
The Significance of Prostate Specific Antigen Persistence in Prostate Cancer Risk Groups on Long-Term Oncological Outcomes



Abstract
:Simple Summary
Abstract
1. Introduction
2. Material and Methods
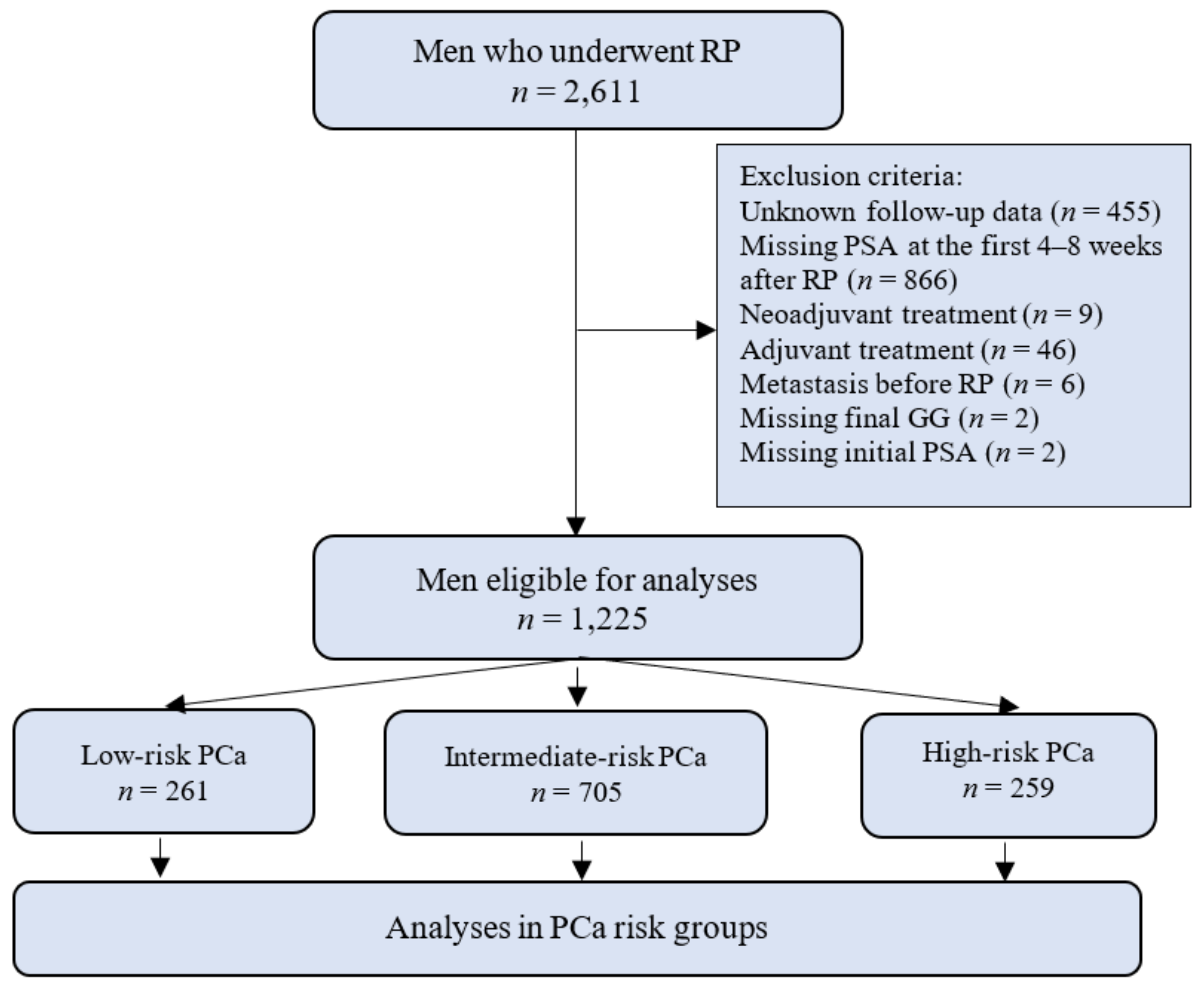
2.1. Patient Population
2.2. Outcomes
2.3. Statistical Analysis
3. Results
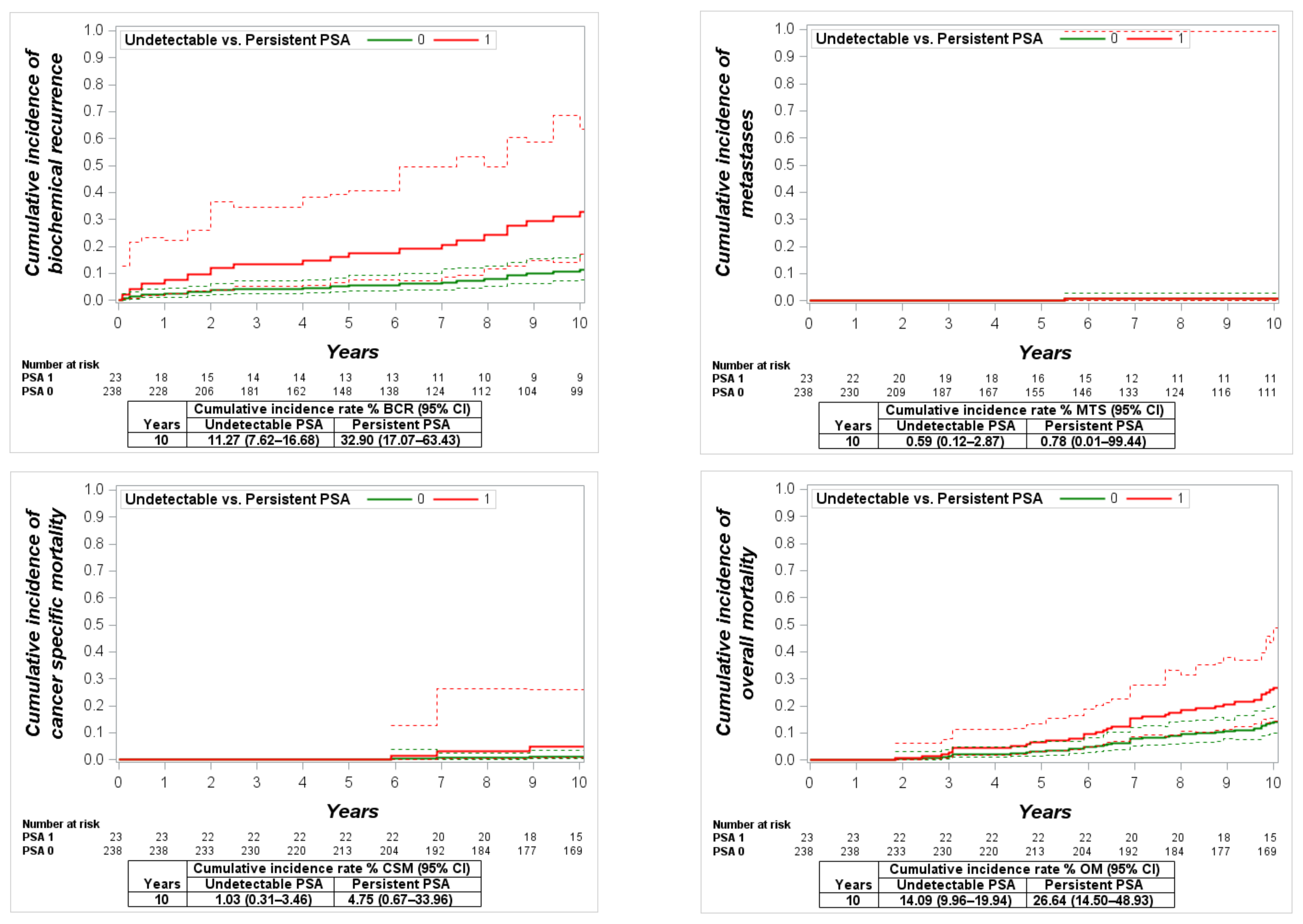
3.1. Outcomes in the Low-Risk Group
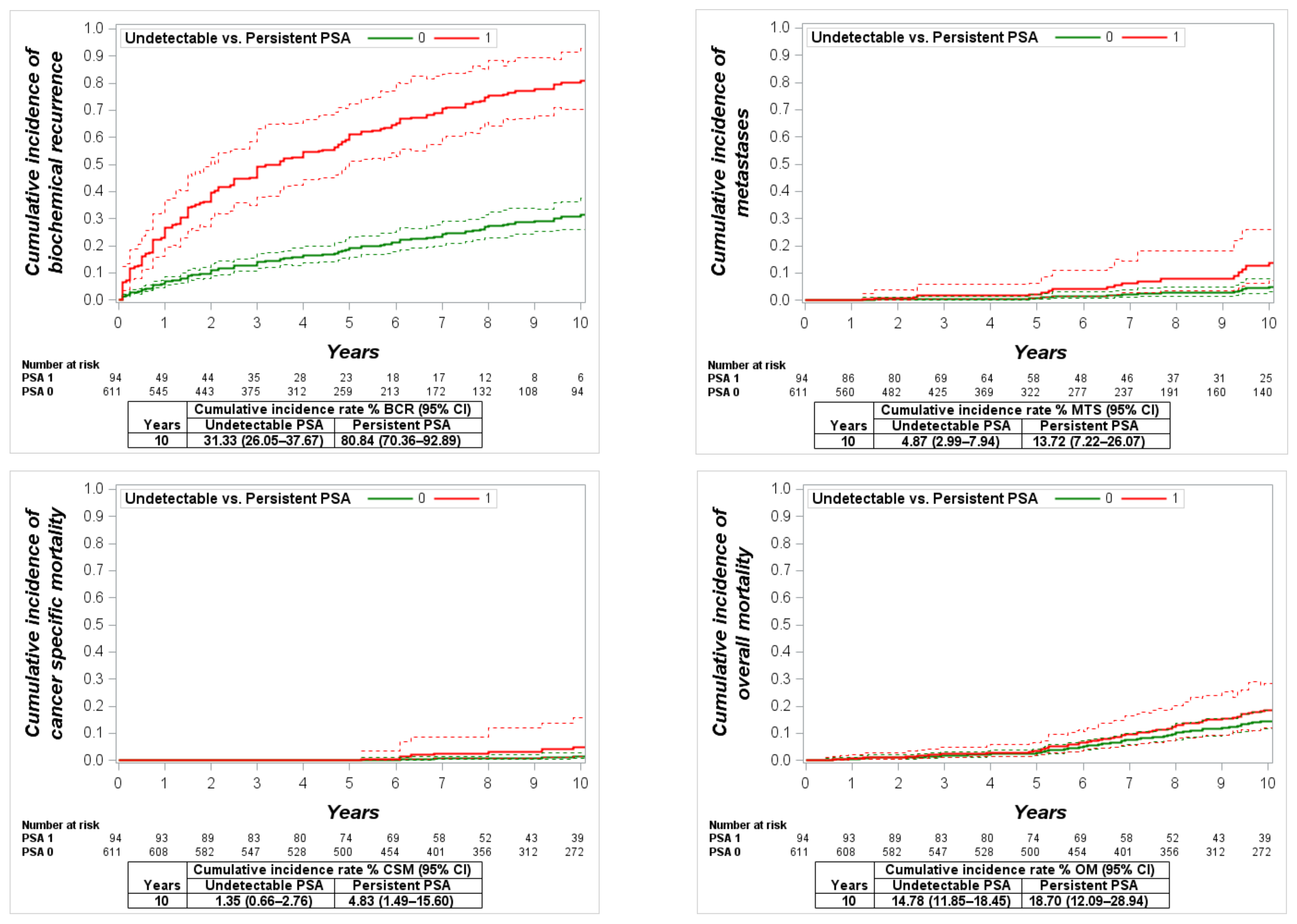
3.2. Outcomes in the Intermediate-Risk Group
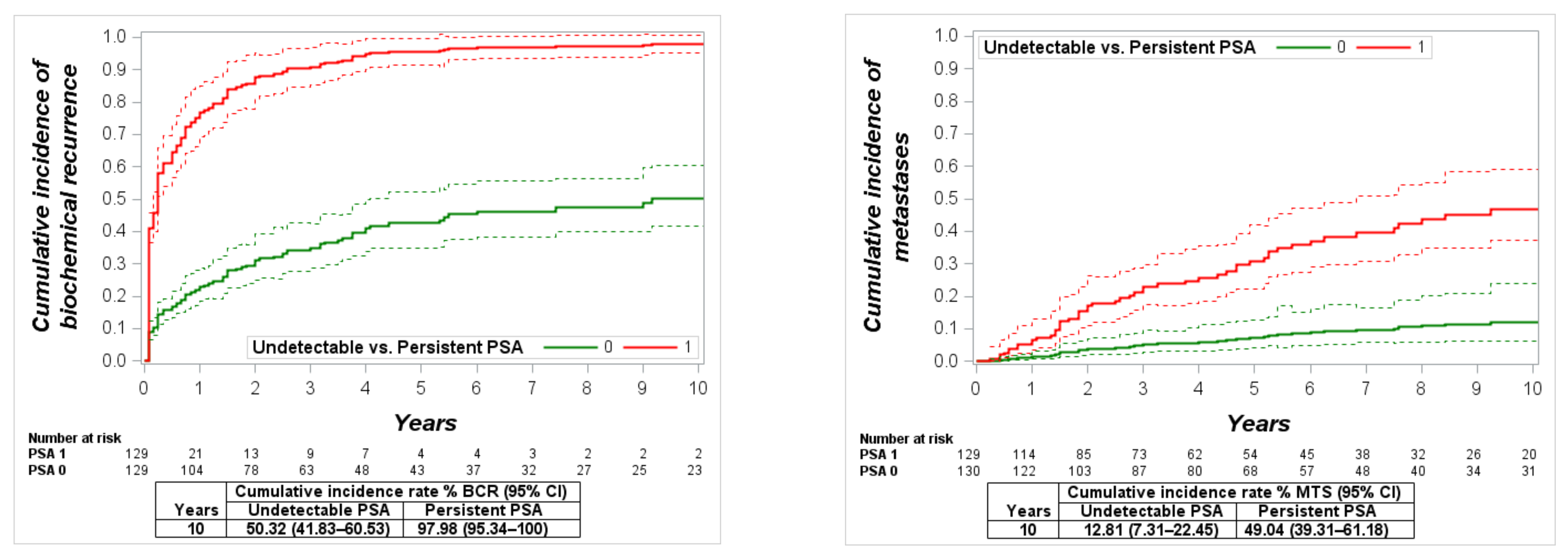
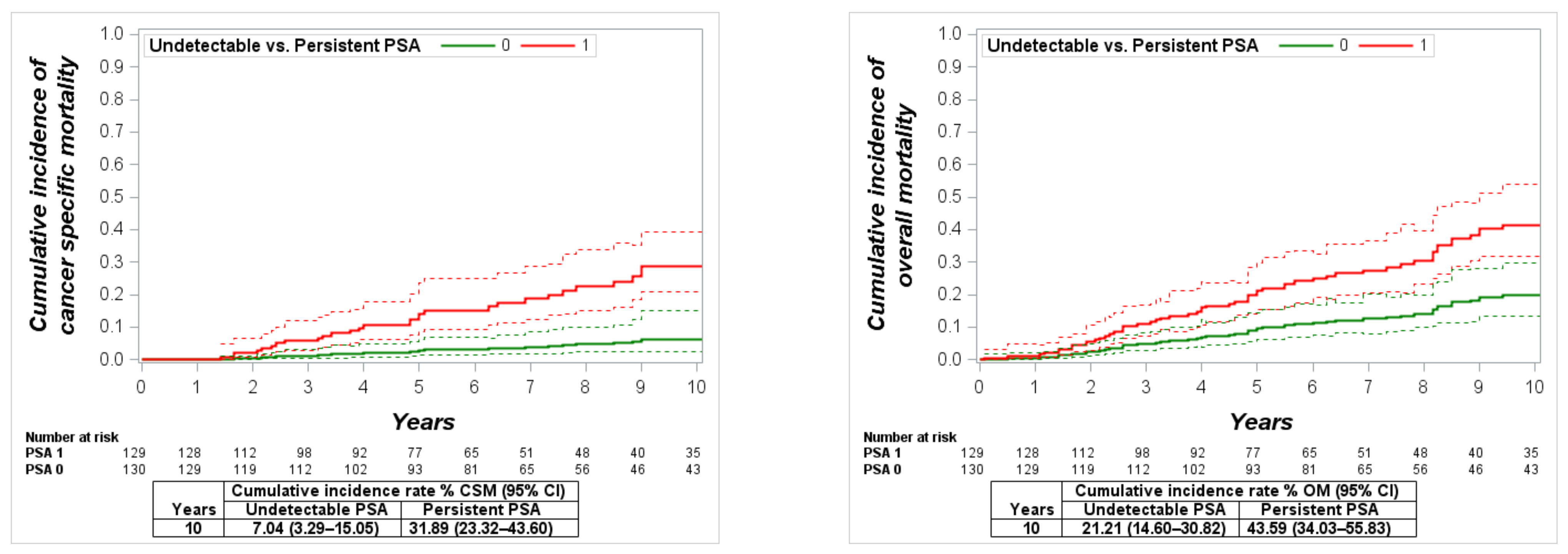
3.3. Outcomes in the High-Risk Group
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Moris, L.; Cumberbatch, M.G.; Van Den Broeck, T.; Gandaglia, G.; Fossati, N.; Kelly, B.; Pal, R.; Briers, E.; Cornford, P.; De Santis, M.; et al. Benefits and Risks of Primary Treatments for High-risk Localized and Locally Advanced Prostate Cancer: An International Multidisciplinary Systematic Review. Eur. Urol. 2020, 77, 614–627. [Google Scholar] [CrossRef]
- Joniau, S.G.; Van Baelen, A.A.; Hsu, C.Y.; Van Poppel, H.P. Complications and functional results of surgery for locally advanced prostate cancer. Adv. Urol. 2012, 2012, 706309. [Google Scholar] [CrossRef]
- Milonas, D.; Baltrimavicius, R.; Grybas, A.; Gudinaviciene, I.; Trumbeckas, D.; Kincius, M.; Auskalnis, S.; Jievaltas, M. Outcome of surgery in locally advanced pT3a prostate cancer. Cent. Eur. J. Urol. 2011, 64, 209–212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mottet, N.; Bellmunt, J.; Bolla, M.; Briers, E.; Cumberbatch, M.G.; De Santis, M.; Fossati, N.; Gross, T.; Henry, A.M.; Joniau, S.; et al. EAU-ESTRO-SIOG Guidelines on Prostate Cancer. Part 1: Screening, Diagnosis, and Local Treatment with Curative Intent. Eur. Urol. 2017, 71, 618–629. [Google Scholar] [CrossRef]
- Preisser, F.; Chun, F.K.H.; Pompe, R.S.; Heinze, A.; Salomon, G.; Graefen, M.; Huland, H.; Tilki, D. Persistent Prostate-Specific Antigen After Radical Prostatectomy and Its Impact on Oncologic Outcomes. Eur. Urol. 2019, 76, 106–114. [Google Scholar] [CrossRef]
