The Clinicopathological and Prognostic Significance of Nrf2 and Keap1 Expression in Hepatocellular Carcinoma

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Results
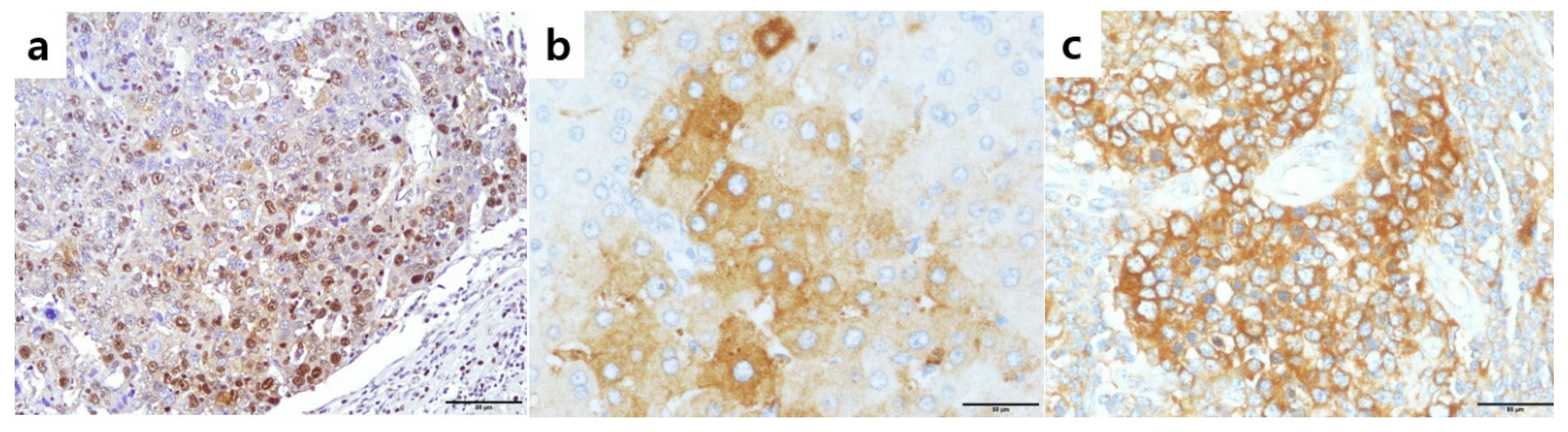
2.1. pNrf2 Expression in HCCs and Clinicopathological Correlation
2.2. Cytoplasmic Nrf2 Expression in HCCs and Clinicopathological Correlation
2.3. Keap1 Expression in HCCs and Clinicopathological Correlation
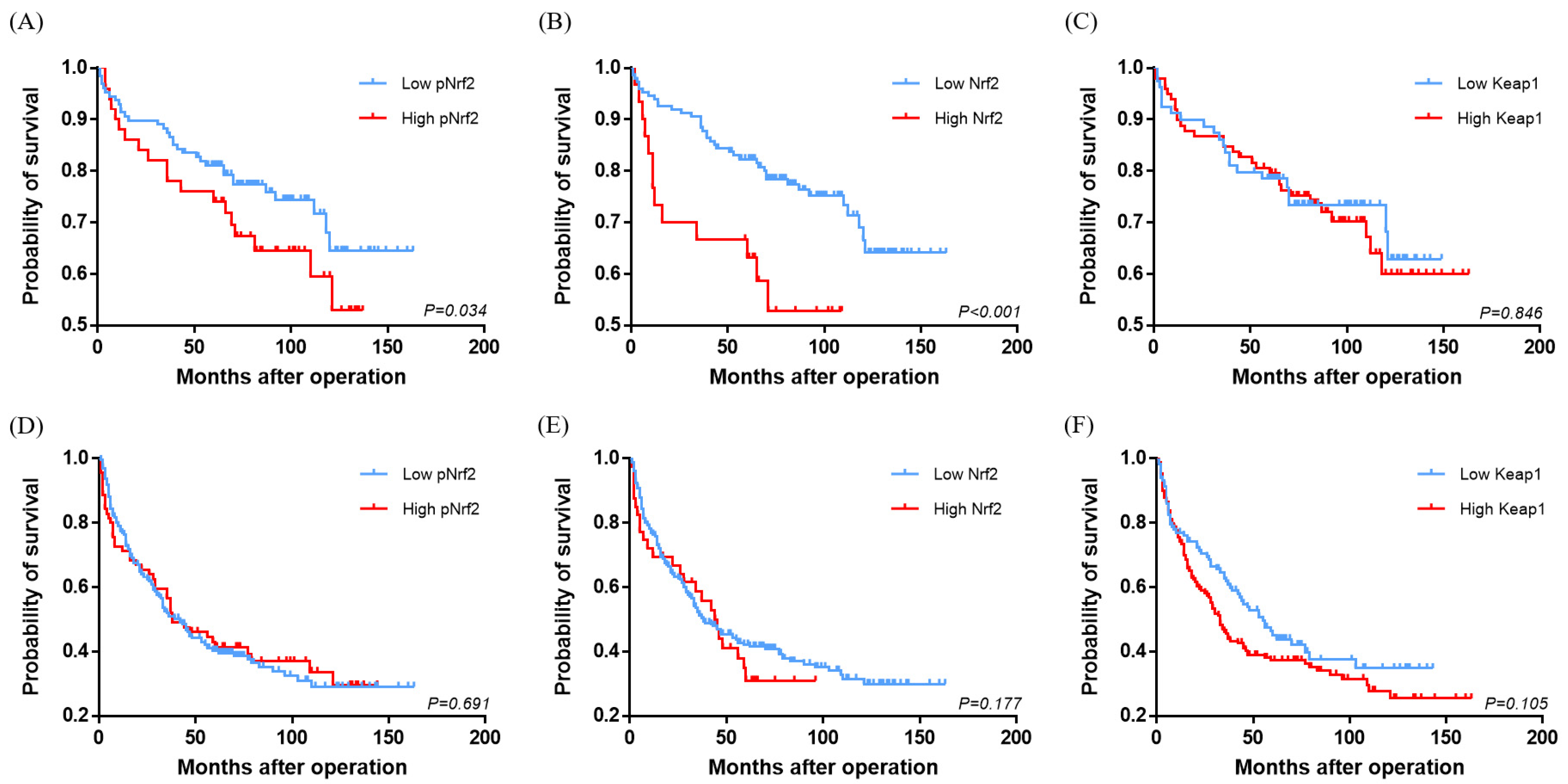
2.4. Multivariate Survival Analysis
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Tissue Samples and Immunohistochemistry
4.3. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Mathers, C.; Parkin, D.M.; Piñeros, M.; Znaor, A.; Bray, F. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int. J. Cancer 2019, 144, 1941–1953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujimoto, A.; Furuta, M.; Totoki, Y.; Tsunoda, T.; Kato, M.; Shiraishi, Y.; Tanaka, H.; Taniguchi, H.; Kawakami, Y.; Ueno, M.; et al. Whole-genome mutational landscape and characterization of noncoding and structural mutations in liver cancer. Nat. Genet. 2016, 48, 500–509. [Google Scholar] [CrossRef] [PubMed]
- Guichard, C.; Amaddeo, G.; Imbeaud, S.; Ladeiro, Y.; Pelletier, L.; Ben Maad, I.; Calderaro, J.; Bioulac-Sage, P.; Letexier, M.; Degos, F.; et al. Integrated analysis of somatic mutations and focal copy-number changes identifies key genes and pathways in hepatocellular carcinoma. Nat. Genet. 2012, 44, 694. [Google Scholar] [CrossRef] [PubMed]
- Cancer Genome Atlas Research Network. Comprehensive and Integrative Genomic Characterization of Hepatocellular Carcinoma. Cell 2017, 169, 1327–1341. [Google Scholar] [CrossRef] [PubMed]
- Torbenson, M.S.; Ng, I.O.L.; Park, Y.N.; Roncalli, M.; Sakamoto, M. Hepatocellular carcinoma. In WHO Classification of Tumours Editorial Board, 5th ed.; Digestive System Tumours, Ed.; International Agency for Research on Cancer: Lyon, France, 2019; pp. 229–239. [Google Scholar]
- Zucman-Rossi, J.; Villanueva, A.; Nault, J.C.; Llovet, J.M. Genetic Landscape and Biomarkers of Hepatocellular Carcinoma. Gastroenterology 2015, 149, 1226–1239. [Google Scholar] [CrossRef] [Green Version]
- Sporn, M.B.; Liby, K.T. NRF2 and cancer: The good, the bad and the importance of context. Nat. Rev. Cancer 2012, 12, 564–571. [Google Scholar] [CrossRef]
