
Methods and Designs of Modern Breast Cancer Confirmatory Trials

 , , , ,
, , , , 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
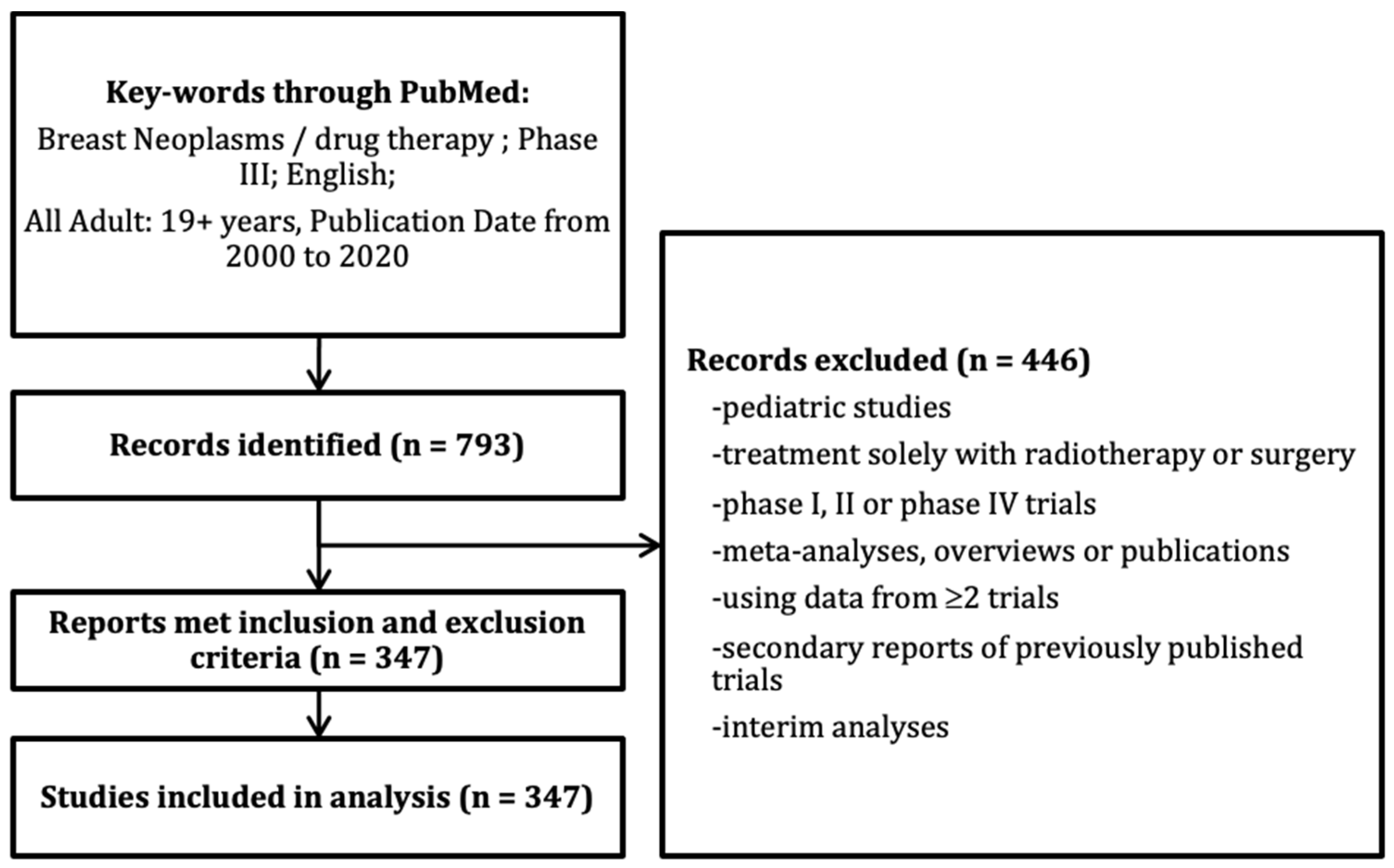
2.1. Study Selection
2.2. Definition of Trial Characteristics
2.3. Statistical Analysis
3. Results
3.1. Characteristics of Selected RCTs
3.2. Trial Designs
3.3. Statistical Analysis Procedures
