Clinical Course from Diagnosis to Death in Patients with Well-Differentiated Thyroid Cancer


Abstract
:1. Introduction
2. Results
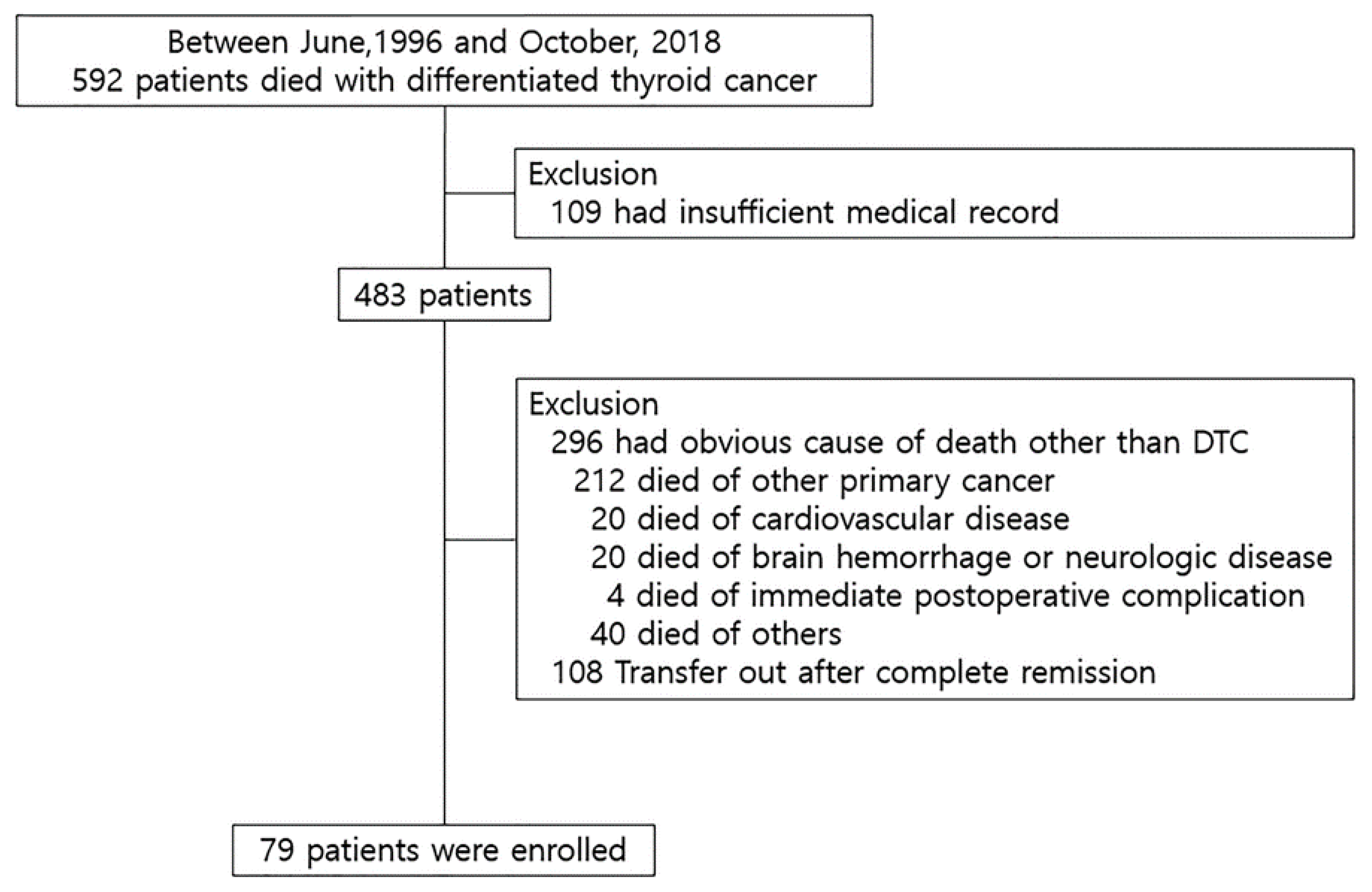
2.1. Causes of Death in 483 Patients Who Died with WDTC
2.2. Clinicopathologic Characteristics of 79 Patients Who Died of WDTC
2.3. Causes of Death of 79 Patients Who Died of WDTC
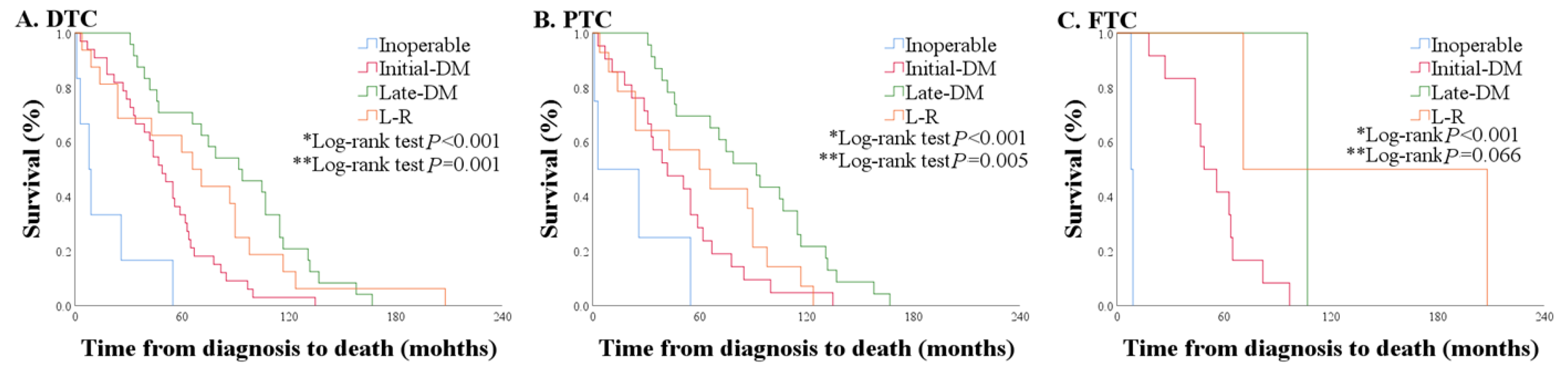
2.4. Overall Survival and Clinical Courses of 79 Patients Who Died of WDTC
2.5. Comparison of PTC with FTC According to Clinical Courses
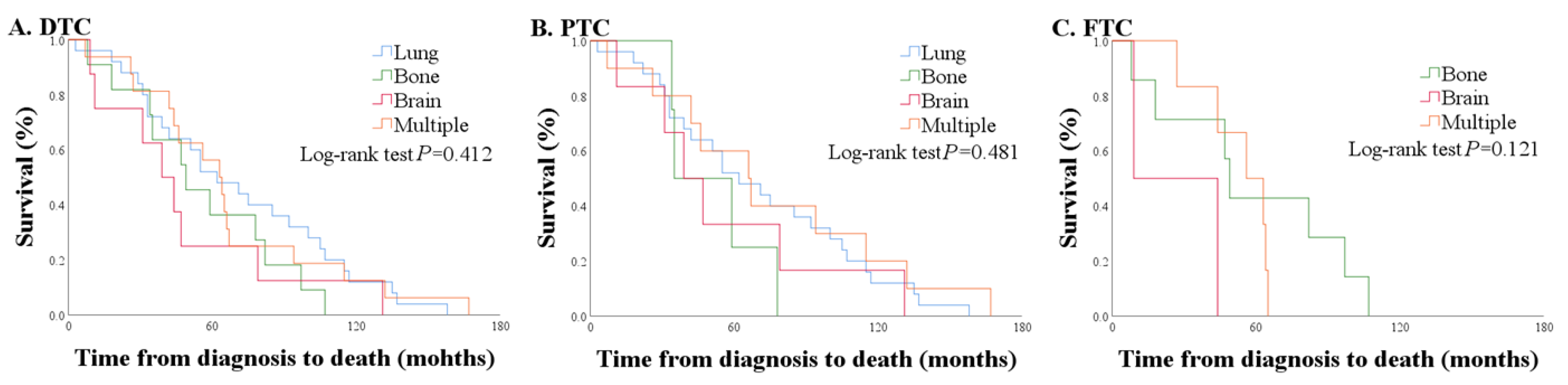
2.6. Comparison of OS According to Distant Metastatic Site
2.7. Comparison of OS According to Time Period
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Treatment and Follow-Up
4.3. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Fagin, J.A.; Wells, S.A., Jr. Biologic and Clinical Perspectives on Thyroid Cancer. N. Engl. J. Med. 2016, 375, 1054–1067. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aschebrook-Kilfoy, B.; Ward, M.H.; Sabra, M.M.; Devesa, S.S. Thyroid cancer incidence patterns in the United States by histologic type, 1992-2006. Thyroid 2011, 21, 125–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davies, L.; Welch, H.G. Current thyroid cancer trends in the United States. JAMA Otolaryngol. Head Neck Surg. 2014, 140, 317–322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahn, H.S.; Kim, H.J.; Welch, H.G. Korea’s thyroid-cancer “epidemic”—Screening and overdiagnosis. N. Engl. J. Med. 2014, 371, 1765–1767. [Google Scholar] [CrossRef] [PubMed]
- Mazzaferri, E.L.; Jhiang, S.M. Long-term impact of initial surgical and medical therapy on papillary and follicular thyroid cancer. Am. J. Med. 1994, 97, 418–428. [Google Scholar] [CrossRef]
- Lin, H.W.; Bhattacharyya, N. Survival impact of treatment options for papillary microcarcinoma of the thyroid. Laryngoscope 2009, 119, 1983–1987. [Google Scholar] [CrossRef]
- Hay, I.D.; Grant, C.S.; Taylor, W.F.; McConahey, W.M. Ipsilateral lobectomy versus bilateral lobar resection in papillary thyroid carcinoma: A retrospective analysis of surgical outcome using a novel prognostic scoring system. Surgery 1987, 102, 1088–1095. [Google Scholar]