- Suzuki, T.; Motohashi, H.; Yamamoto, M. Toward clinical application of the Keap1-Nrf2 pathway. Trends Pharm. Sci. 2013, 34, 340–346. [Google Scholar] [CrossRef]
- Chun, Y.; Ye-xiong, T.; Guang-zhen, Y.; Jian, Z.; Yu-fei, P.; Chen, L.; Jing, F.; Yao, C.; Zhi-wen, D.; Li-wei, D.; et al. Gankyrin has an antioxidative role through the feedback regulation of Nrf2 in hepatocellular carcinoma. J. Exp. Med. 2016, 213, 859–875. [Google Scholar]
- Kahroba, H.; Shirmohamadi, M.; Hejazi, M.S.; Samadi, N. The Role of Nrf2 signaling in cancer stem cells: From stemness and self-renewal to tumorigenesis and chemoresistance. Life Sci. 2019, 239, 116986. [Google Scholar] [CrossRef]
- Jaramillo, M.C.; Zhang, D.D. The emerging role of the Nrf2-Keap1 signaling pathway in cancer. Genes Dev. 2013, 27, 2179–2191. [Google Scholar] [CrossRef] [Green Version]
- Ngo, H.K.C.; Kim, D.H.; Cha, Y.N.; Na, H.K.; Surh, Y.J. Nrf2 Mutagenic Activation Drives Hepatocarcinogenesis. Cancer Res. 2017, 77, 4797–4808. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raghunath, A.; Sundarraj, K.; Arfuso, F.; Sethi, G.; Perumal, E. Dysregulation of Nrf2 in Hepatocellular Carcinoma: Role in Cancer Progression and Chemoresistance. Cancers 2018, 10, 481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, C.; Cheng, L.; Wu, H.; He, P.; Zhang, Y.; Yang, Y.; Chen, J.; Chen, M. Activation of the KEAP1-NRF2-ARE signaling pathway reduces oxidative stress in Hep2 cells. Mol. Med. Rep. 2018, 18, 2541–2550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahtikoski, A.M.; Kangas, J.; Salonen, R.; Puistola, U.; Karihtala, P. Cytoplasmic Keap1 Expression Is Associated With Poor Prognosis in Endometrial Cancer. Anticancer. Res. 2019, 39, 585–590. [Google Scholar] [CrossRef]
- Chen, J.; Yu, Y.; Ji, T.; Ma, R.; Chen, M.; Li, G.; Li, F.; Ding, Q.; Kang, Q.; Huang, D.; et al. Clinical implication of Keap1 and phosphorylated Nrf2 expression in hepatocellular carcinoma. Cancer Med. 2016, 5, 2678–2687. [Google Scholar] [CrossRef]
- Cho, H.Y.; Kim, K.; Kim, Y.B.; Kim, H.; No, J.H. Expression Patterns of Nrf2 and Keap1 in Ovarian Cancer Cells and their Prognostic Role in Disease Recurrence and Patient Survival. Int. J. Gynecol. Cancer 2017, 27, 412–419. [Google Scholar] [CrossRef]
- Guo, Y.; Shen, L. Overexpression of NRF 2 is correlated with prognoses of patients with malignancies: A meta-analysis. Thorac. Cancer 2017, 8, 558–564. [Google Scholar] [CrossRef]