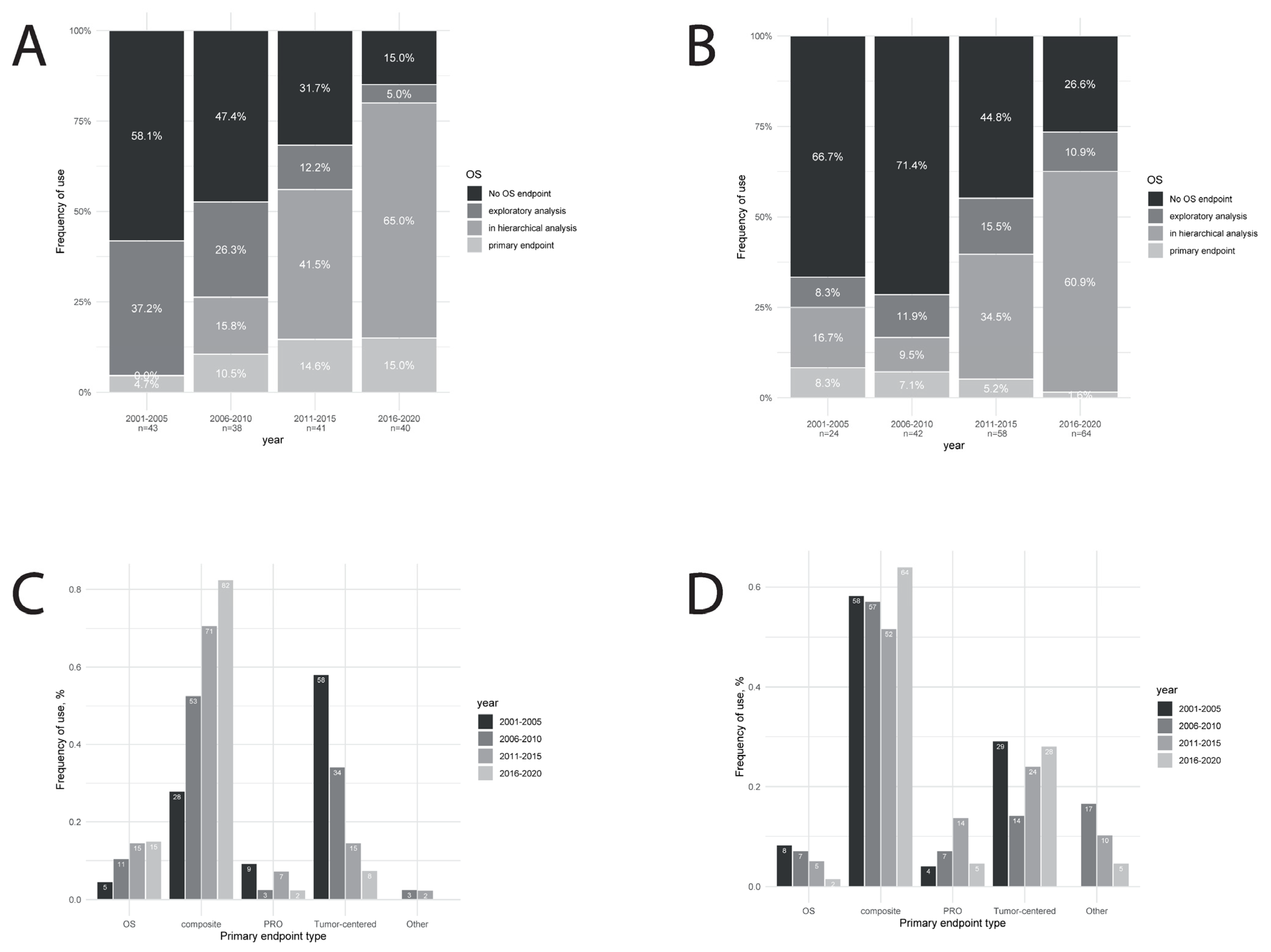
3.4. Trial Endpoints
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- US Food and Drug Administration Clinical Trial Endpoints for the Approval of Cancer Drugs and Biologics Guidance for Industry. 2018. Available online: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/clinical-trial-endpoints-approval-cancer-drugs-and-biologics (accessed on 25 May 2021).
