
Neuroendocrine Carcinomas of the Digestive Tract: What Is New?


Abstract
:Simple Summary
Abstract
1. Introduction
2. Epidemiological Features and Tumor Presentation
2.1. Incidence and Tumor Site
2.2. Clinical Presentation and Biomarkers
2.3. Tumoral Staging and Prognosis
3. Imaging
3.1. Morphological Imaging
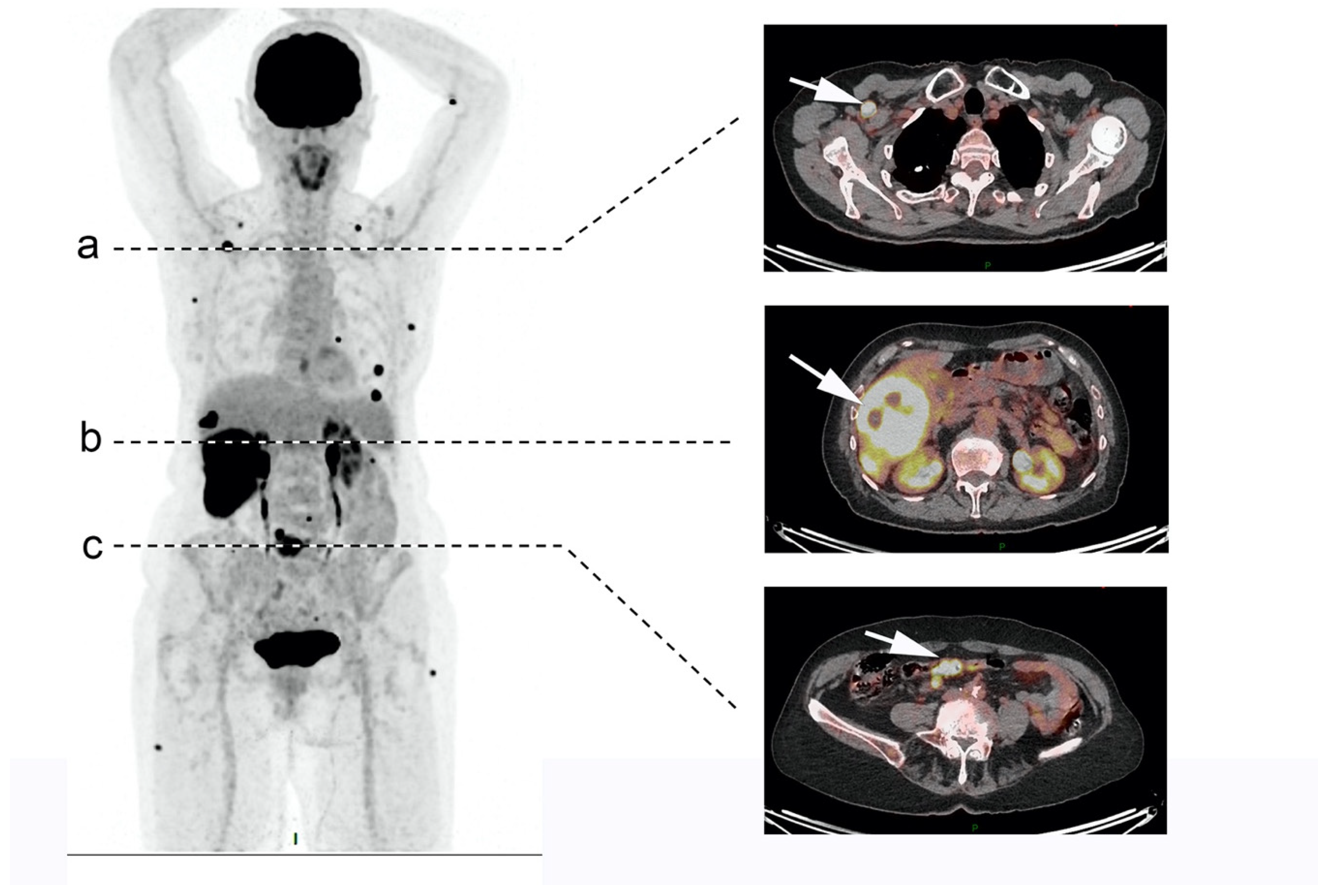
3.2. Functional Imaging
4. Histology
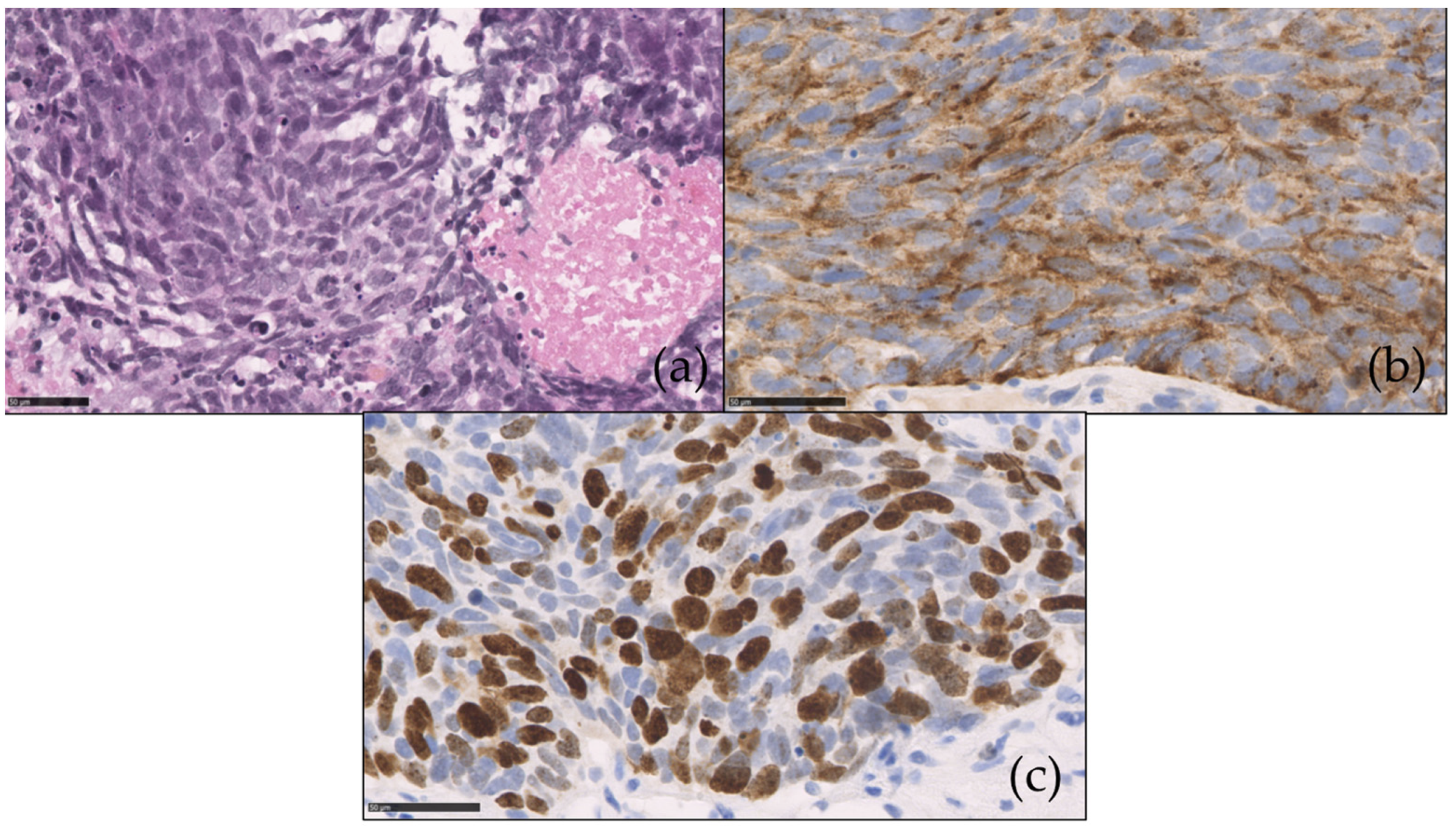
4.1. Morphological and Immunohistochemistry Features
4.2. Molecular Biology
4.3. Circulating Tumor Deoxyribonucleic Acid (DNA)
5. Treatment
5.1. In the Localized Setting
5.1.1. Surgery
5.1.2. Radiotherapy and Concurrent Chemoradiotherapy
5.2. In the Metastatic Setting
5.2.1. Surgery
5.2.2. Liver-Directed Therapies
5.2.3. First-Line Chemotherapy
5.2.4. Second-Line Chemotherapy
5.2.5. Peptide Receptor Radionuclide Therapy (PRRT)
5.2.6. Targeted Therapies
5.2.7. Immunotherapy
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Baudin, E. Gastroenteropancreatic Endocrine Tumors: Clinical Characterization before Therapy. Nat. Clin. Pract. Endocrinol. Metab. 2007, 3, 228–239. [Google Scholar] [CrossRef]
- Klöppel, G. Neuroendocrine Neoplasms: Dichotomy, Origin and Classifications. Visc. Med. 2017, 33, 324–330. [Google Scholar] [CrossRef]
- Hijioka, S.; Hosoda, W.; Matsuo, K.; Ueno, M.; Furukawa, M.; Yoshitomi, H.; Kobayashi, N.; Ikeda, M.; Ito, T.; Nakamori, S.; et al. Rb Loss and KRAS Mutation Are Predictors of the Response to Platinum-Based Chemotherapy in Pancreatic Neuroendocrine Neoplasm with Grade 3: A Japanese Multicenter Pancreatic NEN-G3 Study. Clin. Cancer Res. 2017, 23, 4625–4632. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagtegaal, I.D.; Odze, R.D.; Klimstra, D.; Paradis, V.; Rugge, M.; Schirmacher, P.; Washington, K.M.; Carneiro, F.; Cree, I.A.; WHO Classification of Tumours Editorial Board. The 2019 WHO Classification of Tumours of the Digestive System. Histopathology 2020, 76, 182–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basturk, O.; Yang, Z.; Tang, L.H.; Hruban, R.H.; Adsay, V.; McCall, C.M.; Krasinskas, A.M.; Jang, K.T.; Frankel, W.L.; Balci, S.; et al. The High-Grade (WHO G3) Pancreatic Neuroendocrine Tumor Category Is Morphologically and Biologically Heterogenous and Includes Both Well Differentiated and Poorly Differentiated Neoplasms. Am. J. Surg. Pathol. 