Histopathologic Response Is a Positive Predictor of Overall Survival in Patients Undergoing Neoadjuvant/Perioperative Chemotherapy for Locally Advanced Gastric or Gastroesophageal Junction Cancers—Analysis from a Large Single Center Cohort in Germany



Abstract
:1. Introduction
2. Results
2.1. Patient Data
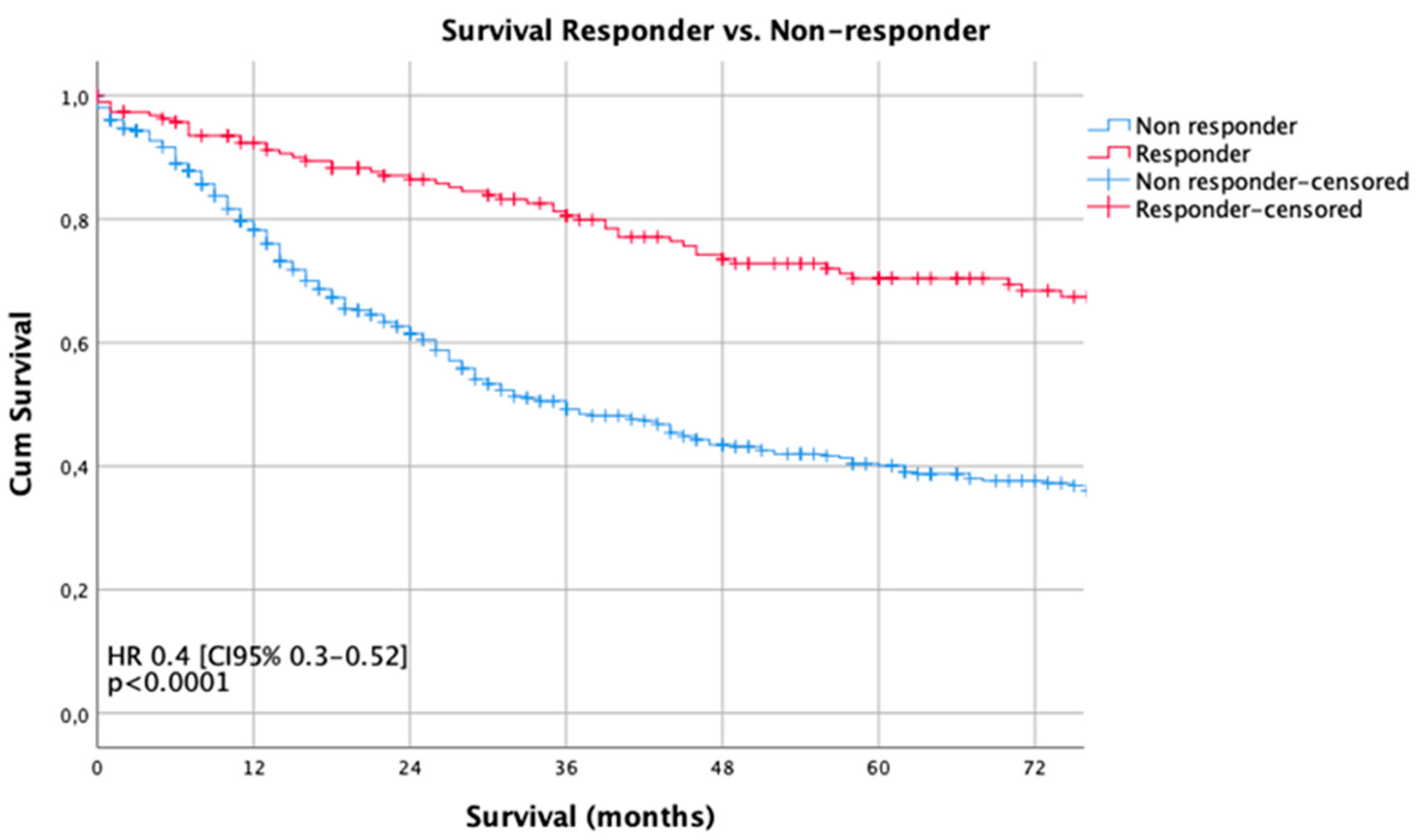
2.2. Predictors of Overall Survival
2.3. Histopathologic Response
Predictors of HPR
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lagarde, S.M.; ten Kate, F.J.; Reitsma, J.B.; Busch, O.R.; van Lanschot, J.J. Prognostic factors in adenocarcinoma of the esophagus or gastroesophageal junction. J. Clin. Oncol. 2006, 24, 4347–4355. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, D.; Allum, W.H.; Stenning, S.P.; Thompson, J.N.; Van de Velde, C.J.; Nicolson, M.; Scarffe, J.H.; Lofts, F.J.; Falk, S.J.; Iveson, T.J.; et al. Perioperative chemotherapy versus surgery alone for resectable gastroesophageal cancer. N. Engl. J. Med. 2006, 355, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Van Hagen, P.; Hulshof, M.C.; van Lanschot, J.J.; Steyerberg, E.W.; van Berge Henegouwen, M.I.; Wijnhoven, B.P.; Richel, D.J.; Nieuwenhuijzen, G.A.; Hospers, G.A.; Bonenkamp, J.J.; et al. Preoperative chemoradiotherapy for esophageal or junctional cancer. N. Engl. J. Med. 2012, 366, 2074–2084. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ychou, M.; Boige, V.; Pignon, J.P.; Conroy, T.; Bouche, O.; Lebreton, G.; Ducourtieux, M.; Bedenne, L.; Fabre, J.M.; Saint-Aubert, B.; et al. Perioperative chemotherapy compared with surgery alone for resectable gastroesophageal adenocarcinoma: An FNCLCC and FFCD multicenter phase III trial. J. Clin. Oncol. 2011, 29, 1715–1721. [Google Scholar] [CrossRef] [PubMed]
- Reim, D.; Gertler, R.; Novotny, A.; Becker, K.; zum Büschenfelde, C.M.; Ebert, M.; Dobritz, M.; Langer, R.; Hoefler, H.; Friess, H.; et al. Adenocarcinomas of the esophagogastric junction are more likely to respond to preoperative chemotherapy than distal gastric cancer. Ann. Surg. Oncol. 2012, 19, 2108–2118. [Google Scholar] [CrossRef] [PubMed]
- Ronellenfitsch, U.; Schwarzbach, M.; Hofheinz, R.; Kienle, P.; Kieser, M.; Slanger, T.E.; Burmeister, B.; Kelsen, D.; Niedzwiecki, D.; Schuhmacher, C.; et al. Preoperative chemo(radio)therapy versus primary surgery for gastroesophageal adenocarcinoma: Systematic review with meta-analysis combining individual patient and aggregate data. Eur. J. Cancer 2013, 49, 3149–3158. [Google Scholar] [CrossRef]
