
Trajectories of Cognitive Symptoms in Sick-Listed Cancer Survivors

 and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Sample and Procedure
2.2. Measurements
2.2.1. Sociodemographic Characteristics
2.2.2. Clinical and Treatment-Related Characteristics
2.2.3. Work Disability
2.2.4. Patient-Reported Outcomes
Cognitive Functioning
Fatigue, Depression and Coping
2.3. Statistical Analysis
3. Results
3.1. Sample Characteristics
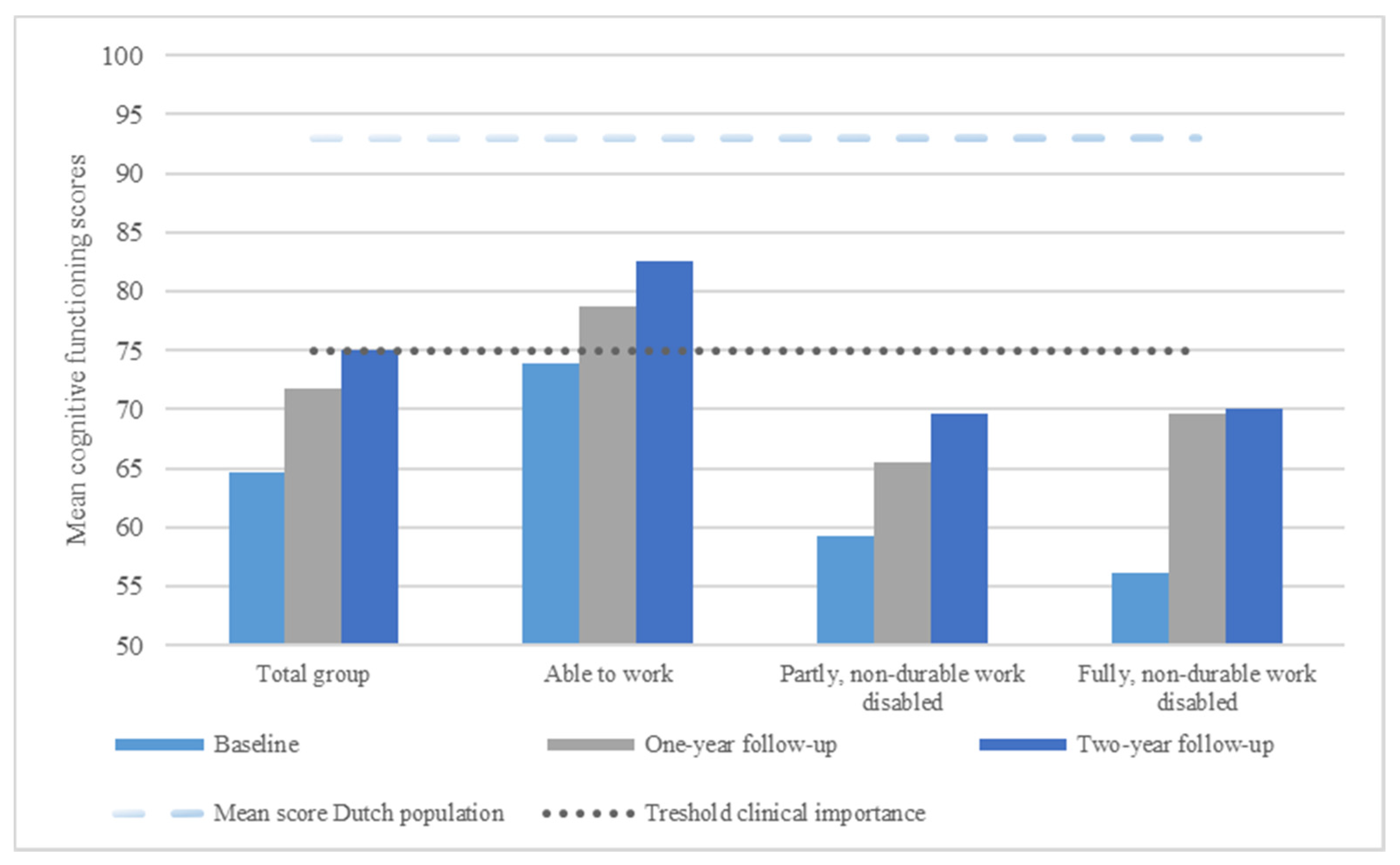
3.2. Trajectory of Cognitive Functioning
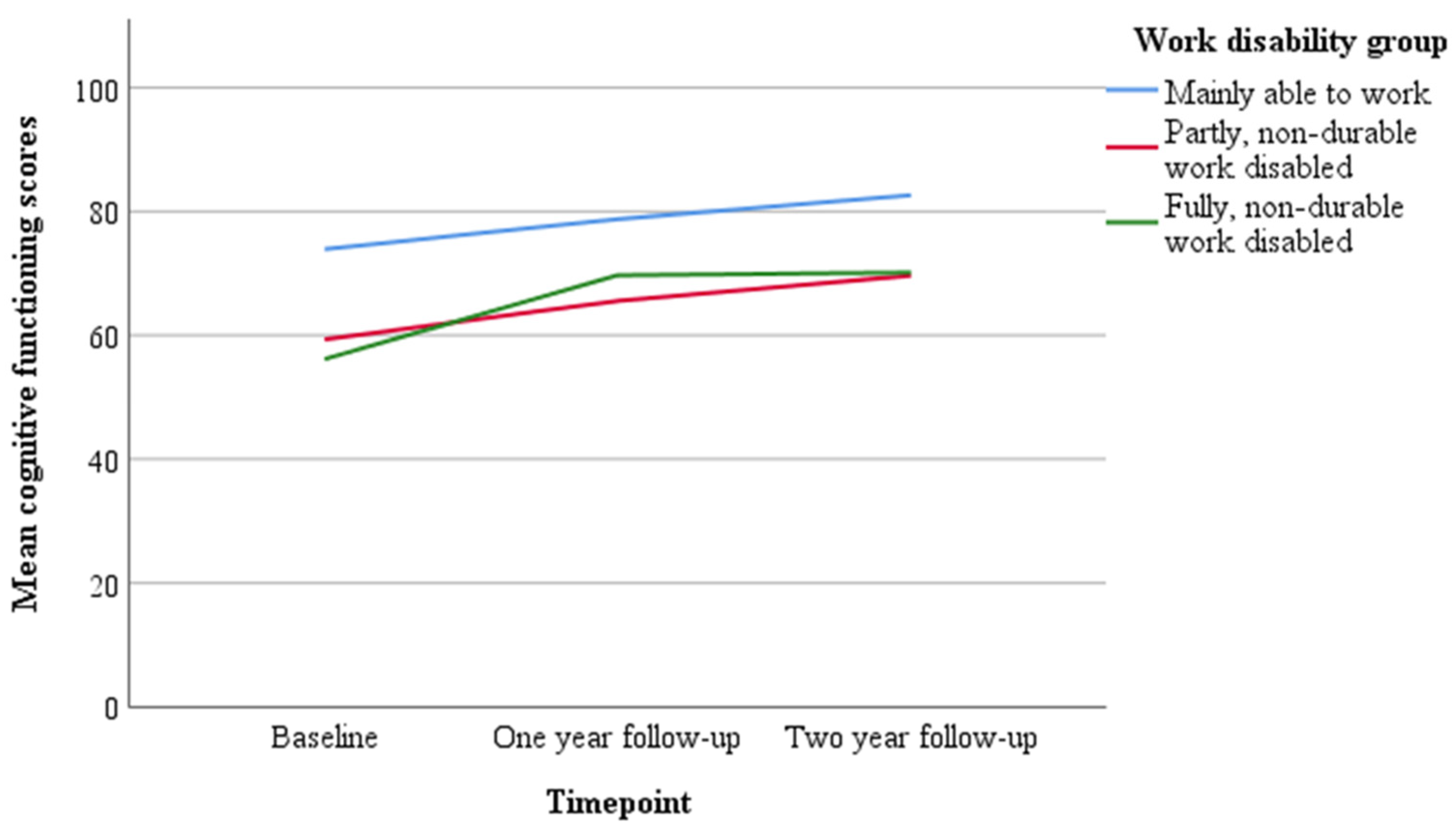
3.3. Level of Work Disability and Trajectories of Cognitive Functioning
3.4. Factors Associated with Trajectories of Cognitive Symptoms
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AIC | Akaike information criterion |
| BIC | Bayesian information criterion |
| CES-D | Center for Epidemiologic Studies Depression Scale |
| CNS | Central nervous system |
| EORTC QLQ | European Organization for Research and Treatment of Cancer—Quality of Life questionnaire |
| ES | Effect Size |
| FACIT-F | Functional Assessment of Chronic Illness Therapy—Fatigue |
| IP | Insurance phycisian |
| RTW | Return to work |
| SD | Standard Deviation |
| SSA | Social Security |
| UCL | Utrecht Coping List |
References
- Torre, L.A.; Siegel, R.L.; Ward, E.M.; Jemal, A. Global Cancer Incidence and Mortality Rates and Trends: An Update. Cancer Epidemiol. Biomarkers Prev. 2015, 25, 16–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Boer, A.G. The European Cancer and Work Network: CANWON. J. Occup. Rehabil. 2014, 24, 393–398. [Google Scholar] [CrossRef] [PubMed]
- Mehnert, A.; de Boer, A.; Feuerstein, M. Employment challenges for cancer survivors. Cancer 2013, 119, 2151–2159. [Google Scholar] [CrossRef] [PubMed]
- Mehnert, A. Employment and work-related issues in cancer survivors. Crit. Rev. Oncol. 2011, 77, 109–130. [Google Scholar] [CrossRef]
- Moran, J.R.; Short, P.F.; Hollenbeak, C.S. Long-term employment effects of surviving cancer. J. Health Econ. 2011, 30, 505–514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Von Ah, D.; Storey, S.; Tallman, E.; Nielsen, A.; Johns, S.A.; Pressler, S.J. Cancer, Cognitive Impairment, and Work-Related Outcomes: An Integrative Review. Oncol. Nurs. Forum 2016, 43, 602–616. [Google Scholar] [CrossRef] [PubMed]
