Systematic Review of Patient-Reported Outcomes following Surgical Treatment of Lymphedema


Abstract
:1. Introduction
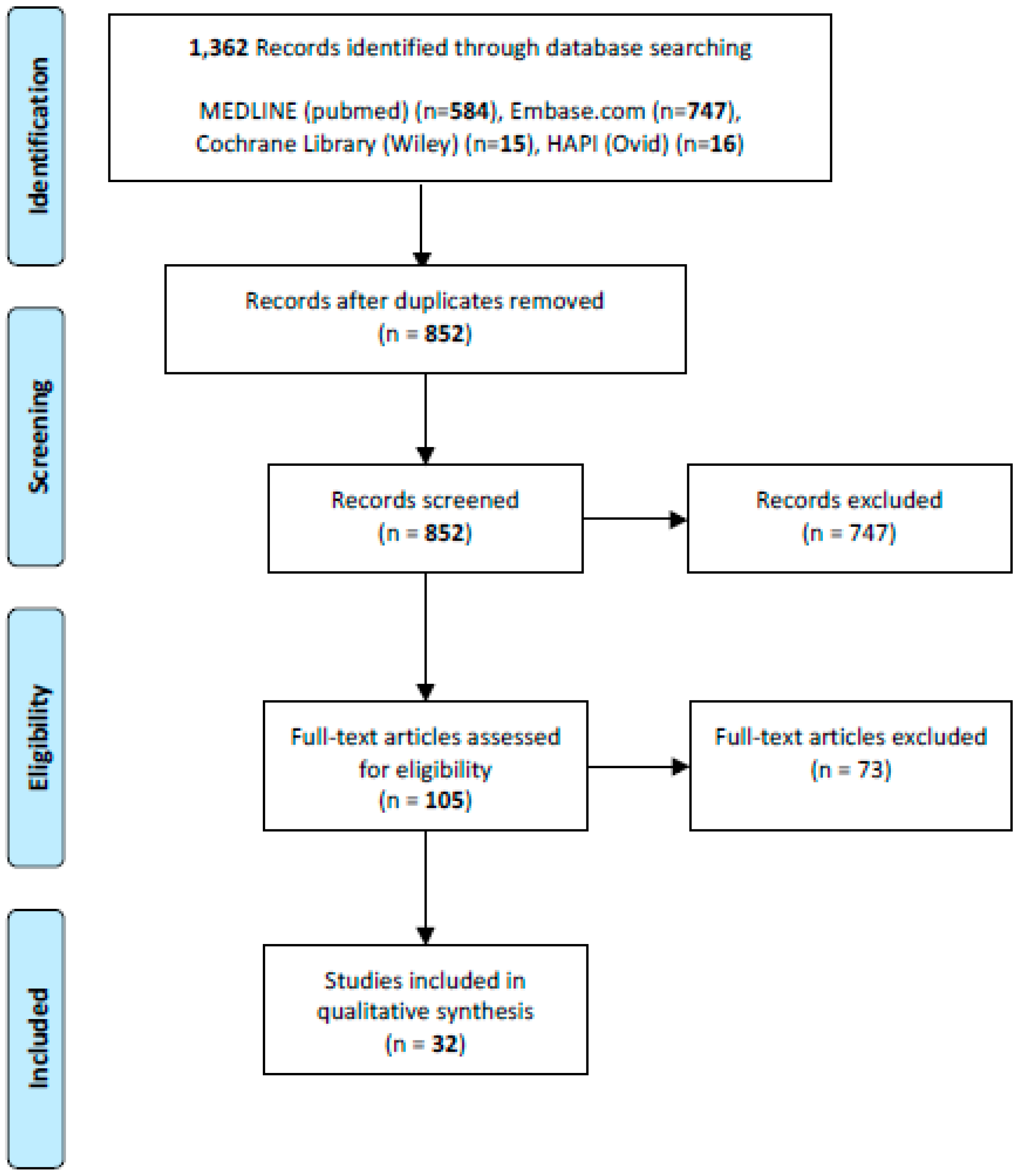
2. Methods
3. Results
3.1. Patient-Reported Outcomes after LVB
3.1.1. Ad-Hoc Patient Questionnaires
3.1.2. LYMQOL
3.1.3. Lymph-ICF
3.1.4. SF-36
3.2. Patient-Reported Outcomes after VLNT
3.2.1. Ad-Hoc Patient Questionnaires
3.2.2. LYMQOL
3.2.3. ULL27
3.2.4. LLIS
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Lawenda, B.D.M.T.; Johnstone, P.A.S. Lymphedema: A primer on the identification and management of a chronic condition in oncologic treatment. Cancer J. Clin. 2009, 59, 8–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ribeiro Pereira, A.C.P.K.R.; Bergmann, A. Incidence and risk factors of lymphedema after breast cancer treatment: 10 years of follow-up. Breast 2017, 36, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Cormier, J.N.A.R.; Mungovan, K.S.; Xing, Y.; Ross, M.I.; Armer, J.M. Lymphedema beyond breast cancer. Cancer 2010, 116, 5138–5149. [Google Scholar] [CrossRef] [PubMed]
- Todo, Y.Y.R.; Minobe, S.; Suzuki, Y.; Takeshi, U.; Nakatani, M.; Aoyagi, Y.; Ohba, Y.; Okamoto, K.; Kato, H. Risk factors for postoperative lower-extremity lymphedema in endometrial cancer survivors who had treatment including lymphadenectomy. Gynecol. Oncol. 2010, 119, 60–64. [Google Scholar] [CrossRef]
- Zou, L.L.F.; Shen, P.P.; Hu, Y.; Liu, X.Q.; Xu, Y.Y.; Pen, Q.L.; Wang, B.; Zhu, Y.Q.; Tian, Y. The incidence and risk factors of related lymphedema for breast cancer survivors post-operation: A 2-year follow-up prospective cohort study. Breast Cancer 2018, 5, 309–314. [Google Scholar] [CrossRef]
- Carlson, J.W.K.J.; Hutson, A.; Carter, J.; Armer, J.; Lockwood, S.; Nolte, S.; Stewart, B.R.; Wenzel, L.; Walker, J.; Fleury, A.; et al. GOG 244-The lymphedema and gynecologic cancer (LEG) study: Incidence and risk factors in newly diagnosed patients. Gynecol. Oncol. 2020, 156, 467–474. [Google Scholar] [CrossRef]
- Zhang, Z.Z.X.; Chen, S.; Jiang, J.; Qi, R.; Zhang, X.; Xi, Y.; Li, M.; Zheng, H.; Hua, B. Taxane-based chemotherapy and risk of breast cancer-related lymphedema: Protocol for a systematic review and meta-analysis. Medicine 2019, 98, e16563. [Google Scholar] [CrossRef]
- Byun, H.K.C.J.; Im, S.H.; Kirova, Y.M.; Arsene-Henry, A.; Choi, S.H.; Cho, Y.U.; Park, H.S.; Kim, J.Y.; Suh, C.O.; Keum, K.C.; et al. Risk of Lymphedema Following Contemporary Treatment for Breast Cancer: An Analysis of 7617 Consecutive Patients From a Multidisciplinary Perspective. Ann. Surg. 2019. epub ahead of print. [Google Scholar] [CrossRef]
- Michelotti, A.I.M.; Lopez, G.; Lorenzini, D.; Nesa, F.; De Sire, A.; Fusco, N. Tackling the diversity of breast cancer related lymphedema: Perspectives on diagnosis, risk assessment, and clinical management. Breast 2019, 44, 15–23. [Google Scholar] [CrossRef]
- Huang, J.Y.N.; Wang, X.; Long, X. Incidence of lower limb lymphedema after vulvar cancer: A systematic review and meta-analysis. Medicine 2017, 96, e8722. [Google Scholar] [CrossRef]
