
Development of a Metastatic Uveal Melanoma Prognostic Score (MUMPS) for Use in Patients Receiving Immune Checkpoint Inhibitors

 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
1.1. Study Design
1.2. Study Population
1.3. Data Collection and Treatment Outcomes
1.4. Data Analysis and Statistics
2. Results
2.1. Patient Characteristics
2.2. ICI Treatment Duration and Toxicity
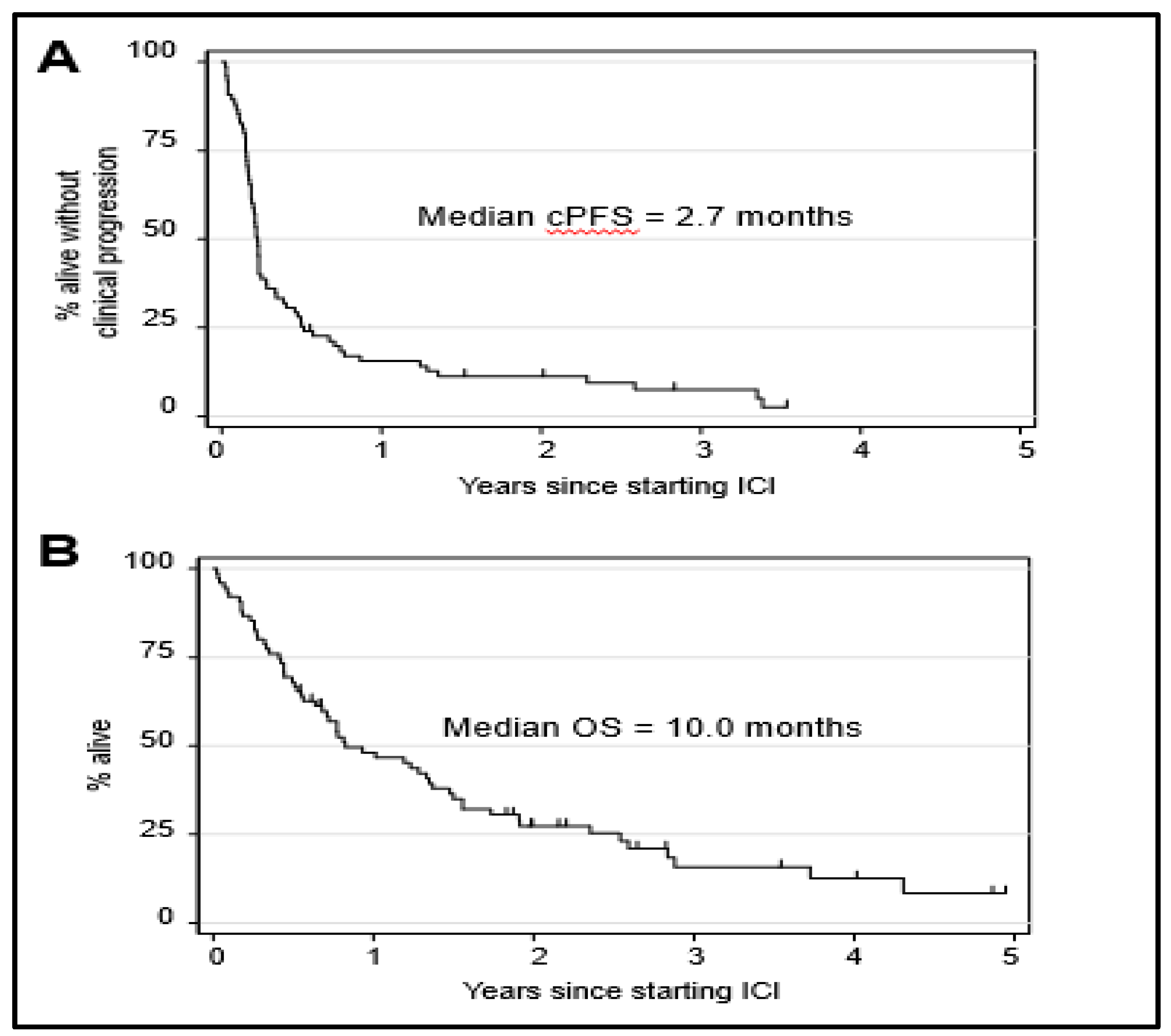
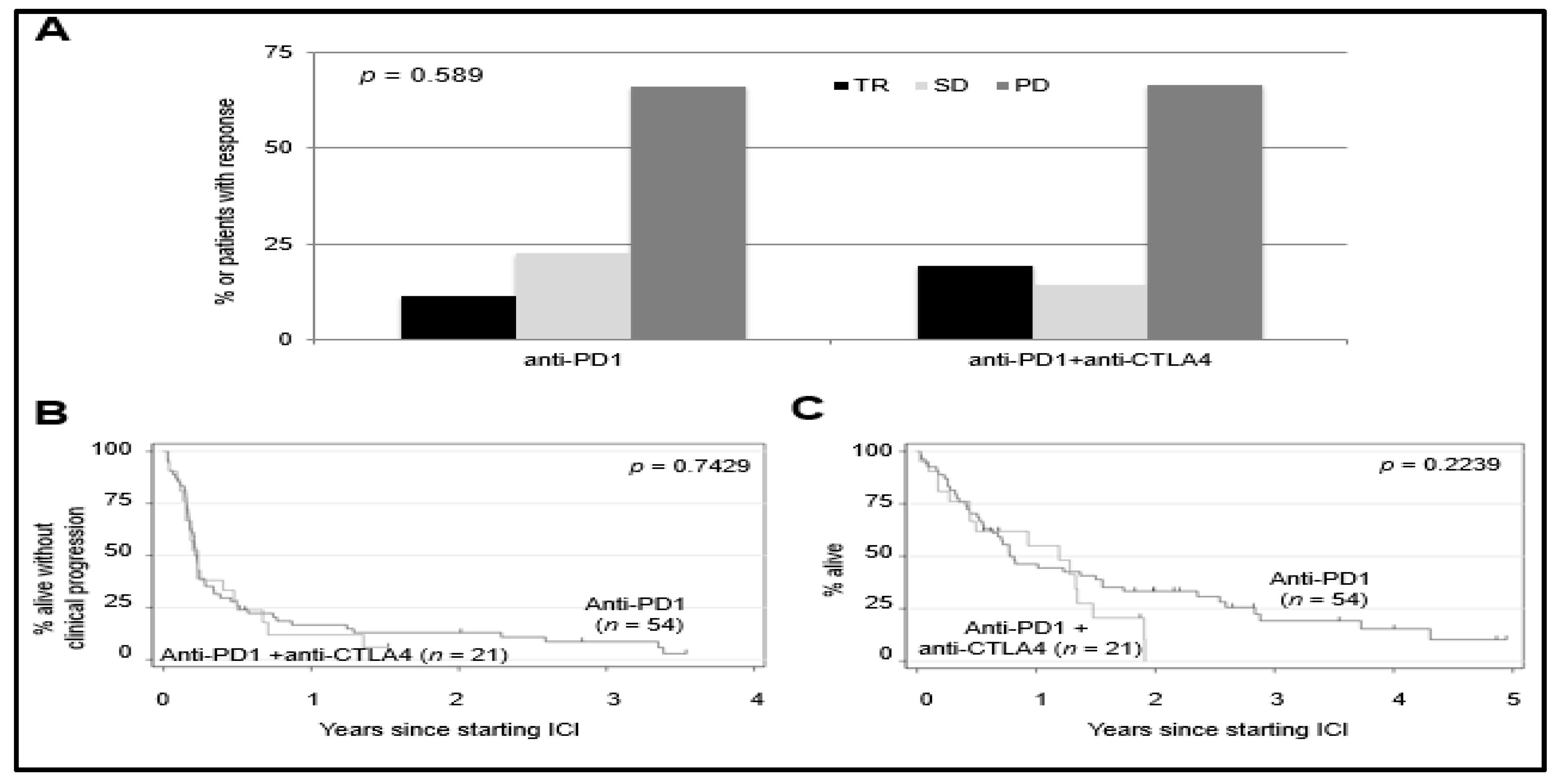
2.3. ICI Treatment Outcomes
2.4. Genomic Analyses of Study Population
2.5. Identification of Clinical Variables Associated with Survival
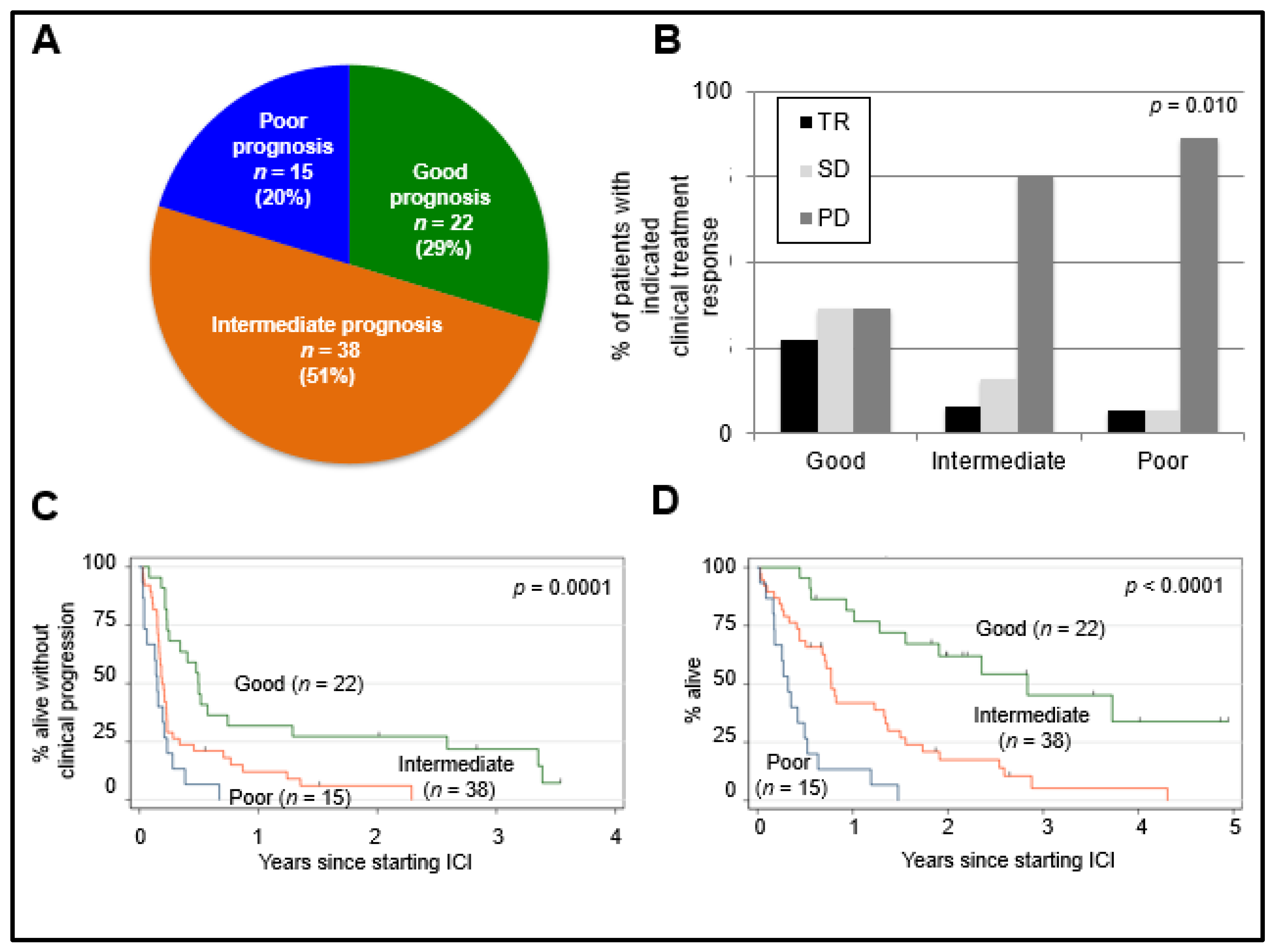
2.6. Prognostic Value of MUMPS Score
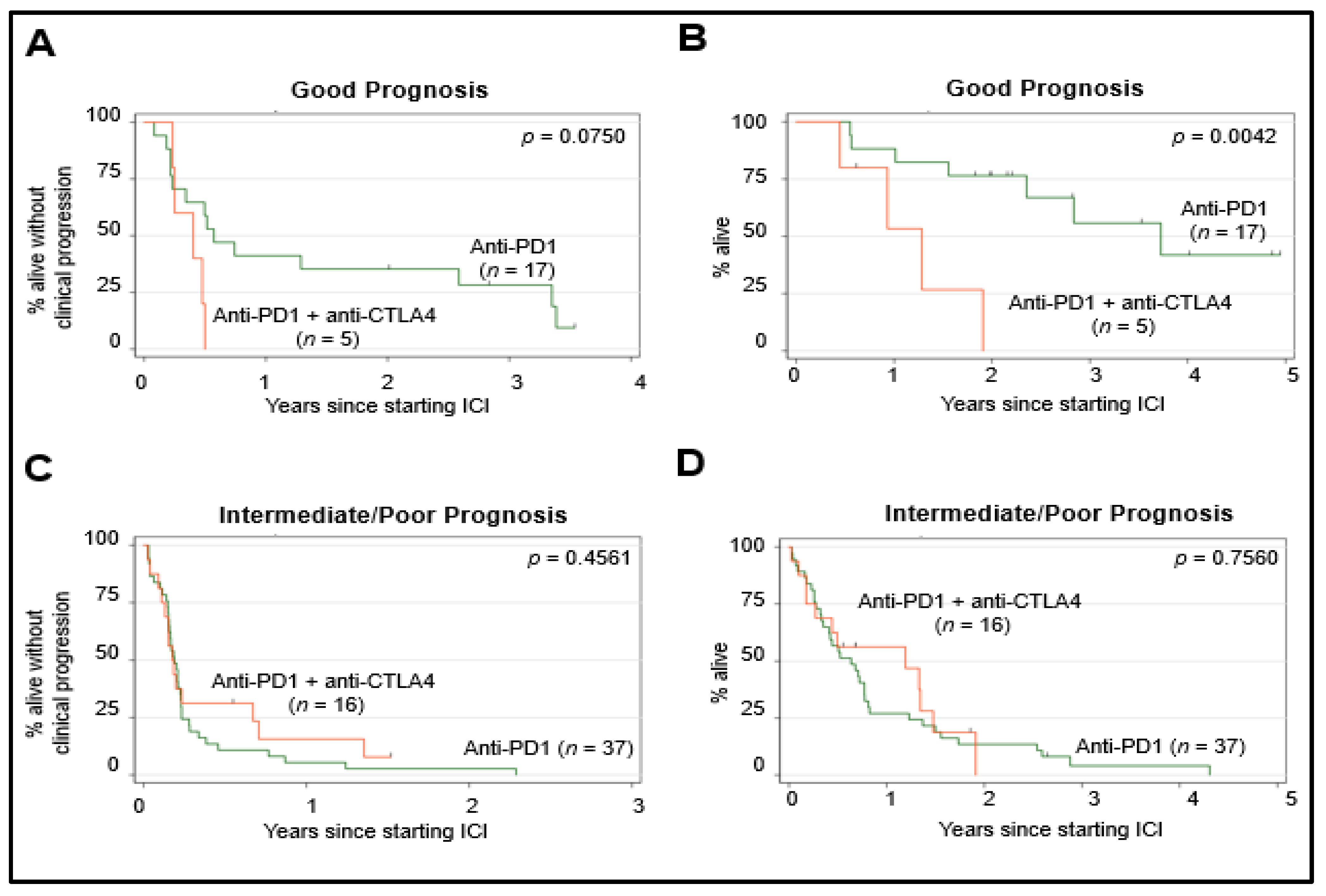
2.7. Predictive Value of MUMPS Score
3. Discussion
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kujala, E.; Mäkitie, T.; Kivelä, T. Very Long-Term Prognosis of Patients with Malignant Uveal Melanoma. Investig. Ophthalmol. Vis. Sci. 2003, 44, 4651–4659. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piulats, J.M.; Espinosa, E.; de la Cruz Merino, L.; Varela, M.; Carrión, L.A.; Martín-Algarra, S.; Castro, R.L.; Curiel, T.; Rodríguez-Abreu, D.; Redrado, M.; et al. Nivolumab Plus Ipilimumab for Treatment-Naïve Metastatic Uveal Melanoma: An Open-Label, Multicenter, Phase Ii Trial by the Spanish Multidisciplinary Melanoma Group (Gem-1402). J. Clin. Oncol. 2021, 39, 586–598. [Google Scholar] [CrossRef] [PubMed]
- Khoja, L.; Atenafu, E.G.; Suciu, S.; Leyvraz, S.; Sato, T.; Marshall, E.; Keilholz, U.; Zimmer, L.; Patel, S.P.; Piperno-Neumann, S.; et al. Meta-Analysis in Metastatic Uveal Melanoma to Determine Progression Free and Overall Survival Benchmarks: An International Rare Cancers Initiative (Irci) Ocular Melanoma Study. Ann. Oncol. 2019, 30, 1370–1380. [Google Scholar] [CrossRef] [PubMed]
- Virgili, G.; Gatta, G.; Ciccolallo, L.; Capocaccia, R.; Biggeri, A.; Crocetti, E.; Lutz, J.M.; Paci, E. Survival in Patients with Uveal Melanoma in Europe. Arch. Ophthalmol. 2008, 126, 1413–1418. [Google Scholar] [CrossRef] [Green Version]
- Diener-West, M.; Reynolds, S.M.; Agugliaro, D.J.; Caldwell, R.; Cumming, K.; Earle, J.D.; Hawkins, B.S.; Hayman, J.A.; Jaiyesimi, I.; Jampol, L.M.; et al. Development of Metastatic Disease after Enrollment in the Coms Trials for Treatment of Choroidal Melanoma: Collaborative Ocular Melanoma Study Group Report No. 26. Arch. Ophthalmol. 2005, 123, 1639–1643. [Google Scholar] [PubMed]