- Von Ah, D.; Storey, S.; Crouch, A. Relationship between self-reported cognitive function and work-related outcomes in breast cancer survivors. J. Cancer Surviv. 2018, 12, 246–255. [Google Scholar] [CrossRef] [PubMed]
- Duijts, S.F.A.; Van Egmond, M.P.; Spelten, E.; Van Muijen, P.; Anema, J.R.; Van Der Beek, A.J. Physical and psychosocial problems in cancer survivors beyond return to work: A systematic review. Psycho-Oncology 2014, 23, 481–492. [Google Scholar] [CrossRef]
- Cheng, A.S.K.; Zeng, Y.; Liu, X.; Liu, S.; Cheng, S.W.C.; Kwok, C.T.T.; Chung, R.C.K.; Xie, J.; Feuerstein, M. Cognitive challenges while at work and work output in breast cancer survivors employed in a rapidly evolving economy. J. Cancer Surviv. 2018, 12, 753–761. [Google Scholar] [CrossRef]
- Bijker, R.; Duijts, S.F.A.; Smith, S.N.; De Wildt-Liesveld, R.; Anema, J.R.; Regeer, B.J. Functional Impairments and Work-Related Outcomes in Breast Cancer Survivors: A Systematic Review. J. Occup. Rehab. 2018, 28, 429–451. [Google Scholar] [CrossRef] [Green Version]
- Boscher, C.; Joly, F.; Clarisse, B.; Humbert, X.; Grellard, J.-M.; Binarelli, G.; Tron, L.; Licaj, I.; Lange, M. Perceived Cognitive Impairment in Breast Cancer Survivors and Its Relationships with Psychological Factors. Cancers 2020, 12, 3000. [Google Scholar] [CrossRef] [PubMed]
- Oberst, K.; Bradley, C.J.; Gardiner, J.C.; Schenk, M.; Given, C.W. Work task disability in employed breast and prostate cancer patients. J. Cancer Surviv. 2010, 4, 322–330. [Google Scholar] [CrossRef] [PubMed]
- Van Muijen, P.; Duijts, S.; Bonefaas-Groenewoud, K.; van der Beek, A.J. Factors associated with work disability in employed cancer survivors at 24-month sick leave. BMC Cancer 2014, 14, 236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Muijen, P.; Duijts, S.F.A.; van der Beek, A.J.; Anema, J.R. Prognostic factors of work disability in sick-listed cancer survivors. J. Cancer Surviv. 2013, 7, 582–591. [Google Scholar] [CrossRef] [PubMed]
- Dorland, H.; Abma, F.; Roelen, C.; Stewart, R.; Amick, B.; Bültmann, U.; Ranchor, A. Work-specific cognitive symptoms and the role of work characteristics, fatigue, and depressive symptoms in cancer patients during 18 months post return to work. Psycho-Oncology 2018, 27, 2229–2236. [Google Scholar] [CrossRef] [PubMed]