- Bianchi, L.; Nini, A.; Bianchi, M.; Gandaglia, G.; Fossati, N.; Suardi, N.; Moschini, M.; Dell’Oglio, P.; Schiavina, R.; Montorsi, F.; et al. The Role of Prostate-specific Antigen Persistence After Radical Prostatectomy for the Prediction of Clinical Progression and Cancer-specific Mortality in Node-positive Prostate Cancer Patients. Eur. Urol. 2016, 69, 1142–1148. [Google Scholar] [CrossRef]
- Kumar, A.; Samavedi, S.; Mouraviev, V.; Bates, A.S.; Coelho, R.F.; Rocco, B.; Patel, V.R. Predictive factors and oncological outcomes of persistently elevated prostate-specific antigen in patients following robot-assisted radical prostatectomy. J. Robot. Surg. 2017, 11, 37–45. [Google Scholar] [CrossRef] [PubMed]
- Bartkowiak, D.; Siegmann, A.; Böhmer, D.; Budach, V.; Wiegel, T. The impact of prostate-specific antigen persistence after radical prostatectomy on the efficacy of salvage radiotherapy in patients with primary N0 prostate cancer. BJU Int. 2019, 124, 785–791. [Google Scholar] [CrossRef] [PubMed]
- Audenet, F.; Seringe, E.; Drouin, S.J.; Comperat, E.; Cussenot, O.; Bitker, M.-O.; Rouprêt, M. Persistently elevated prostate-specific antigen at six weeks after radical prostatectomy helps in early identification of patients who are likely to recur. World J. Urol. 2012, 30, 239–244. [Google Scholar] [CrossRef]
- Wiegel, T.; Bartkowiak, D.; Bottke, D.; Thamm, R.; Hinke, A.; Stockle, M.; Rube, C.; Semjonow, A.; Wirth, M.; Storkel, S.; et al. Prostate-specific antigen persistence after radical prostatectomy as a predictive factor of clinical relapse-free survival and overall survival: 10-year data of the ARO 96-02 trial. Int. J. Radiat. Oncol. Biol. Phys. 2015, 91, 288–294. [Google Scholar] [CrossRef] [PubMed]
