Overexpression of Canonical Prefoldin Associates with the Risk of Mortality and Metastasis in Non-Small Cell Lung Cancer

 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Methods and Materials
2.1. mRNA Expression
2.2. Patient Population
2.3. Tissue Microarrays Immunohistochemical Analysis
2.4. Statistical Analysis
3. Results
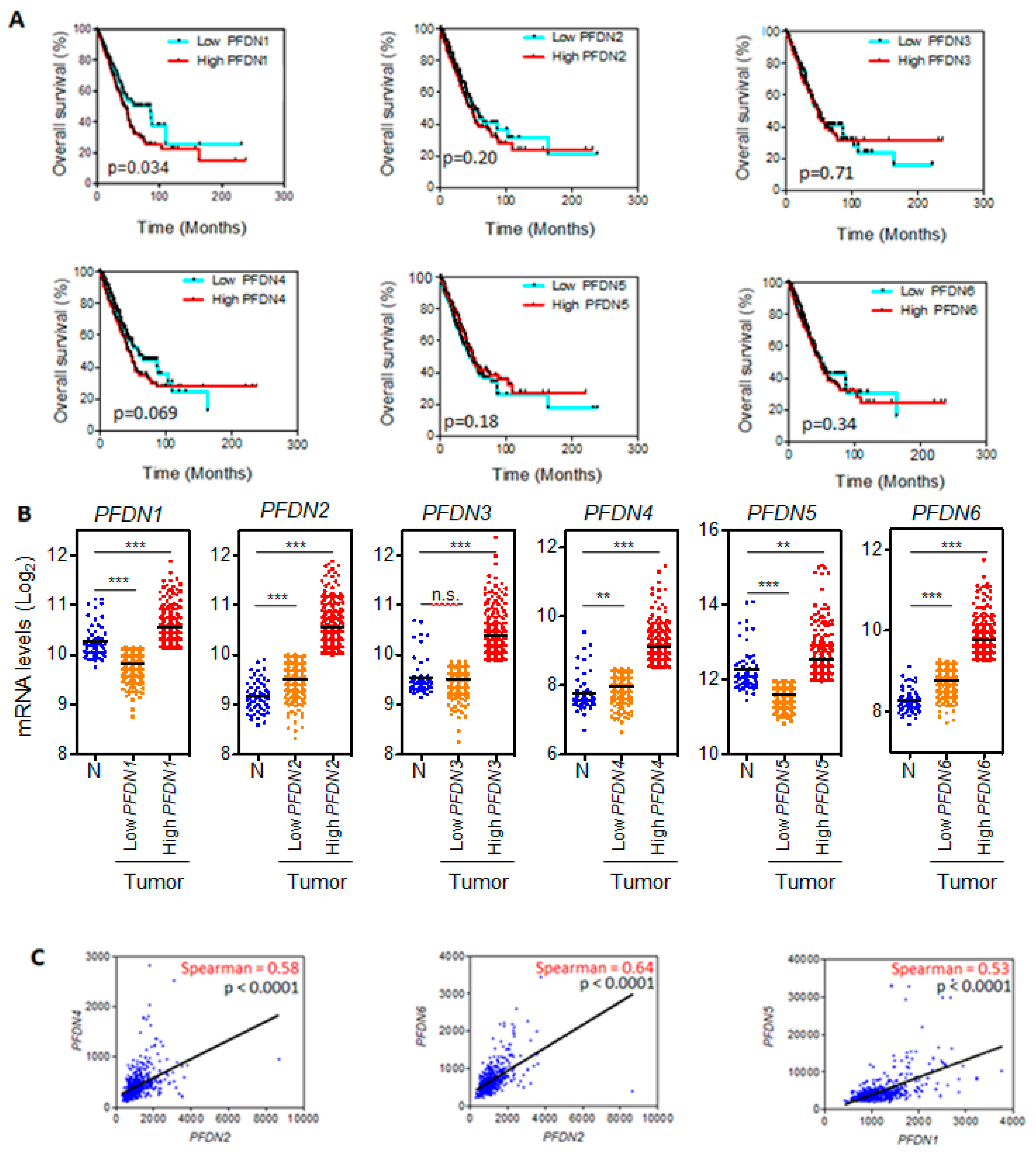
3.1. PFDN1 mRNA Levels Associates with OS in NSCLC
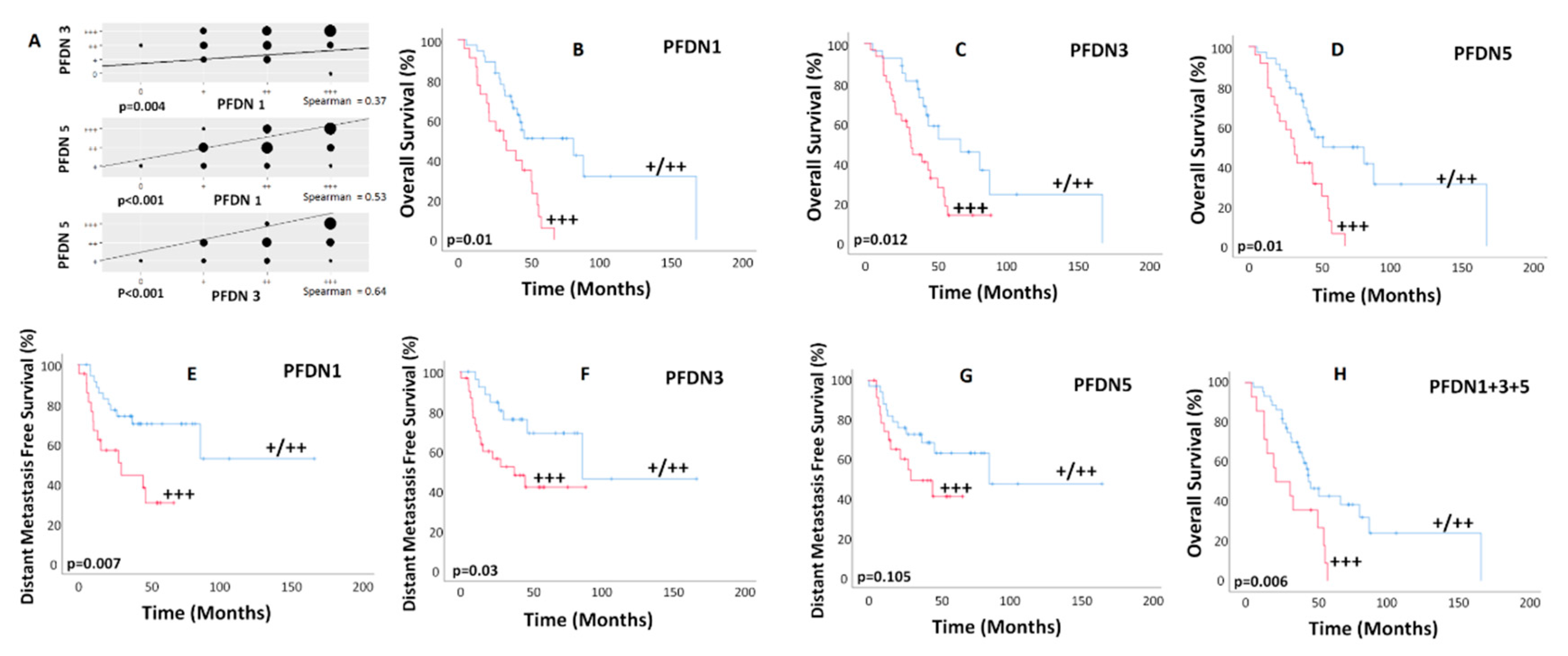
3.2. Association of PFDN and Survival in NSCLC Patients
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Mittal, V. Epithelial Mesenchymal Transition in Tumor Metastasis. Annu. Rev. Pathol. 2018, 13, 395–412. [Google Scholar] [CrossRef] [PubMed]
- Roche, J. The Epithelial-to-Mesenchymal Transition in Cancer. Cancers (Basel) 2018, 10, 52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brabletz, T. To differentiate or not-routes towards metastasis. Nat. Rev. Cancer 2012, 12, 425–436. [Google Scholar] [CrossRef] [PubMed]
- Gupta, P.B.; Pastushenko, I.; Skibinski, A.; Blanpain, C.; Kuperwasser, C. Phenotypic Plasticity: Driver of Cancer Initiation, Progression, and Therapy Resistance. Cell Stem Cell 2019, 24, 65–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lou, Y.; Diao, L.; Cuentas, E.R.; Denning, W.L.; Chen, L.; Fan, Y.H.; Byers, L.A.; Wang, J.; Papadimitrakopoulou, V.A.; Behrens, C.; et al. Epithelial-Mesenchymal Transition Is Associated with a Distinct Tumor Microenvironment Including Elevation of Inflammatory Signals and Multiple Immune Checkpoints in Lung Adenocarcinoma. Clin. Cancer Res. 2016, 22, 3630–3642. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lamouille, S.; Xu, J.; Derynck, R. Molecular mechanisms of epithelial-mesenchymal transition. Nat. Rev. Mol. Cell Biol. 2014, 15, 178–196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lovisa, S.; LeBleu, V.S.; Tampe, B.; Sugimoto, H.; Vadnagara, K.; Carstens, J.L.; Wu, C.C.; Hagos, Y.; Burckhardt, B.C.; Pentcheva-Hoang, T.; et al. Epithelial-to-mesenchymal transition induces cell cycle arrest and parenchymal damage in renal fibrosis. Nat. Med. 2015, 21, 998–1009. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Shi, W.; Tang, Y.; Liu, Y.; He, K.; Hu, Y.; Li, J.; Yang, Y.; Song, J. Prefoldin 1 promotes EMT and lung cancer progression by suppressing cyclin A expression. Oncogene 2017, 36, 885–898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vainberg, I.E.; Lewis, S.A.; Rommelaere, H.; Ampe, C.; Vandekerckhove, J.; Klein, H.L.; Cowan, N.J. Prefoldin, a chaperone that delivers unfolded proteins to cytosolic chaperonin. Cell 1998, 93, 863–873. [Google Scholar] [CrossRef] [Green Version]
- Millan-Zambrano, G.; Chavez, S. Nuclear functions of prefoldin. Open Biol. 2014, 4, 140085. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Payan-Bravo, L.; Penate, X.; Chavez, S. Functional Contributions of Prefoldin to Gene Expression. Adv. Exp. Med. Biol. 2018, 1106, 1–10. [Google Scholar] [PubMed]
- Chaves-Perez, A.; Thompson, S.; Djouder, N. Roles and Functions of the Unconventional Prefoldin URI. Adv. Exp. Med. Biol. 2018, 1106, 95–108. [Google Scholar] [PubMed]
- Abreu, R.d.; Penalva, L.O.; Marcotte, E.M.; Vogel, C. Global signatures of protein and mRNA expression levels. Mol. BioSyst. 2009, 5, 1512–1526. [Google Scholar]
- Vogel, C.; Marcotte, E.M. Insights into the regulation of protein abundance from proteomic and transcriptomic analyses. Nat. Rev. Genet. 2012, 13, 227–232. [Google Scholar] [CrossRef] [PubMed]