- Isohookana, J.; Haapasaari, K.M.; Soini, Y.; Karihtala, P. Keap1 expression has independent prognostic value in pancreatic adenocarcinomas. Diagn. Pathol. 2015, 10, 28. [Google Scholar] [CrossRef] [Green Version]
- Lingzhi, P.; Yaoxing, D.; Yongbin, Z.; Diande, Z.; Yanghui, W.; Jibin, Y.; Mingxu, D. Expression of Nrf2 and NQO1 in human gastric cancer and their clinical significance. Int. J. Clin. Exp. Pathol. 2016, 9, 1635–1643. [Google Scholar]
- Wang, L.; Zhang, C.; Qin, L.; Xu, J.; Li, X.; Wang, W.; Kong, L.; Zhou, T.; Li, X. The prognostic value of NRF2 in solid tumor patients: A meta-analysis. Oncotarget 2018, 9, 1257–1265. [Google Scholar] [CrossRef] [Green Version]
- Zhang, M.; Zhang, C.; Zhang, L.; Yang, Q.; Zhou, S.; Wen, Q.; Wang, J. Nrf2 is a potential prognostic marker and promotes proliferation and invasion in human hepatocellular carcinoma. BMC Cancer 2015, 15, 531. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olivier, G.; Mina, K.; Johannes, B.; Bart, S.; Carl, J.; Francesca, L.; Aezam, K.; Jasper, W.; Léon, K.; Anne, D.; et al. Keratin 19: A key role player in the invasion of human hepatocellular carcinomas. Gut 2014, 63, 674–685. [Google Scholar]
- Kawai, T.; Yasuchika, K.; Ishii, T.; Katayama, H.; Yoshitoshi, E.Y.; Ogiso, S.; Kita, S.; Yasuda, K.; Fukumitsu, K.; Mizumoto, M.; et al. Keratin 19, a Cancer Stem Cell Marker in Human Hepatocellular Carcinoma. Clin. Cancer Res. 2015, 21, 3081–3091. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, H.; Choi, G.H.; Na, D.C.; Ahn, E.Y.; Kim, G.I.; Lee, J.E.; Cho, J.Y.; Yoo, J.E.; Choi, J.S.; Park, Y.N. Human hepatocellular carcinomas with “Stemness”-related marker expression: Keratin 19 expression and a poor prognosis. Hepatology 2011, 54, 1707–1717. [Google Scholar] [CrossRef] [PubMed]
- Rhee, H.; Nahm, J.H.; Kim, H.; Choi, G.H.; Yoo, J.E.; Lee, H.S.; Koh, M.J.; Park, Y.N. Poor outcome of hepatocellular carcinoma with stemness marker under hypoxia: Resistance to transarterial chemoembolization. Mod. Pathol. 2016, 29, 1038–1049. [Google Scholar] [CrossRef]
- Uhlen, M.; Fagerberg, L.; Hallstrom, B.M.; Lindskog, C.; Oksvold, P.; Mardinoglu, A.; Sivertsson, A.; Kampf, C.; Sjöstedt, E.; Asplund, A.; et al. Proteomics. Tissue-based map of the human proteome. Science 2015, 347, 1260419. [Google Scholar] [CrossRef]