- Piessen, G.; Messager, M.; Leteurtre, E.; Jean-Pierre, T.; Mariette, C. Signet ring cell histology is an independent predictor of poor prognosis in gastric adenocarcinoma regardless of tumoral clinical presentation. Ann. Surg. 2009, 250, 878–887. [Google Scholar] [CrossRef]
- Al-Batran, S.E.; Homann, N.; Pauligk, C.; Goetze, T.O.; Meiler, J.; Kasper, S.; Kopp, H.G.; Mayer, F.; Haag, G.M.; Luley, K.; et al. Perioperative chemotherapy with fluorouracil plus leucovorin, oxaliplatin, and docetaxel versus fluorouracil or capecitabine plus cisplatin and epirubicin for locally advanced, resectable gastric or gastro-oesophageal junction adenocarcinoma (FLOT4): A randomised, phase 2/3 trial. Lancet 2019, 393, 1948–1957. [Google Scholar] [CrossRef]
- Becker, K.; Mueller, J.D.; Schulmacher, C.; Ott, K.; Fink, U.; Busch, R.; Böttcher, K.; Siewert, J.R.; Höfler, H. Histomorphology and grading of regression in gastric carcinoma treated with neoadjuvant chemotherapy. Cancer 2003, 98, 1521–1530. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Zheng, G.; Zhang, T.; Zhao, Y.; Zheng, Z. Is pathologic tumor regression grade after neo-adjuvant chemotherapy a promising prognostic indicator for patients with locally advanced gastric cancer? A cohort study evaluating tumor regression response. Cancer Chemother. Pharmacol. 2019, 84, 635–646. [Google Scholar] [CrossRef] [PubMed]
- Hass, H.G.; Smith, U.; Jäger, C.; Schäffer, M.; Wellhäuber, U.; Hehr, T.; Markmann, H.U.; Nehls, O.; Denzlinger, C. Signet ring cell carcinoma of the stomach is significantly associated with poor prognosis and diffuse gastric cancer (Lauren’s): Single-center experience of 160 cases. Onkologie 2011, 34, 682–686. [Google Scholar] [CrossRef] [PubMed]
- Mariette, C.; Carneiro, F.; Grabsch, H.I.; van der Post, R.S.; Allum, W.; de Manzoni, G. Correction to: Consensus on the pathological definition and classification of poorly cohesive gastric carcinoma. Gastric Cancer 2019, 22, 421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Becker, K.; Langer, R.; Reim, D.; Novotny, A.; Meyer zum Buschenfelde, C.; Engel, J.; Friess, H.; Hofler, H. Significance of histopathological tumor regression after neoadjuvant chemotherapy in gastric adenocarcinomas: A summary of 480 cases. Ann. Surg. 2011, 253, 934–939. [Google Scholar] [CrossRef] [PubMed]