- Biswas, D.; Birkbak, N.J.; Rosenthal, R.; Hiley, C.T.; Lim, E.L.; Papp, K.; Boeing, S.; Krzystanek, M.; Djureinovic, D.; la Fleur, L.; et al. A clonal expression biomarker associates with lung cancer mortality. Nat. Med. 2019, 25, 1540–1548. [Google Scholar] [CrossRef] [PubMed]
- Hung, J.J.; Yang, M.H.; Hsu, H.S.; Hsu, W.H.; Liu, J.S.; Wu, K.J. Prognostic significance of hypoxia-inducible factor-1alpha, TWIST1 and Snail expression in resectable non-small cell lung cancer. Thorax 2009, 64, 1082–1089. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Characteristics | NO. of Patients (%) n = 58 |
|---|---|
| Gender | |
| Female | 8 (14) |
| Male | 50 (86) |
| Age, years | |
| Median (range) | 67 (41–82) |
| Chronic obstructive pulmonary disease | |
| No | 34 (59) |
| Yes | 24 (41) |
| Hypertension | |
| No | 31 (53) |
| Yes | 27 (57) |
| Diabetes Mellitus | |
| No | 42 (58) |
| Yes | 16 (42) |
| Dyslipidemia | |
| No | 26 (45) |
| Yes | 32 (55) |
| Cardiovascular disease | |
| No | 45 (78) |
| Yes | 13 (22) |
| Thrombosis | |
| No | 49 (84) |
| Yes | 9 (16) |
| Smoking status | |
| Never | 3 (5) |
| Former | 28 (48) |
| Current | 27 (47) |
| History of alcohol consumption | |
| No | 31 (53) |
| Yes | 27 (47) |
| Karnofsky Performance Status | |
| 100 | 13 (22) |
| 90 | 15 (26) |
| 80 | 16 (28) |
| 70 | 14 (24) |
| Histology | |
| Adenocarcinoma | 24 (41) |
| Squamous | 34 (59) |
| T stage | |
| T1 | 13 (22) |
| T2 | 28 (48) |
| T3 | 11 (19) |
| T4 | 6 (10) |
| N stage | |
| N0 | 19 (33) |
| N1 | 8 (14) |
| N2 | 25 (43) |
| N3 | 6 (10) |
| M stage | |
| M0 | 53 (91) |
| M1 | 5 (9) |
| Stage | |
| IA | 1 (2) |
| IB | 13 (22) |
| IIA | 4 (7) |
| IIIA | 27 (47) |
| IIIB | 8 (14) |
| IV | 5 (9) |
| Surgery | |
| Yes | 52 (90) |
| No | 6 (10) |