- Ploussard, G.; Staerman, F.; Pierrevelcin, J.; Saad, R.; Beauval, J.B.; Roupret, M.; Audenet, F.; Peyromaure, M.; Delongchamps, N.B.; Vincendeau, S.; et al. Predictive factors of oncologic outcomes in patients who do not achieve undetectable prostate specific antigen after radical prostatectomy. J. Urol. 2013, 190, 1750–1756. [Google Scholar] [CrossRef] [PubMed]
- Fossati, N.; Karnes, R.J.; Colicchia, M.; Boorjian, S.A.; Bossi, A.; Seisen, T.; Di Muzio, N.; Cozzarini, C.; Noris Chiorda, B.; Fiorino, C.; et al. Impact of Early Salvage Radiation Therapy in Patients with Persistently Elevated or Rising Prostate-specific Antigen After Radical Prostatectomy. Eur. Urol. 2018, 73, 436–444. [Google Scholar] [CrossRef]
- Gandaglia, G.; Boorjian, S.A.; Parker, W.P.; Zaffuto, E.; Fossati, N.; Bandini, M.; Dell’Oglio, P.; Suardi, N.; Montorsi, F.; Karnes, R.J.; et al. Impact of Postoperative Radiotherapy in Men with Persistently Elevated Prostate-specific Antigen After Radical Prostatectomy for Prostate Cancer: A Long-term Survival Analysis. Eur. Urol. 2017, 72, 910–917. [Google Scholar] [CrossRef] [PubMed]
- Kimura, S.; Urabe, F.; Sasaki, H.; Kimura, T.; Miki, K.; Egawa, S. Prognostic Significance of Prostate-Specific Antigen Persistence after Radical Prostatectomy: A Systematic Review and Meta-Analysis. Cancers 2021, 13, 948. [Google Scholar] [CrossRef]
- Ploussard, G.; Fossati, N.; Wiegel, T.; D’Amico, A.; Hofman, M.S.; Gillessen, S.; Mottet, N.; Joniau, S.; Spratt, D.E. Management of Persistently Elevated Prostate-specific Antigen After Radical Prostatectomy: A Systematic Review of the Literature. Eur. Urol. Oncol. 2021, 4, 150–169. [Google Scholar] [CrossRef]
- Epstein, J.I.; Allsbrook, W.C., Jr.; Amin, M.B.; Egevad, L.L.; Committee, I.G. The 2005 International Society of Urological Pathology (ISUP) Consensus Conference on Gleason Grading of Prostatic Carcinoma. Am. J. Surg. Pathol. 