Role of Microtubule-Associated Protein 1b in Urothelial Carcinoma: Overexpression Predicts Poor Prognosis



Abstract
:1. Introduction
2. Results
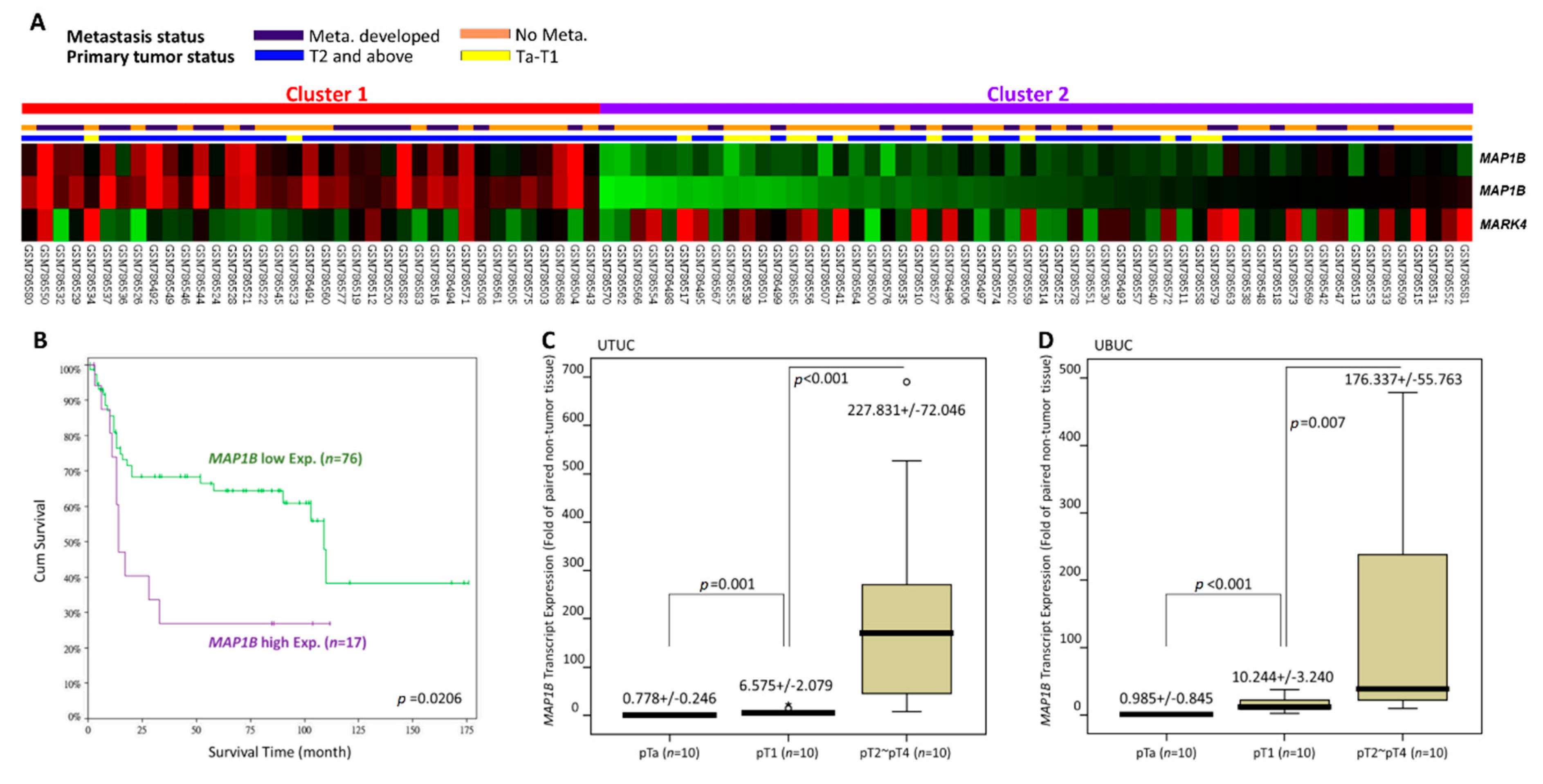
2.1. MAP1B Is the Most Significantly Upregulated Gene Associated with Microtubule Bundle Formation in UBUC Transcriptomes
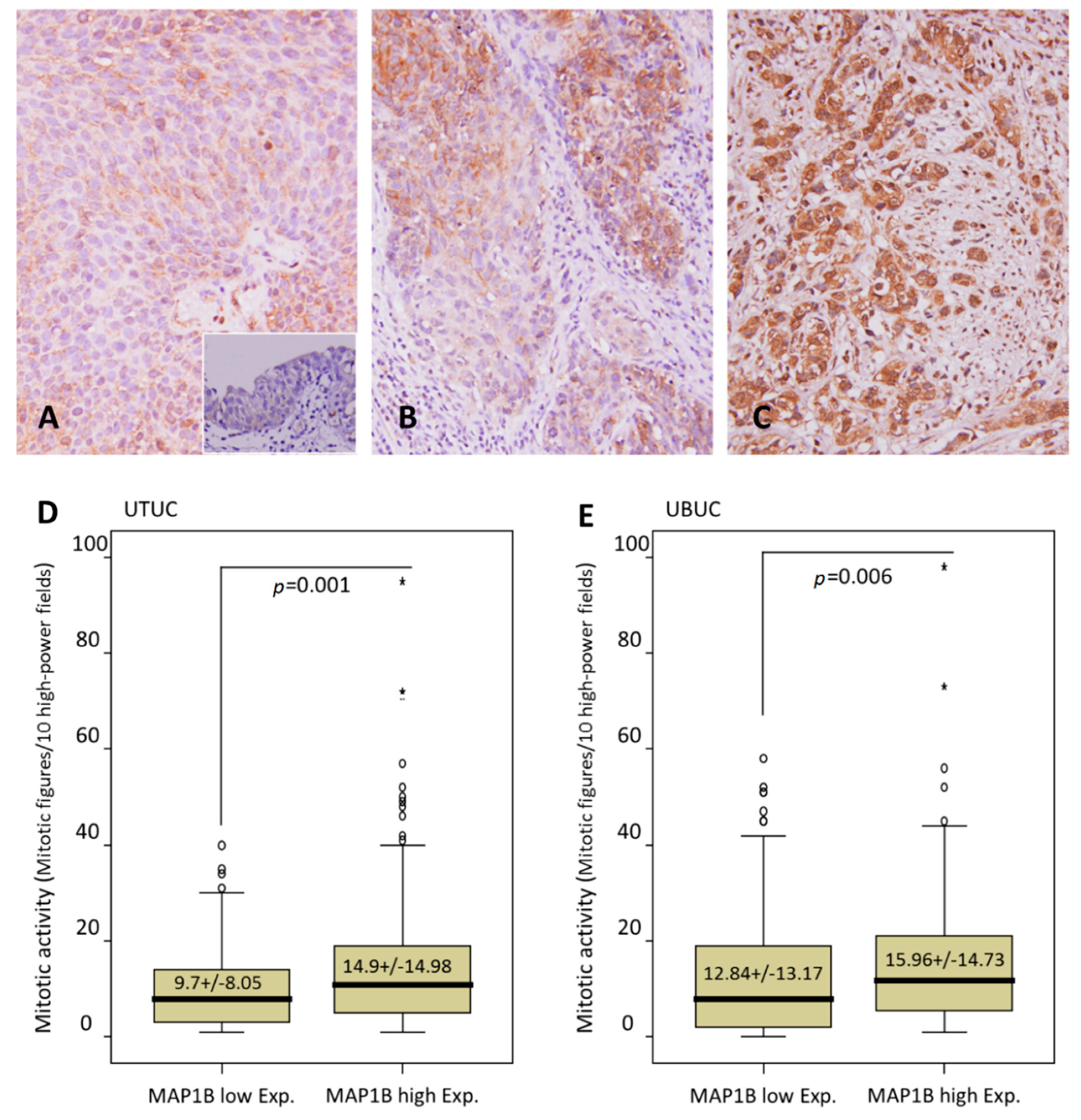
2.2. MAP1B Immunoexpression and Clinicopathological and Genomic Correlations in UTUC and UBUC
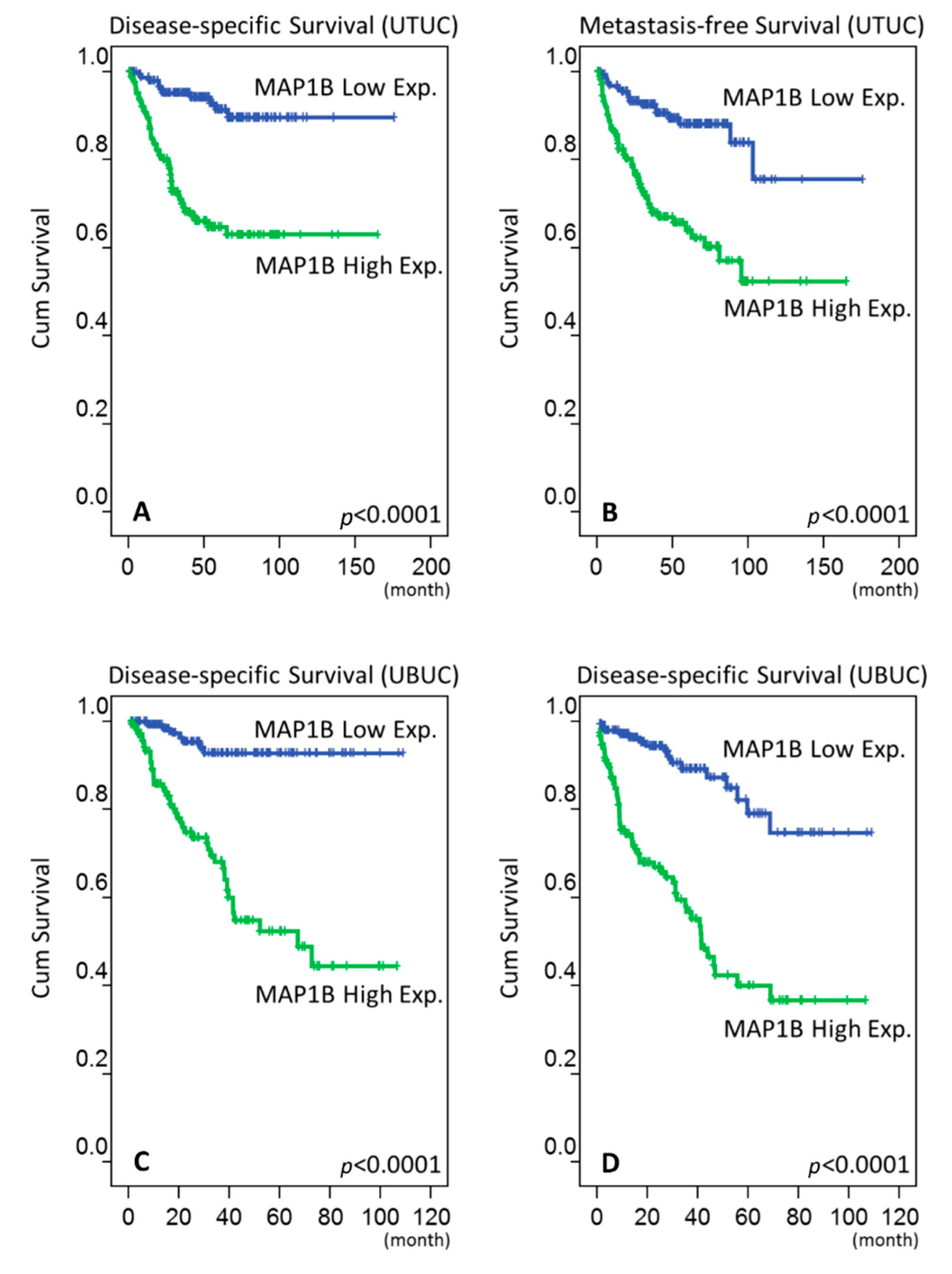
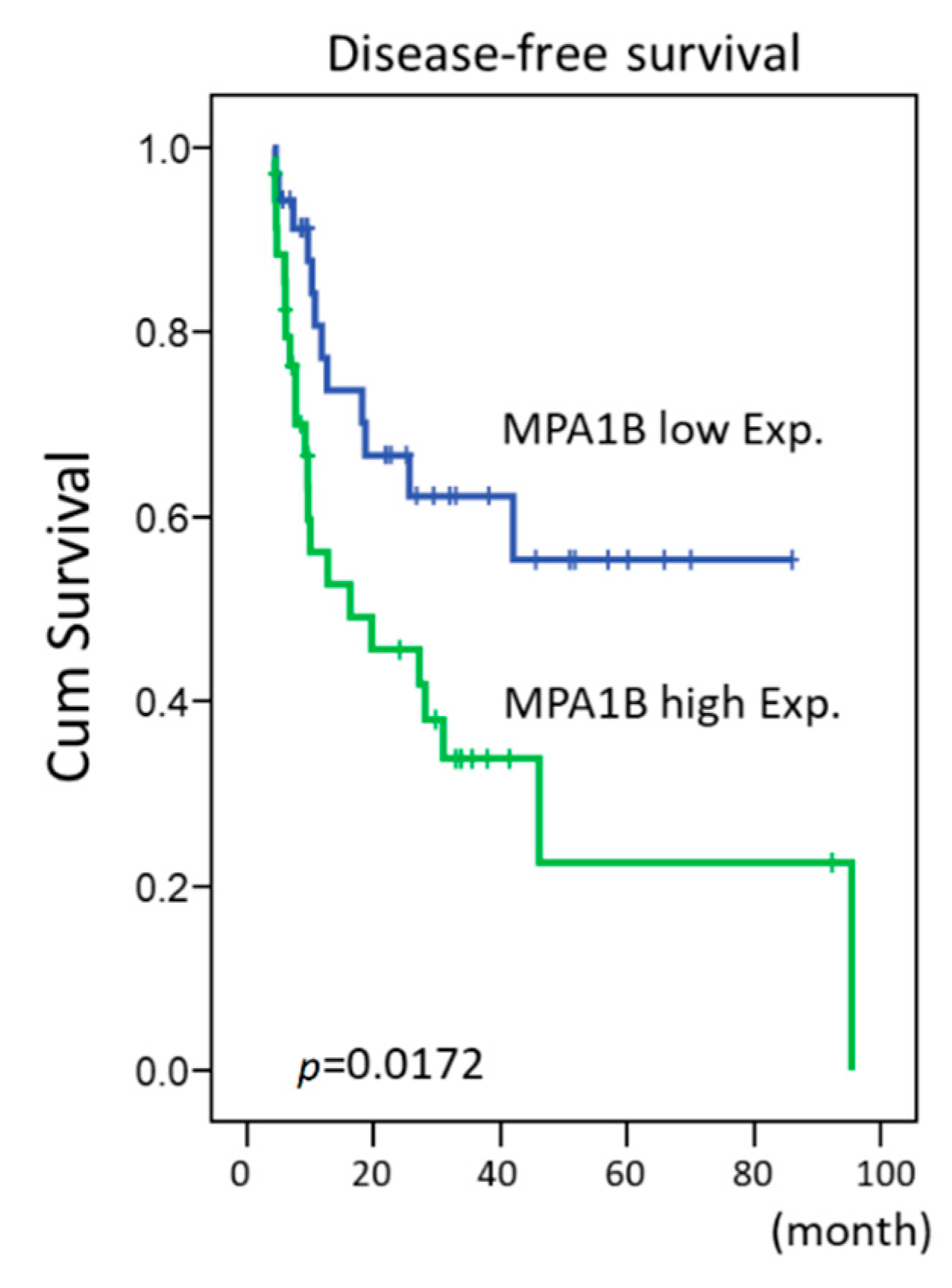
2.3. Survival Analysis in UTUC and UBUC
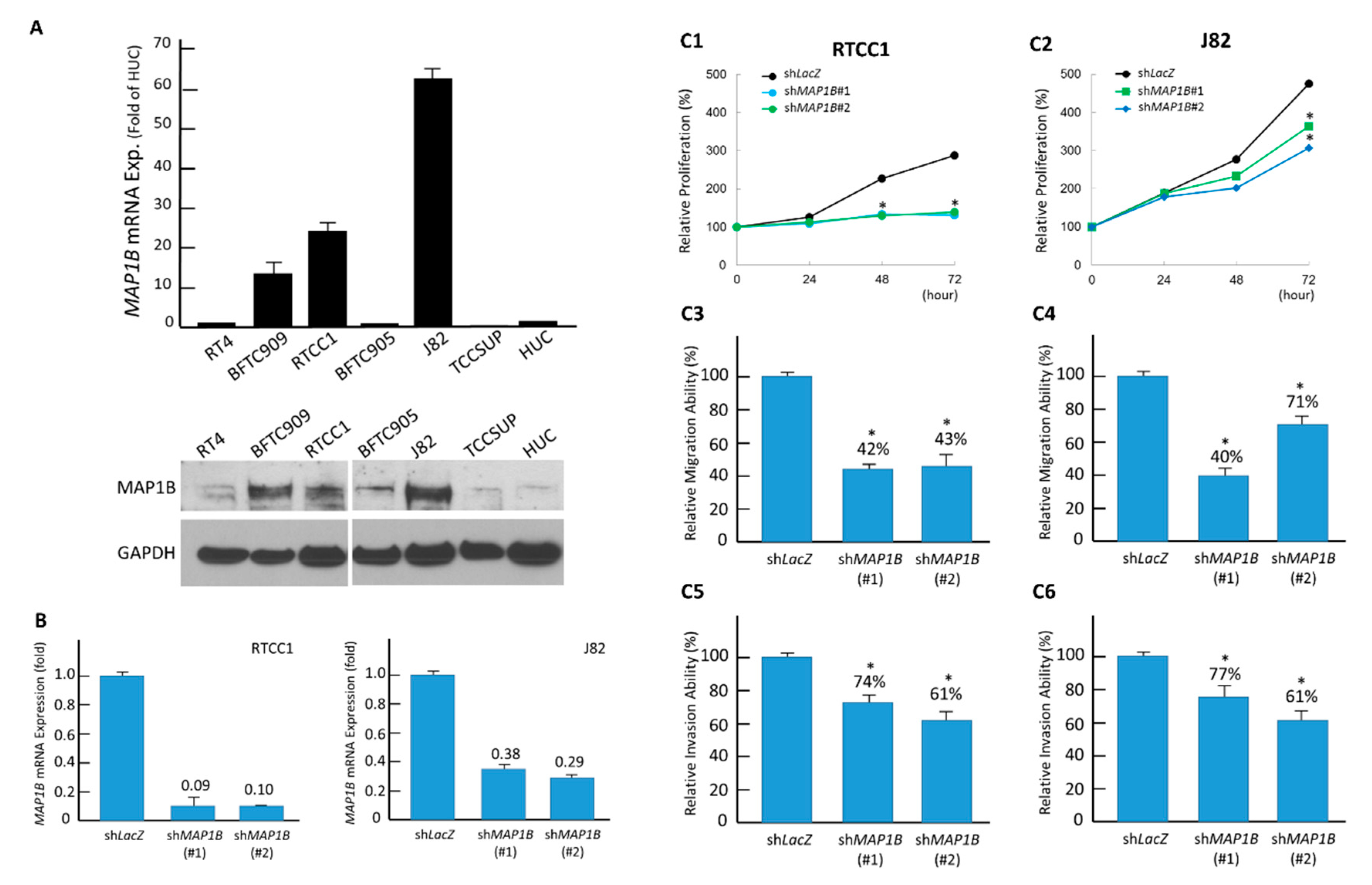
2.4. MAP1B Promotes the Cell Proliferation, Migration, and Invasion of UC Cell Lines
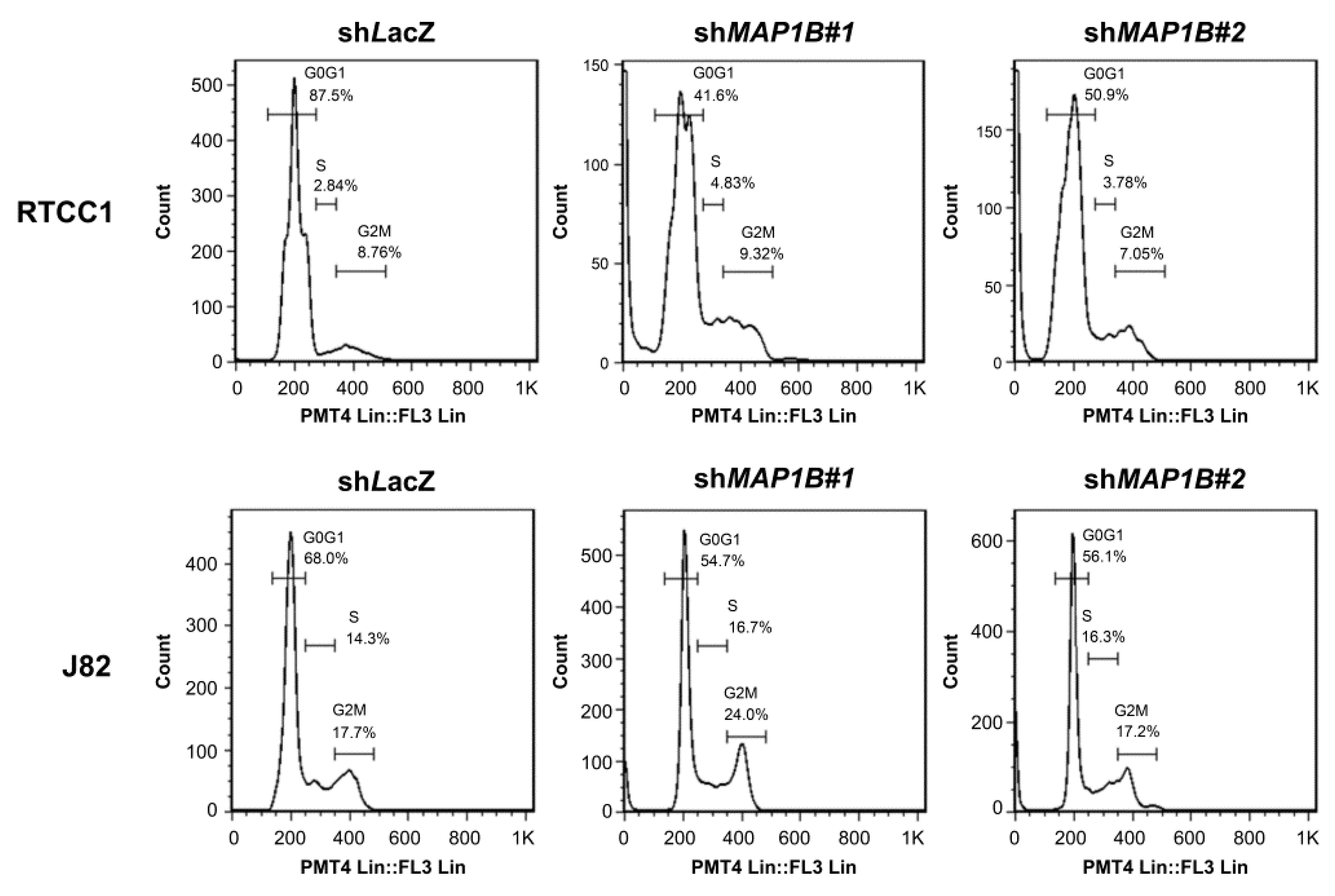
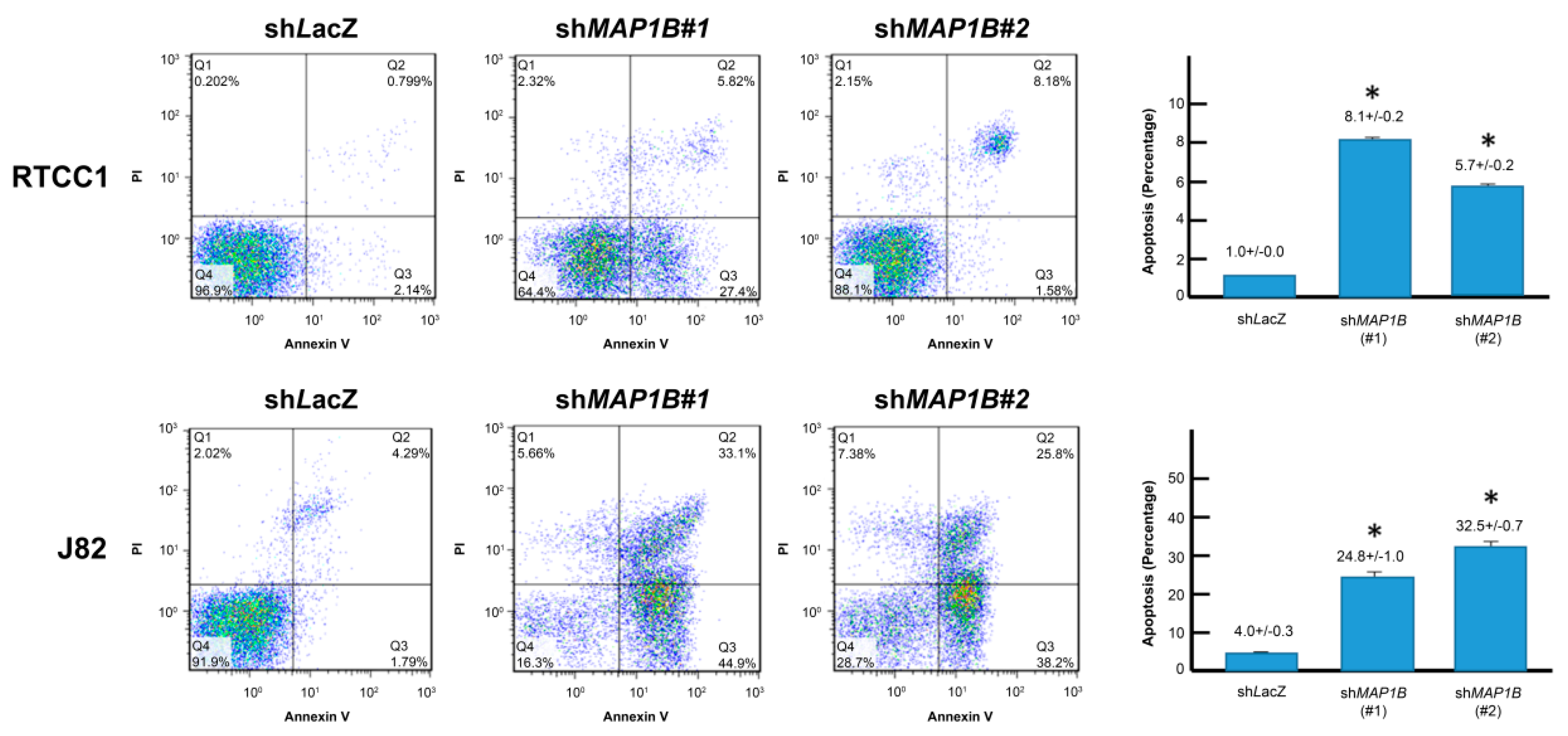
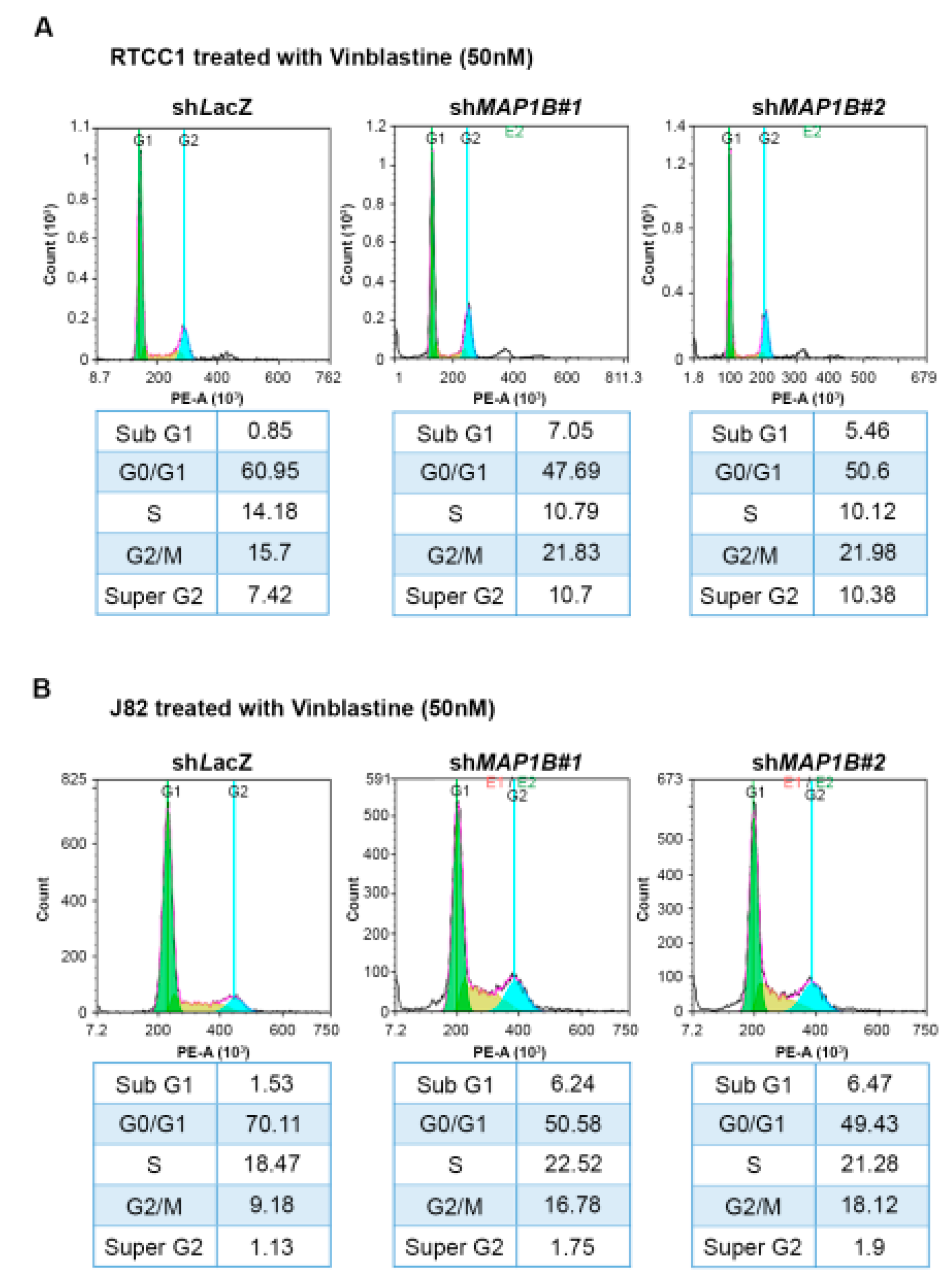
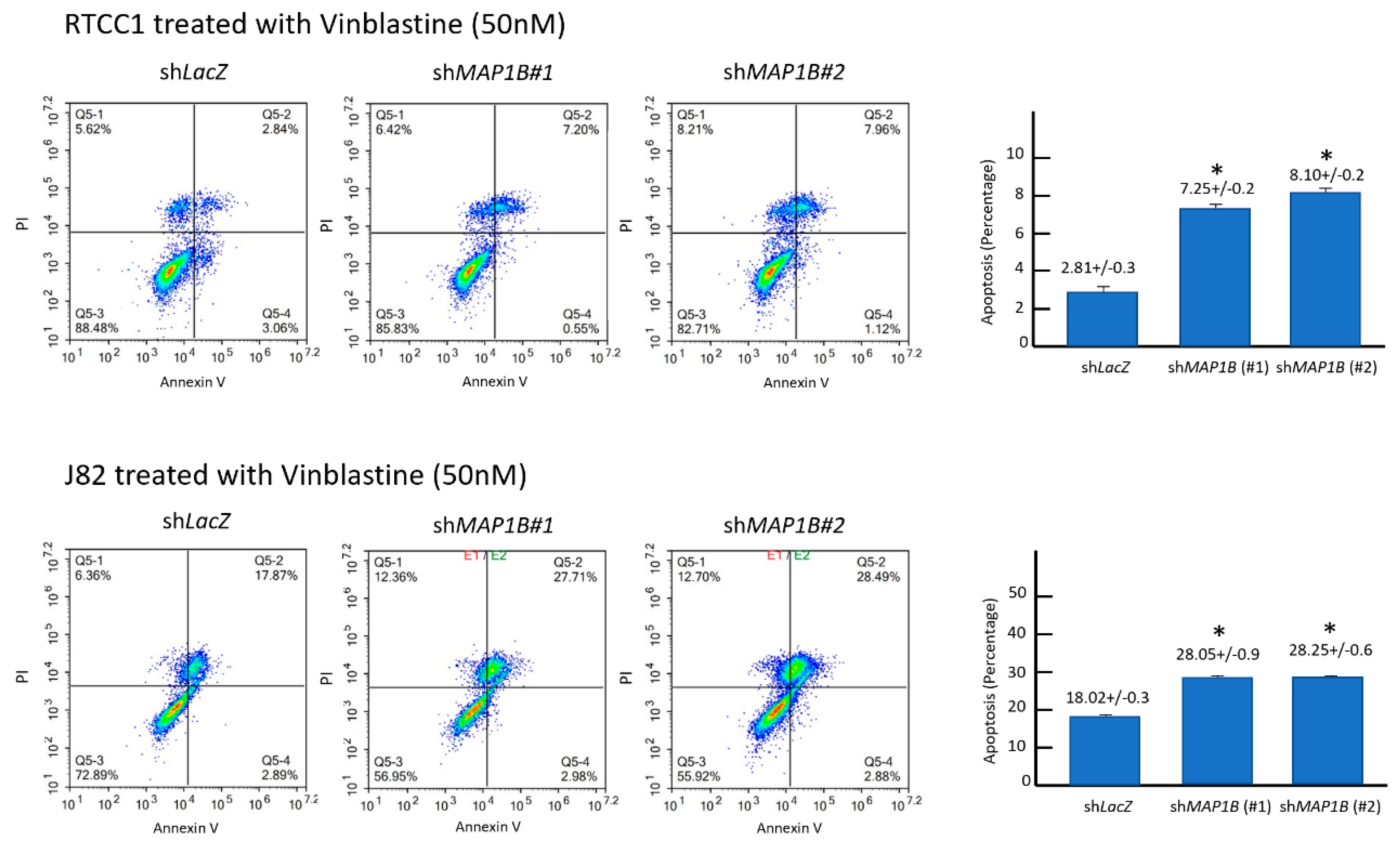
2.5. MAP1B Expression Correlates with Chemoresistance In Vitro and In Vivo
3. Discussion
4. Materials and Methods
4.1. Data Mining of GSE31684 to Identify Altered Gene Expression in UC
4.2. Patients and Tumor Specimens
4.3. Immunohistochemical Staining
4.4. Real-Time Reverse-Transcription Polymerase Chain Reaction (RT-PCR) to Assess the Transcription Levels of MAP1B in Cell Lines and UC Samples
4.5. Cell Culture
4.6. RNA Interference
4.7. Western Blotting
4.8. Bromodeoxyuridine (BrdU) Assay to Assess DNA Synthesis
4.9. Pharmacological Assays
4.10. Migration and Invasion Assays
4.11. Flow Cytometry Analysis of Cell-Cycle Kinetics
4.12. Flow Cytometry Analysis of Apoptosis
4.13. Mutation Analysis
4.14. Postoperative Adjuvant Chemotherapy in UBUC
4.15. Statistical Analyses
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Torre, L.A.; Bray, F.; Siegel, R.L.; Ferlay, J.; Lortet-Tieulent, J.; Jemal, A. Global cancer statistics, 2012. CA Cancer J. Clin. 2015, 65, 87–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lynch, C.F.; Davila, J.A.; Platz, C.E. Cancer of the urinary bladder. In SEER Survival Monograph: Cancer Survival Among Adults: US SEER Program, 1988–2001, Patient and Tumor Characteristics, National; Ries, Y.J., Keel, G.E., Eisner, M.P., Eds.; Cancer Institute, SEER Program: Bethesda, MD, USA, 2007; pp. 193–202. [Google Scholar]