- Rao, P.K.; Barker, C.; Coit, D.G.; Joseph, R.W.; Materin, M.; Rengan, R.; Sosman, J.; Thompson, J.A.; Albertini, M.R.; Boland, G.; et al. Nccn Guidelines Insights: Uveal Melanoma, Version 1. 2019. J. Natl. Compr. Canc. Netw. 2020, 18, 120–131. [Google Scholar] [PubMed]
- Sato, T. Locoregional Management of Hepatic Metastasis from Primary Uveal Melanoma. Semin. Oncol. 2010, 37, 127–138. [Google Scholar] [CrossRef]
- Klingenstein, A.; Haug, A.R.; Zech, C.J.; Schaller, U.C. Radioembolization as Locoregional Therapy of Hepatic Metastases in Uveal Melanoma Patients. Cardiovasc. Intervent. Radiol. 2013, 36, 158–165. [Google Scholar] [CrossRef]
- Gonsalves, C.F.; Eschelman, D.J.; Adamo, R.D.; Anne, P.R.; Orloff, M.M.; Terai, M.; Hage, A.N.; Yi, M.; Chervoneva, I.; Sato, T. A Prospective Phase Ii Trial of Radioembolization for Treatment of Uveal Melanoma Hepatic Metastasis. Radiology 2019, 293, 223–231. [Google Scholar] [CrossRef]
- Muhammad Zubair, A.; Mabaera, R.; Shirai, K. Metastatic Uveal Melanoma Showing Durable Response to Anti-Ctla-4 and Anti-Pd-1 Combination Therapy after Experiencing Progression on Anti-Pd-1 Therapy Alone. J. Immunother. Cancer 2018, 6, 1–8. [Google Scholar]
- Weiss, S.A.; Wolchok, J.D.; Sznol, M. Immunotherapy of Melanoma: Facts and Hopes. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2019, 25, 5191–5201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bender, C.; Enk, A.; Gutzmer, R.; Hassel, J.C. Anti-Pd-1 Antibodies in Metastatic Uveal Melanoma: A Treatment Option? Cancer Med. 2017, 6, 1581–1586. [Google Scholar] [CrossRef]
- Algazi, A.P.; Tsai, K.K.; Shoushtari, A.N.; Munhoz, R.R.; Eroglu, Z.; Piulats, J.M.; Ott, P.A.; Johnson, D.B.; Hwang, J.; Daud, A.I.; et al. Clinical Outcomes in Metastatic Uveal Melanoma Treated with Pd-1 and Pd-L1 Antibodies. Cancer 2016, 122, 3344–3353. [Google Scholar] [CrossRef]
- Heppt, M.V.; Amaral, T.; Kähler, K.C.; Heinzerling, L.; Hassel, J.C.; Meissner, M.; Kreuzberg, N.; Loquai, C.; Reinhardt, L.; Utikal, J.; et al. Combined Immune Checkpoint Blockade for Metastatic Uveal Melanoma: A Retrospective, Multi-Center Study. J. Immunother. Cancer 2019, 7, 299. [Google Scholar] [CrossRef]
