Occurrence of Fibrotic Tumor Vessels in Grade I Meningiomas Is Strongly Associated with Vessel Density, Expression of VEGF, PlGF, IGFBP-3 and Tumor Recurrence

 , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Results
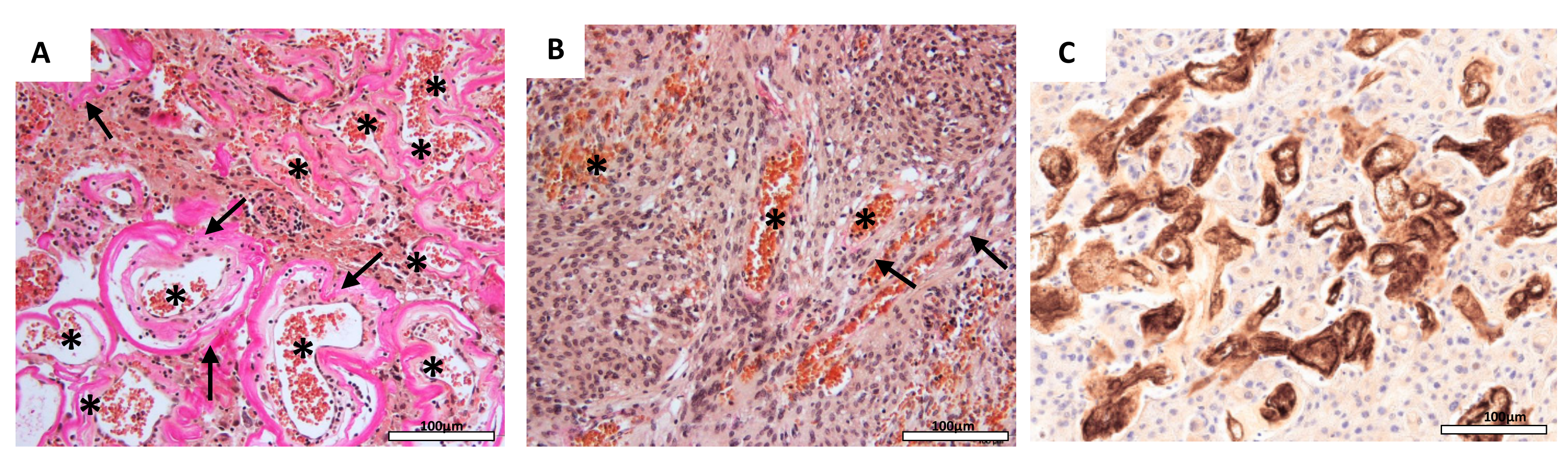
2.1. Vessel Density is Correlated with Fibrotic Tumor Vessels and Histopathological Tumor Subtypes
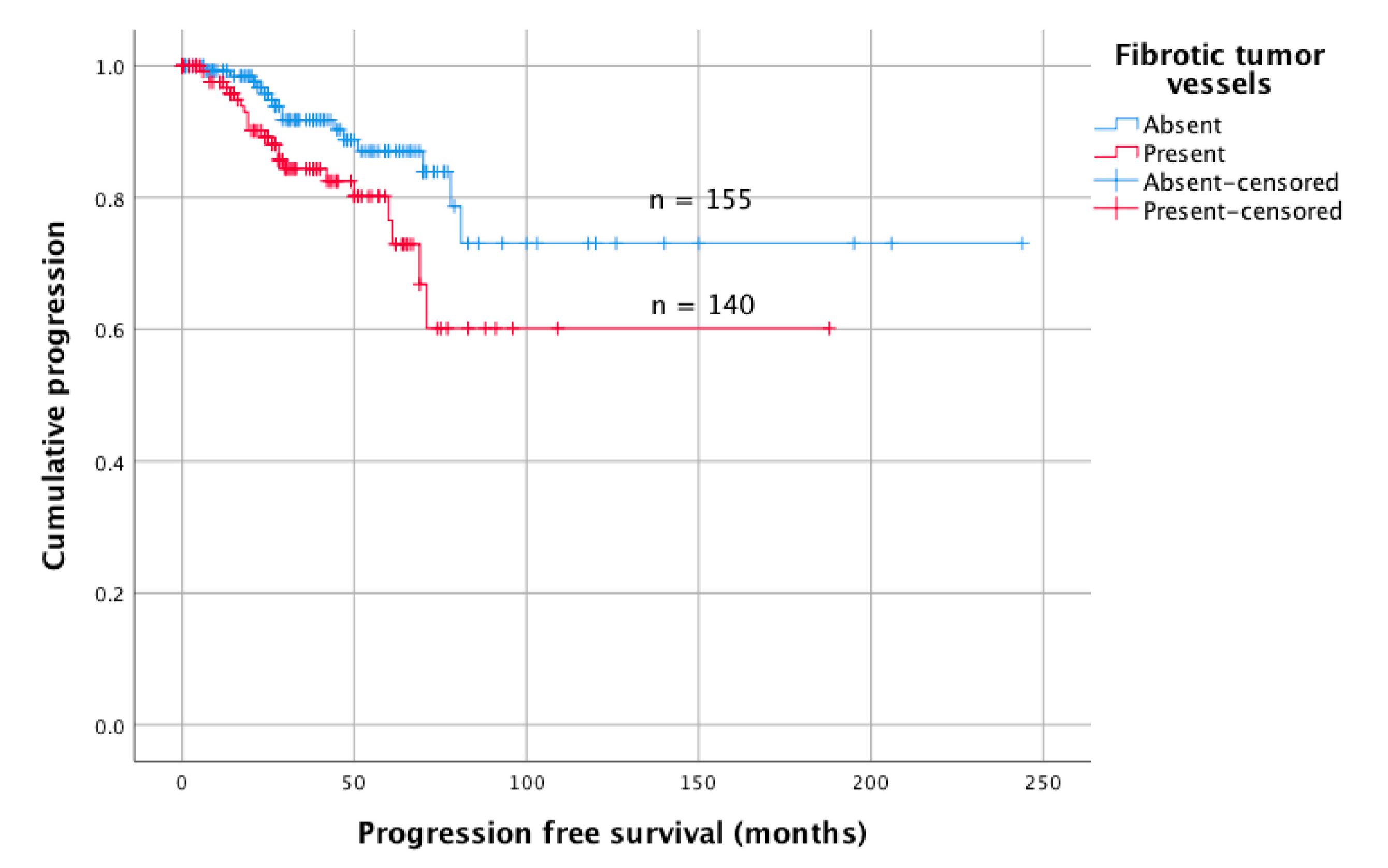
2.2. Vessel Fibrosis is Correlated with Tumor Recurrence
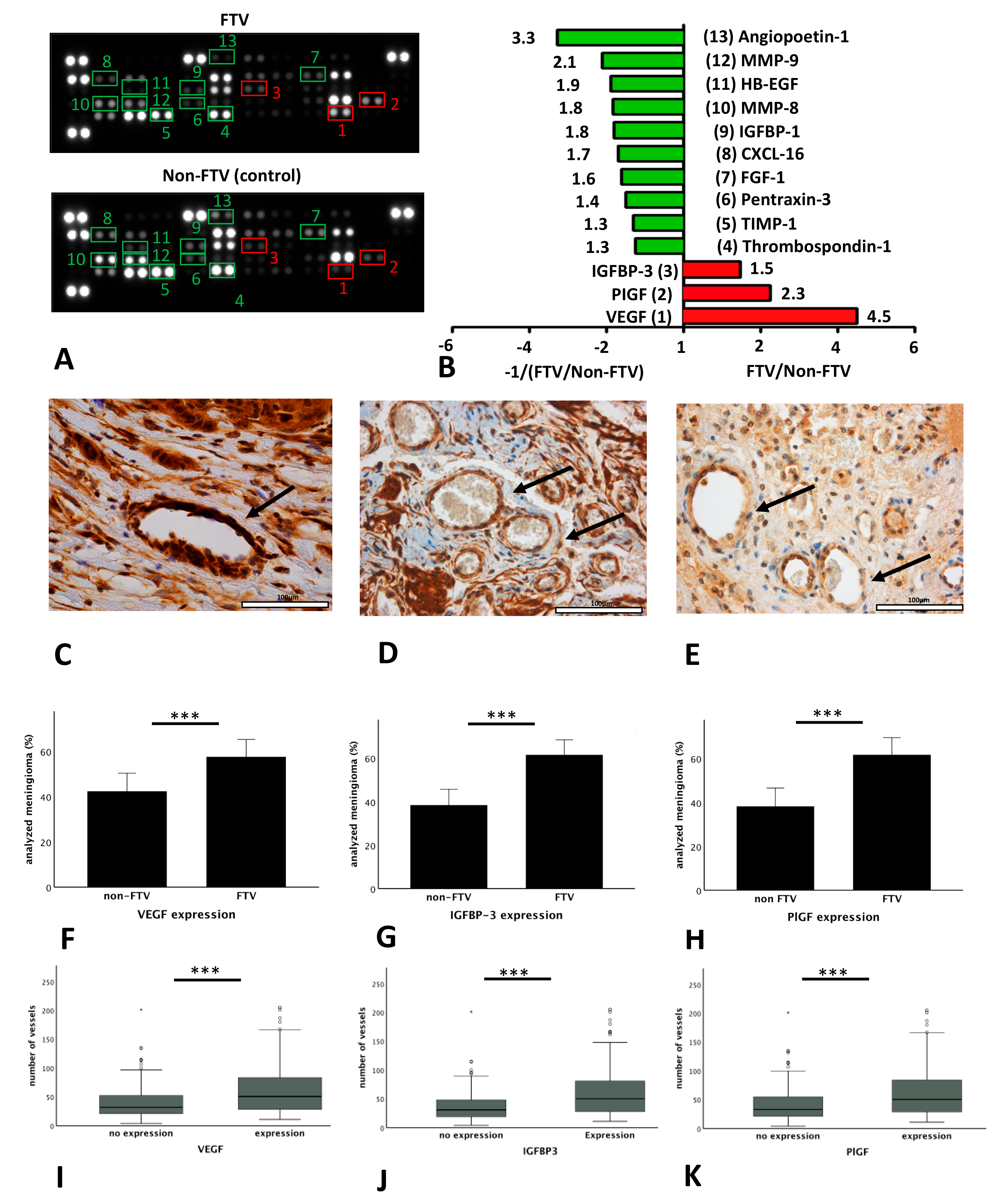
2.3. Expression of Angiogenesis Related Proteins Correlates with Vessel Fibrosis and Vessel Density
2.4. Vessel Fibrosis is Associated with Morphological Characteristics on MRI
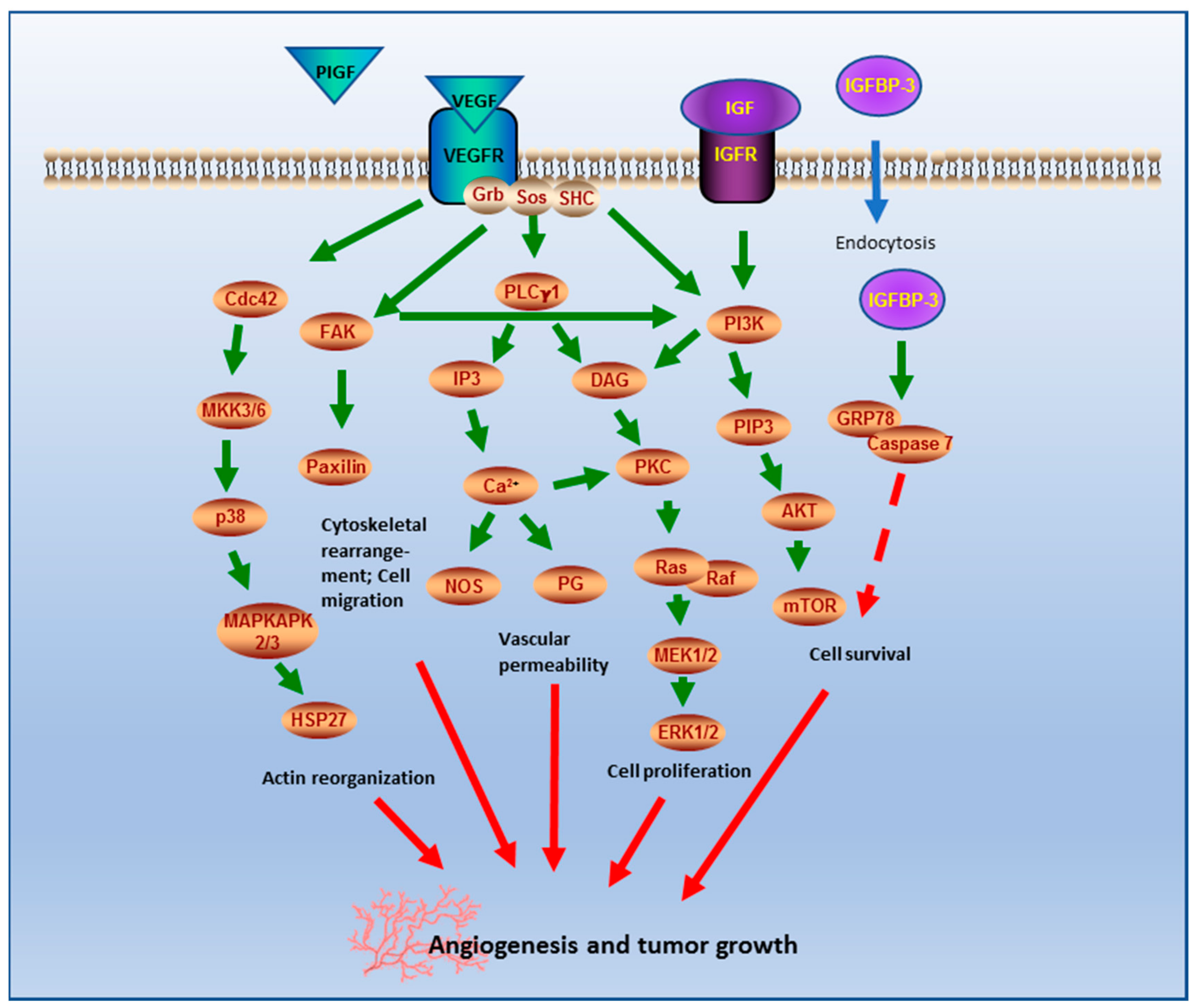
3. Discussion
4. Material and Methods
4.1. Data Collection
4.2. Histopathological Analyses
4.3. Proteome Profiling Array
4.4. Immunohistochemical Analysis
4.5. Radiological Imaging
4.6. Statistical Analyses
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Perry, A.; Louis, D.N.; von Deimling, A.; Sahm, F.; Rushing, E.J.; Mawrin, C.; Claus, E.B.; Loeffler, J.; Sadetzki, S. Meningiomas. In WHO Classification of Tumors of the Central Nervous System; Louis, D.N., Ohgaki, H., Wiestler, O.D., Cavenee, W.K., Ellison, D.W., Figarella-Branger, D., Perry, A., Reifenberger, G., von Deimlig, A., Eds.; International Agency on Cancer Research: Lyon, France, 2016; pp. 232–245. [Google Scholar]
- Saraf, S.; McCarthy, B.J.; Villano, J.L. Update on meningiomas. Oncologist 2011, 16, 1604–1613. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Alkemade, H.; de Leau, M.; Dieleman, E.M.; Kardaun, J.W.; van Os, R.; Vandertop, W.P.; van Furth, W.R.; Stalpers, L.J. Impaired survival and long-term neurological problems in benign meningioma. Neuro-Oncology 2012, 14, 658–666. [Google Scholar] [CrossRef] [PubMed]
- Corniola, M.V.; Lemée, J.M.; Meling, T.R. Histological transformation in recurrent WHO grade I meningiomas. Sci. Rep. 2020, 10, 11220. [Google Scholar] [CrossRef] [PubMed]
- Goldbrunner, R.; Minniti, G.; Preusser, M.; Jenkinson, M.D.; Sallabanda, K.; Houdart, E.; von Deimling, A.; Stavrinou, P.; Lefranc, F.; Lund-Johansen, M.; et al. EANO guidelines for the diagnosis and treatment of meningiomas. Lancet Oncol. 2016, 17, e383–e391. [Google Scholar] [CrossRef] [Green Version]
- Reuss, D.E.; Piro, R.M.; Jones, D.T.; Simon, M.; Ketter, R.; Kool, M.; Becker, A.; Sahm, F.; Pusch, S.; Meyer, J.; et al. Secretory meningiomas are defined by combined KLF4 K409Q and TRAF7 mutations. Acta Neuropathol. 2013, 125, 351–358. [Google Scholar] [CrossRef] [PubMed]
- Sahm, F.; Bissel, J.; Koelsche, C.; Schweizer, L.; Capper, D.; Reuss, D.; Böhmer, K.; Lass, U.; Göck, T.; Kalis, K.; et al. AKT1E17K mutations cluster with meningothelial and transitional meningiomas and can be detected by SFRP1 immunohistochemistry. Acta Neuropathol. 2013, 126, 757–762. [Google Scholar] [CrossRef]