- Lindqvist, E.W.M.; Fredrikson, M.; Kjølhede, P. Lymphedema after treatment for endometrial cancer—A review of prevalence and risk factors. Eur. J. Obstet. Gynecol. Reprod. Biol. 2017, 211, 112–121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, A.M.J. Lymphedema. JAMA Oncol. 2018, 4, 755. [Google Scholar] [CrossRef] [PubMed]
- Warren, A.G.B.H.; Borud, L.J.; Slavin, S.A. Lymphedema: A comprehensive review. Ann. Plast. Surg. 2007, 59, 464–472. [Google Scholar] [CrossRef] [PubMed]
- Hayes, S.C.J.K.; Stout, N.L.; Prosnitz, R.; Armer, J.M.; Gabram, S.; Schmitz, K.H. Upper-body morbidity after breast cancer: Incidence and evidence for evaluation, prevention, and management within a prospective surveillance model of care. Cancer 2012, 118, 2237–2249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hormes, J.M.B.C.; Lytle, L.A.; Gross, C.R.; Ahmed, R.L.; Troxel, A.B.; Schmitz, K.H. Impact of lymphedema and arm symptoms on quality of life in breast cancer survivors. Lymphology 2010, 43, 1–13. [Google Scholar] [PubMed]
- Keeley, V.C.S.; Locke, J.; Veigas, D.; Riches, K.; Hilliam, R. A quality of life measure for limb lymphoedema (LYMQOL). J. Lymphoedema 2010, 5, 26–37. [Google Scholar]
- Launois, R.M.A.; Pocquet, K.; Alliot, F. A specific quality of life scale in upper limb lymphoedema: The ULL-27 questionnaire. Lymphology 2002, 35, 181–187. [Google Scholar] [CrossRef] [Green Version]
- Devoogdt, N.V.K.M.; Geraerts, I.; Coremans, T.; Christiaens, M.R. Lymphoedema Functioning, Disability and Health questionnaire (Lymph-ICF): Reliability and validity. Phys. Ther. 2011, 91, 944–957. [Google Scholar] [CrossRef]
- Weiss, J.D.T. Validation of the Lymphedema Life Impact Scale (LLIS): A Condition-Specific Measurement Tool for Persons with Lymphedema. Lymphology 2015, 48, 128–138. [Google Scholar]
- Treanor, C.D.M. A methodological review of the Short Form Health Survey 36 (SF-36) and its derivatives among breast cancer survivors. Qual. Life Res. 2015, 24, 339–362. [Google Scholar] [CrossRef]
- Carl, H.M.W.G.; Bello, R.; Clarke-Pearson, E.; Hassanein, A.H.; Cho, B.; Pedreira, R.; Sacks, J.M. Systematic Review of the Surgical Treatment of Extremity Lymphedema. J. Reconstr. Microsurg. 2017, 33, 412–425. [Google Scholar] [CrossRef] [PubMed]
- Cochrane Handbook for Systematic Reviews of Interventions, Version 5.1.0 ed.; The Cochrane Collaboration: London, UK, 2011.
- Bramer, W.M.G.D.; de Jonge, G.B.; Holland, L.; Bekhuis, T. De-duplication of database search results for systematic reviews in EndNote. J. Med. Libr. Assoc. 2016, 4, 240–243. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, B.M.; Mellow, C.G.; Khazanchi, R.K.; Dvir, E.; Kumar, V.; Pederson, W.C. Long-term results after microlymphaticovenous anastomoses for the treatment of obstructive lymphedema. Plast. Reconstr. Surg. 1990, 85, 562–572. [Google Scholar] [CrossRef] [PubMed]
- Demirtas, Y.O.N.; Yapici, O.; Topalan, M. Supermicrosurgical lymphaticovenular anastomosis and lymphaticovenous implantation for treatment of unilateral lower extremity lymphedema. Microsurgery 2009, 29, 609–618. [Google Scholar] [CrossRef] [PubMed]
- Auba, C.; Marre, D.; Rodriguez-Losada, G.; Hontanilla, B. Lymphaticovenular anastomoses for lymphedema treatment: 18 months postoperative outcomes. Microsurgery 2012, 32, 261–268. [Google Scholar] [CrossRef]