- Heppt, M.V.; Heinzerling, L.; Kähler, K.C.; Forschner, A.; Kirchberger, M.C.; Loquai, C.; Meissner, M.; Meier, F.; Terheyden, P.; Schell, B.; et al. Prognostic Factors and Outcomes in Metastatic Uveal Melanoma Treated with Programmed Cell Death-1 or Combined Pd-1/Cytotoxic T-Lymphocyte Antigen-4 Inhibition. Eur. J. Cancer 2017, 82, 56–65. [Google Scholar] [CrossRef]
- Najjar, Y.G.; Navrazhina, K.; Ding, F.; Bhatia, R.; Tsai, K.; Abbate, K.; Durden, B.; Eroglu, Z.; Bhatia, S.; Park, S.; et al. Ipilimumab Plus Nivolumab for Patients with Metastatic Uveal Melanoma: A Multicenter, Retrospective Study. J. Immunother. Cancer 2020, 8, e000331. [Google Scholar] [CrossRef]
- Hogg, D.; Monzon, J.G.; Ernst, S.; Song, X.; McWhirter, E.; Savage, K.J.; Skinn, B.; Romeyer, F.; Smylie, M. Canadian Cohort Expanded-Access Program of Nivolumab Plus Ipilimumab in Advanced Melanoma. Curr. Oncol. 2020, 27, 204–214. [Google Scholar] [CrossRef]
- Hodi, F.S.; Chapman, P.B.; Sznol, M.; Lao, C.D.; Gonzalez, R.; Smylie, M.; Daniels, G.A.; Thompson, J.A.; Kudchadkar, R.; Sharfman, W.; et al. Safety and Efficacy of Combination Nivolumab Plus Ipilimumab in Patients with Advanced Melanoma: Results from a North American Expanded Access Program (Checkmate 218). Melanoma Res. 2021, 31, 67–75. [Google Scholar] [CrossRef] [PubMed]
- Hassel, J.C.; Rutkowski, P.; Baurain, J.-E.; Butler, M.O.; Schlaak, M.; Sullivan, R.; Ochsenreither, S.; Dummer, R.; Kirkwood, J.M.; Joshua, A.M.; et al. Co-Primary Endpoint of Overall Survival for Tebentafusp (Tebe)-Induced Rash in a Phase 3 Randomized Trial Comparing Tebe Versus Investigator’s Choice (Ic) in First-Line Metastatic Uveal Melanoma. J. Clin. Oncol. 2021, 39, 9527–9627. [Google Scholar] [CrossRef]
- Pelster, M.S.; Gruschkus, S.K.; Bassett, R.; Gombos, D.S.; Shephard, M.; Posada, L.; Glover, M.S.; Simien, R.; Diab, A.; Hwu, P.; et al. Nivolumab and Ipilimumab in Metastatic Uveal Melanoma: Results from a Single-Arm Phase Ii Study. J. Clin. Oncol. 2020, 39, 599–607. [Google Scholar] [CrossRef]
