cancer. Metastasis. Rev. 2013, 32, 39–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tong, Y.; Yang, W.; Koeffler, H.P. Mouse models of colorectal cancer. Chin. J. Cancer 2011, 30, 450–462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Young, M.; Ordonez, L.; Clarke, A.R. What are the best routes to effectively model human colorectal cancer? Mol. Oncol. 2013, 7, 178–189. [Google Scholar] [CrossRef]
- Gock, M.; Kuhn, F.; Mullins, C.S.; Krohn, M.; Prall, F.; Klar, E.; Linnebacher, M. Tumor Take Rate Optimization for Colorectal Carcinoma Patient-Derived Xenograft Models. Biomed. Res. Int. 2016, 2016, 1715053. [Google Scholar] [CrossRef]
- Kuehn, F.; Mullins, C.S.; Krohn, M.; Harnack, C.; Ramer, R.; Krämer, O.H.; Klar, E.; Huehns, M.; Linnebacher, M. Establishment and characterization of HROC69—A Crohn s related colonic carcinoma cell line and its matched patient-derived xenograft. Sci. Rep. 2016, 6, 24671. [Google Scholar] [CrossRef] [Green Version]
- Tseng, W.; Leong, X.; Engleman, E. Orthotopic mouse model of colorectal cancer. J. Vis. Exp. 2007, 10, 484. [Google Scholar] [CrossRef]
- Zhao, X.; Li, L.; Starr, T.K.; Subramanian, S. Tumor location impacts immune response in mouse models of colon cancer. Oncotarget 2017, 8, 54775–54787. [Google Scholar] [CrossRef] [Green Version]
- Evans, J.P.; Sutton, P.A.; Winiarski, B.K.; Fenwick, S.W.; Malik, H.Z.; Vimalachandran, D.; Tweedle, E.M.; Costello, E.; Palmer, D.H.; Park, B.K.; et al. From mice to men: Murine models of colorectal cancer for use in translational research. Crit. Rev. Oncol. Hematol. 2016, 98, 94–105. [Google Scholar] [CrossRef]
- Vandamme, T.F. Use of rodents as models of human diseases. J. Pharm. Bioallied. Sci. 2014, 6, 2–9. [Google Scholar] [CrossRef] [PubMed]
- Liu, E.; Kitajima, S.; Morimoto, M. Application and recent advances of laboratory mouse in human cancer research. Chin. J. Cancer 2005, 24, 249–254. [Google Scholar]
- Oliveira, R.C.; Abrantes, A.M.; Tralhao, J.G.; Botelho, M.F. The role of mouse models in colorectal cancer research-The need and the importance of the orthotopic models. Anim. Models. Exp. Med. 2020, 3, 1–8. [Google Scholar] [CrossRef]
- Mittal, V.K.; Bhullar, J.S.; Jayant, K. Animal models of human colorectal cancer: Current status, uses and limitations. World. J. Gastroenterol. 2015, 21, 11854–11861. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shankaran, V.; Ikeda, H.; Bruce, A.T.; White, J.M.; Swanson, P.E.; Old, L.J.; Schreiber, R.D. IFNgamma and lymphocytes prevent primary tumour development and shape tumour immunogenicity. Nature 2001, 410, 1107–1111. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.W.; Park, Y.A.; Cho, Y.J.; Kang, K.-H.; Choi, J.-J.; Lee, Y.-Y.; Kim, T.-J.; Choi, C.H.; Kim, B.-G.; Bae, D.-S. The effect of surgical wound on ovarian carcinoma growth in an animal model. Anticancer. Res. 2013, 33, 3177–3184. [Google Scholar]
- Becker, C.; Fantini, M.C.; Neurath, M.F. High resolution colonoscopy in live mice. Nat. Protoc. 2006, 1, 2900–2904. [Google Scholar] [CrossRef]
- Zigmond, E.; Halpern, Z.; Elinav, E.; Brazowski, E.; Jung, S.; Varol, C. Utilization of murine colonoscopy for orthotopic implantation of colorectal cancer. PLoS ONE 2011, 6, e28858. [Google Scholar] [CrossRef]