- Paramasivam, N.; Hübschmann, D.; Toprak, U.H.; Ishaque, N.; Neidert, M.; Schrimpf, D.; Stichel, D.; Reuss, D.; Sievers, P.; Reinhardt, A.; et al. Mutational patterns and regulatory networks in epigenetic subgroups of meningioma. Acta Neuropathol. 2019, 138, 295–308. [Google Scholar] [CrossRef]
- Jungwirth, G.; Yu, T.; Moustafa, M.; Rapp, C.; Warta, R.; Jungk, C.; Sahm, F.; Dettling, S.; Zweckberger, K.; Lamszus, K.; et al. Identification of KIF11 As a Novel Target in Meningioma. Cancers 2019, 11, 545. [Google Scholar] [CrossRef] [Green Version]
- Kaley, T.J.; Wen, P.; Schiff, D.; Ligon, K.; Haidar, S.; Karimi, S.; Lassman, A.B.; Nolan, C.P.; DeAngelis, L.M.; Gavrilovic, I.; et al. Phase II trial of sunitinib for recurrent and progressive atypical and anaplastic meningioma. Neuro-Oncology 2015, 17, 116–121. [Google Scholar] [CrossRef] [Green Version]
- Lou, E.; Sumrall, A.L.; Turner, S.; Peters, K.B.; Desjardins, A.; Vredenburgh, J.J.; McLendon, R.E.; Herndon, J.E., 2nd; McSherry, F.; Norfleet, J.; et al. Bevacizumab therapy for adults with recurrent/progressive meningioma: A retrospective series. J. Neurooncol. 2012, 109, 63–70. [Google Scholar] [CrossRef] [Green Version]
- Raizer, J.J.; Grimm, S.A.; Rademaker, A.; Chandler, J.P.; Muro, K.; Helenowski, I.; Rice, L.; McCarthy, K.; Johnston, S.K.; Mrugala, M.M.; et al. A phase II trial of PTK787/ZK 222584 in recurrent or progressive radiation and surgery refractory meningiomas. J. Neurooncol. 2014, 117, 93–101. [Google Scholar] [CrossRef]
- Niu, G.; Chen, X. Vascular endothelial growth factor as an anti-angiogenic target for cancer therapy. Curr. Drug Targets 2010, 11, 1000–1017. [Google Scholar] [CrossRef]
- Barresi, V.; Tuccari, G. Increased ratio of vascular endothelial growth factor to semaphorin3A is a negative prognostic factor in human meningiomas. Neuropathology 2010, 30, 537–546. [Google Scholar] [CrossRef]
- Dasanu, C.A.; Samara, Y.; Codreanu, I.; Limonadi, F.M.; Hamid, O.; Alvarez-Argote, J. Systemic therapy for relapsed/refractory meningioma: Is there potential for antiangiogenic agents? J. Oncol. Pharm. Pract. 2019, 25, 638–647. [Google Scholar] [CrossRef]
- Pistolesi, S.; Boldrini, L.; Gisfredi, S.; De Ieso, K.; Camacci, T.; Caniglia, M.; Lupi, G.; Leocata, P.; Basolo, F.; Pingitore, R.; et al. Angiogenesis in intracranial meningiomas: Immunohistochemical and molecular study. Neuropathol. Appl. Neurobiol. 2004, 30, 118–125. [Google Scholar] [CrossRef]
- Karsy, M.; Burnett, B.; Di Ieva, A.; Cusimano, M.D.; Jensen, R.L. Microvascularization of Grade I meningiomas: Effect on tumor volume, blood loss, and patient outcome. J. Neurosurg. 2018, 128, 657–666. [Google Scholar] [CrossRef] [Green Version]