2015, 39, 683–690. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Velayoudom-Cephise, F.L.; Duvillard, P.; Foucan, L.; Hadoux, J.; Chougnet, C.N.; Leboulleux, S.; Malka, D.; Guigay, J.; Goere, D.; Debaere, T.; et al. Are G3 ENETS Neuroendocrine Neoplasms Heterogeneous? Endocr. Relat. Cancer 2013, 20, 649–657. [Google Scholar] [CrossRef] [Green Version]
- Fazio, N.; Milione, M. Heterogeneity of Grade 3 Gastroenteropancreatic Neuroendocrine Carcinomas: New Insights and Treatment Implications. Cancer Treat. Rev. 2016, 50, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Perren, A.; Couvelard, A.; Scoazec, J.-Y.; Costa, F.; Borbath, I.; Delle Fave, G.; Gorbounova, V.; Gross, D.; Grossma, A.; Jense, R.T.; et al. ENETS Consensus Guidelines for the Standards of Care in Neuroendocrine Tumors: Pathology: Diagnosis and Prognostic Stratification. Neuroendocrinology 2017, 105, 196–200. [Google Scholar] [CrossRef]
- Rindi, G.; Klimstra, D.S.; Abedi-Ardekani, B.; Asa, S.L.; Bosman, F.T.; Brambilla, E.; Busam, K.J.; de Krijger, R.R.; Dietel, M.; El-Naggar, A.K.; et al. A Common Classification Framework for Neuroendocrine Neoplasms: An International Agency for Research on Cancer (IARC) and World Health Organization (WHO) Expert Consensus Proposal. Mod. Pathol. 2018, 31, 1770–1786. [Google Scholar] [CrossRef]
- Pellat, A.; Coriat, R. Well Differentiated Grade 3 Neuroendocrine Tumors of the Digestive Tract: A Narrative Review. J. Clin. Med. 2020, 9, 1677. [Google Scholar] [CrossRef]
- Yao, J.C.; Hassan, M.; Phan, A.; Dagohoy, C.; Leary, C.; Mares, J.E.; Abdalla, E.K.; Fleming, J.B.; Vauthey, J.N.; Rashid, A.; et al. One Hundred Years after “Carcinoid”: Epidemiology of and Prognostic Factors for Neuroendocrine Tumors in 35,825 Cases in the United States. J. Clin. Oncol. 2008, 26, 3063–3072. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Korse, C.M.; Taal, B.G.; van Velthuysen, M.L.; Visser, O. Incidence and Survival of Neuroendocrine Tumours in the Netherlands According to Histological Grade: Experience of Two Decades of Cancer Registry. Eur. J. Cancer 2013, 49, 1975–1983. [Google Scholar] [CrossRef] [PubMed]