- Margulis, V.; Shariat, S.F.; Matin, S.F.; Kamat, A.M.; Zigeuner, R.; Kikuchi, E.; Lotan, Y.; Weizer, A.; Raman, J.D.; Wood, C.G. Outcomes of radical nephroureterectomy: A series from the Upper Tract Urothelial Carcinoma Collaboration. Cancer 2009, 115, 1224–1233. [Google Scholar] [CrossRef] [PubMed]
- Lai, M.N.; Wang, S.M.; Chen, P.C.; Chen, Y.Y.; Wang, J.D. Population-based case-control study of Chinese herbal products containing aristolochic acid and urinary tract cancer risk. J. Natl. Cancer Inst. 2010, 102, 179–186. [Google Scholar] [CrossRef] [Green Version]
- Li, C.C.; Chang, T.H.; Wu, W.J.; Ke, H.L.; Huang, S.P.; Tsai, P.C.; Chang, S.J.; Shen, J.T.; Chou, Y.H.; Huang, C.H. Significant predictive factors for prognosis of primary upper urinary tract cancer after radical nephroureterectomy in Taiwanese patients. Eur. Urol. 2008, 54, 1127–1134. [Google Scholar] [CrossRef] [PubMed]
- Ploussard, G.; Xylinas, E.; Lotan, Y.; Novara, G.; Margulis, V.; Rouprêt, M.; Matsumoto, K.; Karakiewicz, P.I.; Montorsi, F.; Remzi, M.; et al. Conditional survival after radical nephroureterectomy for upper tract carcinoma. Eur. Urol. 2015, 67, 803–812. [Google Scholar] [CrossRef] [PubMed]
- Raman, J.D.; Scherr, D.S. Management of patients with upper urinary tract transitional cell carcinoma. Nat. Clin. Pract. Urol. 2007, 4, 432–443. [Google Scholar] [CrossRef] [PubMed]
- Knowles, M.A. What we could do now: Molecular pathology of bladder cancer. Mol. Pathol. 2001, 54, 215–221. [Google Scholar] [CrossRef] [PubMed]
- McConkey, D.J.; Lee, S.; Choi, W.; Tran, M.; Majewski, T.; Lee, S.; Siefker-Radtke, A.; Dinney, C.; Czerniak, B. Molecular genetics of bladder cancer: Emerging mechanisms of tumor initiation and progression. Urol. Oncol. 2010, 28, 429–440. [Google Scholar] [CrossRef] [Green Version]
- Amin, M.B. Histological variants of urothelial carcinoma: Diagnostic, therapeutic and prognostic implications. Mod. Pathol. 2009, 22 (Suppl. 2), S96–S118. [Google Scholar] [CrossRef]
- Zhang, Z.; Furge, K.A.; Yang, X.J.; Teh, B.T.; Hansel, D.E. Comparative gene expression profiling analysis of urothelial carcinoma of the renal pelvis and bladder. BMC Med. Genom. 2010, 3, 58. [Google Scholar] [CrossRef] [Green Version]
- Halpain, S.; Dehmelt, L. The MAP1 family of microtubule-associated proteins. Genome Biol. 2006, 76, 224. [Google Scholar] [CrossRef] [PubMed]