- Hasselblatt, M.; Nolte, K.W.; Paulus, W. Angiomatous meningioma: A clinicopathologic study of 38 cases. Am. J. Surg. Pathol. 2004, 28, 390–393. [Google Scholar] [CrossRef]
- Probst-Cousin, S.; Villagran-Lillo, R.; Lahl, R.; Bergmann, M.; Schmid, K.W.; Gullotta, F. Secretory meningioma. Cancer 1997, 79, 2003–2015. [Google Scholar] [CrossRef]
- Ben Nsir, A.; Chabaane, M.; Krifa, H.; Jeme, H.; Hattab, N. Intracranial angiomatous meningiomas: A 15-year, multicenter study. Clin. Neurol. Neurosurg. 2016, 149, 111–117. [Google Scholar] [CrossRef]
- Hua, L.; Luan, S.; Li, H.; Zhu, H.; Tang, H.; Liu, H.; Chen, X.; Bozinov, O.; Xie, Q.; Gong, Y. Angiomatous Meningiomas Have a Very Benign Outcome Despite Frequent Peritumoral Edema at Onset. World Neurosurg. 2017, 108, 465–473. [Google Scholar] [CrossRef]
- Ferrara, N.; Davis-Smyth, T. The biology of vascular endothelial growth factor. Endocr. Rev. 1997, 18, 4–25. [Google Scholar] [CrossRef]
- Huang, H.; Held-Feindt, J.; Buhl, R.; Mehdorn, H.M.; Mentlein, R. Expression of VEGF and its receptors in different brain tumors. Neurol. Res. 2005, 27, 371–377. [Google Scholar] [CrossRef]
- Nishikawa, R.; Cheng, S.Y.; Nagashima, R.; Huang, H.J.; Cavenee, W.K.; Matsutani, M. Expression of vascular endothelial growth factor in human brain tumors. Acta Neuropathol. 1998, 96, 453–462. [Google Scholar] [CrossRef]
- Lamszus, K.; Lengler, U.; Schmidt, N.O.; Stavrou, D.; Ergun, S.; Westphal, M. Vascular endothelial growth factor, hepatocyte growth factor/scatter factor, basic fibroblast growth factor, and placenta growth factor in human meningiomas and their relation to angiogenesis and malignancy. Neurosurgery 2000, 46, 938–947. [Google Scholar]
- Lee, S.H.; Lee, Y.S.; Hong, Y.G.; Kang, C.S. Significance of COX-2 and VEGF expression in histopathologic grading and invasiveness of meningiomas. APMIS 2014, 122, 16–24. [Google Scholar] [CrossRef]
- Reszec, J.; Hermanowicz, A.; Rutkowski, R.; Turek, G.; Mariak, Z.; Chyczewski, L. Expression of MMP-9 and VEGF in meningiomas and their correlation with peritumoral brain edema. Biomed. Res. Int. 2015, 2015, 646853. [Google Scholar] [CrossRef]
- Bordeleau, F.; Mason, B.N.; Lollis, E.M.; Mazzola, M.; Zanotelli, M.R.; Somasegar, S.; Califano, J.P.; Montague, C.; LaValley, D.J.; Huynh, J.; et al. Matrix stiffening promotes a tumor vasculature phenotype. Proc. Natl. Acad. Sci. USA 2017, 114, 492–497. [Google Scholar] [CrossRef] [Green Version]
- Parr, C.; Watkins, G.; Boulton, M.; Cai, J.; Jiang, W.G. Placenta growth factor is over-expressed and has prognostic value in human breast cancer. Eur. J. Cancer 2005, 41, 2819–2827. [Google Scholar] [CrossRef]
- Wei, S.C.; Tsao, P.N.; Yu, S.C.; Shun, C.T.; Tsai-Wu, J.J.; Wu, C.H.; Su, Y.N.; Hsieh, F.J.; Wong, J.M. Placenta growth factor expression is correlated with survival of patients with colorectal cancer. Gut 2005, 54, 666–672. [Google Scholar] [CrossRef] [Green Version]