- Schuhmacher, C.; Gretschel, S.; Lordick, F.; Reichardt, P.; Hohenberger, W.; Eisenberger, C.F.; Haag, C.; Mauer, M.E.; Hasan, B.; Welch, J.; et al. Neoadjuvant chemotherapy compared with surgery alone for locally advanced cancer of the stomach and cardia: European Organisation for Research and Treatment of Cancer randomized trial 40954. J. Clin. Oncol. 2010, 28, 5210–5218. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, J.; van Lanschot, J.J.B.; Hulshof, M.; van Hagen, P.; van Berge Henegouwen, M.I.; Wijnhoven, B.P.L.; van Laarhoven, H.W.M.; Nieuwenhuijzen, G.A.P.; Hospers, G.A.P.; Bonenkamp, J.J.; et al. Neoadjuvant chemoradiotherapy plus surgery versus surgery alone for oesophageal or junctional cancer (CROSS): Long-term results of a randomised controlled trial. Lancet Oncol. 2015, 16, 1090–1098. [Google Scholar] [CrossRef]
- Bang, Y.J.; Kim, Y.W.; Yang, H.K.; Chung, H.C.; Park, Y.K.; Lee, K.H.; Lee, K.W.; Kim, Y.H.; Noh, S.I.; Cho, J.Y.; et al. Adjuvant capecitabine and oxaliplatin for gastric cancer after D2 gastrectomy (CLASSIC): A phase 3 open-label, randomised controlled trial. Lancet 2012, 379, 315–321. [Google Scholar] [CrossRef]
- Japanese gastric cancer treatment guidelines 2014 (ver. 4). Gastric Cancer 2017, 20, 1–19. [CrossRef] [PubMed] [Green Version]
- Sano, T.; Coit, D.G.; Kim, H.H.; Roviello, F.; Kassab, P.; Wittekind, C.; Yamamoto, Y.; Ohashi, Y. Proposal of a new stage grouping of gastric cancer for TNM classification: International Gastric Cancer Association staging project. Gastric Cancer 2017, 20, 217–225. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | n | % |
|---|---|---|
| Gender | ||
| Female | 172 | 24.50 |
| Male | 530 | 75.50 |
| Age (years) * | 58.8+/−11.5 (range 3–83 years) | |
| <70 | 590 | 84.05 |
| >70 | 112 | 15.95 |
| Localization | ||
| Siewert II/III # | 477 | 67.95 |
| Middle | 111 | 15.81 |
| Distal | 88 | 12.54 |
| Total | 26 | 3.70 |
| Clinical Staging $ | ||
| cT2 cN0 | 56 | 7.98 |
| cT1/cT2 cN+ | 57 | 8.12 |
| cT3/cT4 cN0 | 102 | 14.53 |
| cT3/cT4 cN+ | 487 | 69.37 |
| Type of chemotherapy & | ||
| PLF | 351 | 50.00 |
| OLF | 70 | 9.97 |
| Taxol+PLF | 57 | 8.12 |
| ECF/ECX | 64 | 9.12 |
| FLOT | 56 | 7.98 |
| Modified platin based CTx | 104 | 14.81 |
| Type of Surgery | ||
| Esophagectomy | 147 | 20.94 |
| Transhiatal ext. Gastrectomy | 326 | 46.44 |
| Total gastrectomy | 191 | 27.21 |
| Subtotal gastrectomy | 38 | 5.41 |
| Surgical extension | ||
| None | 238 | 33.90 |
| Luminal/transhiatal | 288 | 41.03 |
| Splenectomy | 19 | 2.71 |