- Rodriguez, J.M.P.; De La Cruz Merino, L.; Espinosa, E.; Carrion, L.A.; Algarra, S.M.; Lopez-Castro, R.; Garcıa, M.T.C.; Abreu, D.R.; Iriarte, A.J.R.; Jaime, A.B. Phase II Multicenter, Single Arm, Open Label Study of Nivolumab in Combination with Ipilimumab in Untreated Patients with Metastatic Uveal Melanoma (Gem1402.Nct02626962). Ann. Oncol. 2018, 29, viii443. [Google Scholar] [CrossRef]
- Damato, B.; Dopierala, J.; Klaasen, A.; van Dijk, M.; Sibbring, J.; Coupland, S.E. Multiplex Ligation-Dependent Probe Amplification of Uveal Melanoma: Correlation with Metastatic Death. Investig. Ophthalmol. Vis. Sci. 2009, 50, 3048–3055. [Google Scholar] [CrossRef] [Green Version]
- Bellerive, C.; Grossniklaus, H.E.; Singh, A.D. Prognostication for Uveal Melanoma: Are Two Tests Better Than One. Ocul. Oncol. Pathol. 2017, 3, 301–303. [Google Scholar] [CrossRef]
- Dogrusöz, M.; Jager, M.J. Genetic Prognostication in Uveal Melanoma. Acta Ophthalmol. 2018, 96, 331–347. [Google Scholar] [CrossRef] [PubMed]
- Chakravarty, D.; Gao, J.; Phillips, S.M.; Kundra, R.; Zhang, H.; Wang, J.; Rudolph, J.E.; Yaeger, R.; Soumerai, T.; Nissan, M.H.; et al. Oncokb: A Precision Oncology Knowledge Base. JCO Precis. Oncol. 2017, 1, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Nicholas, M.N.; Khoja, L.; Atenafu, E.G.; Hogg, D.; Quirt, I.; Butler, M.; Joshua, A.M. Prognostic Factors for First-Line Therapy and Overall Survival of Metastatic Uveal Melanoma: The Princess Margaret Cancer Centre Experience. Melanoma Res. 2018, 28, 571–577. [Google Scholar] [CrossRef] [PubMed]
- Motzer, R.J.; Bacik, J.; Murphy, B.A.; Russo, P.; Mazumdar, M. Interferon-Alfa as a Comparative Treatment for Clinical Trials of New Therapies against Advanced Renal Cell Carcinoma. J. Clin. Oncol. 2002, 20, 289–296. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.L.; Belldegrun, A.S.; Freitas, D.G.; Bui, M.H.; Han, K.R.; Dorey, F.J.; Figlin, R.A. Paraneoplastic Signs and Symptoms of Renal Cell Carcinoma: Implications for Prognosis. J. Urol. 2003, 170, 1742–1746. [Google Scholar] [CrossRef] [Green Version]
- Heng, D.Y.C.; Xie, W.; Regan, M.M.; Warren, M.A.; Golshayan, A.R.; Sahi, C.; Eigl, B.J.; Ruether, J.D.; Cheng, T.; North, S.; et al. Prognostic Factors for Overall Survival in Patients with Metastatic Renal Cell Carcinoma Treated with Vascular Endothelial Growth Factor–Targeted Agents: Results from a Large, Multicenter Study. J. Clin. Oncol. 2009, 27, 5794–5799. [Google Scholar] [CrossRef]