- Ayestaray, B.B.F.; Andreoletti, J.B. Patent blue-enhanced lymphaticovenular anastomosis. J. Plast. Reconstr. Aesthet. Surg. 2013, 66, 382–389. [Google Scholar] [CrossRef]
- Chang, D.W. Lymphaticovenular bypass for lymphedema management in breast cancer patients: A prospective study. Plast. Reconstr. Surg. Glob. Open. 2010, 126, 752–758. [Google Scholar] [CrossRef] [Green Version]
- Chang, D.W.; Suami, H.; Skoracki, R. A prospective analysis of 100 consecutive lymphovenous bypass cases for treatment of extremity lymphedema. Plast. Reconstr. Surg. Glob. Open. 2013, 132, 1305–1314. [Google Scholar] [CrossRef]
- Poumellec, M.A.; Foissac, R.; Cegarra-Escolano, M.; Barranger, E.; Ihrai, T. Surgical treatment of secondary lymphedema of the upper limb by stepped microsurgical lymphaticovenous anastomoses. Breast Cancer Res. Treat. 2017, 162, 219–224. [Google Scholar] [CrossRef]
- Chung, J.H.; Baek, S.O.; Park, H.J.; Lee, B.I.; Park, S.H.; Yoon, E.S. Efficacy and patient satisfaction regarding lymphovenous bypass with sleeve-in anastomosis for extremity lymphedema. Arch. Plast. Surg. 2019, 46, 46–56. [Google Scholar] [CrossRef] [Green Version]
- Mihara, M.; Hara, H.; Kikuchi, K.; Yamamoto, T.; Iida, T.; Narushima, M.; Araki, J.; Murai, N.; Mitsui, K.; Gennaro, P.; et al. Scarless lymphatic venous anastomosis for latent and early-stage lymphoedema using indocyanine green lymphography and non-invasive instruments for visualising subcutaneous vein. J. Plast. Reconstr. Aesthet. Surg. 2012, 65, 1551–1558. [Google Scholar] [CrossRef] [PubMed]
- Mihara, M.; Hara, H.; Tange, S.; Zhou, H.P.; Kawahara, M.; Shimizu, Y.; Murai, N. Multisite Lymphaticovenular Bypass Using Supermicrosurgery Technique for Lymphedema Management in Lower Lymphedema Cases. Plast. Reconstr. Surg. 2016, 138, 262–272. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.F.; Zhao, H.; Yamamoto, T.; Hara, H.; Ding, J. Indocyanine Green Lymphographic Evidence of Surgical Efficacy Following Microsurgical and Supermicrosurgical Lymphedema Reconstructions. J. Reconstr. Microsurg. 2016, 32, 688–698. [Google Scholar] [PubMed]
- Masia, J.; Pons, G.; Rodriguez-Bauza, E. Barcelona Lymphedema Algorithm for Surgical Treatment in Breast Cancer-Related Lymphedema. J. Reconstr. Microsurg. 2016, 32, 329–335. [Google Scholar]
- Winters, H.; Tielemans, H.J.P.; Hameeteman, M.; Paulus, V.A.A.; Beurskens, C.H.; Slater, N.J.; Ulrich, D.J.O. The efficacy of lymphaticovenular anastomosis in breast cancer-related lymphedema. Breast Cancer Res. Treat. 2017, 165, 321–327. [Google Scholar] [CrossRef] [Green Version]
- Winters, H.; Tielemans, H.J.P.; Verhulst, A.C.; Paulus, V.A.A.; Slater, N.J.; Ulrich, D.J.O. The Long-term Patency of Lymphaticovenular Anastomosis in Breast Cancer-Related Lymphedema. Ann. Plast. Surg. 2019, 82, 196–200. [Google Scholar] [CrossRef]
- Gentileschi, S.; Servillo, M.; Albanese, R.; De Bonis, F.; Tartaglione, G.; Salgarello, M. Lymphatic mapping of the upper limb with lymphedema before lymphatic supermicrosurgery by mirroring of the healthy limb. Microsurgery 2017, 37, 881–889. [Google Scholar] [CrossRef]