- Committee for Medicinal Products for Human Use Reflection Paper on the Regulatory Guidance for the Use of Health-Related Quality of Life Measures in the Evaluation of Medicinal Products. 2005. Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/reflection-paper-regulatory-guidance-use-healthrelated-quality-life-hrql-measures-evaluation_en.pdf (accessed on 25 May 2021).
- French Transparency Committee Transparency Committee Doctrine Principles of Medicinal Product Assessments and Appraisal for Reimbursement Purposes. 2021. Available online: https://www.has-sante.fr/upload/docs/application/pdf/2019-07/doctrine_de_la_commission_de_la_transparence_-version_anglaise.pdf (accessed on 25 May 2021).
- Davis, C.; Naci, H.; Gurpinar, E.; Poplavska, E.; Pinto, A.; Aggarwal, A. Availability of evidence of benefits on overall survival and quality of life of cancer drugs approved by European Medicines Agency: Retrospective cohort study of drug approvals 2009-13. BMJ 2017, 359, j4530. [Google Scholar] [CrossRef] [Green Version]
- Salas-Vega, S.; Iliopoulos, O.; Mossialos, E. Assessment of Overall Survival, Quality of Life, and Safety Benefits Associated with New Cancer Medicines. JAMA Oncol. 2017, 3, 382. [Google Scholar] [CrossRef] [Green Version]
- Davis, C. Drugs, cancer and end-of-life care: A case study of pharmaceuticalization? Soc. Sci. Med. 2015, 131, 207–214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Booth, C.M.; Del Paggio, J.C. Approvals in 2016: Questioning the clinical benefit of anticancer therapies. Nat. Rev. Clin. Oncol. 2017, 14, 135–136. [Google Scholar] [CrossRef] [PubMed]
- Naci, H.; Cylus, J.; Vandoros, S.; Sato, A.; Perampaladas, K. Raising the bar for market authorisation of new drugs. BMJ 2012, 345, e4261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- U.S. Food and Drugs Administration. Patient-Reported Outcome Measures: Guidance for Industry Use in Medical Product Development to Support Labeling Claims Guidance for Industry. 2009. Available online: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/patient-reported-outcome-measures-use-medical-product-development-support-labeling-claims (accessed on 25 May 2021).
- European Medical Agency Statistical Principles for Clinical Trials. 1998. Available online: https://www.ema.europa.eu/en/ich-e9-statistical-principles-clinical-trials (accessed on 25 May 2021).
- Lawrence, N.J.; Roncolato, F.; Martin, A.; Simes, R.J.; Stockler, M.R. Effect Sizes Hypothesized and Observed in Contemporary Phase III Trials of Targeted and Immunological Therapies for Advanced Cancer. JNCI Cancer Spectr. 2018, 2. [Google Scholar] [CrossRef]
- MacEwan, J.P.; Doctor, J.; Mulligan, K.; May, S.G.; Batt, K.; Zacker, C.; Lakdawalla, D.; Goldman, D. The Value of Progression-Free Survival in Metastatic Breast Cancer: Results from a Survey of Patients and Providers. MDM Policy Pract. 2019, 4. [Google Scholar] [CrossRef]
- Saad, E.D.; Squifflet, P.; Burzykowski, T.; Quinaux, E.; Delaloge, S.; Mavroudis, D.; Perez, E.; Piccart-Gebhart, M.; Schneider, B.P.; Slamon, D.; et al. Disease-free survival as a surrogate for overall survival in patients with HER2-positive, early breast cancer in trials of adjuvant trastuzumab for up to 1 year: A systematic review and meta-analysis. Lancet Oncol. 2019, 20, 361–370. [Google Scholar] [CrossRef]