- Dasari, A.; Shen, C.; Halperin, D.; Zhao, B.; Zhou, S.; Xu, Y.; Shih, T.; Yao, J.C. Trends in the Incidence, Prevalence, and Survival Outcomes in Patients With Neuroendocrine Tumors in the United States. JAMA Oncol. 2017, 3, 1335–1342. [Google Scholar] [CrossRef] [PubMed]
- Scoazec, J.-Y.; Couvelard, A.; Monges, G.; Leteurtre, E.; Belleannee, G.; Guyetant, S.; Duvillard, P.; Danjoux, M.; Parot, X.; Lepage, C. Well-Differentiated Grade 3 Digestive Neuroendocrine Tumors: Myth or Reality? The PRONET Study Group. J. Clin. Oncol. 2012, 30, 4129. [Google Scholar] [CrossRef]
- Lepage, C.; Ciccolallo, L.; Angelis, R.D.; Bouvier, A.M.; Faivre, J.; Gatta, G. European Disparities in Malignant Digestive Endocrine Tumours Survival. Int. J. Cancer 2010, 126, 2928–2934. [Google Scholar] [CrossRef]
- Lepage, C.; Bouvier, A.M.; Faivre, J. Endocrine Tumours: Epidemiology of Malignant Digestive Neuroendocrine Tumours. Eur. J. Endocrinol. 2013, 168, R77–R83. [Google Scholar] [CrossRef] [PubMed]
- Scoazec, J.-Y.; Couvelard, A.; Monges, G.; Guyétant, S.; Bisot-Locard, S.; Parot, X.; Lepage, C.; PRONET Study Group. Professional Practices and Diagnostic Issues in Neuroendocrine Tumour Pathology: Results of a Prospective One-Year Survey among French Pathologists (the PRONET Study). Neuroendocrinology 2017, 105, 67–76. [Google Scholar] [CrossRef] [PubMed]
- Heetfeld, M.; Chougnet, C.N.; Olsen, I.H.; Rinke, A.; Borbath, I.; Crespo, G.; Barriuso, J.; Pavel, M.; O’Toole, D.; Walter, T.; et al. Characteristics and Treatment of Patients with G3 Gastroenteropancreatic Neuroendocrine Neoplasms. Endocr. Relat. Cancer 2015, 22, 657–664. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dasari, A.; Mehta, K.; Byers, L.A.; Sorbye, H.; Yao, J.C. Comparative Study of Lung and Extrapulmonary Poorly Differentiated Neuroendocrine Carcinomas: A SEER Database Analysis of 162,983 Cases. Cancer 2017, 124, 807–815. [Google Scholar] [CrossRef]
- Kumar, A.; Sundararajan, S.; Cui, H.; Patel, H.; Elquza, E. Epidemiology and Survival of Small Cell Carcinoma of Gastrointestional Tract: A Surveillance, Epidemiology, and End Results (SEER) Database Review. J. Clin. Oncol. 2016, 34, 518. [Google Scholar] [CrossRef]