- Donnini, S.; Machein, M.R.; Plate, K.H.; Weich, H.A. Expression and localization of placenta growth factor and PlGF receptors in human meningiomas. J. Pathol. 1999, 189, 66–71. [Google Scholar] [CrossRef]
- Weindel, K.; Moringlane, J.R.; Marme, D.; Weich, H.A. Detection and quantification of vascular endothelial growth factor/vascular permeability factor in brain tumor tissue and cyst fluid: The key to angiogenesis? Neurosurgery 1994, 35, 439–448. [Google Scholar] [CrossRef] [PubMed]
- Johnson, M.A.; Firth, S.M. IGFBP-3: A cell fate pivot in cancer and disease. Growth Horm. IGF Res. 2014, 24, 164–173. [Google Scholar] [CrossRef] [PubMed]
- Yamada, P.M.; Lee, K.W. Perspectives in mammalian IGFBP-3 biology: Local vs. systemic action. Am. J. Physiol. Cell Physiol. 2009, 296, C954–C976. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tarsitano, A.; Asioli, S.; Morandi, L.; Monti, V.; Righi, A.; Morselli Labate, A.M.; Nardi, E.; Foschini, M.P.; Marchetti, C. Laminin-5 and insulin-like growth factor-II mRNA binding protein-3 (IMP3) expression in preoperative biopsy specimens from oral cancer patients: Their role in neural spread risk and survival stratification. J. Craniomaxillofac. Surg. 2016, 44, 1896–1902. [Google Scholar] [CrossRef]
- Yamamoto, N.; Oshima, T.; Yoshihara, K.; Aoyama, T.; Hayashi, T.; Yamada, T.; Sato, T.; Shiozawa, M.; Yoshikawa, T.; Morinaga, S.; et al. Clinicopathological significance and impact on outcomes of the gene expression levels of IGF-1, IGF-2 and IGF-1R, IGFBP-3 in patients with colorectal cancer: Overexpression of the IGFBP-3 gene is an effective predictor of outcomes in patients with colorectal cancer. Oncol. Lett. 2017, 13, 3958–3966. [Google Scholar]
- Wrobel, G.; Roerig, P.; Kokocinski, F.; Neben, K.; Hahn, M.; Reifenberger, G.; Lichter, P. Microarray-based gene expression profiling of benign, atypical and anaplastic meningiomas identifies novel genes associated with meningioma progression. Int. J. Cancer 2005, 114, 249–256. [Google Scholar] [CrossRef]
- Norden, A.D.; Drappatz, J.; Wen, P.Y. Targeted drug therapy for meningiomas. Neurosurg. Focus 2007, 23, E12. [Google Scholar] [CrossRef]
- Kim, J.H.; Choi, D.S.; Lee, O.H.; Oh, S.H.; Lippman, S.M.; Lee, H.Y. Antiangiogenic antitumor activities of IGFBP-3 are mediated by IGF-independent suppression of Erk1/2 activation and Egr-1-mediated transcriptional events. Blood 2011, 118, 2622–2631. [Google Scholar] [CrossRef] [Green Version]
- De Falco, S. The discovery of placenta growth factor and its biological activity. Exp. Mol. Med. 2012, 44, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Moazzam, A.A.; Wagle, N.; Zada, G. Recent developments in chemotherapy for meningiomas: A review. Neurosurg. Focus 2013, 35, E18. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.A.; Sun, Y.; Palmer, J.; Solomides, C.; Huang, L.C.; Shyr, Y.; Dicker, A.P.; Lu, B. IGFBP3 modulates lung tumorigenesis and cell growth through IGF1 signaling. Mol. Cancer Res. 2017, 15, 896–904. [Google Scholar] [CrossRef] [Green Version]