- Michiels, S.; Pugliano, L.; Marguet, S.; Grun, D.; Barinoff, J.; Cameron, D.; Cobleigh, M.; Di Leo, A.; Johnston, S.; Gasparini, G.; et al. Progression-free survival as surrogate end point for overall survival in clinical trials of HER2-targeted agents in HER2-positive metastatic breast cancer. Ann. Oncol. 2016, 27, 1029–1034. [Google Scholar] [CrossRef]
- Gyawali, B.; Hey, S.P.; Kesselheim, A.S. Evaluating the evidence behind the surrogate measures included in the FDA’s table of surrogate endpoints as supporting approval of cancer drugs. EClinicalMedicine 2020, 21, 100332. [Google Scholar] [CrossRef]
- Fiteni, F.; Bonnetain, F. Surrogate end points for overall survival in breast cancer trials: A review. Breast 2016, 29, 44–48. [Google Scholar] [CrossRef] [PubMed]
- Saad, E.D.; Katz, A.; Buyse, M. Overall survival and post-progression survival in advanced breast cancer: A review of recent randomized clinical trials. J. Clin. Oncol. 2010, 28, 1958–1962. [Google Scholar] [CrossRef] [PubMed]
- Slamon, D.J.; Neven, P.; Chia, S.; Fasching, P.A.; De Laurentiis, M.; Im, S.-A.; Petrakova, K.; Bianchi, G.V.; Esteva, F.J.; Martín, M.; et al. Overall Survival with Ribociclib plus Fulvestrant in Advanced Breast Cancer. N. Engl. J. Med. 2020, 382, 514–524. [Google Scholar] [CrossRef]
- Sledge, G.W.; Toi, M.; Neven, P.; Sohn, J.; Inoue, K.; Pivot, X.; Burdaeva, O.; Okera, M.; Masuda, N.; Kaufman, P.A.; et al. The Effect of Abemaciclib Plus Fulvestrant on Overall Survival in Hormone Receptor–Positive, ERBB2-Negative Breast Cancer That Progressed on Endocrine Therapy—MONARCH 2. JAMA Oncol. 2020, 6, 116. [Google Scholar] [CrossRef] [PubMed]
- Burzykowski, T.; Buyse, M.; Piccart-Gebhart, M.J.; Sledge, G.; Carmichael, J.; Lück, H.-J.; Mackey, J.R.; Nabholtz, J.-M.; Paridaens, R.; Biganzoli, L.; et al. Evaluation of tumor response, disease control, progression-free survival, and time to progression as potential surrogate end points in metastatic breast cancer. J. Clin. Oncol. 2008, 26, 1987–1992. [Google Scholar] [CrossRef] [PubMed]
- Chen, E.Y.; Raghunathan, V.; Prasad, V. An Overview of Cancer Drugs Approved by the US Food and Drug Administration Based on the Surrogate End Point of Response Rate. JAMA Intern. Med. 2019, 179, 915–921. [Google Scholar] [CrossRef]
- Gyawali, B.; Hey, S.P.; Kesselheim, A.S. Assessment of the Clinical Benefit of Cancer Drugs Receiving Accelerated Approval. JAMA Intern. Med. 2019, 179, 906. [Google Scholar] [CrossRef]
- Carpenter, D.; Kesselheim, A.S.; Joffe, S. Reputation and Precedent in the Bevacizumab Decision. N. Engl. J. Med. 2011, 365, e3. [Google Scholar] [CrossRef] [Green Version]
- Bottomley, A.; Reijneveld, J.C.; Koller, M.; Flechtner, H.; Tomaszewski, K.A.; Greimel, E.; Ganz, P.A.; Ringash, J.; O’Connor, D.; Kluetz, P.G.; et al. Current state of quality of life and patient-reported outcomes research. Eur. J. Cancer 2019, 121, 55–63. [Google Scholar] [CrossRef] [Green Version]
- Food and Drugs Administration. Value and Use of Patient-Reported Outcomes (PROs) in Assessing Effects of Medical Devices. 2016. Available online: https://www.fda.gov/files/about%20fda/published/Value-and-Use-of-Patient-Reported-Outcomes-%28PROs%29-in-Assessing-Effects-of-Medical-Devices.pdf (accessed on 25 May 2021).