2005, 29, 1228–1242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Epstein, J.I.; Egevad, L.; Amin, M.B.; Delahunt, B.; Srigley, J.R.; Humphrey, P.A.; Grading, C. The 2014 International Society of Urological Pathology (ISUP) Consensus Conference on Gleason Grading of Prostatic Carcinoma: Definition of Grading Patterns and Proposal for a New Grading System. Am. J. Surg. Pathol. 2016, 40, 244–252. [Google Scholar] [CrossRef]
- Van den Broeck, T.; van den Bergh, R.C.N.; Arfi, N.; Gross, T.; Moris, L.; Briers, E.; Cumberbatch, M.; De Santis, M.; Tilki, D.; Fanti, S.; et al. Prognostic Value of Biochemical Recurrence Following Treatment with Curative Intent for Prostate Cancer: A Systematic Review. Eur. Urol. 2019, 75, 967–987. [Google Scholar] [CrossRef] [Green Version]
- Fossati, N.; Karnes, R.J.; Cozzarini, C.; Fiorino, C.; Gandaglia, G.; Joniau, S.; Boorjian, S.A.; Goldner, G.; Hinkelbein, W.; Haustermans, K.; et al. Assessing the Optimal Timing for Early Salvage Radiation Therapy in Patients with Prostate-specific Antigen Rise After Radical Prostatectomy. Eur. Urol. 2016, 69, 728–733. [Google Scholar] [CrossRef]
- Joniau, S.; Briganti, A.; Gontero, P.; Gandaglia, G.; Tosco, L.; Fieuws, S.; Tombal, B.; Marchioro, G.; Walz, J.; Kneitz, B.; et al. Stratification of high-risk prostate cancer into prognostic categories: A European multi-institutional study. Eur. Urol. 2015, 67, 157–164. [Google Scholar] [CrossRef]
- Moris, L.; Devos, G.; Van den Broeck, T.; Milonas, D.; Maarten, M.; Berghen, C.; Meerleer, G.; Devlies, W.; Everaerts, W.; Gevaert, T.; et al. Current and emerging therapies for localized high-risk prostate cancer. Expert Rev. Anticancer Ther. 2020, 21, 267–282. [Google Scholar] [CrossRef] [PubMed]
- Bryant, A.K.; D’Amico, A.V.; Nguyen, P.L.; Einck, J.P.; Kane, C.J.; McKay, R.R.; Simpson, D.R.; Mundt, A.J.; Murphy, J.D.; Rose, B.S. Three-month posttreatment prostate-specific antigen level as a biomarker of treatment response in patients with intermediate-risk or high-risk prostate cancer treated with androgen deprivation therapy and radiotherapy. Cancer 2018, 124, 2939–2947. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | All n = 1225 | Low-Risk n = 261 | Intermediate-Risk n = 705 | High-Risk n = 259 | p-Value |