- Boelhouwer, I.G.; Vermeer, W.; van Vuuren, T. The associations between late effects of cancer treatment, work ability and job resources: A systematic review. Int. Arch. Occup. Environ. Health 2021, 94, 147–189. [Google Scholar] [CrossRef] [PubMed]
- Vardy, J.L.; Dhillon, H.M. “Mind the gaps”: Cognition and cancer. Psychooncology 2018, 27, 10–12. [Google Scholar] [CrossRef] [PubMed]
- Ahles, T.A.; Root, J.C. Cognitive Effects of Cancer and Cancer Treatments. Annu. Rev. Clin. Psychol. 2018, 14, 425–451. [Google Scholar] [CrossRef]
- Lange, M.; Joly, F.; Vardy, J.; Ahles, T.; Dubois, M.; Tron, L.; Winocur, G.; De Ruiter, M.; Castel, H. Cancer-related cognitive impairment: An update on state of the art, detection, and management strategies in cancer survivors. Ann. Oncol. 2019, 30, 1925–1940. [Google Scholar] [CrossRef] [Green Version]
- Dorland, H.F.; Abma, F.I.; Van Zon, S.K.R.; Stewart, R.E.; Amick, B.C.; Ranchor, A.V.; Roelen, C.A.M.; Bültmann, U. Fatigue and depressive symptoms improve but remain negatively related to work functioning over 18 months after return to work in cancer patients. J. Cancer Surviv. 2018, 12, 371–378. [Google Scholar] [CrossRef] [Green Version]
- Mandelblatt, J.S.; Jacobsen, P.B.; Ahles, T. Cognitive Effects of Cancer Systemic Therapy: Implications for the Care of Older Patients and Survivors. J. Clin. Oncol. 2014, 32, 2617–2626. [Google Scholar] [CrossRef] [Green Version]
- Oh, P.J. Predictors of cognitive decline in people with cancer undergoing chemotherapy. Eur. J. Oncol. Nurs. 2017, 27, 53–59. [Google Scholar] [CrossRef]
- Andreotti, C.; Root, J.C.; Ahles, T.A.; McEwen, B.S.; Compas, B.E. Cancer, coping, and cognition: A model for the role of stress reactivity in cancer-related cognitive decline. Psycho-Oncology 2015, 24, 617–623. [Google Scholar] [CrossRef] [PubMed]
- Reid-Arndt, S.A.; Cox, C.R. Stress, coping and cognitive deficits in women after surgery for breast cancer. J. Clin. Psychol. Med. Settings 2012, 19, 127–137. [Google Scholar] [CrossRef] [PubMed]
- Duijts, S.F.A.; Kieffer, J.M.; Van Muijen, P.; Van Der Beek, A.J. Sustained employability and health-related quality of life in cancer survivors up to four years after diagnosis. Acta Oncol. 2017, 56, 174–182. [Google Scholar] [CrossRef] [Green Version]
- Aaronson, N.K.; Ahmedzai, S.; Bergman, B.; Bullinger, M.; Cull, A.; Duez, N.J.; Filiberti, A.; Flechtner, H.; Fleishman, S.B.; De Haes, J.C.; et al. The European Organization for Research and Treatment of Cancer QLQ-C30: A Quality-of-Life Instrument for Use in International Clinical Trials in Oncology. J. Natl. Cancer Inst. 1993, 85, 365–376. [Google Scholar] [CrossRef] [PubMed]