- Karsy, M.; Azab, M.A.; Abou-Al-Shaar, H.; Guan, J.; Eli, I.; Jensen, R.L.; Ormond, D.R. Clinical potential of meningioma genomic insights: A practical review for neurosurgeons. Neurosurg. Focus 2018, 44, E10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sahm, F.; Schrimpf, D.; Stichel, D.; Jones, D.T.W.; Hielscher, T.; Schefzyk, S.; Okonechnikov, K.; Koelsche, C.; Reuss, D.E.; Capper, D.; et al. DNA methylation-based classification and grading system for meningioma: A multicentre, retrospective analysis. Lancet Oncol. 2017, 18, 682–694. [Google Scholar] [CrossRef] [Green Version]
- Strieter, R.M.; Belperio, J.A.; Keane, M.P. CXC chemokines in angiogenesis related to pulmonary fibrosis. Chest 2002, 122, 298S–301S. [Google Scholar] [CrossRef] [PubMed]
- Abraham, D.J.; Varga, J. Scleroderma: From cell and molecular mechanisms to disease models. Trends Immunol. 2005, 26, 587–595. [Google Scholar] [CrossRef] [PubMed]
- Mayes, M.D. Scleroderma epidemiology. Rheum. Dis. Clin. N. Am. 1996, 22, 751–764. [Google Scholar] [CrossRef]
- Kikuchi, K.; Kubo, M.; Kadono, T.; Yazawa, N.; IHN, H.; Tamaki, K. Serum concentrations of vascular endothelial growth factor in collagen diseases. Br. J. Dermatol. 1998, 139, 1049–1051. [Google Scholar] [CrossRef]
- Arevalo, J.F.; Sanchez, J.G.; Lasave, A.F.; Wu, L.; Maia, M.; Bonafonte, S.; Brito, M.; Alezzandrini, A.A.; Restrepo, N.; Berrocal, M.H.; et al. Intravitreal Bevacizumab (Avastin) for Diabetic Retinopathy: The 2010 GLADAOF Lecture. J. Ophthalmol. 2011, 2011, 584238. [Google Scholar] [CrossRef]
- Zhang, X.; Wu, J.; Wu, C.; Bian, A.L.; Geng, S.; Dai, R.P. Comparison of aqueous humor levels of PlGF and VEGF in proliferative diabetic retinopathy before and after intravitreal conbercept injection. Diabetes Res. Clin. Pract. 2020, 162, 108083. [Google Scholar] [CrossRef]
- Holm, P.W.; Slart, R.H.; Zeebregts, C.J.; Hillebrands, J.L.; Tio, R.A. Atherosclerotic plaque development and instability: A dual role for VEGF. Ann. Med. 2009, 41, 257–264. [Google Scholar] [CrossRef]
- Heinonen, S.E.; Kivela, A.M.; Huusko, J.; Dijkstra, M.H.; Gurzeler, E.; Makinen, P.I.; Leppanen, P.; Olkkonen, V.M.; Eriksson, U.; Jauhiainen, M.; et al. The effects of VEGF-A on atherosclerosis, lipoprotein profile, and lipoprotein lipase in hyperlipidaemic mouse models. Cardiovasc. Res. 2013, 99, 716–723. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Viallard, C.; Larrivée, B. Tumor angiogenesis and vascular normalization: Alternative therapeutic targets. Angiogenesis 2017, 20, 409–426. [Google Scholar] [CrossRef] [PubMed]