|---|---|---|---|---|---|
| Age (years): median (IQR) | 64 (59–68) | 63.5 (59–68) | 63 (58–68) | 65 (60–69) | 0.01 |
| PSA (ng/mL): median (IQR) | 6.5 (4.8–9.95) | 55 (4.3–6.9) | 6.3 (4.8–9.6) | 10.8 (6.2–21.1) | <0.0001 |
| Clinical stage: n, (%) | <0.0001 | ||||
| cT1 | 337 (27.5) | 106 (40.6) | 197 (27.9) | 34 (13.1) | |
| cT2 | 706 (57.6) | 144 (55.2) | 428 (60.7) | 134 (51.7) | |
| cT3 | 178 (14.5) | 11 (4.2) | 76 (10.8) | 91 (35.1) | |
| Unknown | 4 (0.3) | - | 4 (0.6) | - | |
| Biopsy Gleason score: n, (%) | <0.0001 | ||||
| 6 | 710 (58) | 249 (95.4) | 394 (55.9) | 67 (25.9) | |
| 3 + 4 | 363 (29.6) | 11 (4.2) | 270 (38.3) | 82 (31.7) | |
| 4 + 3 | 53 (4.3) | 1 (0.4) | 22 (3.2) | 30 (11.6) | |
| 8 | 64 (5.2) | - | 16 (2.3) | 48 (18.5) | |
| 9–10 | 33 (2.7) | - | 1 (0.1) | 32 (12.4) | |
| Unknown | 2 (0.2) | - | 2 (0.2) | - | |
| Pathological Gleason Score: n, (%) | <0.0001 | ||||
| 6 | 329 (26.9) | 261 (100) | 58 (8.2) | 10 (3.9) | |
| 3 + 4 | 626 (51.1) | - | 569 (80.7) | 57 (22) | |
| 4 + 3 | 113 (9.2) | - | 78 (11.1) | 35 (13.5) | |
| 8 | 70 (5.7) | - | - | 70 (27.0) | |
| 9–10 | 87 (7.1) | - | - | 87 (33.6) | |
| Pathologic stage: n, (%) | <0.0001 | ||||
| pT2 | 776 (63.3) | 261 (100) | 459 (65.1) | 56 (21.6) | |
| pT3a | 326 (26.6) | - | 246 (34.9) | 80 (30.9) | |
| pT3b-pT4 | 123 (10) | - | - | 123 (47.5) | |
| Positive surgical margin: n, (%) | 399 (33.7) | 41 (16.1) | 221 (32.2) | 137 (56.1) | <0.0001 |
| PLND: n, (%) | 489 (39.9) | 61 (23.4) | 228 (32.3) | 200 (77.2) | <0.0001 |
| LNI: n, (%) | 65 (13.3) | - | - | 65 (32.5) | <0.0001 |
| Persistent PSA | 246 (20.1) | 23 (8.8) | 94 (13.3) | 129 (49.8) | <0.0001 |
| BCR: n, (%) | 383 (31.3) | 27 (10.3) | 179 (25.4) | 177 (68.3) | <0.0001 |