- Butt, Z.; Lai, J.S.; Rao, D.; Heinemann, A.W.; Bill, A.; Cella, D. Measurement of fatigue in cancer, stroke, and HIV using the Functional Assessment of Chronic Illness Therapy—Fatigue (FACIT-F) scale. J. Psychosom. Res. 2013, 74, 64–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Radloff, L.S. The CES-D scale: A self-report depression scale for research in the general population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Schreurs, P.; van de Willige, G.; Brosschot, J.F.; Tellegen, B.; Graus, G.M.H. Handleiding Utrechtse Coping Lijst UCL (Herziene Versie); Zwets & Zeitlinger: Lisse, The Netherlands, 1993. [Google Scholar]
- Turner, H.; Bryant-Waugh, R.; Peveler, R.; Bucks, R.S. A Psychometric Evaluation of an English Version of the Utrecht Coping List. Eur. Eat. Disord. Rev. 2012, 20, 339–342. [Google Scholar] [CrossRef] [PubMed]
- Shek, D.T.L.; Ma, C.M.S. Longitudinal Data Analyses Using Linear Mixed Models in SPSS: Concepts, Procedures and Illustrations. Sci. World J. 2011, 11, 246739. [Google Scholar] [CrossRef] [Green Version]
- Little, R.J.A. A Test. of Missing Completely at Random for Multivariate Data with Missing Values. J. Am. Stat. Assoc. 1988, 83, 1198–1202. [Google Scholar] [CrossRef]
- Anderson, D.R.; Burnham, K.P.; White, G.C. Comparison of Akaike information criterion and consistent Akaike information criterion for model selection and statistical inference from capture-recapture studies. J. Appl. Stat. 1998, 25, 263–282. [Google Scholar] [CrossRef]
- Schwarz, G. Estimating the Dimension of a Model. Ann. Stat. 1978, 6, 461–464. [Google Scholar] [CrossRef]
- Van de Poll-Franse, L.V.; Mols, F.; Gundy, C.M.; Creutzberg, C.L.; Nout, R.A.; Verdonck-de Leeuw, I.M.; Taphoorn, M.J.; Aaronson, N.K. Normative data for the EORTC QLQ-C30 and EORTC-sexuality items in the general Dutch population. Eur. J. Cancer 2011, 47, 667–675. [Google Scholar] [CrossRef]