- Beyaz, S.; Mana, M.D.; Roper, J.; Kedrin, D.; Saadatpour, A.; Hong, S.-J.; Bauer-Rowe, K.E.; Xifaras, M.E.; Akkad, A.; Arias, E.; et al. High-fat diet enhances stemness and tumorigenicity of intestinal progenitors. Nature 2016, 3, 53–58. [Google Scholar] [CrossRef]
- Roper, J.; Tammela, T.; Cetinbas, N.M.; Akkad, A.; Roghanian, A.; Rickelt, S.; Almeqdadi, M.; Wu, K.; Oberli, M.A.; Sánchez-Rivera, F.J.; et al. In vivo genome editing and organoid transplantation models of colorectal cancer and metastasis. Nat. Biotechnol. 2017, 35, 569–576. [Google Scholar] [CrossRef] [PubMed]
- Ulivi, P.; Scarpi, E.; Chiadini, E.; Marisi, G.; Valgiusti, M.; Capelli, L.; Gardini, A.C.; Monti, M.; Ruscelli, S.; Frassineti, G.L.; et al. Right- vs. Left-Sided Metastatic Colorectal Cancer: Differences in Tumor Biology and Bevacizumab Efficacy. Int. J. Mol. Sci. 2017, 18, 1240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karim, B.O.; Huso, D.L. Mouse models for colorectal cancer. Am. J. Cancer. Res. 2013, 3, 240–250. [Google Scholar] [PubMed]
- Terracina, K.P.; Aoyagi, T.; Huang, W.C.; Nagahashi, M.; Yamada, A.; Aoki, K.; Takabe, K. Development of a metastatic murine colon cancer model. J. Surg. Res. 2015, 199, 106–114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thiran, A. The Effect of Colorectal Surgery on Liver Metastases—Development of a Mouse Model. Ghent University. 2019. Available online: https://lib.ugent.be/fulltxt/RUG01/002/782/981/RUG01-002782981_2019_0001_AC.pdf (accessed on 1 September 2020).
- Bettenworth, D.; Mucke, M.M.; Schwegmann, K.; Faust, A.; Poremba, C.; Schäfers, M.; Domagk, D.; Lenz, P. Endoscopy-guided orthotopic implantation of colorectal cancer cells results in metastatic colorectal cancer in mice. Clin. Exp. Metastasis 2016, 33, 551–562. [Google Scholar] [CrossRef]
- Kodani, T.; Rodriguez-Palacios, A.; Corridoni, D.; Lopetuso, L.; Di Martino, L.; Marks, B.; Pizarro, J.; Pizarro, T.; Chak, A.; Cominelli, F. Flexible colonoscopy in mice to evaluate the severity of colitis and colorectal tumors using a validated endoscopic scoring system. J. Vis. Exp. 2013, 16, e50843. [Google Scholar] [CrossRef]
- Zheng, D.W.; Dong, X.; Pan, P.; Chen, K.-W.; Fan, J.-X.; Cheng, S.-X.; Zhang, X.Z. Phage-guided modulation of the gut microbiota of mouse models of colorectal cancer augments their responses to chemotherapy. Nat. Biomed. Eng. 2019, 3, 717–728. [Google Scholar] [CrossRef]
- Jung, K.; Heishi, T.; Incio, J.; Huang, Y.; Beech, E.Y.; Pinter, M.; Ho, W.W.; Kawaguchi, K.; Rahbari, N.N.; Chung, E.; et al. Targeting CXCR4-dependent immunosuppressive Ly6C (low) monocytes improves antiangiogenic therapy in colorectal cancer. Proc. Natl. Acad. Sci. USA 2017, 114, 10455–10460. [Google Scholar] [CrossRef] [Green Version]
- Guillen, J. FELASA guidelines and recommendations. J. Am. Assoc. Lab. Anim. Sci. 2012, 51, 311–321. [Google Scholar]
- Kilkenny, C.; Browne, W.J.; Cuthi, I.; Emerson, M.; Altman, D.G. Improving bioscience research reporting: The ARRIVE guidelines for reporting animal research. Vet. Clin. Pathol. 2012, 41, 27–31. [Google Scholar] [CrossRef] [Green Version]
- Freeling, J.L.; Rezvani, K. Assessment of murine colorectal cancer by micro-ultrasound using three dimensional reconstruction and non-linear contrast imaging. Mol. Ther. Methods. Clin. Dev. 2016, 5, 16070. [Google Scholar] [CrossRef] [PubMed]
- Treuting, P.M.; Snyder, J.M. Mouse Necropsy. Curr. Protoc. Mouse. Biol. 2015, 5, 223–233. [Google Scholar] [CrossRef]