- Hay, I.D.; Bergstralh, E.J.; Goellner, J.R.; Ebersold, J.R.; Grant, C.S. Predicting outcome in papillary thyroid carcinoma: Development of a reliable prognostic scoring system in a cohort of 1779 patients surgically treated at one institution during 1940 through 1989. Surgery 1993, 114, 1050–1057; discussion 1057–1058. [Google Scholar]
- Cady, B.; Rossi, R. An expanded view of risk-group definition in differentiated thyroid carcinoma. Surgery 1988, 104, 947–953. [Google Scholar]
- Mazzaferri, E.L.; Kloos, R.T. Clinical review 128: Current approaches to primary therapy for papillary and follicular thyroid cancer. J. Clin. Endocrinol. Metab. 2001, 86, 1447–1463. [Google Scholar] [CrossRef]
- Muresan, M.M.; Olivier, P.; Leclere, J.; Sirveaux, F.; Brunaud, L.; Klein, M.; Zarnegar, R.; Weryha, G. Bone metastases from differentiated thyroid carcinoma. Endocr. Relat. Cancer 2008, 15, 37–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruegemer, J.J.; Hay, I.D.; Bergstralh, E.J.; Ryan, J.J.; Offord, K.P.; Gorman, C.A. Distant metastases in differentiated thyroid carcinoma: A multivariate analysis of prognostic variables. J. Clin. Endocrinol. Metab. 1988, 67, 501–508. [Google Scholar] [CrossRef]
- Nixon, I.J.; Whitcher, M.M.; Palmer, F.L.; Tuttle, R.M.; Shaha, A.R.; Shah, J.P.; Patel, S.G.; Ganly, I. The impact of distant metastases at presentation on prognosis in patients with differentiated carcinoma of the thyroid gland. Thyroid 2012, 22, 884–889. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daniels, G.H. Follicular Thyroid Carcinoma: A Perspective. Thyroid 2018, 28, 1229–1242. [Google Scholar] [CrossRef] [PubMed]
- Fidler, M.M.; Gupta, S.; Soerjomataram, I.; Ferlay, J.; Steliarova-Foucher, E.; Bray, F. Cancer incidence and mortality among young adults aged 20-39 years worldwide in 2012: A population-based study. Lancet Oncol. 2017, 18, 1579–1589. [Google Scholar] [CrossRef] [Green Version]
- Silliphant, W.M.; Klinck, G.H.; Levitin, M.S. Thyroid Carcinoma and Death. A Clinicopathological Study of 193 Autopsies. Cancer 1964, 17, 513–525. [Google Scholar] [CrossRef]
- Tollefsen, H.R.; Decosse, J.J.; Hutter, R.V. Papillary Carcinoma of the Thyroid. A Clinical and Pathological Study of 70 Fatal Cases. Cancer 1964, 17, 1035–1044. [Google Scholar] [CrossRef]