- Pires da Silva, I.; Lo, S.; Quek, C.; Gonzalez, M.; Carlino, M.S.; Long, G.V.; Menzies, A.M. Site-Specific Response Patterns, Pseudoprogression, and Acquired Resistance in Patients with Melanoma Treated with Ipilimumab Combined with Anti-Pd-1 Therapy. Cancer 2020, 126, 86–97. [Google Scholar] [CrossRef] [Green Version]
- Landi, L.; D’Incà, F.; Gelibter, A.; Chiari, R.; Grossi, F.; Delmonte, A.; Passaro, A.; Signorelli, D.; Gelsomino, F.; Galetta, D.; et al. Bone Metastases and Immunotherapy in Patients with Advanced Non-Small-Cell Lung Cancer. J. Immunother. Cancer 2019, 7, 316. [Google Scholar] [CrossRef]
- de Liaño Lista, A.G.; van Dijk, N.; de Rueda, G.D.O.; Necchi, A.; Lavaud, P.; Morales-Barrera, R.; Gordoa, T.A.; Maroto, P.; Ravaud, A.; Durán, I.; et al. Clinical Outcome after Progressing to Frontline and Second-Line Anti-Pd-1/Pd-L1 in Advanced Urothelial Cancer. Eur. Urol. 2020, 77, 269–276. [Google Scholar] [CrossRef]
- Bollig, C.A.; Newberry, C.I.; Galloway, T.L.I.; Zitsch, R.P.; Hanly, E.K.; Zhu, V.L.; Pagedar, N.; Nallani, R.; Bur, A.M.; Spanos, W.C.; et al. Prognostic Impact of Metastatic Site and Pattern in Patients with Metastatic Head and Neck Cancer. Laryngoscope 2020, 131, E1838–E1846. [Google Scholar]
- McKay, R.R.; Kroeger, N.; Xie, W.; Lee, J.L.; Knox, J.J.; Bjarnason, G.A.; MacKenzie, M.J.; Wood, L.; Srinivas, S.; Vaishampayan, U.N.; et al. Impact of Bone and Liver Metastases on Patients with Renal Cell Carcinoma Treated with Targeted Therapy. Eur. Urol. 2014, 65, 577–584. [Google Scholar] [CrossRef] [Green Version]
- Motzer, R.J.; Tannir, N.M.; McDermott, D.F.; Frontera, O.A.; Melichar, B.; Choueiri, T.K.; Plimack, E.R.; Barthélémy, P.; Porta, C.; George, S.; et al. Nivolumab Plus Ipilimumab Versus Sunitinib in Advanced Renal-Cell Carcinoma. N. Engl. J. Med. 2018, 378, 1277–1290. [Google Scholar] [CrossRef] [PubMed]
- Nathan, P.; Ascierto, P.A.; Haanen, J.; Espinosa, E.; Demidov, L.; Garbe, C.; Guida, M.; Lorigan, P.; Chiarion-Sileni, V.; Gogas, H.; et al. Safety and Efficacy of Nivolumab in Patients with Rare Melanoma Subtypes Who Progressed on or after Ipilimumab Treatment: A Single-Arm, Open-Label, Phase Ii Study (Checkmate 172). Eur. J. Cancer 2019, 119, 168–178. [Google Scholar] [CrossRef] [PubMed]