- Mirniaharikandehei, S.; Van Osdol, J.; Heidari, M.; Danala, G.; Sethuraman, S.N.; Ranjan, A.; Zheng, B. Developing a Quantitative Ultrasound Image Feature Analysis Scheme to Assess Tumor Treatment Efficacy Using a Mouse Model. Sci. Rep. 2019, 9, 7293. [Google Scholar] [CrossRef] [PubMed]
- Hendry, S.; Salgado, R.; Gevaert, T.; Russell, P.A.; John, T.; Thapa, B.; Christie, M.; van de Vijver, K.; Estrada, M.V.; Gonzalez-Ericsson, P.I.; et al. Assessing Tumor-infiltrating Lymphocytes in Solid Tumors: A Practical Review for Pathologists and Proposal for a Standardized Method From the International Immunooncology Biomarkers Working Group: Part 1: Assessing the Host Immune Response, TILs in Invasive Breast Carcinoma and Ductal Carcinoma In Situ, Metastatic Tumor Deposits and Areas for Further Research. Adv. Anat. Pathol. 2017, 24, 235–251. [Google Scholar] [PubMed] [Green Version]
- Salgado, R.; Denkert, C.; Demaria, S.; Sirtaine, N.; Klauschen, F.; Pruneri, G.; Wienert, S.; Van den Eynden, G.; Baehner, F.L.; Penault-Llorca, F.; et al. The evaluation of tumor-infiltrating lymphocytes (TILs) in breast cancer: Recommendations by an International TILs Working Group 2014. Ann. Oncol. 2015, 26, 259–271. [Google Scholar] [CrossRef]
- Schiergens, T.S.; Reu, S.; Neumann, J.; Renz, B.W.; Niess, H.; Boeck, S.; Heinemann, V.; Bruns, C.J.; Jauch, K.-W.; Kleespies, A. Histomorphologic and molecular phenotypes predict gemcitabine response and overall survival in adenocarcinoma of the ampulla of Vater. Surgery 2015, 158, 151–161. [Google Scholar] [CrossRef]
- Hernandez, B.Y.; Frierson, H.F.; Moskaluk, C.A.; Li, Y.J.; Clegg, L.; Cote, T.R.; McCusker, M.E.; Hankey, B.F.; Edwards, B.K.; Goodman, M.T. CK20 and CK7 protein expression in colorectal cancer: Demonstration of the utility of a population-based tissue microarray. Hum. Pathol. 2005, 36, 275–281. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number of Injected Cells | Observation Period (d) | Mortality [mice(%)] | Tumor Take Rate [mice(%)] | Tumor Volume (Mean ± SD, mm3) | Metastasis Rate [mice(%)] a | ||
|---|---|---|---|---|---|---|---|
| Mesenteric Lymph Node Metastasis | Peritoneal Carcinosis | Hepatic Metastasis | |||||
| 104 | 7 | 0/4(0) | 2/4(50) | 2.5 ± 0.7 | 0/2(0) | 0/2(0) | 0/2(0) |
| 14 | 0/4(0) | 4/4(100) | 2.6 ± 1.5 | 3/4(75) | 0/4(0) | 1/4(25) | |
| 21 | 0/4(0) | 4/4(100) | 5.8 ± 2.9 | 1/4(25) | 1/4(25) | 0/4(0) | |
| 28 | 0/4(0) | 4/4(100) | 20.0 ± 1.6 | 1/4(25) | 0/4(0) | 0/4(0) | |
| 105 | 7 | 0/4(0) | 4/4(100) | 4.8 ± 5.2 | 2/4(50) | 0/4(0) | 1/4(25) |
| 14 | 0/4(0) | 4/4(100) | 7.0 ± 7.4 | 4/4(100) | 1/4(25) | 2/4(50) | |
| 21 | 0/4(0) | 3/4(75) | 31.0 ± 20.7 | 2/3(67) | 0/3(0) | 0/3(0) | |
| 28 | 0/4(0) | 3/4(75) | 22.7 ± 2.3 | 1/3(33) | 0/3(0) | 0/3(0) | |
| 106 | 7 | 0/4(0) | 4/4(100) | 31.3 ± 17.7 | 2/4(50) | 0/4(0) | 1/4(25) |
| 14 | 0/4(0) | 4/4(100) | 15.8 ± 8.5 | 2/4(50) | 0/4(0) | 2/4(50) | |
| 21 | 3/4(75) b | 4/4(100) | 44.3 ± 45.2 | 2/4(50) | 0/4(0) | 0/4(0) | |
| 28 | 4/4(100) b | 4/4(100) | 27.5 ± 11.9 | 2/4(50) | 1/4(25) | 1/4(25) | |
| Number of Injected Cells | Observation Period (d) | Mortality [mice(%)] | Tumor Take Rate [mice(%)] | Tumor Volume (Mean ± SD, mm3) | Metastasis Rate [mice(%)] a | ||
|---|---|---|---|---|---|---|---|