- Walter, T.; Tougeron, D.; Baudin, E.; Le Malicot, K.; Lecomte, T.; Malka, D.; Hentic, O.; Manfredi, S.; Bonnet, I.; Guimbaud, R.; et al. Poorly Differentiated Gastro-Entero-Pancreatic Neuroendocrine Carcinomas: Are They Really Heterogeneous? Insights from the FFCD-GTE National Cohort. Eur. J. Cancer 2017, 79, 158–165. [Google Scholar] [CrossRef]
- Brenner, B.; Tang, L.H.; Klimstra, D.S.; Kelsen, D.P. Small-Cell Carcinomas of the Gastrointestinal Tract: A Review. J. Clin. Oncol. 2004, 22, 2730–2739. [Google Scholar] [CrossRef]
- Cicin, I.; Karagol, H.; Uzunoglu, S.; Uygun, K.; Usta, U.; Kocak, Z.; Caloglu, M.; Saynak, M.; Tokatli, F.; Uzal, C. Extrapulmonary Small-Cell Carcinoma Compared with Small-Cell Lung Carcinoma: A Retrospective Single-Center Study. Cancer 2007, 110, 1068–1076. [Google Scholar] [CrossRef] [PubMed]
- Alese, O.B.; Jiang, R.; Shaib, W.; Wu, C.; Akce, M.; Behera, M.; El-Rayes, B.F. High-Grade Gastrointestinal Neuroendocrine Carcinoma Management and Outcomes: A National Cancer Database Study. Oncologist 2019, 24, 911–920. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sorbye, H.; Welin, S.; Langer, S.W.; Vestermark, L.W.; Holt, N.; Osterlund, P.; Dueland, S.; Hofsli, E.; Guren, M.G.; Ohrling, K.; et al. Predictive and Prognostic Factors for Treatment and Survival in 305 Patients with Advanced Gastrointestinal Neuroendocrine Carcinoma (WHO G3): The NORDIC NEC Study. Ann. Oncol. 2013, 24, 152–160. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.D.; Reidy, D.L.; Goodman, K.A.; Shia, J.; Nash, G.M. A Retrospective Review of 126 High-Grade Neuroendocrine Carcinomas of the Colon and Rectum. Ann. Surg. Oncol. 2014, 21, 2956–2962. [Google Scholar] [CrossRef]
- Meijer, W.G.; Kema, I.P.; Volmer, M.; Willemse, P.H.; de Vries, E.G. Discriminating Capacity of Indole Markers in the Diagnosis of Carcinoid Tumors. Clin. Chem. 2000, 46, 1588–1596. [Google Scholar] [CrossRef] [Green Version]
- Johnson, P.W.M.; Joel, S.P.; Love, S.; Butcher, M.; Pandian, M.R.; Squires, L.; Wrigley, P.F.M.; Slevin, M.L. Tumour Markers for Prediction of Survival and Monitoring of Remission in Small Cell Lung Cancer. Br. J. Cancer 1993, 67, 760–766. [Google Scholar] [CrossRef] [Green Version]