- Sparano, J.A.; Gray, R.J.; Makower, D.F.; Pritchard, K.I.; Albain, K.S.; Hayes, D.F.; Geyer, C.E.; Dees, E.C.; Perez, E.A.; Olson, J.A.; et al. Prospective Validation of a 21-Gene Expression Assay in Breast Cancer. N. Engl. J. Med. 2015, 373, 2005–2014. [Google Scholar] [CrossRef]
- Tolaney, S.M.; Barry, W.T.; Dang, C.T.; Yardley, D.A.; Moy, B.; Marcom, P.K.; Albain, K.S.; Rugo, H.S.; Ellis, M.; Shapira, I.; et al. Adjuvant Paclitaxel and Trastuzumab for Node-Negative, HER2-Positive Breast Cancer. N. Engl. J. Med. 2015, 372, 134–141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piccart, M.J.; Hilbers, F.S.; Bliss, J.M.; Caballero, C.; Frank, E.S.; Renault, P.; Naït Kaoudjt, R.; Schumacher, E.; Spears, P.A.; Regan, M.M.; et al. Road Map to Safe and Well-Designed De-escalation Trials of Systemic Adjuvant Therapy for Solid Tumors. J. Clin. Oncol. 2020, 38, 4120–4129. [Google Scholar] [CrossRef] [PubMed]
- Péron, J.; Pond, G.R.; Gan, H.K.; Chen, E.X.; Almufti, R.; Maillet, D.; You, B. Quality of reporting of modern randomized controlled trials in medical oncology: A systematic review. J. Natl. Cancer Inst. 2012, 104. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Study Characteristics | Studies | ||
|---|---|---|---|
| n | % | ||
| Year of publication | 2001–2005 | 67 | 19 |
| 2006–2010 | 80 | 23 | |
| 2011–2015 | 96 | 28 | |
| 2016–2020 | 104 | 30 | |
| Tumor setting | Localized | 184 | 53 |
| Advanced or metastatic | 158 | 46 | |
| Both | 5 | 1 | |
| Sources of trial funding (NA = 7) | Government/Foundation | 81 | 24 |
| Funded by industry | 259 | 76 | |
| Journal | Journal of Clinical Oncology | 134 | 39 |
| Annals of Oncology | 41 | 18 | |
| New England Journal of Medicine | 32 | 9 | |
| Lancet/Lancet Oncol | 58 | 17 | |
| European Journal of Cancer | 19 | 6 | |
| Other journals | 63 | 18 | |
| Regions in which RCTs were led | North America | 95 | 27 |
| Europe | 200 | 57 | |
| Asia | 27 | 8 | |
| Other | 25 | 7 | |
| Investigational therapy | Cytotoxic chemotherapy | 155 | 45 |
| Hormonal therapy | 59 | 17 | |
| Molecular targeted therapy | 96 | 28 | |
| Immunotherapy | 2 | 1 | |
| Other | 35 | 10 | |
| Study Characteristics | 2001–2005, n = 67 | 2006–2010, n = 80 | 2011–2015, n = 96 | 2016–2020, n = 104 | P |
|---|---|---|---|---|---|
| Non-inferiority design | 13 (20%) | 2 (3%) | 9 (10%) | 16 (16%) | 0.96 |
| Population of interest | <0.0001 | ||||
| All BCs | 52 (79%) | 56 (70%) | 50 (52%) | 28 (27%) | |
| Large intrinsic subgroup | 14 (21%) | 24 (30%) | 45 (47%) | 72 (69%) | |
| Narrower biologically defined subgroup | 0 (0%) | 0 (0%) | 1 (1%) | 4 (4%) | |
| Inclusion period length in months, median (IQR) | 37 (25–49) | 37 (29–56) | 39 (29–60) | 32 (21–51) | 0.27 |
| Sample size, median (IQR) | 375 (258–600) | 532 (250–1027) | 602 (299–1157) | 682 (461–1534) | <0.0001 |
| >2 treatment groups | 2 (3%) | 9 (11%) | 7 (7%) | 6 (6%) | 0.91 |