- Silverberg, S.G.; Hutter, R.V.; Foote, F.W., Jr. Fatal carcinoma of the thyroid: Histology, metastases, and causes of death. Cancer 1970, 25, 792–802. [Google Scholar] [CrossRef]
- Kobayashi, T.; Asakawa, H.; Tamaki, Y.; Umeshita, K.; Monden, M. Fatal differentiated thyroid cancer. J. Surg. Oncol. 1996, 62, 123–127. [Google Scholar] [CrossRef]
- Kitamura, Y.; Shimizu, K.; Nagahama, M.; Sugino, K.; Ozaki, O.; Mimura, T.; Ito, K.; Ito, K.; Tanaka, S. Immediate causes of death in thyroid carcinoma: Clinicopathological analysis of 161 fatal cases. J. Clin. Endocrinol. Metab. 1999, 84, 4043–4049. [Google Scholar] [CrossRef]
- Nixon, I.J.; Ganly, I.; Palmer, F.L.; Whitcher, M.M.; Patel, S.G.; Tuttle, R.M.; Shaha, A.R.; Shah, J.P. Disease-related death in patients who were considered free of macroscopic disease after initial treatment of well-differentiated thyroid carcinoma. Thyroid 2011, 21, 501–504. [Google Scholar] [CrossRef] [PubMed]
- Eustatia-Rutten, C.F.; Corssmit, E.P.; Biermasz, N.R.; Pereira, A.M.; Romijn, J.A.; Smit, J.W. Survival and death causes in differentiated thyroid carcinoma. J. Clin. Endocrinol. Metab. 2006, 91, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Beasley, N.J.; Walfish, P.G.; Witterick, I.; Freeman, J.L. Cause of death in patients with well-differentiated thyroid carcinoma. Laryngoscope 2001, 111, 989–991. [Google Scholar] [CrossRef] [PubMed]
- Sugino, K.; Ito, K.; Nagahama, M.; Kitagawa, W.; Shibuya, H.; Ohkuwa, K.; Yano, Y.; Uruno, T.; Akaishi, J.; Kameyama, K.; et al. Prognosis and prognostic factors for distant metastases and tumor mortality in follicular thyroid carcinoma. Thyroid 2011, 21, 751–757. [Google Scholar] [CrossRef]
- Parameswaran, R.; Shulin Hu, J.; Min En, N.; Tan, W.B.; Yuan, N.K. Patterns of metastasis in follicular thyroid carcinoma and the difference between early and delayed presentation. Ann. R. Coll. Surg. Engl. 2017, 99, 151–154. [Google Scholar] [CrossRef] [Green Version]
- Sugitani, I.; Fujimoto, Y.; Yamamoto, N. Papillary thyroid carcinoma with distant metastases: Survival predictors and the importance of local control. Surgery 2008, 143, 35–42. [Google Scholar] [CrossRef]