- Giesinger, J.M.; Loth, F.L.; Aaronson, N.K.; Arraras, J.I.; Caocci, G.; Efficace, F.; Groenvold, M.; van Leeuwen, M.; Petersen, M.A.; Ramage, J.; et al. Thresholds for clinical importance were established to improve interpretation of the EORTC QLQ-C30 in clinical practice and research. J. Clin. Epidemiol. 2020, 118, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sullivan, G.M.; Feinn, R. Using Effect Size-or Why the P Value Is Not. Enough. J. Grad. Med. Educ. 2012, 4, 279–282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Todd, B.L.; Feuerstein, E.L.; Feuerstein, M. When breast cancer survivors report cognitive problems at work. Int. J. Psychiatry Med. 2011, 42, 279–294. [Google Scholar] [CrossRef]
- George, M.A.; Lustberg, M.B.; Orchard, T.S. Psychoneurological symptom cluster in breast cancer: The role of inflammation and diet. Breast Cancer Res. Treat. 2020, 184, 1–9. [Google Scholar] [CrossRef]
- Lövdén, M.; Brehmer, Y.; Li, S.C.; Lindenberger, U. Training-induced compensation versus magnification of individual differences in memory performance. Front. Hum. Neurosci. 2012, 6, 141. [Google Scholar] [CrossRef] [Green Version]
- Fiszdon, J.M.; Kurtz, M.M.; Parente, L.; Choi, J. What variables predict cognitive remediation associated improvement in individuals with psychosis? Schizophr. Res. Cogn. 2020, 19, 100148. [Google Scholar] [CrossRef] [PubMed]
- McConathey, E.M.; White, N.C.; Gervits, F.; Ash, S.; Coslett, H.B.; Grossman, M.; Hamilton, R.H. Baseline Performance Predicts tDCS-Mediated Improvements in Language Symptoms in Primary Progressive Aphasia. Front. Hum. Neurosci. 2017, 11, 347. [Google Scholar] [CrossRef] [PubMed]
- Cramer, P.; Fraser, G.; Santucci-Silva, R.; Grosicki, S.; Dilhuydy, M.-S.; Janssens, A.; Loscertales, J.; Rule, S.; Goy, A.; Traina, S.; et al. Improvement of fatigue, physical functioning, and well-being among patients with severe impairment at baseline receiving ibrutinib in combination with bendamustine and rituximab for relapsed chronic lymphocytic leukemia/small lymphocytic lymphoma in the HELIOS study. Leuk. Lymphoma 2017, 59, 2075–2084. [Google Scholar] [CrossRef]
- Koutoukidis, D.A.; Land, J.; Hackshaw, A.; Heinrich, M.; McCourt, O.; Beeken, R.J.; Philpott, S.; DeSilva, D.; Rismani, A.; Rabin, N.; et al. Fatigue, quality of life and physical fitness following an exercise intervention in multiple myeloma survivors (MASCOT): An exploratory randomised Phase 2 trial utilising a modified Zelen design. Br. J. Cancer 2020, 123, 187–195. [Google Scholar] [CrossRef] [PubMed]
- Hardy, S.J.; Krull, K.R.; Wefel, J.S.; Janelsins, M. Cognitive Changes in Cancer Survivors. Am. Soc. Clin. Oncol. Educ. Book 2018, 2018, 795–806. [Google Scholar] [CrossRef]