| Thoracic radiation therapy * | |
| Yes | 24 (41) |
| No | 34 (59) |
| Chemotherapy ** | |
| Yes | 40 (69) |
| No | 18 (31) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peñate, X.; Praena-Fernández, J.M.; Romero Pareja, P.; Enguix-Riego, M.d.V.; Payán-Bravo, L.; Vieites, B.; Gomez-Izquierdo, L.; Jaen Olasolo, J.; Rivin del Campo, E.; Reyes, J.C.; et al. Overexpression of Canonical Prefoldin Associates with the Risk of Mortality and Metastasis in Non-Small Cell Lung Cancer. Cancers 2020, 12, 1052. https://doi.org/10.3390/cancers12041052
Peñate X, Praena-Fernández JM, Romero Pareja P, Enguix-Riego MdV, Payán-Bravo L, Vieites B, Gomez-Izquierdo L, Jaen Olasolo J, Rivin del Campo E, Reyes JC, et al. Overexpression of Canonical Prefoldin Associates with the Risk of Mortality and Metastasis in Non-Small Cell Lung Cancer. Cancers. 2020; 12(4):1052. https://doi.org/10.3390/cancers12041052
Chicago/Turabian StylePeñate, Xenia, Juan Manuel Praena-Fernández, Pedro Romero Pareja, María del Valle Enguix-Riego, Laura Payán-Bravo, Begoña Vieites, Lourdes Gomez-Izquierdo, Javier Jaen Olasolo, Eleonor Rivin del Campo, Jose Carlos Reyes, and et al. 2020. "Overexpression of Canonical Prefoldin Associates with the Risk of Mortality and Metastasis in Non-Small Cell Lung Cancer" Cancers 12, no. 4: 1052. https://doi.org/10.3390/cancers12041052
APA StylePeñate, X., Praena-Fernández, J. M., Romero Pareja, P., Enguix-Riego, M. d. V., Payán-Bravo, L., Vieites, B., Gomez-Izquierdo, L., Jaen Olasolo, J., Rivin del Campo, E., Reyes, J. C., Chávez, S., & Lopez Guerra, J. L. (2020). Overexpression of Canonical Prefoldin Associates with the Risk of Mortality and Metastasis in Non-Small Cell Lung Cancer. Cancers, 12(4), 1052. https://doi.org/10.3390/cancers12041052