- McWilliams, R.R.; Giannini, C.; Hay, I.D.; Atkinson, J.L.; Stafford, S.L.; Buckner, J.C. Management of brain metastases from thyroid carcinoma: A study of 16 pathologically confirmed cases over 25 years. Cancer 2003, 98, 356–362. [Google Scholar] [CrossRef]
- Kim, I.Y.; Kondziolka, D.; Niranjan, A.; Flickinger, J.C.; Lunsford, L.D. Gamma knife radiosurgery for metastatic brain tumors from thyroid cancer. J. Neurooncol. 2009, 93, 355–359. [Google Scholar] [CrossRef]
- Chiu, A.C.; Delpassand, E.S.; Sherman, S.I. Prognosis and treatment of brain metastases in thyroid carcinoma. J. Clin. Endocrinol. Metab. 1997, 82, 3637–3642. [Google Scholar] [CrossRef]
- Mihailovic, J.; Stefanovic, L.; Malesevic, M. Differentiated thyroid carcinoma with distant metastases: Probability of survival and its predicting factors. Cancer Biother. Radiopharm. 2007, 22, 250–255. [Google Scholar] [CrossRef]
- Kim, H.; Park, S.Y.; Jung, J.; Kim, J.H.; Hahn, S.Y.; Shin, J.H.; Oh, Y.L.; Chung, M.K.; Kim, H.I.; Kim, S.W.; et al. Improved survival after early detection of asymptomatic distant metastasis in patients with thyroid cancer. Sci. Rep. 2019, 9, 18745. [Google Scholar] [CrossRef]
- Lim, H.; Devesa, S.S.; Sosa, J.A.; Check, D.; Kitahara, C.M. Trends in Thyroid Cancer Incidence and Mortality in the United States, 1974-2013. JAMA 2017, 317, 1338–1348. [Google Scholar] [CrossRef] [PubMed]
- Elisei, R.; Molinaro, E.; Agate, L.; Bottici, V.; Masserini, L.; Ceccarelli, C.; Lippi, F.; Grasso, L.; Basolo, F.; Bevilacqua, G.; et al. Are the clinical and pathological features of differentiated thyroid carcinoma really changed over the last 35 years? Study on 4187 patients from a single Italian institution to answer this question. J. Clin. Endocrinol. Metab. 2010, 95, 1516–1527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, B.Y.; Choi, H.S.; Park, Y.J.; Lim, J.A.; Ahn, H.Y.; Lee, E.K.; Kim, K.W.; Yi, K.H.; Chung, J.K.; Youn, Y.K.; et al. Changes in the clinicopathological characteristics and outcomes of thyroid cancer in Korea over the past four decades. Thyroid 2013, 23, 797–804. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duffy, S.W.; Nagtegaal, I.D.; Wallis, M.; Cafferty, F.H.; Houssami, N.; Warwick, J.; Allgood, P.C.; Kearins, O.; Tappenden, N.; O’Sullivan, E.; et al. Correcting for lead time and length bias in estimating the effect of screen detection on cancer survival. Am. J. Epidemiol. 2008, 168, 98–104. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Causes of Death | n |