- Spille, D.C.; Sporns, P.B.; Hess, K.; Stummer, W.; Brokinkel, B. Prediction of High-Grade Histology and Recurrence in Meningiomas Using Routine Preoperative Magnetic Resonance Imaging: A Systematic Review. World Neurosurg. 2019, 128, 174–181. [Google Scholar] [CrossRef]
- Uchida, H.; Hirano, H.; Moinuddin, F.M.; Hanaya, R.; Sadamura, Y.; Hosoyama, H.; Yonezawa, H.; Tokimura, H.; Yamahata, H.; Arita, K. Radiologic and histologic features of the T2 hyperintensity rim of meningiomas on magnetic resonance images. Neuroradiol. J. 2017, 30, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Adeli, A.; Hess, K.; Mawrin, C.; Streckert, E.M.S.; Stummer, W.; Paulus, W.; Kemmling, A.; Holling, M.; Heindel, W.; Schmidt, R.; et al. Prediction of brain invasion in patients with meningiomas using preoperative magnetic resonance imaging. Oncotarget 2018, 9, 35974–35982. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brokinkel, B.; Holling, M.; Spille, D.C.; Hess, K.; Sauerland, C.; Bleimuller, C.; Paulus, W.; Wolfer, J.; Stummer, W. Surgery for meningioma in the elderly and long-term survival: Comparison with an age- and sex-matched general population and with younger patients. J. Neurosurg. 2017, 126, 1201–1211. [Google Scholar] [CrossRef] [Green Version]
- Hess, K.; Spille, D.C.; Adeli, A.; Sporns, P.B.; Brokinkel, C.; Grauer, O.; Mawrin, C.; Stummer, W.; Paulus, W.; Brokinkel, B. Brain invasion and the risk of seizures in patients with meningioma. J. Neurosurg. 2018, 130, 789–796. [Google Scholar] [CrossRef] [Green Version]
- Sicking, J.; Voss, K.M.; Spille, D.C.; Schipmann, S.; Holling, M.; Paulus, W.; Hess, K.; Steinbicker, A.U.; Stummer, W.; Grauer, O.; et al. The evolution of cranial meningioma surgery-a single-center 25-year experience. Acta Neurochir. 2018, 160, 1801–1812. [Google Scholar] [CrossRef]
- Spille, D.C.; Hess, K.; Sauerland, C.; Sanai, N.; Stummer, W.; Paulus, W.; Brokinkel, B. Brain Invasion in Meningiomas: Incidence and Correlations with Clinical Variables and Prognosis. World Neurosurg. 2016, 93, 346–354. [Google Scholar] [CrossRef]
- Voss, K.M.; Spille, D.C.; Sauerland, C.; Suero Molina, E.; Brokinkel, C.; Paulus, W.; Stummer, W.; Holling, M.; Jeibmann, A.; Brokinkel, B. The Simpson grading in meningioma surgery: Does the tumor location influence the prognostic value? J. Neurooncol. 2017, 133, 641–651. [Google Scholar] [CrossRef]
- Simpson, D. The recurrence of intracranial meningiomas after surgical treatment. J. Neurol. Neurosurg. Psychiatry 1957, 20, 22–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ling, C.; Pouget, C.; Rech, F.; Pflaum, R.; Treffel, M.; Bielle, F.; Mokhtari, K.; Casse, J.M.; Vignaud, J.M.; Kalamarides, M.; et al. Endothelial Cell Hypertrophy and Microvascular Proliferation in Meningiomas Are Correlated with Higher Histological Grade and Shorter Progression-Free Survival. J. Neuropathol. Exp. Neurol. 