- Dehmelt, L.; Halpain, S. The MAP2/Tau family of microtubule-associated proteins. Genome Biol. 2005, 6, 204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhat, K.M.; Setaluri, V. Microtubule-associated proteins as targets in cancer chemotherapy. Clin. Cancer Res. 2007, 13, 2849–2854. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parker, A.L.; Kavallaris, M.; McCarroll, J.A. Microtubules and their role in cellular stress in cancer. Front. Oncol. 2014, 4, 153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niegisch, G.; Lorch, A.; Droller, M.J.; Lavery, H.J.; Stensland, K.D.; Albers, P. Neoadjuvant chemotherapy in patients with muscle-invasive bladder cancer: Which patients benefit? Eur. Urol. 2013, 64, 355–357. [Google Scholar] [CrossRef] [PubMed]
- Adibi, M.; Youssef, R.; Shariat, S.F.; Lotan, Y.; Wood, C.G.; Sagalowsky, A.I.; Zigeuner, R.; Montorsi, F.; Bolenz, C.; Margulis, V. Oncological outcomes after radical nephroureterectomy for upper tract urothelial carcinoma: Comparison over the three decades. Int. J. Urol. 2012, 19, 1060–1066. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Altmann, K.H. Preclinical Pharmacology and Structure-Activity Studies of Epothilones. In The Epothilones: An Outstanding Family of Anti-Tumor Agents. Fortschritte der Chemie Organischer Naturstoffe/Progress in the Chemistry of Organic Natural Products; Springer: Vienna, Austria, 2009; Volume 90. [Google Scholar] [CrossRef]
- Villarroel-Campos, D.; Gonzalez-Billault, C. The MAP1B case: An old MAP that is new again. Dev. Neurobiol. 2014, 74, 953–971. [Google Scholar] [CrossRef]
- Wang, Z.; Zhang, Y.; Zhang, S.; Guo, Q.; Tan, Y.; Wang, X.; Xiong, R.; Ding, J.; Chen, S. DJ-1 can inhibit microtubule associated protein 1 B formed aggregates. Mol. Neurodegener. 2011, 6, 38. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.Y.; Kim, J.W.; Jeong, M.H.; An, J.H.; Jang, S.M.; Song, K.H.; Choi, K.H. Microtubule-associated protein 1B light chain (MAP1B-LC1) negatively regulates the activity of tumor suppressor p53 in neuroblastoma cells. FEBS Lett. 2008, 582, 2826–2832. [Google Scholar] [CrossRef] [Green Version]