- Chandrashekar, D.S.; Bashel, B.; Balasubramanya, S.A.H.; Creighton, C.J.; Ponce-Rodriguez, I.; Chakravarthi, B.V.; Varambally, S. UALCAN: A Portal for Facilitating Tumor Subgroup Gene Expression and Survival Analyses. Neoplasia 2017, 19, 649–658. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Parameters | Frequency (%) or Median (Range) |
|---|---|
| Sex, n (%) | |
| Male | 216 (75.8) |
| Female | 69 (24.2) |
| Age at operation, median (range, years) | 63 (29–87) |
| Etiology, n (%) | |
| Hepatitis B virus (HBV) | 202 (70.9) |
| Hepatitis C virus (HCV) | 25 (8.8) |
| HBV + HCV | 1 (0.3) |
| Alcohol | 14 (4.9) |
| Non-alcoholic fatty liver disease | 12 (4.2) |
| Uncertain etiology | 31 (10.9) |
| Tumor size, median (range, cm) | 3.2 (0.9–17) |
| Multiplicity present, n (%) | 49 (17.2) |
| Edmondson–Steiner grade, n (%) | |
| Grade I | 3 (1.0) |
| Grade II | 77 (27.0) |
| Grade III | 171 (60.0) |
| Grade IV | 34 (12.0) |
| Microvascular invasion present, n (%) | 113 (39.6) |
| Portal vein invasion present, n (%) | 19 (6.7) |
| Pathologic T category (AJCC 8th edition), n (%) | |
| pT1a | 37 (13.0) |
| pT1b | 101 (35.4) |
| pT2 | 112 (39.3) |
| pT3 | 11 (3.9) |
| pT4 | 24 (8.4) |
| Extrahepatic metastasis present, n (%) | 55 (19.3) |
| Cirrhosis in background liver present, n (%) | 152 (533.3) |
| Recurrence on follow-up present, n (%) | 161 (56.5) |
| Status at last follow-up, n (%) | |
| Alive | 128 (44.9) |
| Deceased of disease | 44 (15.4) |
| Deceased of other cause | 10 (3.5) |
| Follow up loss | 103 (36.2) |
| Overall survival, median (range, months) | 66.5 (0–163) |
| Disease-free survival, median (range, months) | 32.5 (0–163) |
| Parameter | pNrf2 | p-Value | Nrf2 | p-Value | Keap1 | p-Value | |||
|---|---|---|---|---|---|---|---|---|---|
| Low pNrf2 | High pNrf2 | Low Nrf2 | High Nrf2 | Low Keap1 | High Keap1 | ||||
| Frequency | 212 (74.3) | 73 (25.6) | - | 237 (83.2) | 48 (16.8) | - | 124 (43.5) | 161 (56.5) | - |
| Sex (male/female) | 159 (75.0)/53 (25.0) | 57 (78.1)/16 (21.9) | 0.638 | 179 (75.5)/58 (24.5) | 37 (77.1)/11 (22.9) | 1.000 | 94 (75.8)/30 (24.2) | 122 (75.8)/39 (24.2) | 1.000 |
| Age ≥60 years | 95 (44.8) | 28 (38.4) | 0.411 | 100 (42.2) | 23 (47.9) | 0.542 | 55 (44.7) | 68 (42.2) | 0.809 |
| HBV-related etiology | 150 (70.8) | 53 (72.6) | 0.881 | 167 (70.5) | 36 (75.0) | 0.602 | 86 (69.4) | 117 (72.7) | 0.598 |
| Size (cm, mean ± SD) | 4.2 ± 3.0 | 4.0 ± 2.4 | 0.274 | 4.4 ± 2.9 | 3.1 ± 1.8 | 0.005 | 4.4 ± 3.1 | 3.9 ± 2.5 | 0.105 |