| MTS: n, (%) | 87 (7.1) | 4 (1.5) | 24 (3.4) | 59 (22.8) | <0.0001 |
| Death: n, (%) | 226 (18.4) | 46 (17.6) | 113 (16) | 67 (25.9) | <0.0001 |
| Cancer related death: n, (%) | 45 (3.8) | 3 (1.1) | 11 (1.6) | 33 (12.7) | <0.0001 |
| Parameter | BCR | MTS | OM | CSM | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| HR | 95% CI | p | HR | 95% CI | p | HR | 95% CI | p | HR | 95% CI | p | |
| PSA (ng/mL) | 1.1 | 1–1.02 | 0.05 | 0.9 | 0.97–1.01 | 0.3 | 0.9 | 0.97–1.02 | 0.6 | 0.9 | 0.92–1.01 | 0.08 |
| Age (years) | 1.1 | 0.99–1.04 | 0.2 | 1.1 | 0.97–1.06 | 0.6 | 1.1 | 1.04–1.12 | <0.001 | 1.1 | 1.0–1.14 | 0.04 |
| PSA persistence | 4.2 | 3.06–5.76 | <0.001 | 2.7 | 1.44–5.09 | 0.002 | 1.8 | 1.13–2.76 | 0.01 | 5.5 | 2.08–14.49 | 0.006 |
| Stage: | ||||||||||||
| pT2 | Ref. | Ref. | Ref. | Ref. | ||||||||
| pT3a | 1.7 | 1.19–2.55 | 0.004 | 0.7 | 0.33–1.54 | 0.4 | 0.8 | 0.48–1.44 | 0.5 | 0.7 | 0.21–2.38 | 0.6 |
| pT3b-pT4 | 2.3 | 1.48–3.59 | 0.0002 | 1.4 | 0.62–2.97 | 0.5 | 1.7 | 0.89–3.07 | 0.1 | 2.5 | 0.84–7.4 | 0.09 |
| Grade Group: | ||||||||||||
| GG 1 | Ref. | Ref. | Ref. | Ref. | ||||||||
| GG 2 | 1.8 | 1.11–3.08 | 0.018 | 3 | 0.82–11.09 | 0.09 | 1.1 | 0.58–1.75 | 0.9 | 1.2 | 0.29–5.4 | 0.8 |
| GG 3 | 3.6 | 1.99–6.43 | <0.001 | 10.6 | 2.71–41.42 | 0.0007 | 1.1 | 0.43–2.59 | 0.9 | 0.9 | 0.09–9.98 | 0.9 |
| GG 4 | 2.7 | 1.45–5.03 | 0.002 | 8.1 | 1.93–33.81 | 0.004 | 0.9 | 0.39–2.18 | 0.9 | 3.2 | 0.69–14.94 | 0.1 |
| GG 5 | 3.6 | 1.99–6.44 | <0.001 | 31.9 | 8.08–126.2 | <0.0001 | 2.9 | 1.39–6.03 | 0.005 | 5.8 | 1.29–25.7 | 0.02 |
| LNI | 2.1 | 1.37–3.22 | 0.0006 | 1.4 | 0.75–2.78 | 0.3 | 1.3 | 0.67–2.57 | 0.4 | 2 | 0.83–5.01 | 0.1 |
| SM | 1.7 | 1.22–2.25 | 0.0013 | 1.8 | 0.96–3.2 | 0.07 | 1.3 | 0.84–2.04 | 0.2 | 2.2 | 0.89–5.45 | 0.09 |
| BCR | MTS | OM | CSM | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Parameter | HR | 95% CI | p | HR | 95% CI | p | HR | 95% CI | p | HR | 95% CI | p |