| Coprimary endpoint (type-1 error split) | 2 (3%) | 3 (4%) | 7 (7%) | 7 (7%) | 0.54 |
| Hierarchical analysis | 6 (9%) | 22 (28%) | 44 (46%) | 74 (71%) | <0.0001 |
| Other analysis population | 0 (0%) | 6 (2%) | 6 (2%) | 7 (2%) | 0.097 |
| Other endpoint except OS | 2 (3%) | 6 (8%) | 12 (13%) | 26 (25%) | 0.00012 |
| OS endpoint | 4 (6%) | 10 (13%) | 37 (39%) | 66 (63%) | <0.0001 |
| Metastatic Trials (n = 162) | |||||
|---|---|---|---|---|---|
| Study Characteristics | 2001–2005, n = 43 | 2006–2010, n = 38 | 2011–2015, n = 41 | 2016–2020, n = 40 | P |
| Control arm | 0.47 | ||||
| Active treatment +/−placebo | 38 (88%) | 37 (97%) | 37 (90%) | 34 (85%) | |
| Placebo+BSC/observation | 3 (7%) | 0 | 2 (5%) | 5 (13%) | |
| BSC/observation | 2 (5%) | 1 (3%) | 2 (5%) | 1 (3%) | |
| Treatment line | 0.94 | ||||
| 1st only | 27 (63%) | 24 (63%) | 22 (54%) | 23 (58%) | |
| 1st and more | 9 (21%) | 7 (18%) | 9 (22%) | 8 (20%) | |
| 2nd and more | 6 (14%) | 5 (13%) | 9 (22%) | 6 (15%) | |
| 3rd and more | 1 (2%) | 2 (5%) | 1 (2%) | 3 (8%) | |
| Early breast cancer trials (n = 188) | |||||
| Study characteristics | 2001–2005, n = 24 | 2006–2010, n = 42 | 2011–2015, n = 58 | 2016–2020, n = 64 | P |
| Control arm | 0.098 | ||||
| Active treatment +/−placebo | 22 (82%) | 31 (74%) | 46 (79%) | 50 (78%) | |
| Placebo+BSC/observation | 2 (8%) | 9 (21%) | 4 (7%) | 6 (9%) | |
| BSC/observation | 0 (0%) | 2 (5%) | 8 (14%) | 8 (13%) | |
| Experimental treatment duration vs. standard | 0.14 | ||||
| Shorter | |||||
| Same | 4 (17%) | 3 (8%) | 2 (4%) | 12 (19%) | |
| Longer | 12 (52%) | 20 (51%) | 35 (65%) | 33 (53%) | |
| 7 (30%) | 16 (41%) | 17 (32%) | 17 (27%) | ||
| Experimental strategy | 0.45 | ||||
| Addition of a new drug to standard | 11 (46%) | 20 (48%) | 30 (52%) | 28 (44%) | |
| Replacement of a standard drug | 9 (38%) | 19 (45%) | 16 (28%) | 26 (41%) | |
| No new drug | 4 (17%) | 3 (7%) | 10 (21%) | 10 (16%) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Péron, J.; Reverdy, T.; Smenteck, C.; Cortet, M.; You, B.; Freyer, G. Methods and Designs of Modern Breast Cancer Confirmatory Trials. Cancers 2021, 13, 2757. https://doi.org/10.3390/cancers13112757
Péron J, Reverdy T, Smenteck C, Cortet M, You B, Freyer G. Methods and Designs of Modern Breast Cancer Confirmatory Trials. Cancers. 2021; 13(11):2757. https://doi.org/10.3390/cancers13112757
Chicago/Turabian StylePéron, Julien, Thibaut Reverdy, Colette Smenteck, Marion Cortet, Benoît You, and Gilles Freyer. 2021. "Methods and Designs of Modern Breast Cancer Confirmatory Trials" Cancers 13, no. 11: 2757. https://doi.org/10.3390/cancers13112757
APA StylePéron, J., Reverdy, T., Smenteck, C., Cortet, M., You, B., & Freyer, G. (2021). Methods and Designs of Modern Breast Cancer Confirmatory Trials. Cancers, 13(11), 2757. https://doi.org/10.3390/cancers13112757