- Janelsins, M.C.; Kesler, S.R.; Ahles, T.A.; Morrow, G.R. Prevalence, mechanisms, and management of cancer-related cognitive impairment. Int. Rev. Psychiatry 2014, 26, 102–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Janelsins, M.C.; Heckler, C.E.; Peppone, L.J.; Kamen, C.; Mustian, K.M.; Mohile, S.G.; Magnuson, A.; Kleckner, I.R.; Guido, J.J.; Young, K.L.; et al. Cognitive Complaints in Survivors of Breast Cancer After Chemotherapy Compared With Age-Matched Controls: An Analysis From a Nationwide, Multicenter, Prospective Longitudinal Study. J. Clin. Oncol. 2017, 35, 506–514. [Google Scholar] [CrossRef] [PubMed]
- Wefel, J.S.; Kesler, S.R.; Noll, K.R.; Schagen, S.B. Clinical characteristics, pathophysiology, and management of noncentral nervous system cancer-related cognitive impairment in adults. CA Cancer J. Clin. 2015, 65, 123–138. [Google Scholar] [CrossRef] [Green Version]
- Klaver, K.M.; Duijts, S.F.A.; Geusgens, C.A.V.; Aarts, M.J.B.; Ponds, R.W.H.M.; Van Der Beek, A.J.; Schagen, S.B. Internet-based cognitive rehabilitation for WORking Cancer survivors (i-WORC): Study protocol of a randomized controlled trial. Trials 2020, 21, 1–12. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Total | |
|---|---|
| N = 206 | |
| Sociodemographic characteristics | |
| Age at T0 (years): mean (SD)/range | 51.0 (6.8)/28–63 |
| Gender, N (%) | |
| Male | 62 (30) |
| Female | 144 (70) |
| Marital status, N (%) | |
| Single | 22 (11) |
| Married | 135 (66) |
| Living with partner | 27 (13) |
| Divorced/widowed | 22 (11) |
| Education, N (%) | |
| None/primary/lower vocational | 47 (20) |
| Secondary school | 29 (14) |
| Vocational education/upper secondary school | 67 (33) |
| Upper vocational education/university | 63 (31) |
| Clinical and treatment-related characteristics at baseline | |
| Cancer type, N (%) | |
| Breast | 104 (51) |
| Digestive—colon | 11 (5) |
| Digestive—other | 13 (6) |
| Head and Neck | 12 (6) |
| Hodgkin lymphoma | 3 (2) |
| Non-Hodgkin lymphoma | 11 (5) |
| Hematologic | 11 (5) |
| Respiratory | 9 (4) |
| Urogenital (female/male) | 20 (10) |
| Urinary tract | 8 (4) |
| Endocrine | 2 (1) |
| Dermatologic | 1 (0.5) |
| Locomotor (bone/sarcoma) | 1 (0.5) |
| Metastasis, N (%) | |
| Lymph node | 78 (38) |
| Distance | 21 (10) |
| None | 104 (51) |