| Low Risk Group * | ||||||||||||
| PSA (ng/mL) | 0.94 | 0.65–1.37 | 0.7 | 14.6 | 0.11− | 0.2 | 1.3 | 0.88–1.9 | 0.1 | 0.9 | 0.33–2.23 | 0.7 |
| Age (years) | 1.1 | 0.97–1.26 | 0.1 | 1.1 | 0.62–1.65 | 0.9 | 1.1 | 0.95–1.18 | 0.2 | 0.8 | 0.6–1.18 | 0.3 |
| Persistent PSA | 3.9 | 0.79–19.84 | 0.09 | 21.4 | 0.1− | 0.5 | 2.3 | 0.6–8.84 | 0.2 | 3.9 | <0.0001− | 0.9 |
| SM | 10.1 | 2.05–49.68 | 0.004 | <0.1 | <0.0001− | 0.9 | 2.1 | 0.48–9.19 | 0.3 | 2.3 | <0.0001− | 0.9 |
| Intermediate Risk Group ** | ||||||||||||
| PSA (ng/mL) | 1.1 | 0.99–1.11 | 0.1 | 0.96 | 0.82–1.1 | 0.6 | 0.9 | 0.91–1.07 | 0.8 | 1.2 | 0.95–1.51 | 0.1 |
| Age (years) | 1.1 | 0.99–1.06 | 0.2 | 1.1 | 0.94–1.14 | 0.5 | 1.1 | 1.05–1.19 | 0.002 | 1.2 | 0.93–1.61 | 0.2 |
| Persistent PSA | 3.8 | 2.16–6.77 | <0.0001 | 2.6 | 0.74–9.4 | 0.1 | 1.1 | 0.42–2.5 | 0.9 | 4.2 | 0.48–36.11 | 0.2 |
| Stage | ||||||||||||
| pT2 | Ref. | Ref. | Ref. | Ref. | ||||||||
| pT3a | 1.6 | 0.98–2.64 | 0.06 | 1.7 | 0.49–5.8 | 0.4 | 0.8 | 0.38–1.47 | 0.4 | 2.8 | 0.26–31.19 | 0.4 |
| Grade Group | ||||||||||||
| GG 1 | Ref. | Ref. | Ref. | Ref. | ||||||||
| GG 2 | 0.73–3.07 | 0.3 | 1 | <0.0001− | 0.9 | 0.8 | 0.38–1.73 | 0.6 | 1 | <0.0001− | 0.9 | |
| GG 3 | 2.3 | 0.98–5.6 | 0.06 | 1 | <0.0001− | 0.9 | 0.9 | 0.26–3.79 | 0.9 | 2.1 | <0.0001− | 0.9 |
| SM | 2.9 | 1.75–4.88 | <0.0001 | 3.9 | 1.04–14.5 | 0.04 | 1.8 | 0.93–3.39 | 0.08 | 1.3 | 0.15–11.87 | 0.8 |
| High Risk Group *** | ||||||||||||
| PSA (ng/mL) | 1.1 | 0.99–1.02 | 0.5 | 0.9 | 0.97–1.01 | 0.5 | 0.9 | 0.96–1.02 | 0.4 | 0.9 | 0.91–1.01 | 0.08 |
| Age (years) | 1.1 | 0.98–1.03 | 0.8 | 1.1 | 0.96–1.06 | 0.7 | 1.1 | 1.01–1.12 | 0.015 | 1.1 | 0.99–1.15 | 0.09 |
| Persistent PSA | 5.1 | 3.31–7.99 | <0.0001 | 2.6 | 1.2–5.62 | 0.015 | 2.7 | 1.36–5.45 | 0.005 | 6.2 | 1.66–23.06 | 0.007 |
| Stage | ||||||||||||
| pT2 | Ref. | Ref. | Ref. | Ref. | ||||||||
| pT3a | 1.8 | 0.95–3.39 | 0.07 | 0.5 | 0.17–1.32 | 0.2 | 0.9 | 0.33–2.41 | 0.8 | 0.3 | 0.05–1.75 | 0.2 |