- Byrne, F.L.; Yang, L.; Phillips, P.A.; Hansford, L.M.; Fletcher, J.I.; Ormandy, C.J.; McCarroll, J.A.; Kavallaris, M. RNAi-mediated stathmin suppression reduces lung metastasis in an orthotopic neuroblastoma mouse model. Oncogene 2014, 33, 882–890. [Google Scholar] [CrossRef]
- Dallol, A.; Agathanggelou, A.; Fenton, S.L.; Ahmed-Choudhury, J.; Hesson, L.; Vos, M.D.; Clark, G.J.; Downward, J.; Maher, E.R.; Latif, F. RASSF1A interacts with microtubule-associated proteins and modulates microtubule dynamics. Cancer Res. 2004, 64, 4112–4116. [Google Scholar] [CrossRef] [Green Version]
- Liu, L.; Vo, A.; Liu, G.; McKeehan, W.L. Distinct Structural Domains within C19ORF5 Support Association with Stabilized Microtubules and Mitochondrial Aggregation and Genome Destruction. Cancer Res. 2005, 65, 4191–4201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laes, J.F.; Quan, X.; Ravoet, M.; Stieber, D.; Van Vooren, P.; Van Reeth, T.; Szpirer, J.; Szpirer, C. Analysis of candidate genes included in the mammary cancer susceptibility 1 (Mcs1) region. Mamm. Genome 2001, 12, 199–206. [Google Scholar] [CrossRef] [PubMed]
- Gödel, M.; Temerinac, D.; Grahammer, F.; Hartleben, B.; Kretz, O.; Riederer, B.M.; Propst, F.; Kohl, S.; Huber, T.B. Microtubule associated protein 1b (MAP1B) is a marker of the microtubular cytoskeleton in podocytes but is not essential for the function of the kidney filtration barrier in mice. PLoS ONE 2015, 10, e0140116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fan, E.W.; Li, C.C.; Wu, W.J.; Huang, C.N.; Li, W.M.; Ke, H.L.; Yeh, H.C.; Wu, T.F.; Liang, P.I.; Ma, L.J.; et al. FGF7 Over expression is an independent prognosticator in patients with urothelial carcinoma of the upper urinary tract and bladder. J. Urol. 2015, 194, 223–229. [Google Scholar] [CrossRef] [PubMed]
- Chiang, L.C.; Chiang, W.; Chang, L.L.; Wu, W.J.; Huang, C.H. Characterization of a new human transitional cell carcinoma cell line from the renal pelvis, RTCC-1/KMC. Kaohsiung J. Med. Sci. 1996, 12, 448–452. [Google Scholar] [PubMed]
- Li, C.F.; Chen, L.T.; Lan, J.; Chou, F.F.; Lin, C.Y.; Chen, Y.Y.; Chen, T.J.; Li, S.H.; Yu, S.; Fang, F.M.; et al. AMACR amplification and overexpression in primary imatinib-naïve gastrointestinal stromal tumors: A driver of cell proliferation indicating adverse prognosis. Oncotarget 2014, 5, 11588–11630. [Google Scholar] [CrossRef] [Green Version]