2016, 75, 1160–1170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peetz-Dienhart, S.; Spille, D.C.; Sporns, P.B.; Adeli, A.; Bunk, E.C.; Wagner, A.; Paulus, W.; Stummer, W.; Hess, K.; Brokinkel, B. Letter: Parasagittal/Falcine Tumor Location Strongly Predicts Human Telomerase Reverse Transcriptase Promoter Mutations in High-Grade Meningiomas. Neurosurgery 2020, 86, E362–E365. [Google Scholar] [CrossRef] [PubMed]
- Streckert, E.M.S.; Hess, K.; Sporns, P.B.; Adeli, A.; Brokinkel, C.; Kriz, J.; Holling, M.; Eich, H.T.; Paulus, W.; Spille, D.C.; et al. Clinical, radiological, and histopathological predictors for long-term prognosis after surgery for atypical meningiomas. Acta Neurochir. 2019, 161, 1647–1656. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Frequency n (%) |
|---|---|
| Primary diagnosis | 275 (93%) |
| Recurrence | 20 (7%) |
| Age (median, range) | 57 years (16–88 years) |
| Males | 77 (26%) |
| Females | 218 (74%) |
| Extent of resection | |
| Gross total (GTR, Simpson I/II) | 199 (70%) |
| Subtotal (STR, Simpson III-V) | 84 (30%) |
| Histopathological subtype | |
| Meningothelial | 185 (63%) |
| Transitional | 84 (29%) |
| Angiomatous | 4 (1%) |
| Fibrous | 12 (4%) |
| Secretory | 10 (3%) |
| Tumor location | |
| Convexity | 93 (32%) |
| Falx/parasagittal | 38 (13%) |
| Skull base | 146 (49%) |
| Posterior fossa | 14 (5%) |
| Intraventricular | 4 (1%) |
| Tumor/edema volume | |
| Tumor volume (median, range) | 10.00 ccm (0.02–267.77 ccm) |
| Edema volume (median, range) | 0.00 ccm (0.00–364.63 ccm) |
| Intensity on T2-weighted MRI | |
| Hypointense | 143 (52%) |
| Isointense | 17 (6%) |
| Hyperintense | 114 (42%) |
| Further radiological criteria | |
| Arachnoid layer disrupted/absent | 154 (52%) |
| Heterogeneous T1 contrast enhancement | 127 (44%) |
| Tumor shape irregular | 108 (38%) |
| Tumor calcifications | 64 (23%) |
| Capsular contrast enhancement | 100 (37%) |
| Variable | Frequency n(%) | ||
|---|---|---|---|
| Indication for Surgery | non-FTV | FTV | p-Value |
| Primary diagnosis | 144 (49%) | 131 (44%) | 0.503 |
| Recurrence | 11 (4%) | 9 (3%) | |
| Age (mean, range) | 58 years (16–88 years) | 55 years (16–88 years) | 0.065 |
| Sex | 0.288 | ||
| Male | 36 (12%) | 41 (14%) | |
| Female | 119 (40%) | 99 (34%) | |
| Extent of resection | |||
| Gross total (GTR, Simpson I/II) | 110 (39%) | 89 (31%) | 0.136 |
| Subtotal (STR, Simpson III/IV) | 37 (13%) | 47 (17%) | |
| Histopathological subtype | 0.136 | ||
| Meningothelial | 92 (31%) | 93 (32%) | |
| Transitional | 50 (17%) | 34 (12%) | |
| Angiomatous | 0 (0%) | 4 (1%) | |
| Fibrous | 7 (2%) | 5 (2%) | |
| Secretory | 6 (2%) | 4 (1%) | |
| Tumor location | 0.493 | ||
| Convexity | 50 (17%) | 43 (15%) | |
| Falx/parasagittal | 22 (8%) | 16 (5%) | |