| Time since diagnosis (months): mean (SD)/range | 23.2 (9.4)/15–98 |
| Being free of disease, N (%) | |
| Yes | 108 (52) |
| Don’t know | 56 (27) |
| No | 39 (19) |
| Treatment, N (%) | |
| Surgery | 154 (75) |
| Chemotherapy | 148 (72) |
| Hormonal therapy | 77 (37) |
| Immunotherapy | 20 (10) |
| Radiotherapy | 124 (60) |
| None | 2 (1) |
| Time since completion treatment (months): mean (SD)/range | 13.7 (6.5) 1–49 |
| Ongoing treatment, N (%) | 78 (38) |
| Surgery | 6 (3) |
| Hormonal therapy | 67 (33) |
| Immunotherapy | 4 (2) |
| Stem cell transplant | 1 (0.5) |
| Treatment intensity, N (%) | |
| Local treatment only (surgery and/or radiotherapy) | 30 (16) |
| Systemic treatment (whether or not part of combination therapy) | 173 (84) |
| Work-related characteristics—at time of diagnosis | |
| Sector, N (%) | |
| Education | 21 (10) |
| Business and financial | 21 (10) |
| Industry | 28 (14) |
| Health care | 69 (34) |
| Trade | 17 (8) |
| Public services | 12 (6) |
| Transport | 12 (6) |
| Other | 26 (13) |
| Working hours per week: mean (SD)/range | 31.9 (7.9)/7–48 |
| Full time, N (%) | 141 (68) |
| Shift work, N (%) | |
| Yes | 68 (33) |
| No | 137 (67) |
| Managerial tasks, N (%) | |
| Yes | 45 (22) |
| No | 160 (78) |
| Job tenure, N (%) | |
| ≤10 years | 101 (49) |
| >10 years | 105 (51) |
| Work-related characteristics—at baseline | |
| Work disability, N (%) | |
| <35% | 84 (41) |
| 35–80% | 84 (41) |
| >80% | 38 (18) |
| Total Group | Able to Work | Partly, Non-Durable Work Disabled | Fully, Non-Durable Work Disabled | |||||
|---|---|---|---|---|---|---|---|---|
| N | Mean (SD) * | N | Mean (SD) * | N | Mean (SD) * | N | Mean (SD) * | |
| Baseline | 206 | 64.6 (27.2) | 84 | 73.9 (22.7) | 84 | 59.3 (26.0) | 38 | 56.1 (32.7) |
| One-year follow-up | 180 | 71.7 (26.1) | 73 | 78.7 (23.4) | 74 | 65.5 (25.3) | 33 | 69.7 (30.2) |
| Two-year follow-up | 173 | 75.0 (23.8) | 71 | 82.6 (22.1) | 73 | 69.6 (22.3) | 29 | 70.1 (27.2) |
| CI | |||||||
|---|---|---|---|---|---|---|---|
| Factors | Beta | SE | Df | T | p | Lower Bound | Upper Bound |
| Sociodemographic characteristics | |||||||
| Educational level * | |||||||
| Medium | 2.36 | 5.86 | 198.23 | 0.40 | 0.69 | −9.19 | 13.92 |
| High | 1.97 | 5.80 | 198.96 | 0.34 | 0.74 | −9.47 | 13.40 |
| Treatment-related characteristics | |||||||
| Treatment modality (yes/no) ** | |||||||