| Mesenteric Lymph Node Metastasis | Peritoneal Carcinosis | Hepatic Metastasis | |||||
| 104 | 7 | 0/4(0) | 0/4(0) | - | 0/0(0) | 0/0(0) | 0/0(0) |
| 14 | 0/4(0) | 0/4(0) | - | 0/0(0) | 0/0(0) | 0/0(0) | |
| 21 | 0/4(0) | 0/4(0) | - | 0/0(0) | 0/0(0) | 0/0(0) | |
| 28 | 0/4(0) | 0/4(0) | - | 0/0(0) | 0/0(0) | 0/0(0) | |
| 105 | 7 | 0/4(0) | 0/4(0) | - | 0/0(0) | 0/0(0) | 0/0(0) |
| 14 | 0/4(0) | 1/4(25) | 4.0 ± 0.0 | 0/1(0) | 0/1(0) | 0/1(0) | |
| 21 | 0/4(0) | 2/4(50) | 2.2 ± 1.3 | 0/2(0) | 0/2(0) | 0/2(0) | |
| 28 | 0/4(0) | 3/4(75) | 9.7 ± 5.5 | 2/3(67) | 1/3(33) | 0/3(0) | |
| 106 | 7 | 0/4(0) | 0/4(0) | - | 0/0(0) | 0/0(0) | 0/0(0) |
| 14 | 0/4(0) | 2/4(50) | 10.0 ± 8.5 | 0/2(0) | 0/2(0) | 0/2(0) | |
| 21 | 0/4(0) | 1/4(25) | 18.0 ± 0.0 | 0/1(0) | 0/1(0) | 0/1(0) | |
| 28 | 0/4(0) | 2/4(50) | 14.1 ± 15.5 | 1/2(50) | 0/2(0) | 0/2(0) | |
| Before Anesthesia |
| ⬜ Mark gradations on the endoscope sheath to facilitate recording of injection location/tumor position |
| ⬜ Set the light intensity to ~70% and do not change it during the whole procedure to avoid bias |
| ⬜ Set the white balance by pointing the telescope/camera directly at a white object 3–5 cm away |
| ⬜ Set the focus so that objects at a distance of 3–5 mm give a crisp picture |
| Before Endoscope Induction |
| ⬜ Carefully examine the perianal area of the animal to ensure there are no lesions |
| ⬜ Make sure the needle is completely inside the sheath. An exposed needle during endoscope insertion may cause harm to the colon and perforation |
| ⬜ Adjust the valve of the Luer lock adapter until a slow constant flow of air is observed when the needle is submerged in a tube of water |
| ⬜ Rinse the endoscope in warm PBS for lubrication and to avoid a fogged-up optical lens |
| Cell Injection (Supplementary Video S1) |
| ⬜ Monitor the abdomen to localize the tip of the scope with transillumination and to avoid over-inflation |
| ⬜ Examine the colonic mucosa carefully to ensure its health |
| ⬜ Avoid injection into or near a blood vessel which would lead to direct intravascular dissemination of cells and hemorrhage |
| ⬜ Choose a suitable injection position, lift the sheath a little bit to expose the needle in the camera view⬜ Adjust the needle such that the beveled surface faces the lumen, then lower the sheath so that the needle is almost parallel to the colonic wall |
| ⬜ Gently penetrate the colonic mucosa with the needle ensuring that its beveled edge is always facing the lumen before slowly injecting 50μL (or less) of tumor cell suspension |
| ⬜ The first injection should be done in a more proximal location as this allows for additional injections (if desired) in increasingly distal locations with up to four possible injections per mouse |
| ⬜ A characteristic lifting sign (Supplementary Video S1) of the mucosa during injection indicates successful injection⬜ Two investigators are optimal for the injection procedure (one navigating the endoscope, one the injection maneuver) |
| After Injection |
| ⬜ Withdraw the needle 10 s after injection to make sure that all cells are injected |
| ⬜ Withdraw the needle to make sure it is totally inside the sheath, then withdraw the sheath |
| ⬜ Disinfect the endoscope, needle, and catheter using gigasept® AF forte (2% v/v) and then rinse well with water |
| Follow-up Colonoscopy |