| Colon | 5 | 0.71 |
| Pancreas | 18 | 2.56 |
| Others | 134 | 19.09 |
| Dissected LN [Median] | 29 (Range 5–218) | |
| <=25 | 232 | 33.05 |
| >25 | 470 | 66.95 |
| Complications ? | ||
| None | 515 | 73.36 |
| CD I/II | 84 | 11.97 |
| CD III-V | 103 | 14.67 |
| pT ! | ||
| pT0/is | 35 | 4.99 |
| pT1a | 22 | 3.13 |
| pT1b | 50 | 7.12 |
| pT2 | 88 | 12.54 |
| pT3 | 331 | 47.15 |
| pT4a | 148 | 21.08 |
| pT4b | 28 | 3.99 |
| pN ! | ||
| pN0 | 306 | 43.59 |
| pN1 | 130 | 18.52 |
| pN2 | 109 | 15.53 |
| pN3a | 106 | 15.10 |
| pN3b | 51 | 7.26 |
| UICC ! | ||
| UICC 0 | 32 | 4.56 |
| UICC IA | 58 | 8.26 |
| UICC IB | 69 | 9.83 |
| UICC IIA | 126 | 17.95 |
| UICC IIB | 125 | 17.81 |
| UICC IIIA | 97 | 13.82 |
| UICC IIIB | 134 | 19.09 |
| UICC IIIC | 61 | 8.69 |
| Grading | ||
| G1/G2 | 191 | 27.21 |
| G3/G4 | 511 | 72.79 |
| R | ||
| R0 | 615 | 87.61 |
| R1 | 87 | 12.39 |
| Lauren histotype | ||
| Intestinal | 339 | 48.29 |
| Diffuse | 177 | 25.21 |
| Mixed | 92 | 13.11 |
| Not classified | 94 | 13.39 |
| Histopathologic Response | ||
| Becker Ia/Ib | 189 | 26.92 |
| Becker II | 202 | 28.77 |
| Becker III | 311 | 44.30 |
| Univariate | HR | CI95% Lower | CI95% Upper | p |
|---|---|---|---|---|
| Gender ! | 1.19 | 0.92 | 1.53 | 0.190 |
| Age (>70y) | 1.23 | 0.93 | 1.64 | 0.150 |
| Localization § | 1.26 | 0.99 | 1.59 | 0.060 |
| cT2 cN0 $ | 1.00 | 0.032 | ||
| cT3/4 cN0 | 1.65 | 0.99 | 2.74 | 0.050 |
| cT1/2 cN+ | 1.74 | 1.00 | 3.02 | 0.050 |
| cT3/4 cN+ | 1.90 | 1.23 | 2.93 | 0.004 |
| PLF $ | 1.00 | 0.007 | ||
| OLF | 1.20 | 0.83 | 1.72 | 0.335 |
| MAGIC | 0.89 | 0.58 | 1.37 | 0.594 |
| FLOT | 0.39 | 0.16 | 0.96 | 0.040 |
| PLF-Taxol | 0.79 | 0.53 | 1.17 | 0.241 |
| Other | 1.46 | 1.10 | 1.94 | 0.008 |
| Esophagectomy $ | 1.00 | 0.052 | ||
| Extended gastrectomy | 1.17 | 0.88 | 1.56 | 0.274 |
| Gastrectomy | 0.88 | 0.63 | 1.22 | 0.430 |
| Subtotal Gastrectomy | 0.67 | 0.37 | 1.22 | 0.192 |
| Surgical Extension | 1.37 | 1.08 | 1.73 | 0.009 |
| LN dissected (>25/<25) | 1.02 | 0.81 | 1.28 | 0.870 |
| Complication (any) + | 1.21 | 0.96 | 1.53 | 0.110 |
| UICC I $ | 1.00 | 0.000 | ||
| UICC II | 2.74 | 1.87 | 4.01 | 0.000 |
| UICC III | 5.48 | 3.80 | 7.90 | 0.000 |
| G1/2 vs G3/4 | 1.61 | 1.24 | 2.09 | 0.000 |
| R1 vs. R0 | 2.43 | 1.84 | 3.20 | 0.000 |
| Lauren intestinal $ | 1.00 | 0.001 | ||
| Lauren diffuse | 1.51 | 1.18 | 1.93 | 0.001 |
| Lauren mixed | 0.97 | 0.68 | 1.39 | 0.884 |