| Surgery | 1.52 | 2.13 | 180.52 | 0.71 | 0.48 | −2.69 | 5.73 |
| Chemotherapy | 2.47 | 2.00 | 175.48 | 1.24 | 0.22 | −1.48 | 6.43 |
| Hormonal therapy | 1.32 | 1.87 | 176.54 | 0.70 | 0.48 | −2.38 | 5.01 |
| Immunotherapy | 0.38 | 3.16 | 186.01 | 0.12 | 0.91 | −5.86 | 6.61 |
| Radiotherapy | 1.32 | 1.86 | 177.04 | 0.71 | 0.48 | −2.35 | 4.98 |
| Treatment intensity | |||||||
| Local treatment only (surgery and/or radiotherapy) | −0.94 | 2.53 | 172.22 | −0.37 | 0.71 | −5.94 | 4.07 |
| Systemic treatment (whether or not part of combination therapy) | 0.44 | 2.43 | 171.78 | 0.18 | 0.86 | −4.37 | 5.24 |
| Time since completion treatment | 0.28 | 0.18 | 83.99 | 1.50 | 0.14 | −0.090 | 0.65 |
| Patient-reported outcomes | |||||||
| Fatigue | −0.23 | 0.086 | 178.42 | −2.70 | 0.008 | −0.40 | −0.062 |
| Depression | 0.18 | 0.093 | 186.12 | 1.89 | 0.061 | −0.0082 | 0.36 |
| Coping | |||||||
| active tackling | −0.26 | 0.24 | 179.17 | −1.048 | 0.30 | −0.74 | 0.23 |
| seeking social support | 0.28 | 0.28 | 173.04 | 1.021 | 0.31 | −0.26 | 0.83 |
| palliative reacting | 0.071 | 0.26 | 174.57 | 0.28 | 0.78 | −0.44 | 0.58 |
| avoiding | −0.028 | 0.30 | 178.19 | −0.095 | 0.92 | −0.62 | 0.56 |
| passive reacting | 0.24 | 0.28 | 186.22 | 0.87 | 0.39 | −0.31 | 0.79 |
| reassuring thoughts | 0.49 | 0.33 | 178.64 | 1.50 | 0.14 | −0.16 | 1.14 |
| expression of emotions | 0.89 | 0.62 | 181.75 | 1.44 | 0.15 | −0.34 | 2.12 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Klaver, K.M.; Schagen, S.B.; Kieffer, J.M.; van der Beek, A.J.; Duijts, S.F.A. Trajectories of Cognitive Symptoms in Sick-Listed Cancer Survivors. Cancers 2021, 13, 2444. https://doi.org/10.3390/cancers13102444
Klaver KM, Schagen SB, Kieffer JM, van der Beek AJ, Duijts SFA. Trajectories of Cognitive Symptoms in Sick-Listed Cancer Survivors. Cancers. 2021; 13(10):2444. https://doi.org/10.3390/cancers13102444
Chicago/Turabian StyleKlaver, Kete M., Sanne B. Schagen, Jacobien M. Kieffer, Allard J. van der Beek, and Saskia F. A. Duijts. 2021. "Trajectories of Cognitive Symptoms in Sick-Listed Cancer Survivors" Cancers 13, no. 10: 2444. https://doi.org/10.3390/cancers13102444
APA StyleKlaver, K. M., Schagen, S. B., Kieffer, J. M., van der Beek, A. J., & Duijts, S. F. A. (2021). Trajectories of Cognitive Symptoms in Sick-Listed Cancer Survivors. Cancers, 13(10), 2444. https://doi.org/10.3390/cancers13102444