| ⬜ Carefully examine the perianal area of the animal to ensure that there are no lesions |
| ⬜ Gently clean the colon if feces obstruct the view and slow down air inflation speed, since tumor-burdened colorectum is fragile and easy to perforate |
| ⬜ Keep a record of the appearance of the colonic mucosa |
| ⬜ Score the tumor (endoscopic score) using pictures taken from colonoscopy, do not score during colonoscopy to avoid excessive air inflation⬜ Usually, one investigator is sufficient to carry out follow-up colonoscopy |
| Troubleshooting, Pitfalls and General tips |
| ⬜ Mice should be no younger than 10 weeks to enable introduction of the endoscope without harming the animals⬜ Attach a suitable catheter to the injection needle (31G or smaller) for insertion into the working channel of the endoscope: the catheter should be rotatable within the channel to facilitate orientation of the bevel before injection (see above). On the other hand, the catheter should be thick enough so that the needle is sufficiently stabilized during injection. |
| ⬜ If feces obstruct the view, they can usually be moved orally with gentle air inflation; if this does not work, apply 1–2 mL warm PBS to wash the colon using a soft transfer pipette |
| ⬜ Application of more than 2 mL of PBS solution leads to a blurry/bubble-filled view of the colon and a higher risk of perforation |
| ⬜ The use of tap water for colorectal rinsing should be avoided, since the mucosa will become less transparent or even white (bad view) |
| ⬜ If feces or blood is coating the optical lens, withdraw the endoscope, clean it with warm PBS, and reintroduce it |
| ⬜ If the mucosa gets folded due to peristalsis, wait a few seconds until the peristaltic wave has passed. Do not compensate by increasing air flow |
| ⬜ Keep the mouse on a heated pad from the start of anesthesia until the mouse is fully recovered |
| ⬜ Do not advance the endoscope anymore once you see the colonic curve (splenic flexure), maximal insertion length is approximately up to 4 cm |
| ⬜ Limit air inflation time as increased time could cause respiratory distress, pneumoperitoneum, or even death of the mouse |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, C.; Neumann, J.; Kühn, F.; Lee, S.M.L.; Drefs, M.; Andrassy, J.; Werner, J.; Bazhin, A.V.; Schiergens, T.S. Establishment of an Endoscopy-Guided Minimally Invasive Orthotopic Mouse Model of Colorectal Cancer. Cancers 2020, 12, 3007. https://doi.org/10.3390/cancers12103007
Chen C, Neumann J, Kühn F, Lee SML, Drefs M, Andrassy J, Werner J, Bazhin AV, Schiergens TS. Establishment of an Endoscopy-Guided Minimally Invasive Orthotopic Mouse Model of Colorectal Cancer. Cancers. 2020; 12(10):3007. https://doi.org/10.3390/cancers12103007
Chicago/Turabian StyleChen, Chen, Jens Neumann, Florian Kühn, Serene M. L. Lee, Moritz Drefs, Joachim Andrassy, Jens Werner, Alexandr V. Bazhin, and Tobias S. Schiergens. 2020. "Establishment of an Endoscopy-Guided Minimally Invasive Orthotopic Mouse Model of Colorectal Cancer" Cancers 12, no. 10: 3007. https://doi.org/10.3390/cancers12103007
APA StyleChen, C., Neumann, J., Kühn, F., Lee, S. M. L., Drefs, M., Andrassy, J., Werner, J., Bazhin, A. V., & Schiergens, T. S. (2020). Establishment of an Endoscopy-Guided Minimally Invasive Orthotopic Mouse Model of Colorectal Cancer. Cancers, 12(10), 3007. https://doi.org/10.3390/cancers12103007