- Salgarello, M.; Mangialardi, M.L.; Pino, V.; Gentileschi, S.; Visconti, G. A Prospective Evaluation of Health-Related Quality of Life following Lymphaticovenular Anastomosis for Upper and Lower Extremities Lymphedema. J. Reconstr. Microsurg. 2018, 34, 701–707. [Google Scholar] [CrossRef]
- Cornelissen, A.J.M.; Kool, M.; Lopez Penha, T.R.; Keuter, X.H.A.; Piatkowski, A.A.; Heuts, E.; van der Hulst, R.; Qiu, S.S. Lymphatico-venous anastomosis as treatment for breast cancer-related lymphedema: A prospective study on quality of life. Breast Cancer Res. Treat. 2017, 163, 281–286. [Google Scholar] [CrossRef] [Green Version]
- Damstra, R.J.; Voesten, H.G.; van Schelven, W.D.; van der Lei, B. Lymphatic venous anastomosis (LVA) for treatment of secondary arm lymphedema. A prospective study of 11 LVA procedures in 10 patients with breast cancer related lymphedema and a critical review of the literature. Breast Cancer Res. Treat. 2009, 113, 199–206. [Google Scholar] [CrossRef]
- Gharb, B.B.; Rampazzo, A.; Spanio di Spilimbergo, S.; Xu, E.S.; Chung, K.P.; Chen, H.C. Vascularized lymph node transfer based on the hilar perforators improves the outcome in upper limb lymphedema. Ann. Plast. Surg. 2011, 67, 589–593. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, A.T.; Suami, H.; Hanasono, M.M.; Womack, V.A.; Wong, F.C.; Chang, E.I. Long-term outcomes of the minimally invasive free vascularized omental lymphatic flap for the treatment of lymphedema. J. Surg. Oncol. 2017, 115, 84–89. [Google Scholar] [CrossRef] [PubMed]
- Coriddi, M.; Wee, C.; Meyerson, J.; Eiferman, D.; Skoracki, R. Vascularized Jejunal Mesenteric Lymph Node Transfer: A Novel Surgical Treatment for Extremity Lymphedema. J. Am. Coll. Surg. 2017, 225, 650–657. [Google Scholar] [CrossRef] [PubMed]
- Dionyssiou, D.; Demiri, E.; Tsimponis, A.; Sarafis, A.; Mpalaris, V.; Tatsidou, G.; Arsos, G. A randomized control study of treating secondary stage II breast cancer-related lymphoedema with free lymph node transfer. Breast Cancer Res. Treat. 2016, 156, 73–79. [Google Scholar] [CrossRef]
- Ciudad, P.; Maruccia, M.; Socas, J.; Lee, M.H.; Chung, K.P.; Constantinescu, T.; Kiranantawat, K.; Nicoli, F.; Sapountzis, S.; Yeo, M.S.; et al. The laparoscopic right gastroepiploic lymph node flap transfer for upper and lower limb lymphedema: Technique and outcomes. Microsurgery 2017, 37, 197–205. [Google Scholar] [CrossRef]
- Patel, K.M.; Lin, C.Y.; Cheng, M.H. A Prospective Evaluation of Lymphedema-Specific Quality-of-Life Outcomes Following Vascularized Lymph Node Transfer. Ann. Surg. Oncol. 2015, 22, 2424–2430. [Google Scholar] [CrossRef]
- Asuncion, M.O.; Chu, S.Y.; Huang, Y.L.; Lin, C.Y.; Cheng, M.H. Accurate Prediction of Submental Lymph Nodes Using Magnetic Resonance Imaging for Lymphedema Surgery. Plast. Reconstr. Surg. Glob. Open. 2018, 6, e1691. [Google Scholar] [CrossRef]
- Ciudad, P.; Manrique, O.J.; Adabi, K.; Huang, T.C.; Agko, M.; Trignano, E.; Chang, W.L.; Chen, T.W.; Salgado, C.J.; Chen, H.C. Combined double vascularized lymph node transfers and modified radical reduction with preservation of perforators for advanced stages of lymphedema. J. Surg. Oncol. 2019, 119, 439–448. [Google Scholar] [CrossRef]