- Lebbé, C.; Meyer, N.; Mortier, L.; Marquez-Rodas, I.; Robert, C.; Rutkowski, P.; Menzies, A.M.; Eigentler, T.; Ascierto, P.A.; Smylie, M.; et al. Evaluation of Two Dosing Regimens for Nivolumab in Combination with Ipilimumab in Patients with Advanced Melanoma: Results from the Phase Iiib/Iv Checkmate 511 Trial. J. Clin. Oncol. 2019, 37, 867–875. [Google Scholar] [CrossRef] [PubMed]
- Carlino, M.S.; Menzies, A.M.; Atkinson, V.; Cebon, J.S.; Jameson, M.B.; Fitzharris, B.M.; McNeil, C.M.; Hill, A.G.; Ribas, A.; Atkins, M.B.; et al. Long-Term Follow-up of Standard-Dose Pembrolizumab Plus Reduced-Dose Ipilimumab in Patients with Advanced Melanoma: Keynote-029 Part 1b. Clin. Cancer Res. 2020, 26, 5086–5091. [Google Scholar] [CrossRef] [PubMed]
- Lipson, E.J.; Tawbi, H.A.H.; Schadendorf, D.; Ascierto, P.A.; Matamala, L.; Gutiérrez, E.C.; Rutkowski, P.; Gogas, H.; Lao, C.D.; de Menezes, J.J.; et al. Relatlimab (Rela) Plus Nivolumab (Nivo) Versus Nivo in First-Line Advanced Melanoma: Primary Phase Iii Results from Relativity-047 (Ca224-047). J. Clin. Oncol. 2021, 39, 9503. [Google Scholar] [CrossRef]
- de Ávila Machado, M.A.; de Moura, C.S.; Chan, K.; Curtis, J.R.; Hudson, M.; Abrahamowicz, M.; Jamal, R.; Pilote, L.; Bernatsky, S. Real-World Analyses of Therapy Discontinuation of Checkpoint Inhibitors in Metastatic Melanoma Patients. Sci. Rep. 2020, 10, 14607. [Google Scholar] [CrossRef]
- Hoefsmit, E.P.; Rozeman, E.A.; Van, T.M.; Dimitriadis, P.; Krijgsman, O.; Conway, J.W.; da Silva, I.P.; van der Wal, J.E.; Ketelaars, S.L.C.; Bresser, K.; et al. Comprehensive Analysis of Cutaneous and Uveal Melanoma Liver Metastases. J. Immunother. Cancer 2020, 8, e001501. [Google Scholar] [CrossRef]
- Waterhouse, D.M.; Garon, E.B.; Chandler, J.; McCleod, M.; Hussein, M.; Jotte, R.; Horn, L.; Daniel, D.B.; Keogh, G.; Creelan, B.; et al. Continuous Versus 1-Year Fixed-Duration Nivolumab in Previously Treated Advanced Non-Small-Cell Lung Cancer: Checkmate 153. J. Clin. Oncol. 2020, 38, 3863–3873. [Google Scholar] [CrossRef]
- NIH. “Recruiting Studies; Uveal Melanoma, Metastatic” NIH U.S. National Library of Medicine Clinical Trials.gov. Available online: https://clinicaltrials.gov/ct2/results?cond=Uveal+Melanoma%2C+Metastatic&Search=Apply&recrs=a&age_v=&gndr=&type=&rslt= (accessed on 24 January 2021).