| Multiplicity | 37 (17.5) | 12 (16.4) | 1.000 | 41 (17.3) | 8 (16.7) | 1.000 | 23 (18.5) | 26 (16.1) | 0.636 |
| E–S grade III and IV | 155 (73.1) | 50 (68.5) | 0.454 | 173 (73.0) | 32 (66.7) | 0.382 | 92 (74.2) | 113 (70.2) | 0.507 |
| Microvascular invasion | 78 (36.8) | 35 (47.9) | 0.098 | 96 (40.5) | 17 (35.4) | 0.628 | 47 (37.9) | 66 (41.0) | 0.627 |
| Portal vein invasion | 12 (5.7) | 7 (9.6) | 0.278 | 17 (7.2) | 2 (4.2) | 0.750 | 12 (9.7) | 7 (4.3) | 0.094 |
| pT category | 0.146 | 0.323 | 0.166 | ||||||
| pT1a | 31 (14.6) | 6 (8.2) | 33 (13.9) | 4 (8.3) | 18 (14.5) | 19 (11.8) | |||
| pT1b | 75 (35.4) | 26 (35.6) | 83 (35.0) | 18 (37.5) | 46 (37.1) | 55 (34.2) | |||
| pT2 | 76 (35.8) | 36 (49.3) | 89 (37.6) | 23 (47.9) | 41 (33.1) | 71 (44.1) | |||
| pT3 | 10 (4.7) | 1 (1.4) | 11 (4.6) | 0 (0) | 4 (3.2) | 7 (4.3) | |||
| pT4 | 20 (9.4) | 4 (5.5) | 21 (8.9) | 3 (6.3) | 15 (12.1) | 9 (5.6) | |||
| Recurrence | 118 (55.7) | 43 (58.9) | 0.784 | 133 (56.1) | 28 (58.3) | 0.748 | 64 (51.6) | 97 (60.2) | 0.183 |
| Extrahepatic metastasis | 37 (17.6) | 18 (24.7) | 0.229 | 50 (21.2) | 5 (9.1) | 0.109 | 24 (19.5) | 31 (19.4) | 1.000 |
| Underlying cirrhosis | 108 (52.9) | 44 (60.3) | 0.338 | 125 (54.1) | 27 (58.7) | 0.628 | 65 (55.1) | 87 (54.7) | 1.000 |
| K19 expression | 38 (17.9) | 16 (21.9) | 0.490 | 42 (17.7) | 12 (25.0) | 0.233 | 18 (14.5) | 36 (22.4) | 0.127 |
| EpCAM expression | 84 (39.6) | 41 (56.2) | 0.020 | 103 (43.5) | 22 (45.8) | 0.873 | 49 (39.5) | 76 (47.2) | 0.229 |
| CAIX expression | 48 (23.4) | 27 (37.5) | 0.030 | 55 (24.0) | 20 (41.7) | 0.019 | 31 (25.4) | 44 (28.4) | 0.589 |
| Ezrin expression | 78 (36.8) | 43 (59.7) | 0.001 | 90 (38.1) | 31 (64.6) | 0.001 | 48 (38.7) | 73 (45.6) | 0.277 |
| uPAR expression | 58 (27.5) | 26 (36.1) | 0.180 | 70 (29.7) | 14 (29.8) | 1.000 | 29 (23.4) | 55 (34.6) | 0.049 |
| E-cadherin loss | 128 (60.4) | 56 (76.7) | 0.015 | 153 (64.6) | 31 (64.6) | 1.000 | 81 (65.3) | 103 (64.0) | 0.901 |
| p53 overexpression | 40 (20.5) | 26 (37.1) | 0.009 | 53 (24.1) | 13 (28.9) | 0.570 | 19 (16.1) | 47 (32.0) | 0.004 |
| Mitotic index (/10 HPF, mean ± SD) | 10.1 ± 13.4 | 17.4 ± 20.0 | <0.001 | 11.9 ± 15.6 | 12.2 ± 16.1 | 0.623 | 10.5 ± 13.6 | 13.1 ± 16.9 | 0.056 |
| Ki-67 labeling index (%, mean ± SD) | 5.1 ± 7.5 | 12.9 ± 12.2 | <0.001 | 7.2 ± 9.6 | 6.7 ± 9.6 | 0.935 | 5.7 ± 8.5 | 8.1 ± 10.2 | 0.035 |