- Li, C.F.; Fang, F.M.; Chen, Y.Y.; Chen, Y.Y.; Liu, T.T.; Chan, T.C.; Yu, S.C.; Chen, L.T.; Huang, H.Y. Overexpressed fatty acid synthase in gastrointestinal stromal tumors: Targeting a progression-associated metabolic driver enhances the antitumor effect of imatinib. Clin. Cancer Res. 2017, 23, 4908–4918. [Google Scholar] [CrossRef] [Green Version]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Probe Title 1 | Comparing T2-4 to Ta-T1 | Comparing Meta. to Non-Meta. # | Gene Symbol | Gene Title | Biological Process | Molecular Function | ||
|---|---|---|---|---|---|---|---|---|
| Log ratio | p-Value | Log ratio | p-Value | |||||
| 214577_at | 0.3773 | 0.0029 | 0.3943 | <0.0001 | MAP1B | Microtubule-associated protein 1B | Dendrite development, microtubule bundle formation | Protein binding, structural molecule activity |
| 221560_at | −0.3436 | 0.0058 | −0.0115 | 0.9048 | MARK4 | MAP/microtubule affinity-regulating kinase 4 | G1/S transition of mitotic cell cycle, G2/M transition of mitotic cell cycle, Wnt receptor signaling pathway, microtubule bundle formation, microtubule cytoskeleton organization and biogenesis, nervous system development, positive regulation of cell proliferation, positive regulation of programmed cell death, protein amino acid phosphorylation | ATP binding, gamma-tubulin binding, kinase activity, microtubule-binding, nucleotide-binding, protein-binding, protein kinase activity, protein serine/threonine kinase activity, protein-tyrosine kinase activity, tau-protein kinase activity, transferase activity, ubiquitin-binding |
| 226084_at | 1.2832 | <0.0001 | 0.9436 | <0.0001 | MAP1B | Microtubule-associated protein 1B | Dendrite development, microtubule bundle formation | Protein-binding, structural molecule activity |
| Parameter | Category | Upper Urinary Tract Urothelial Carcinoma | Urinary Bladder Urothelial Carcinoma | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Case no. | MAP1B Expression | p-value | Case no. | MAP1B Expression | p-value | ||||
| Low | High | Low | High | ||||||
| Gender & | Male | 158 | 79 | 79 | 1.000 | 216 | 103 | 113 | 0.223 |
| Female | 182 | 91 | 91 | 79 | 44 | 35 | |||
| Age (years) # | 340 | 65.2+/−9.87 | 65.9+/−9.92 | 0.409 | 295 | 65.76+/−12.02 | 66.33+/−12.44 | 0.759 | |