- Visconti, G.; Tartaglione, G.; Bartoletti, R.; Salgarello, M. Ompartimental harvesting of dual lymph node flap from the right supraclavicular area for the treatment of lower extremity lymphedema: A case series. J. Plast. Reconstr. Aesthet. Surg. 2019, 72, 211–215. [Google Scholar] [CrossRef]
- Maruccia, M.; Elia, R.; Ciudad, P.; Nacchiero, E.; Nicoli, F.; Vestita, M.; Chen, H.C.; Giudice, G. Postmastectomy upper limb lymphedema: Combined vascularized lymph node transfer and scar release with fat graft expedites surgical and patients’ related outcomes. A retrospective comparative study. J. Plast. Reconstr. Aesthet. Surg. 2019, 72, 892–901. [Google Scholar] [CrossRef]
- Gratzon, A.; Schultz, J.; Secrest, K.; Lee, K.; Feiner, J.; Klein, R.D. Clinical and Psychosocial Outcomes of Vascularized Lymph Node Transfer for the Treatment of Upper Extremity Lymphedema After Breast Cancer Therapy. Ann. Surg. Oncol. 2017, 24, 1475–1481. [Google Scholar] [CrossRef]
- Cheng, M.H.; Loh, C.Y.Y.; Lin, C.Y. Outcomes of Vascularized Lymph Node Transfer and Lymphovenous Anastomosis for Treatment of Primary Lymphedema. Plast. Reconstr. Surg. Glob. Open. 2018, 6, e2056. [Google Scholar] [CrossRef] [PubMed]
- De Brucker, B.; Zeltzer, A.; Seidenstuecker, K.; Hendrickx, B.; Adriaenssens, N.; Hamdi, M. Breast Cancer-Related Lymphedema: Quality of Life after Lymph Node Transfer. Plast. Reconstr. Surg. Glob. Open. 2016, 137, 1673–1680. [Google Scholar] [CrossRef] [PubMed]
- Inbal, A.; Teven, C.M.; Chang, D.W. Latissimus dorsi flap with vascularized lymph node transfer for lymphedema treatment: Technique, outcomes, indications and review of literature. J. Surg. Oncol. 2017, 115, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Wiser, I.M.B.; Coriddi, M.; Kenworthy, E.; Cavalli, M.; Encarnacion, E.; Dayan, J. Preoperative Assessment of Upper Extremity Secondary Lymphedema. Cancers 2020, 12, 135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Armer, J.M.B.K.; McCall, L.; Armer, N.C.; Sun, Y.; Udmuangpia, T.; Hunt, K.K.; Mittendorf, E.A.; Byrd, D.R.; Julian, T.B.; Boughey, J.C. Lymphedema symptoms and limb measurement changes in breast cancer survivors treated with neoadjuvant chemotherapy and axillary dissection: Results of American College of Surgeons Oncology Group (ACOSOG) Z1071 (Alliance) substudy. Support Care Cancer 2019, 27, 495–503. [Google Scholar] [CrossRef]
- Tsang, S.R.C.; Terkawi, A.S. Guidelines for developing, translating, and validating a questionnaire in perioperative and pain medicine. Saudi. J. Anaesth. 2017, 11, S80–S89. [Google Scholar] [CrossRef]
- Pusic, A.L.C.Y.; Albornoz, C.; Klassen, A.; Cano, S.; Sulimanoff, I.; Hernandez, M.; Massey, M.; Cordeiro, P.; Morrow, M.; Mehrara, B. Quality of life among breast cancer patients with lymphedema: A systematic review of patient-reported outcome instruments and outcomes. J. Cancer Surviv. 2013, 7, 83–92. [Google Scholar] [CrossRef] [Green Version]
- Mokkink, L.B.; Prinsen, C.; Patrick, D.L.; Alonso, J.; Bouter, L.M.; de Vet, H.C.; Terwee, G.B. COSMIN methodology for systematic reviews of Patient-Reported Outcome Measures (PROMs). User Man. 2018, 78, 1. [Google Scholar]