| Parameter | Overall Survival | Disease-Free Survival | ||||||
|---|---|---|---|---|---|---|---|---|
| Univariate Analysis | Multivariate Analysis | Univariate Analysis | Multivariate Analysis | |||||
| Parameters | HR (95% CI) | p-Value | HR (95% CI) | p-Value | HR (95% CI) | p-Value | HR (95% CI) | p-Value |
| Sex (male/female) | 0.742 (0.345–1.597) | 0.446 | - | - | 0.702 (0.480–1.029) | 0.069 | - | - |
| Age (≥60/<60 years) | 0.960 (0.522–1.765) | 0.894 | - | - | 0.848 (0.621–1.157) | 0.299 | - | - |
| Underlying HBV | 1.160 (0.586–2.296) | 0.671 | - | - | 1.129 (0.801–1.590) | 0.488 | - | - |
| Size (≥5cm/<5cm) | 2.400 (1.315–4.382) | 0.004 | 1.298 (0.650–2.594) | 0.460 | 1.418 (1.012–1.988) | 0.043 | 1.085 (0.765–1.540) | 0.647 |
| Multiplicity | 2.812 (1.488–5.312) | 0.001 | 2.156 (1.093–4.253) | 0.027 | 1.991 (1.375–2.884) | <0.001 | 1.487 (1.015–2.180) | 0.042 |
| E–S grade III and IV | 0.951 (0.497–1.818) | 0.879 | - | - | 1.095 (0.778–1.542) | 0.601 | - | - |
| Microvascular invasion | 1.477 (0.813–2.682) | 0.200 | - | - | 1.308 (0.962–1.779) | 0.087 | - | - |
| Portal vein invasion | 3.289 (1.386–7.804) | 0.007 | 2.435 (0.980–6.052) | 0.055 | 1.573 (0.853–2.903) | 0.147 | - | - |
| Extrahepatic metastasis | 4.458 (2.445–8.130) | <0.001 | 3.256 (1.742–6.083) | <0.001 | 4.799 (3.411–6.753) | <0.001 | 4.475 (3.152–6.354) | <0.001 |
| Underlying cirrhosis | 1.282 (0.702–2.340) | 0.419 | - | - | 1.031 (0.758–1.404) | 0.844 | - | - |
| K19 | 1.860 (0.957–3.614) | 0.067 | - | - | 1.209 (0.826–1.771) | 0.329 | - | - |
| EpCAM | 1.727 (0.951-3.137) | 0.073 | - | - | 0.889 (0.613–1.292) | 0.538 | - | - |
| CAIX | 1.854 (1.015–3.386) | 0.044 | 1.402 (0.738–2.664) | 0.302 | 1.043 (0.743–1.464) | 0.809 | - | - |
| Ezrin | 3.160 (1.674–5.966) | <0.001 | 2.893 (1.527–5.483) | 0.001 | 1.090 (0.766–1.552) | 0.632 | - | - |
| uPAR | 1.492 (0.812–2.743) | 0.198 | 1.058 (0.756–1.480) | 0.742 | ||||
| E-cadherin loss | 1.037 (0.556–1.936) | 0.909 | 0.853 (0.622–1.169) | 0.323 | ||||
| p53 overexpression | 1.777 (0.961–3.288) | 0.067 | - | - | 1.219 (0.854–1.740) | 0.276 | - | - |
| Nrf2 | 3.329 (1.738–6.374) | <0.001 | 4.151 (2.025–8.508) | <0.001 | 1.315 (0.879–1.968) | 0.183 | - | - |
| pNrf2 | 1.894 (1.037–3.458) | 0.038 | 1.181 (0.950–3.450) | 0.071 | 0.933 (0.661–1.317) | 0.693 | - | - |