| Tumor location | Renal pelvis | 141 | 64 | 77 | 0.023 * | - | - | - | - |
| Ureter | 150 | 87 | 63 | - | - | - | - | ||
| Renal pelvis & ureter | 49 | 19 | 30 | - | - | - | - | ||
| Multifocality& | Single | 278 | 144 | 134 | 0.160 | - | - | - | - |
| Multifocal | 62 | 26 | 36 | - | - | - | - | ||
| Primary tumor (T) & | Ta | 89 | 54 | 35 | 0.005 * | 84 | 56 | 28 | <0.001 * |
| T1 | 92 | 5` | 41 | 88 | 45 | 43 | |||
| T2 | 159 | 65 | 94 | 123 | 46 | 77 | |||
| Nodal metastasis & | Negative (N0) | 312 | 164 | 148 | 0.002 * | 266 | 139 | 127 | 0.012 * |
| Positive (N1–N2) | 28 | 6 | 22 | 29 | 8 | 21 | |||
| Histological grade & | Low grade | 56 | 34 | 22 | 0.079 | 56 | 36 | 20 | 0.016 * |
| High grade | 284 | 136 | 148 | 239 | 111 | 128 | |||
| Vascular invasion & | Absent | 234 | 132 | 102 | <0.001 * | 246 | 129 | 117 | 0.045 * |
| Present | 106 | 38 | 68 | 49 | 18 | 31 | |||
| Perineural invasion & | Absent | 321 | 162 | 159 | 0.479 | 275 | 140 | 135 | 0.169 |
| Present | 19 | 8 | 11 | 20 | 7 | 13 | |||
| Parameter | Category | Case No. | Disease-Specific Survival | Metastasis-Free Survival | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Univariate Analysis | Multivariate Analysis | Univariate Analysis | Multivariate Analysis | |||||||||
| No. of Event | p-value | R.R. | 95% C.I. | p-value | No. of Event | p-value | R.R. | 95% C.I. | p-value | |||
| Gender | Male | 158 | 28 | 0.8730 | - | - | - | 32 | 0.8307 | - | - | - |
| Female | 182 | 33 | - | - | - | 38 | - | - | - | |||
| Age (years) | <65 | 138 | 26 | 0.9728 | - | - | - | 30 | 0.8667 | - | - | - |
| ≥65 | 202 | 35 | - | - | - | 40 | - | - | - | |||
| Tumor side | Right | 177 | 34 | 0.7188 | - | - | - | 38 | 0.3903 | - | - | - |
| Left | 154 | 26 | - | - | - | 32 | - | - | - | |||
| Bilateral | 9 | 1 | - | - | - | 0 | - | - | - | |||
| Tumor location | Renal pelvis | 141 | 24 | 0.0100 * | 1 | - | 0.562 | 31 | 0.0752 | - | - | - |
| Ureter | 150 | 22 | 1.167 | 0.618–2.203 | 25 | - | - | - | ||||
| Renal pelvis & ureter | 49 | 15 | 1.261 | 0.345–4.615 | 14 | - | - | |||||
| Multifocality | Single | 273 | 48 | 0.0031 * | 1 | - | 0.050 * | 52 | 0.0144 * | 1 | - | 0.001 * |
| Multifocal | 62 | 18 | 2.238 | 0.998–5.017 | 18 | 2.648 | 1.496–4.687 | |||||