{kind=link}
{kind=link}
| Validated Tool | Lymphedema Specific | Categories | Number of Questions | Lookback Period | Upper/Lower Extremity | Score Calculation |
|---|---|---|---|---|---|---|
| LYMQOL | Yes | Four subscales: pain, mood, function and appearance, and an additional question on overall quality of life | 24 (upper) 25 (lower) | 1 week (mood only) | Both | A 4-point Likert scale with additional questions that are free response. Each dimension is scored, resulting in one number for each section. The overall quality of life score is on a 1-10 scale. |
| ULL27 | Yes | Three subscales: physical, psychological, and social | 27 | 4 weeks | Upper | A 5-point Likert scale. Each dimension is scored, resulting in one number for each section. |
| Lymph-ICF | Yes | Five subscales: physical function, mental function, household activities, mobility activities, and life and social activities | 29 | 2 weeks | Both | An 11-point Likert scale. Each dimension is scored, resulting in one number for each section. |
| LLIS | Yes | Three subscales: physical, psychosocial, functional, and an additional question on infection occurrence | 18 | 1 week | Both | A 5-point Likert scale. Each dimension is scored, resulting in one number for each section. |
| SF-36 | No | Eight subscales: physical functioning, role limitations as a result of physical problems, bodily pain, general health perception, vitality, social functioning, role limitations due to emotional problems, and mental health | 36 | 4 weeks | Both | The domains are combined to create a physical component score and a mental component score. |
| Study | Year Published | Number of Patients | Stage | Lymphedema Site | Primary vs. Secondary | Surgical Procedure | Baseline QOL Measure Administered Pre-Operatively? | Average Follow-Up Time | QOL Measure | Percent of Patients with Subjective Improvement |
|---|---|---|---|---|---|---|---|---|---|---|
| O’Brien | 1990 | 52 | Not mentioned | UE (46), LE (6) | Secondary | LVB | Not mentioned | 4.2 mo | Ad-hoc tool | 73% |
| Demirtas et al. | 2009 | 42 | Campisi stage II (12), III (17), IV (13) | LE | Secondary (34), Primary (8) | LVB | Not mentioned | 11.8 mo | Ad-hoc tool | 95% |
| Chang | 2010 | 20 | Capisi stage II (10), III (10) | UE (20) | Secondary | LVB | Yes | 12 mo | Ad-hoc tool | 80% |
| Auba et al. | 2012 | 10 | Campisi stage II (2), III (8) | LE (4), UE (6) | Secondary (9), Primary (1) | LVB | No | 18 mo | Ad-hoc tool | 90% |
| Mihara et al. | 2012 | 6 | ISL 0 (3), 1 (3) | LE | Secondary | LVB | Yes | 6 mo | Ad-hoc tool | 100% |
| Ayestaray et al. | 2013 | 20 | Campisi stage II (9), III (7), IV (3), V (1) | UE | Not mentioned | LVB | Yes | 6 mo | Ad-hoc tool | 95% |
| Chang et al. | 2013 | 100 | ICG classification stage 1 or 2 (16), 3 or 4 (14). Not all patients classified | UE (89), LE (11) | Secondary | LVB | Not mentioned | 30.4 mo (UE), 18.2 mo (LE) | Ad-hoc tool | 96% (UE), 57% (LE) |
| Mihara et al. | 2016 | 84 | ISL 1 (30), 2a (39), 2b (36), 3 (23) | LE | Primary (15), Secondary (69) | LVB | Yes | 18.3 mo | Ad-hoc tool | 80% |