| Lauren not classified | 0.79 | 0.56 | 1.11 | 0.175 |
| HPR (Y/N) | 0.39 | 0.30 | 0.52 | 0.000 |
| Multivariate | HR | CI95% Lower | CI95% Upper | p |
|---|---|---|---|---|
| Gender ! | 1.22 | 0.93 | 1.60 | 0.154 |
| Age (>70y) | 1.08 | 0.79 | 1.46 | 0.635 |
| Localization § | 1.20 | 0.71 | 2.02 | 0.492 |
| cT2 cN0 $ | 1.00 | 0.550 | ||
| cT3/4 cN0 | 1.29 | 0.76 | 2.20 | 0.354 |
| cT1/2 cN+ | 0.90 | 0.51 | 1.61 | 0.733 |
| cT3/4 cN+ | 1.05 | 0.66 | 1.68 | 0.830 |
| PLF $ | 0.033 | |||
| OLF | 1.01 | 0.69 | 1.47 | 0.980 |
| MAGIC | 0.94 | 0.61 | 1.44 | 0.761 |
| FLOT | 0.53 | 0.21 | 1.29 | 0.161 |
| PLF-Taxol | 0.74 | 0.49 | 1.11 | 0.140 |
| Other | 1.47 | 1.09 | 1.99 | 0.013 |
| Esophagectomy $ | 1.00 | 0.261 | ||
| Extended gastrectomy | 1.17 | 0.87 | 1.57 | 0.298 |
| Gastrectomy | 0.79 | 0.44 | 1.43 | 0.440 |
| Subtotal Gastrectomy | 0.61 | 0.27 | 1.37 | 0.228 |
| Surgical Extension | 1.00 | 0.71 | 1.41 | 0.992 |
| LN dissected (>25/<25) | 0.82 | 0.64 | 1.04 | 0.104 |
| Complication (any) + | 1.17 | 0.91 | 1.49 | 0.222 |
| UICC I $ | 1.00 | 0.000 | ||
| UICC II | 2.07 | 1.35 | 3.16 | 0.001 |
| UICC III | 3.98 | 2.58 | 6.13 | 0.000 |
| G1/2 vs. G3/4 | 1.21 | 0.89 | 1.65 | 0.234 |
| R1 vs. R0 | 1.50 | 1.11 | 2.02 | 0.009 |
| Lauren intestinal $ | 1.00 | 0.002 | ||
| Lauren diffuse | 1.40 | 1.03 | 1.91 | 0.034 |
| Lauren mixed | 0.91 | 0.62 | 1.34 | 0.641 |
| Lauren not classified | 0.66 | 0.45 | 0.96 | 0.031 |
| HPR (Y/N) | 0.71 | 0.51 | 0.99 | 0.045 |
| Variable | NR | % | Responder | % | Total | p |
|---|---|---|---|---|---|---|
| cT2 cN− $ | 25 | 44.6 | 31 | 55.4 | 56 | <0.001 |
| cT3/4 cN− | 68 | 66.7 | 34 | 33.3 | 102 | |
| cT1/2 cN+ | 38 | 66.7 | 19 | 33.3 | 57 | |
| cT3/4 cN+ | 382 | 78.4 | 105 | 21.6 | 487 | |
| Total | 513 | 73.1 | 189 | 26.9 | 702 | |
| PLF& | 263 | 73.9 | 93 | 26.1 | 356 | 0.103 |
| OLF | 58 | 82.9 | 12 | 17.1 | 70 | |
| MAGIC | 49 | 76.6 | 15 | 23.4 | 64 | |
| FLOT | 35 | 62.5 | 21 | 37.5 | 56 | |
| PLF-Taxol | 37 | 64.9 | 20 | 35.1 | 57 | |
| Other | 71 | 71.7 | 28 | 28.3 | 99 | |
| Total | 513 | 73.1 | 189 | 26.9 | 702 | |
| Non-AEG# | 178 | 79.11 | 47 | 20.89 | 225 | |
| AEG | 335 | 70.23 | 142 | 29.77 | 477 | |
| Total | 513 | 73.1 | 189 | 26.9 | 702 | |
| UICC I ! | 45 | 28.30 | 114 | 71.70 | 159 | p < 0.0001 |
| UICC II | 201 | 80.08 | 50 | 19.92 | 251 | |
| UICC III | 267 | 91.44 | 25 | 8.56 | 292 | |
| Total | 513 | 73.1 | 189 | 26.9 | 702 |
| Univariate | OR | CI95% Lower | CI95% Upper | p |