| Keap1 | 1.061 (0.582–1.937) | 0.846 | - | - | 1.290 (0.944–1.762) | 0.109 | - | - |
| Antibody | Description | Source | Dilution | Method |
|---|---|---|---|---|
| Nrf2 | Rabbit monoclonal (EP1808Y) | Abcam | 1:50 | Autostainer |
| (Cambridge, UK) | ||||
| pNrf2 | Rabbit monoclonal (EP1809Y) | Abcam | 1:100 | Autostainer |
| (Cambridge, UK) | ||||
| Keap1 | Rabbit polyclonal | Proteintech | 1:300 | Autostainer |
| (Manchester, UK) | ||||
| Keratin 19 (K19) | Mouse monoclonal (RCK108) | Dako | 1:200 | Autostainer |
| (Glostrup, Denmark) | ||||
| EpCAM | Mouse monoclonal (VU-1D9) | Millipore | 1:1500 | Autostainer |
| (Temecula, CA, USA) | ||||
| Ezrin | Mouse monoclonal (3C12) | Abcam | 1:100 | Manual (pH 6.0) |
| (Cambridge, UK) | ||||
| uPAR | Mouse monoclonal (R-4) | Abcam | 1:40 | Manual (pH 6.0) |
| (Cambridge, UK) | ||||
| E-cadherin | Mouse monoclonal (36B5) | Novocastra | 1:100 | Autostainer |
| (Newcastle, UK) | ||||
| CAIX | Rabbit polyclonal | Abcam | 1:500 | Autostainer |
| (Cambridge, UK) | ||||
| p53 | Mouse monoclonal (DO-7) | Dako | 1:1000 | Autostainer |
| (Glostrup, Denmark) | ||||
| Ki-67 | Mouse monoclonal (MIB-1) | Dako | 1:100 | Autostainer |
| (Glostrup, Denmark) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, K.; Kim, S.; Lee, Y.; Lee, H.; Lee, Y.; Park, H.; Nahm, J.H.; Ahn, S.; Yu, S.J.; Lee, K.; et al. The Clinicopathological and Prognostic Significance of Nrf2 and Keap1 Expression in Hepatocellular Carcinoma. Cancers 2020, 12, 2128. https://doi.org/10.3390/cancers12082128
Lee K, Kim S, Lee Y, Lee H, Lee Y, Park H, Nahm JH, Ahn S, Yu SJ, Lee K, et al. The Clinicopathological and Prognostic Significance of Nrf2 and Keap1 Expression in Hepatocellular Carcinoma. Cancers. 2020; 12(8):2128. https://doi.org/10.3390/cancers12082128
Chicago/Turabian StyleLee, Kiryang, Seunghye Kim, Yangkyu Lee, Hyejung Lee, Youngeun Lee, Hyunjin Park, Ji Hae Nahm, Soomin Ahn, Su Jong Yu, Kyoungbun Lee, and et al. 2020. "The Clinicopathological and Prognostic Significance of Nrf2 and Keap1 Expression in Hepatocellular Carcinoma" Cancers 12, no. 8: 2128. https://doi.org/10.3390/cancers12082128
APA StyleLee, K., Kim, S., Lee, Y., Lee, H., Lee, Y., Park, H., Nahm, J. H., Ahn, S., Yu, S. J., Lee, K., & Kim, H. (2020). The Clinicopathological and Prognostic Significance of Nrf2 and Keap1 Expression in Hepatocellular Carcinoma. Cancers, 12(8), 2128. https://doi.org/10.3390/cancers12082128