| Chen et al. | 2016 | 21 | Campisi I and II (9), III (4), IV (8) | UE (13), LE (8) | Primary (4), Secondary (17) | LVB (18) or VLNT (3) | Yes | 12 mo | Ad-hoc tool | 100% |
| Masia et al. | 2016 | 200 | Not mentioned | UE (200) | Secondary (200) | LVB (81), VLNT (7), DIEP/SIEA with groin lymph nodes (16), LVB+VLNT (44), liposuction (52) | Yes | 12 mo | Ad-hoc tool | 96% |
| Poumellec et al. | 2017 | 31 | Campisi stage 2 (18), 3 (10), 4 (3) | UE | Secondary | LVB | Yes | 12.7 mo | Ad-hoc tool | 84% |
| Chung et al. | 2019 | 18 | Campisi stage II (7), III or IV (11) | UE (8), LE (10) | Secondary | LVB | No | 6 mo | Ad-hoc tool | Individual patient data not reported |
| Study | Year Published | Number of Patients | Stage | Lymphedema Site | Primary vs. Secondary | Surgical Procedure | Baseline QOL Measure Administered Pre-Operatively? | Average Follow-Up Time Regarding Subjective Assessment | QoL Measure | Percent of Patients with Subjective Improvement |
|---|---|---|---|---|---|---|---|---|---|---|
| Damstra et al. | 2009 | 10 | Campisi stage III (10) | UE | Secondary | LVB | Yes | 6 mo | SF-36 | 50% |
| Cornelissen et al. | 2017 | 20 | ISL 1 (1), 2a (19) | UE | Secondary | LVB | Yes | 12 mo | Lymph-ICF | Individual patient data not reported |
| Gentileschi et al. | 2017 | 16 | ISL 2a (7), 2b (9) | UE | Secondary | LVB | Yes | 6 mo | LYMQOL | Individual patient data not reported |
| Winters et al. | 2017 | 29 | Campisi stages 1b–2a | UE | Secondary | LVB | Yes | 12 mo | LYMQOL | Individual patient data not reported |
| Salgarello et al. | 2018 | 74 | Not mentioned | UE (44), LE (26) | Primary (5), Secondary (55) | LVB | Yes | 8.5 mo | LYMQOL | Individual patient data not reported |
| Winters et al. | 2019 | 12 | Campisi stages 1–2a | UE | Secondary | LVB | Yes | 6 mo | LYMQOL | Individual patient data not reported |
| Study | Year Published | Number of Patients | Stage | Lymphedema Site | Primary vs. Secondary | Surgical Procedure | Donor Site (Lymph Node Transplant) | Baseline QOL Measure Administered Pre-Operatively? | Average Follow-Up Time Regarding Subjective Assessment | QOL Measure | Percent of Patients with Subjective Improvement |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Gharb et al. | 2011 | 21 | Not mentioned | UE | Secondary | VLNT (10 also liposuction) | Groin | Yes | 43.1 mo | Ad-hoc tool | Individual patient data not reported |
| Dionyssiou et al. | 2016 | 18 | ISL stage II (18) | UE | Secondary | VLNT | Groin | Yes | 12 mo | Ad-hoc tool | 100% |
| Coriddi et al. | 2017 | 15 | Not mentioned | UE (8), LE (7) | Secondary | VLNT | Jejunal Mesentery | Not mentioned | 9.1 mo | Ad-hoc tool | 86% |
| Nguyen et al. | 2017 | 42 | Modified ICG stage 3 (9), 4 (18), 5 (15) | UE (19), LE (24) | Secondary (37), Primary (2), not mentioned (3) | VLNT (55% also having LVA) | Omentum | Not mentioned | 14 mo | Ad-hoc tool | 83% |