|---|---|
| Other primary cancer | 212 |
| Hepatobiliary cancer | 41 |
| Gastrointestinal cancer | 38 |
| Lung cancer | 35 |
| Breast cancer | 26 |
| Hematologic malignancy | 18 |
| Gynecologic cancer | 13 |
| Urogenital cancer | 10 |
| Brain tumor | 9 |
| Head and neck cancer | 8 |
| Other malignancy † | 14 |
| Cardiovascular disease, heart failure | 20 |
| Brain hemorrhage, neurologic disease | 20 |
| Died of postoperative complications | 4 |
| Other disease ‡ | 40 |
| Transfer out after remission (unknown exact cause of death) | 108 |
| Total | 404 |
| Characteristics | Inoperable n (%) | Initial-DM n (%) | Late-DM n (%) | L-R Group n (%) | p-Value (A vs. B vs. C) | |
|---|---|---|---|---|---|---|
| Number of patients | 6 (7.6) | 33 (41.8) | 24 (30.4) | 16 (20.3) | ||
| Sex | Female | 6 (100) | 21 (63.6) | 13 (54.2) | 12 (75) | 0.407 |
| Age | <55 | 1 (16.7) | 9 (27.3) | 3 (12.5) | 3 (18.8) | 0.387 |
| 55 or more | 5 (83.3) | 24 (72.7) | 21 (87.5) | 13 (81.3) | ||
| Primary tumor size † | <4 cm | 3 (50) | 24 (72.7) | 21 (87.5) | 11 (68.8) | 0.298 |
| 4 cm or more | 3 (50) | 9 (27.3) | 3 (12.5) | 5 (31.3) | ||
| pT | 1 | - | 5 (15.2) | 3 (12.5) | 1 (6.3) | 0.445 |
| 2 | - | 4 (12.1) | 1 (4.2) | 4 (25.0) | ||
| 3 | - | 15 (45.5) | 9 (37.5) | 6 (37.5) | ||
| 4 | - | 9 (27.3) | 11 (45.8) | 5 (31.3) | ||
| pN | Not assessed | - | 1 (3.0) | 1 (4.2) | 1 (6.3) | 0.918 |
| N0 | - | 15 (45.5) | 9 (37.5) | 8 (50) | ||
| N1a | - | 4 (12.1) | 5 (20.8) | 3 (18.8) | ||
| N1b | - | 13 (39.4) | 9 (37.5) | 4 (25.0) | ||
| Lymphovascular invasion | Yes | - | 14 (42.4) | 3 (12.5) | 2 (12.5) | 0.015 |
| Resection margin | Positive | - | 9 (27.3) | 9 (37.5) | 2 (12.5) | 0.221 |
| Extent to central LN | Yes | - | 14 (42.4) | 11 (45.8) | 6 (37.5) | 0.872 |
| Extent to lateral LN | Yes | - | 13 (39.4) | 9 (37.5) | 4 (25.0) | 0.598 |
| Extent of surgery | Total | - | 31 (93.9) | 23 (95.8) | 14 (87.5) | 0.576 |
| Less than total | - | 2 (6.1) | 1 (4.2) | 2 (12.5) | ||
| EBRT | Yes | 4 (66.7) | 22 (66.7) | 7 (29.2) | 3 (18.8) | 0.001 |
| Cumulative dose of RAI | 0 | 450 (175–815) | 310 (280–707.5) | 100 (25–207.5) | 0.001 * | |