- Middleton, M.R.; McAlpine, C.; Woodcock, V.K.; Corrie, P.; Infante, J.R.; Steven, N.M.; Evans, T.R.J.; Anthoney, A.; Shoushtari, A.N.; Hamid, O.; et al. Tebentafusp, a Tcr/Anti-Cd3 Bispecific Fusion Protein Targeting Gp100, Potently Activated Antitumor Immune Responses in Patients with Metastatic Melanoma. Clin. Cancer Res. 2020, 26, 5869–5878. [Google Scholar] [CrossRef]
- Chandran, S.S.; Somerville, R.P.T.; Yang, J.C.; Sherry, R.M.; Klebanoff, C.A.; Goff, S.L.; Wunderlich, J.R.; Danforth, D.N.; Zlott, D.; Paria, B.C.; et al. Treatment of Metastatic Uveal Melanoma with Adoptive Transfer of Tumour-Infiltrating Lymphocytes: A Single-Centre, Two-Stage, Single-Arm, Phase 2 Study. Lancet Oncol. 2017, 18, 792–802. [Google Scholar] [CrossRef]
- Rose, A.A.N.; Armstrong, S.M.; Hogg, D.; Butler, M.O.; Saibil, S.D.; Arteaga, D.P.; Muniz, T.P.; Kelly, D.; Ghazarian, D.; King, I.; et al. Biologic Subtypes of Melanoma Predict Survival Benefit of Combination Anti-Pd1+Anti-Ctla4 Immune Checkpoint Inhibitors Versus Anti-Pd1 Monotherapy. J. Immunother. Cancer 2021, 9, e001642. [Google Scholar] [CrossRef] [PubMed]
- Louie, B.H.; Kurzrock, R. Bap1: Not Just a Brca1-Associated Protein. Cancer Treat. Rev. 2020, 90, 102091. [Google Scholar] [CrossRef] [PubMed]
- Figueiredo, C.R.; Kalirai, H.; Sacco, J.J.; Azevedo, R.A.; Duckworth, A.; Slupsky, J.R.; Coulson, J.M.; Coupland, S.E. Loss of Bap1 Expression Is Associated with an Immunosuppressive Microenvironment in Uveal Melanoma, with Implications for Immunotherapy Development. J. Pathol. 2020, 250, 420–439. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Characteristics |
Entire Cohort (n = 75) |
Anti-PD1 (n = 54) |
Anti-PD1 + Anti-CTLA4 (n = 21) | p -Value |
|---|---|---|---|---|
| Age | ||||
| <65 | 39 (52%) | 25 (46%) | 14 (67%) | 0.130 |
| ≥65 | 36 (48%) | 29 (54%) | 7 (33%) | |
| Sex | ||||
| female | 40 (53%) | 29 (54%) | 11 (52%) | 1.000 |
| male | 35 (47%) | 25 (46%) | 10 (48%) | |
| BMI | ||||
| <25 | 24 (32%) | 21 (39%) | 3 (14%) | 0.054 |
| ≥25 | 51 (68%) | 33 (61%) | 18 (86%) | |
| ECOG | ||||
| 0 | 20 (27%) | 13 (24%) | 7 (33%) | 0.502 |
| 1 | 52 (69%) | 38 (70%) | 14 (67%) | |
| 2 | 3 (4%) | 3 (6%) | 0 (0%) | |
| Time from dx to metastasis | ||||
| <2 years | 40 (53%) | 32 (59%) | 8 (38%) | 0.125 |
| ≥2 years | 35 (47%) | 22 (41%) | 13 (62%) | |
| Liver Directed Therapy | ||||
| None | 66 (88%) | 47 (87%) | 19 (90%) | |
| Radiofrequency Ablation | 1 (1%) | 1 (2%) | 0 | |
| Chemoembolization | 2 (3%) | 1 (2%) | 1 (5%) | |
| Radiation | 2 (3%) | 2 (4%) | 0 | |
| Radioembolization | 4 (5%) | 3 (6%) | 1 (5%) | |
| # Previous systemic therapies | ||||
| 0 | 38 (51%) | 30 (56%) | 8 (38%) | 0.385 |
| 1 | 16 (21%) | 10 (19%) | 6 (29%) | |
| ≥2 | 21 (28%) | 14 (26%) | 7 (33%) | |
| Prior Immunotherapy | ||||
| No | 51 (68%) | 32 (59%) | 9 (42%) | 0.302 |
| Yes | 24 (32%) | 22 (41%) | 12 (58%) | |
| Prior chemotherapy | ||||
| No | 63 (84%) | 47 (87%) | 16 (76%) | 0.299 |
| Yes | 12 (16%) | 7 (13%) | 5 (24%) | |
| Liver Metastases | 0.188 | |||
| Absent | 3 (4%) | 1 (2%) | 2 (10%) | |
| Present | 72 (96%) | 53 (98%) | 19 (90%) | |
| Lung metastases | ||||
| Absent | 49 (65%) | 36 (67%) | 13 (62%) | 0.789 |
| Present | 26 (35%) | 18 (33%) | 8 (38%) | |
| Bone Metastases | ||||
| No | 66 (88%) | 46 (85%) | 20 (95%) | 0.430 |
| Yes | 9 (12%) | 8 (15%) | 1 (5%) | |
| Largest metastasis size | ||||
| <6 cm | 45 (60%) | 32 (59%) | 13 (62%) | 1.000 |
| ≥6 cm | 30 (40%) | 22 (41%) | 8 (38%) | |
| LDH | ||||
| <1.5 × ULN | 45 (60%) | 33 (61%) | 12 (57%) | 0.797 |
| ≥1.5 × ULN | 30 (40%) | 21 (39%) | 9 (43%) | |
| NLR | ||||
| <4 | 47 (63%) | 33 (61%) | 12 (57%) | 0.476 |