| Skull base | 71 (24%) | 75 (25%) | |
| Posterior fossa | 10 (3%) | 4 (1%) | |
| Intraventricular | 2 (1%) | 2 (1%) | |
| Angiogenic proteins | |||
| IGFBP-3 expression/absent | 68 (24%)/82 (28%) | 109 (38%)/29 (10%) | <0.001 |
| PIGF expression/absent | 52 (18%)/99 (34%) | 84 (29%)/55 (19%) | <0.001 |
| VEGF expression/absent | 64 (22%)/88 (30%) | 87 (30%)/52 (18%) | <0.001 |
| Vessel density (vessels/4 HPF) | 35.8 ± 28.0 | 72.2 ± 42.8 | <0.001 |
| Variable | Frequency n (%) | ||
|---|---|---|---|
| non-FTV | FTV | p-Value | |
| Tumor/edema volume | |||
| Tumor volume (median, range) | 10.36 ccm (0.02–141.91 ccm) | 9.97 ccm (0.21–267.77 ccm) | 0.108 |
| Edema volume (median, range) | 0.00 ccm (0.00–364.63) | 0.47 ccm (0.00–355.80) | 0.621 |
| Intensity on T2-weighted MRI | 0.346 | ||
| Hypointense | 72 (26%) | 71 (26%) | |
| Isointense | 9 (3%) | 8 (3%) | |
| Hyperintense | 59 (22%) | 55 (20%) | |
| Further radiological criteria | |||
| Arachnoid layer disrupted/absent | 56 (19%)/99 (34%) | 98 (33%)/42 (14%) | <0.001 |
| Heterogeneous T1 contrast enhancement | 62 (22%) | 65 (23%) | 0.429 |
| Tumor shape irregular | 47 (17%) | 61 (22%) | 0.051 |
| Tumor calcifications | 35 (13%) | 29 (11%) | 0.480 |
| Capsular contrast enhancement | 58 (22%) | 42 (16%) | 0.077 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hess, K.; Spille, D.C.; Adeli, A.; Sporns, P.B.; Zitta, K.; Hummitzsch, L.; Pfarr, J.; Stummer, W.; Brokinkel, B.; Berndt, R.; et al. Occurrence of Fibrotic Tumor Vessels in Grade I Meningiomas Is Strongly Associated with Vessel Density, Expression of VEGF, PlGF, IGFBP-3 and Tumor Recurrence. Cancers 2020, 12, 3075. https://doi.org/10.3390/cancers12103075
Hess K, Spille DC, Adeli A, Sporns PB, Zitta K, Hummitzsch L, Pfarr J, Stummer W, Brokinkel B, Berndt R, et al. Occurrence of Fibrotic Tumor Vessels in Grade I Meningiomas Is Strongly Associated with Vessel Density, Expression of VEGF, PlGF, IGFBP-3 and Tumor Recurrence. Cancers. 2020; 12(10):3075. https://doi.org/10.3390/cancers12103075
Chicago/Turabian StyleHess, Katharina, Dorothee Cäcilia Spille, Alborz Adeli, Peter B. Sporns, Karina Zitta, Lars Hummitzsch, Julian Pfarr, Walter Stummer, Benjamin Brokinkel, Rouven Berndt, and et al. 2020. "Occurrence of Fibrotic Tumor Vessels in Grade I Meningiomas Is Strongly Associated with Vessel Density, Expression of VEGF, PlGF, IGFBP-3 and Tumor Recurrence" Cancers 12, no. 10: 3075. https://doi.org/10.3390/cancers12103075
APA StyleHess, K., Spille, D. C., Adeli, A., Sporns, P. B., Zitta, K., Hummitzsch, L., Pfarr, J., Stummer, W., Brokinkel, B., Berndt, R., & Albrecht, M. (2020). Occurrence of Fibrotic Tumor Vessels in Grade I Meningiomas Is Strongly Associated with Vessel Density, Expression of VEGF, PlGF, IGFBP-3 and Tumor Recurrence. Cancers, 12(10), 3075. https://doi.org/10.3390/cancers12103075