| Primary tumor (T) | Ta | 89 | 2 | <0.0001 * | 1 | - | 0.008 * | 4 | <0.0001 * | 1 | - | 0.036 * |
| T1 | 92 | 9 | 2.641 | 0.561–12.419 | 15 | 2.643 | 0.563–12.410 | |||||
| T2–T4 | 159 | 50 | 5.667 | 1.250–25.699 | 51 | 5.538 | 1.236–24.817 | |||||
| Nodal metastasis | Negative (N0) | 312 | 42 | <0.0001 * | 1 | - | <0.001 * | 55 | <0.0001 * | 1 | - | <0.001 * |
| Positive (N1–N2) | 28 | 19 | 4.188 | 2.244–7.819 | 15 | 4.421 | 2.415–8.094 | |||||
| Histological grade | Low | 56 | 4 | 0.0177 * | 1 | - | 0.008 * | 3 | 0.0022 * | 1 | - | 0.008 * |
| High | 284 | 57 | 4.746 | 1.514–14.881 | 67 | 4.770 | 1.509–15.077 | |||||
| Vascular invasion | Absent | 234 | 24 | <0.0001 * | 1 | - | 0.139 | 26 | <0.0001 * | 1 | - | 0.147 |
| Present | 106 | 37 | 1.571 | 0.863–2.859 | 44 | 1.565 | 0.855–2.868 | |||||
| Perineural invasion | Absent | 321 | 50 | <0.0001 * | 1 | - | <0.001 * | 61 | <0.0001 * | 1 | - | <0.001 * |
| Present | 19 | 11 | 4.768 | 2.251–10.102 | - | 9 | 4.865 | 2.294–10.318 | ||||
| Mitotic rate (per 10 high power fields) | <10 | 173 | 27 | 0.1442 | - | - | - | 30 | 0.0739 | - | - | - |
| ≥10 | 167 | 34 | - | - | - | 40 | - | - | - | |||
| MAP1B expression | Low | 170 | 11 | <0.0001 * | 1 | - | 0.001 * | 17 | <0.0001 * | 1 | - | <0.001 * |
| High | 170 | 50 | 4.115 | 2.077–8.154 | 53 | 3.962 | 2.022–7.763 | |||||
| Parameter | Category | Case No. | Disease-Specific Survival | Metastasis-Free Survival | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Univariate Analysis | Multivariate Analysis | Univariate Analysis | Multivariate Analysis | |||||||||
| No. of Event | p-value | R.R. | 95% C.I. | p-value | No. of Event | p-value | R.R. | 95% C.I. | p-value | |||
| Gender | Male | 216 | 41 | 0.4404 | - | - | - | 60 | 0.2786 | - | - | - |
| Female | 79 | 11 | - | - | - | 16 | - | - | - | |||
| Age (years) | <65 | 121 | 17 | 0.1010 | - | - | - | 31 | 0.6285 | - | - | - |
| ≥65 | 174 | 35 | - | - | - | 45 | ||||||
| Primary tumor (T) | Ta | 84 | 1 | <0.0001 * | 1 | - | <0.001 * | 4 | <0.0001 * | 1 | - | <0.001 * |
| T1 | 88 | 9 | 6.493 | 0.696–60.560 | 23 | 5.044 | 1.469–17.327 | |||||
| T2–T4 | 123 | 42 | 27.783 | 3.011–256.370 | 49 | 7.845 | 2.239–27.484 | |||||
| Nodal metastasis | Negative (N0) | 266 | 41 | 0.0001 * | 1 | - | 0.729 | 61 | <0.0001 * | 1 | - | 0.100 |