| ≥4 | 28 (37%) | 21 (39%) | 9 (43%) |
| Clinical Characteristics | Univariable | Multivariable | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | |
| cPFS | ||||||
| Age > 65 | 0.99 | 0.62–1.60 | 0.984 | - | - | - |
| Male | 0.81 | 0.51–1.30 | 0.393 | - | - | - |
| ECOG ≥ 1 | 1.28 | 0.76–2.18 | 0.355 | - | - | - |
| BMI ≥ 25 | 0.64 | 0.39–1.05 | 0.079 | - | - | - |
| Time from initial dx to stage IV <2 years | 1.82 | 1.14–3.05 | 0.016 | 2.45 | 1.44–4.18 | 0.001 |
| >1 prior systemic therapy | 0.76 | 0.38–1.19 | 0.327 | - | - | - |
| Prior immunotherapy | 1.15 | 0.72–1.86 | 0.557 | - | - | - |
| Prior chemotherapy | 0.78 | 0.37–1.41 | 0.450 | - | - | - |
| ICI regimen: PD1 + CTLA4 vs. PD1 | 1.09 | 0.64–1.87 | 0.745 | - | - | - |
| Lung metastases | 1.16 | 0.71–1.92 | 0.539 | - | - | - |
| Bone metastases | 2.13 | 1.03–4.42 | 0.042 | 1.91 | 0.91–4.00 | 0.086 |
| Largest metastasis diameter ≥6 cm | 1.48 | 0.92–2.40 | 0.105 | - | - | - |
| LDH ≥ 1.5 × ULN | 2.34 | 1.43–3.85 | 0.001 | 2.26 | 1.36–3.77 | 0.002 |
| NLR ≥ 4 | 1.69 | 1.05–2.74 | 0.032 | 2.14 | 1.25–3.65 | 0.005 |
| Clinical Characteristics | Univariable | Multivariable | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | |
| Overall Survivial | ||||||
| Age ≥ 65 | 1.51 | 0.90–2.54 | 0.121 | 1.69 | 0.96–2.97 | 0.068 |
| Male | 0.99 | 0.60–1.66 | 0.981 | - | - | - |
| ECOG ≥ 1 | 2.04 | 1.08–3.89 | 0.029 | - | - | - |
| BMI ≥ 25 | 0.74 | 0.43–1.29 | 0.297 | - | - | - |
| Time from initial dx to stage IV <2 years | 1.86 | 1.11–3.12 | 0.019 | 2.82 | 1.60–4.95 | <0.001 |
| >1 prior systemic therapy | 0.83 | 0.47–1.49 | 0.541 | - | - | - |
| Prior immunotherapy | 1.28 | 0.76–2.14 | 0.679 | - | - | - |
| Prior chemotherapy | 0.77 | 0.38–1.58 | 0.472 | - | - | - |
| ICI regimen: PD1 + CTLA4 vs. PD1 | 1.44 | 0.80–2.62 | 0.227 | - | - | - |
| Lung metastases | 1.48 | 0.87–2.52 | 0.152 | - | - | - |
| Bone metastases | 1.86 | 0.90–3.87 | 0.092 | 2.57 | 1.19–5.55 | 0.016 |
| Largest metastasis diameter ≥6 cm | 2.11 | 1.26–3.56 | 0.005 | 2.22 | 1.25–3.92 | 0.006 |
| LDH ≥ 1.5 × ULN | 4.45 | 2.57–7.73 | <0.001 | 4.25 | 2.35–7.68 | <0.001 |
| NLR ≥ 4 | 1.65 | 0.98–2.79 | 0.062 | - | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kelly, D.; Rose, A.A.N.; Muniz, T.P.; Hogg, D.; Butler, M.O.; Saibil, S.D.; King, I.; Kamil, Z.S.; Ghazarian, D.; Ross, K.; et al. Development of a Metastatic Uveal Melanoma Prognostic Score (MUMPS) for Use in Patients Receiving Immune Checkpoint Inhibitors. Cancers 2021, 13, 3640. https://doi.org/10.3390/cancers13143640
Kelly D, Rose AAN, Muniz TP, Hogg D, Butler MO, Saibil SD, King I, Kamil ZS, Ghazarian D, Ross K, et al. Development of a Metastatic Uveal Melanoma Prognostic Score (MUMPS) for Use in Patients Receiving Immune Checkpoint Inhibitors. Cancers. 2021; 13(14):3640. https://doi.org/10.3390/cancers13143640
Chicago/Turabian StyleKelly, Deirdre, April A. N. Rose, Thiago Pimentel Muniz, David Hogg, Marcus O. Butler, Samuel D. Saibil, Ian King, Zaid Saeed Kamil, Danny Ghazarian, Kendra Ross, and et al. 2021. "Development of a Metastatic Uveal Melanoma Prognostic Score (MUMPS) for Use in Patients Receiving Immune Checkpoint Inhibitors" Cancers 13, no. 14: 3640. https://doi.org/10.3390/cancers13143640
APA StyleKelly, D., Rose, A. A. N., Muniz, T. P., Hogg, D., Butler, M. O., Saibil, S. D., King, I., Kamil, Z. S., Ghazarian, D., Ross, K., Iafolla, M., Araujo, D. V., Waldron, J., Laperriere, N., Krema, H., & Spreafico, A. (2021). Development of a Metastatic Uveal Melanoma Prognostic Score (MUMPS) for Use in Patients Receiving Immune Checkpoint Inhibitors. Cancers, 13(14), 3640. https://doi.org/10.3390/cancers13143640