|---|---|---|---|---|
| Localization § | 1.61 | 1.10 | 2.34 | 0.01 |
| Gender ! | 1.53 | 1.02 | 2.32 | 0.04 |
| Age (>70y) | 0.89 | 0.56 | 1.41 | 0.62 |
| cT2 cN0 $ | 1.00 | <0.001 | ||
| cT3/4 cN0 | 0.40 | 0.21 | 0.79 | 0.01 |
| cT1/2 cN+ | 0.40 | 0.19 | 0.86 | 0.02 |
| cT3/4 cN+ | 0.22 | 0.13 | 0.39 | 0.00 |
| Lauren type (intest. vs. other) | 1.77 | 1.14 | 2.46 | 0.01 |
| Grading (G1/2 vs. G3/4) | 0.34 | 0.24 | 0.49 | <0.001 |
| MULTIVARIATE | OR | CI95% lower | CI95% upper | p |
| Localization § | 1.44 | 0.83 | 2.52 | 0.20 |
| Gender ! | 1.70 | 0.92 | 3.13 | 0.09 |
| Age (>70y) | 0.57 | 0.29 | 1.12 | 0.10 |
| cT2 cN0 $ | 1.00 | <0.001 | ||
| cT3/4 cN0 | 0.20 | 0.03 | 1.18 | 0.08 |
| cT1/2 cN+ | 0.58 | 0.08 | 4.24 | 0.59 |
| cT3/4 cN+ | 0.12 | 0.02 | 0.65 | 0.01 |
| Lauren type (intest. vs. other) | 1.30 | 0.75 | 2.22 | 0.35 |
| Grading (G1/2 vs. G3/4) | 0.47 | 0.27 | 0.82 | 0.01 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schirren, R.; Novotny, A.; Friess, H.; Reim, D. Histopathologic Response Is a Positive Predictor of Overall Survival in Patients Undergoing Neoadjuvant/Perioperative Chemotherapy for Locally Advanced Gastric or Gastroesophageal Junction Cancers—Analysis from a Large Single Center Cohort in Germany. Cancers 2020, 12, 2244. https://doi.org/10.3390/cancers12082244
Schirren R, Novotny A, Friess H, Reim D. Histopathologic Response Is a Positive Predictor of Overall Survival in Patients Undergoing Neoadjuvant/Perioperative Chemotherapy for Locally Advanced Gastric or Gastroesophageal Junction Cancers—Analysis from a Large Single Center Cohort in Germany. Cancers. 2020; 12(8):2244. https://doi.org/10.3390/cancers12082244
Chicago/Turabian StyleSchirren, Rebekka, Alexander Novotny, Helmut Friess, and Daniel Reim. 2020. "Histopathologic Response Is a Positive Predictor of Overall Survival in Patients Undergoing Neoadjuvant/Perioperative Chemotherapy for Locally Advanced Gastric or Gastroesophageal Junction Cancers—Analysis from a Large Single Center Cohort in Germany" Cancers 12, no. 8: 2244. https://doi.org/10.3390/cancers12082244
APA StyleSchirren, R., Novotny, A., Friess, H., & Reim, D. (2020). Histopathologic Response Is a Positive Predictor of Overall Survival in Patients Undergoing Neoadjuvant/Perioperative Chemotherapy for Locally Advanced Gastric or Gastroesophageal Junction Cancers—Analysis from a Large Single Center Cohort in Germany. Cancers, 12(8), 2244. https://doi.org/10.3390/cancers12082244