- Baudin, E.; Gigliotti, A.; Ducreux, M.; Ropers, J.; Comoy, E.; Sabourin, J.C.; Bidart, J.M.; Cailleux, A.F.; Bonacci, R.; Ruffié, P.; et al. Neuron-Specific Enolase and Chromogranin A as Markers of Neuroendocrine Tumours. Br. J. Cancer 1998, 78, 1102–1107. [Google Scholar] [CrossRef] [PubMed]
- Lv, Y.; Han, X.; Zhang, C.; Fang, Y.; Pu, N.; Ji, Y.; Wang, D.; Xuefeng, X.; Lou, W. Combined Test of Serum CgA and NSE Improved the Power of Prognosis Prediction of NF-PNETs. Endocr. Connect. 2018, 7, 169–178. [Google Scholar] [CrossRef] [Green Version]
- Raj, N.; Valentino, E.; Capanu, M.; Tang, L.H.; Basturk, O.; Untch, B.R.; Allen, P.J.; Klimstra, D.S.; Reidy-Lagunes, D. Treatment Response and Outcomes of Grade 3 Pancreatic Neuroendocrine Neoplasms Based on Morphology: Well Differentiated Versus Poorly Differentiated. Pancreas 2017, 46, 296–301. [Google Scholar] [CrossRef]
- Milione, M.; Maisonneuve, P.; Spada, F.; Pellegrinelli, A.; Spaggiari, P.; Albarello, L.; Pisa, E.; Barberis, M.; Vanoli, A.; Buzzoni, R.; et al. The Clinicopathologic Heterogeneity of Grade 3 Gastroenteropancreatic Neuroendocrine Neoplasms: Morphological Differentiation and Proliferation Identify Different Prognostic Categories. Neuroendocrinology 2017, 104, 85–93. [Google Scholar] [CrossRef]
- Sorbye, H.; Strosberg, J.; Baudin, E.; Klimstra, D.S.; Yao, J.C. Gastroenteropancreatic High-Grade Neuroendocrine Carcinoma. Cancer 2014, 120, 2814–2823. [Google Scholar] [CrossRef]
- Mitry, E.; Baudin, E.; Ducreux, M.; Sabourin, J.C.; Rufie, P.; Aparicio, T.; Aparicio, T.; Lasser, P.; Elias, D.; Duvillard, P.; et al. Treatment of Poorly Differentiated Neuroendocrine Tumours with Etoposide and Cisplatin. Br. J. Cancer 1999, 81, 1351–1355. [Google Scholar] [CrossRef] [Green Version]
- Iwasa, S.; Morizane, C.; Okusaka, T.; Ueno, H.; Ikeda, M.; Kondo, S.; Tanaka, T.; Nakachi, K.; Mitsunaga, S.; Kojima, Y.; et al. Cisplatin and Etoposide as First-Line Chemotherapy for Poorly Differentiated Neuroendocrine Carcinoma of the Hepatobiliary Tract and Pancreas. Jpn. J. Clin. Oncol. 2010, 40, 313–318. [Google Scholar] [CrossRef] [Green Version]