| pT3b–pT4 | 2.3 | 1.2–4.24 | 0.01 | 1.1 | 0.42–2.55 | 0.9 | 2 | 0.83–4.83 | 0.1 | 1.9 | 0.56–6.6 | 0.3 |
| Grade Group | ||||||||||||
| GG 1 | Ref. | Ref. | Ref. | Ref. | ||||||||
| GG 2 | 4.1 | 0.92–18.23 | 0.06 | 1.6 | 0.18–15.09 | 0.7 | 0.8 | 0.19–2.99 | 0.7 | 0.7 | 0.06–9.04 | 0.8 |
| GG 3 | 8.7 | 1.87–40.14 | 0.006 | 4.8 | 0.53–44.01 | 0.2 | 0.9 | 0.18–4.37 | 0.9 | 1.6 | 0.08–33.07 | 0.8 |
| GG 4 | 5 | 1.12–22.02 | 0.035 | 3.9 | 0.43–35.07 | 0.2 | 0.8 | 0.2–3.21 | 0.8 | 2.7 | 0.25–30.59 | 0.4 |
| GG 5 | 6.7 | 1.53–29.19 | 0.01 | 14.3 | 1.65–123.4 | 0.016 | 2.7 | 0.6–8.6 | 0.2 | 5.7 | 0.56–58.19 | 0.1 |
| LNI | 1.8 | 1.2–2.78 | 0.005 | 1.4 | 0.74–2.8 | 0.3 | 1.1 | 0.56–2.29 | 0.7 | 2.1 | 0.81–5.39 | 0.1 |
| SM | 1.1 | 0.77–1.65 | 0.5 | 1.6 | 0.8–3.35 | 0.2 | 0.8 | 0.4–1.48 | 0.4 | 1.9 | 0.66–5.77 | 0.2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Milonas, D.; Venclovas, Z.; Sasnauskas, G.; Ruzgas, T. The Significance of Prostate Specific Antigen Persistence in Prostate Cancer Risk Groups on Long-Term Oncological Outcomes. Cancers 2021, 13, 2453. https://doi.org/10.3390/cancers13102453
Milonas D, Venclovas Z, Sasnauskas G, Ruzgas T. The Significance of Prostate Specific Antigen Persistence in Prostate Cancer Risk Groups on Long-Term Oncological Outcomes. Cancers. 2021; 13(10):2453. https://doi.org/10.3390/cancers13102453
Chicago/Turabian StyleMilonas, Daimantas, Zilvinas Venclovas, Gustas Sasnauskas, and Tomas Ruzgas. 2021. "The Significance of Prostate Specific Antigen Persistence in Prostate Cancer Risk Groups on Long-Term Oncological Outcomes" Cancers 13, no. 10: 2453. https://doi.org/10.3390/cancers13102453
APA StyleMilonas, D., Venclovas, Z., Sasnauskas, G., & Ruzgas, T. (2021). The Significance of Prostate Specific Antigen Persistence in Prostate Cancer Risk Groups on Long-Term Oncological Outcomes. Cancers, 13(10), 2453. https://doi.org/10.3390/cancers13102453