| Positive (N1–N2) | 29 | 11 | 1.132 | 0.560–2.288 | 15 | 1.685 | 0.905–3.137 | |||||
| Histological grade | Low grade | 56 | 2 | 0.0010 * | 1 | - | 0.714 | 5 | 0.0005* | 1 | - | 0.572 |
| High grade | 239 | 50 | 0.744 | 0.153–3.610 | 71 | 0.729 | 0.244–2.179 | |||||
| Vascular invasion | Absent | 246 | 37 | 0.0017 * | 1 | - | 0.174 | 54 | 0.0001 * | 1 | - | 0.798 |
| Present | 49 | 15 | 0.624 | 0.316–1.231 | 22 | 1.083 | 0.590–1.985 | |||||
| Perineural invasion | Absent | 275 | 44 | <0.0001 * | 1 | - | 0.099 | 66 | 0.0006 * | 1 | - | 0.339 |
| Present | 20 | 8 | 2.990 | 0.878–4.510 | 10 | 1.422 | 0.690–2.930 | |||||
| Mitotic rate (per 10 high power fields) | <10 | 139 | 12 | <0.0001 * | 1 | - | 0.021 * | 23 | <0.0001 * | 1 | - | 0.045 * |
| ≥10 | 156 | 40 | 2.184 | 1.124–4.246 | 53 | 1.697 | 1.012–2.846 | |||||
| MAP1B expression | Low | 147 | 7 | <0.0001 * | 1 | - | <0.001 * | 16 | <0.0001 * | 1 | - | <0.001 * |
| High | 148 | 45 | 5.551 | 2.466–12.498 | 60 | 3.770 | 2.146–6.622 | |||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chien, T.-M.; Chan, T.-C.; Huang, S.K.-H.; Yeh, B.-W.; Li, W.-M.; Huang, C.-N.; Li, C.-C.; Wu, W.-J.; Li, C.-F. Role of Microtubule-Associated Protein 1b in Urothelial Carcinoma: Overexpression Predicts Poor Prognosis. Cancers 2020, 12, 630. https://doi.org/10.3390/cancers12030630
Chien T-M, Chan T-C, Huang SK-H, Yeh B-W, Li W-M, Huang C-N, Li C-C, Wu W-J, Li C-F. Role of Microtubule-Associated Protein 1b in Urothelial Carcinoma: Overexpression Predicts Poor Prognosis. Cancers. 2020; 12(3):630. https://doi.org/10.3390/cancers12030630
Chicago/Turabian StyleChien, Tsu-Ming, Ti-Chun Chan, Steven Kuan-Hua Huang, Bi-Wen Yeh, Wei-Ming Li, Chun-Nung Huang, Ching-Chia Li, Wen-Jeng Wu, and Chien-Feng Li. 2020. "Role of Microtubule-Associated Protein 1b in Urothelial Carcinoma: Overexpression Predicts Poor Prognosis" Cancers 12, no. 3: 630. https://doi.org/10.3390/cancers12030630
APA StyleChien, T.-M., Chan, T.-C., Huang, S. K.-H., Yeh, B.-W., Li, W.-M., Huang, C.-N., Li, C.-C., Wu, W.-J., & Li, C.-F. (2020). Role of Microtubule-Associated Protein 1b in Urothelial Carcinoma: Overexpression Predicts Poor Prognosis. Cancers, 12(3), 630. https://doi.org/10.3390/cancers12030630