| Cause of Death | WDTC (n = 79) n (%) | PTC (n = 62) n (%) | FTC (n = 17) n (%) |
|---|---|---|---|
| Respiratory failure | 22 (27.8) | 20 (32.3) | 2 (11.8) |
| Airway obstruction | 19 (24.1) | 19 (30.6) | 0 |
| Complications due to immobilization | 11 (13.9) | 5 (8.1) | 6 (35.3) |
| Brain metastasis | 7 (8.9) | 4 (6.5) | 3 (17.6) |
| Cachexia | 6 (7.6) | 3 (4.8) | 3 (17.6) |
| Liver failure due to hepatic metastasis | 2 (2.5) | 1 (1.6) | 1 (5.9) |
| Unclear | 12 (15.2) | 10 (16.1) | 2 (11.8) |
| Characteristics | PTC (n = 62), n (%) | FTC (n = 17), n (%) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Inoperable | Initial-DM Group | Late-DM Group | L-R Group | p-Value (A vs. B vs. C) | Inoperable | Initial-DM Group | Late-DM Group ‡ | L-R Group ‡ | p-Value (A vs. B vs. C) | ||
| Number of patients | 4 (6.5) | 21 (33.9) | 23 (37.1) | 14 (22.6) | 2 (11.8) | 12 (70.6) | 1 (5.9) | 2 (11.8) | |||
| Sex | Female | 4 (100.0) | 9 (42.9) | 13 (56.5) | 11 (78.6) | 0.112 | 2 (100.0) | 12 (100.0) | 0 | 1 | 0.02 |
| Age | <55 | 1 (25.00) | 6 (28.6) | 3 (13.0) | 2 (14.3) | 0.439 | 0 (0.0) | 3 (25.0) | 0 | 1 | >0.99 |
| 55 or more | 3 (75.0) | 15 (71.4) | 20 (87.0) | 12 (85.7) | 2 (100.0) | 9 (75.0) | 1 | 1 | |||
| Primary tumor size † | <4 cm | 1 (25.00) | 13 (61.9) | 20 (87.0) | 10 (71.4) | 0.160 | 2 (100.0) | 11 (91.7) | 1 | 1 | 0.554 |
| 4 cm or more | 3 (75.0) | 8 (38.1) | 3 (13.0) | 4 (28.6) | 0 (0.0) | 1 (8.3) | 0 | 1 | |||
| pT | 1 | - | 2 (9.5) | 3 (13.0) | 1 (7.1) | 0.371 | - | 3 (25.0) | 0 | 0 | >0.99 |
| 2 | - | 1 (4.8) | 0 (0.0) | 3 (21.4) | - | 3 (25.0) | 1 | 1 | |||
| 3 | - | 11 (52.4) | 9 (39.1) | 5 (35.7) | - | 4 (33.3) | 0 | 1 | |||
| 4 | - | 7 (33.3) | 11 (47.8) | 5 (35.7) | - | 2 (16.7) | 0 | 0 | |||
| pN | Not assessed | - | 0 (0.0) | 1 (4.3) | 1 (7.1) | 0.430 | - | 1 (8.3) | 0 | 0 | >0.99 |
| N0 | - | 4 (19.0) | 8 (34.8) | 6 (42.9) | - | 11 (91.7) | 1 | 2 | |||
| N1a | - | 4 (19.0) | 5 (21.7) | 3 (21.4) | - | 0 | 0 | 0 | |||
| N1b | - | 13 (61.9) | 9 (39.1) | 4 (28.6) | - | 0 | 0 | 0 | |||
| Lymphovascular invasion | Yes | - | 6 (28.6) | 2 (8.7) | 1 (7.1) | 0.177 | - | 8 (66.7) | 1 | 1 | >0.99 |
| Resection margin | Positive | - | 8 (38.1) | 9 (39.1) | 2 (14.3) | 0.239 | - | 1 (8.3) | 0 | 0 | >0.99 |