| Study | Year Published | Number of Patients | Stage | Lymphedema Site | Primary vs. Secondary | Surgical Procedure | Donor Site (Lymph Node Transplant) | Baseline QOL Measure Administered Pre-Operatively? | Average Follow-Up Time Regarding Subjective Assessment | QoL Measure | Percent of Patients with Subjective Improvement |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Patel et al. | 2015 | 25 | Scale specific to this paper, I (1), II (6), III (13), IV (5) | UE (15), LE (10) | Secondary (23), Primary (2) | VLNT | Groin or submental | Yes | 12 mo | LYMQOL | Individual patient data not reported |
| De Brucker et al. | 2016 | 25 | Stage 1 and 2 (classification system and number of patients per stage not mentioned) | UE | Secondary | VLNT | Groin | No | 29 mo | ULL27 | 84% |
| Ciudad et al. | 2017 | 10 | ISL stage II (2), ISL stage III (8) | UE (5), LE (5) | Secondary | VLNT | Right gastroepiploic lymph node flap | Yes | 14.7 mo | LYMQOL | Individual patient data not reported |
| Gratzon et al. | 2017 | 24 | Not mentioned | UE | Secondary | VLNT | Groin, lateral thoracic, supraclavicular | Yes | 12 mo | LYMQOL and study specific pain scale and heaviness scale with standard 1-10 rating | Individual patient data not reported |
| Inbal et al. | 2017 | 11 | ISL stage 1 (4), 2 (7) | UE (8), LE (3) | Secondary | VLNT (64% also having LVB) | Thoracic on muscle sparing latissimus dorsi flap | Yes | 6.7 mo | LLIS | 91% |
| Cheng et al. | 2018 | 19 | Not mentioned | LE (19) | Primary (19) | VLNT (15), LVB (4) | Submental | Yes | 12 mo | LYMQOL | Individual patient data not reported |
| Asuncion et al. | 2018 | 15 | Not mentioned | LE (10), UE (4), both LE/UE (1) | Not mentioned | VLNT | Submental | Yes | 12 mo | LYMQOL | Individual pre-operative patient data not reported |
| Ciudad et al. | 2019 | 16 | ISL stage III (16) | UE (6), LE (10) | Secondary (15), Primary (1) | VLNT (with debulking) | Gastroepiploic | Yes | 12 mo | LYMQOL | Individual patient data not reported |
| Maruccia et al. | 2019 | 39 | Not mentioned | UE | Secondary | VLNT (18 also with axillary scar release and fat grafting) | Groin (20), Gastroepiploic (19) | Yes | 12 mo | LYMQOL | Individual patient data not reported |
| Visconti et al. | 2019 | 10 | ISL 2b (10) | LE | Secondary | VLNT | Supraclavicular | Yes | 12 mo | LYMQOL | 100% |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Coriddi, M.; Dayan, J.; Sobti, N.; Nash, D.; Goldberg, J.; Klassen, A.; Pusic, A.; Mehrara, B. Systematic Review of Patient-Reported Outcomes following Surgical Treatment of Lymphedema. Cancers 2020, 12, 565. https://doi.org/10.3390/cancers12030565
Coriddi M, Dayan J, Sobti N, Nash D, Goldberg J, Klassen A, Pusic A, Mehrara B. Systematic Review of Patient-Reported Outcomes following Surgical Treatment of Lymphedema. Cancers. 2020; 12(3):565. https://doi.org/10.3390/cancers12030565
Chicago/Turabian StyleCoriddi, Michelle, Joseph Dayan, Nikhil Sobti, David Nash, Johanna Goldberg, Anne Klassen, Andrea Pusic, and Babak Mehrara. 2020. "Systematic Review of Patient-Reported Outcomes following Surgical Treatment of Lymphedema" Cancers 12, no. 3: 565. https://doi.org/10.3390/cancers12030565
APA StyleCoriddi, M., Dayan, J., Sobti, N., Nash, D., Goldberg, J., Klassen, A., Pusic, A., & Mehrara, B. (2020). Systematic Review of Patient-Reported Outcomes following Surgical Treatment of Lymphedema. Cancers, 12(3), 565. https://doi.org/10.3390/cancers12030565