| Extent to central LN | Yes | - | 14 (66.7) | 11 (47.8) | 6 (42.9) | 0.301 | - | 0 | 0 | 0 | - |
| Extent to lateral LN | Yes | - | 13 (61.9) | 9 (39.1) | 4 (28.6) | 0.118 | - | 0 | 0 | 0 | - |
| Extent of surgery | Total | - | 21 (100.0) | 22 (95.7) | 13 (92.9) | 0.708 | - | 10 (83.3) | 1 | 1 | 0.516 |
| Less than total | - | 0 (0.0) | 1 (4.3) | 1 (7.1) | - | 2 (16.7) | 0 | 1 | |||
| Site of Distant Metastasis | WDTC (n = 60) (n) | PTC (n = 45) (n) | FTC (n = 15) (n) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total (n, %) | Inoperable | Initial-DM Group | Late-DM Group | Total Cases in PTC (n, %) | Inoperable | Initial-DM Group | Late-DM Group | Total Cases in FTC (n, %) | Inoperable | Initial-DM Group | Late-DM Group | |
| Lung | 25 (41.7) | 0 | 14 | 11 | 25 (55.6) | 0 | 14 | 11 | 0 | 0 | 0 | 0 |
| Bone | 11 (18.3) | 1 | 8 | 2 | 4 (8.9) | 0 | 3 | 1 | 7 (46.7) | 1 | 5 | 1 |
| Lung + Bone | 10 (16.7) | 0 | 7 | 3 | 5 (11.1) | 0 | 2 | 3 | 5 (33.3) | 0 | 5 | 0 |
| Brain | 8 (13.3) | 1 | 3 | 4 | 6 (13.3) | 0 | 2 | 4 | 2 (13.3) | 1 | 1 | 0 |
| Bone + Brain | 1 (1.7) | 1 | 0 | 0 | 1 (2.2) | 1 | 0 | 0 | 0 | 0 | 0 | 0 |
| 3 & more organs | 5 (8.3) | 0 | 1 | 4 | 4 (8.9) | 0 | 0 | 4 | 1 (6.7) | 0 | 1 | 0 |
| Total cases | 60 | 3 | 33 | 24 | 45 | 1 | 21 | 23 | 15 | 2 | 12 | 1 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, H.; Park, J.; Park, S.Y.; Kim, T.H.; Kim, S.W.; Chung, J.H. Clinical Course from Diagnosis to Death in Patients with Well-Differentiated Thyroid Cancer. Cancers 2020, 12, 2323. https://doi.org/10.3390/cancers12082323
Park H, Park J, Park SY, Kim TH, Kim SW, Chung JH. Clinical Course from Diagnosis to Death in Patients with Well-Differentiated Thyroid Cancer. Cancers. 2020; 12(8):2323. https://doi.org/10.3390/cancers12082323
Chicago/Turabian StylePark, Hyunju, Jun Park, So Young Park, Tae Hyuk Kim, Sun Wook Kim, and Jae Hoon Chung. 2020. "Clinical Course from Diagnosis to Death in Patients with Well-Differentiated Thyroid Cancer" Cancers 12, no. 8: 2323. https://doi.org/10.3390/cancers12082323
APA StylePark, H., Park, J., Park, S. Y., Kim, T. H., Kim, S. W., & Chung, J. H. (2020). Clinical Course from Diagnosis to Death in Patients with Well-Differentiated Thyroid Cancer. Cancers, 12(8), 2323. https://doi.org/10.3390/cancers12082323