- Moertel, C.G.; Kvols, L.K.; O’Connell, M.J.; Rubin, J. Treatment of Neuroendocrine Carcinomas with Combined Etoposide and Cisplatin. Evidence of Major Therapeutic Activity in the Anaplastic Variants of These Neoplasms. Cancer 1991, 68, 227–232. [Google Scholar] [CrossRef]
- Yamaguchi, T.; Machida, N.; Morizane, C.; Kasuga, A.; Takahashi, H.; Sudo, K.; Nishina, T.; Tobimatsu, K.; Ishido, K.; Furuse, J.; et al. Multicenter Retrospective Analysis of Systemic Chemotherapy for Advanced Neuroendocrine Carcinoma of the Digestive System. Cancer Sci. 2014, 105, 1176–1181. [Google Scholar] [CrossRef]
- Lamarca, A.; Walter, T.; Pavel, M.; Borbath, I.; Freis, P.; Nuñez, B.; Childs, A.; McNamara, M.G.; Hubner, R.A.; Garcia-Carbonero, R.; et al. Design and Validation of the GI-NEC Score to Prognosticate Overall Survival in Patients With High-Grade Gastrointestinal Neuroendocrine Carcinomas. J. Natl. Cancer Inst. 2017, 109, djw227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sundin, A.; Arnold, R.; Baudin, E.; Cwikla, J.B.; Eriksson, B.; Fanti, S.; Fazio, N.; Giammarile, F.; Hicks, R.J.; Kjaer, A.; et al. ENETS Consensus Guidelines for the Standards of Care in Neuroendocrine Tumors: Radiological, Nuclear Medicine & Hybrid Imaging. Neuroendocrinology 2017, 105, 212–244. [Google Scholar] [PubMed]
- Pavel, M.; Öberg, K.; Falconi, M.; Krenning, E.P.; Sundin, A.; Perren, A.; Berruti, A.; ESMO Guidelines Committee. Electronic address: [email protected] Gastroenteropancreatic Neuroendocrine Neoplasms: ESMO Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up. Ann. Oncol. 2020, 31, 844–860. [Google Scholar] [CrossRef] [PubMed]
- Guo, C.; Chen, X.; Xiao, W.; Wang, Q.; Sun, K.; Wang, Z. Pancreatic Neuroendocrine Neoplasms at Magnetic Resonance Imaging: Comparison between Grade 3 and Grade 1/2 Tumors. Onco Targets Ther. 2017, 10, 1465–1474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guo, C.; Zhuge, X.; Wang, Z.; Wang, Q.; Sun, K.; Feng, Z.; Chen, X. Textural Analysis on Contrast-Enhanced CT in Pancreatic Neuroendocrine Neoplasms: Association with WHO Grade. Abdom. Radiol. 2019, 44, 576–585. [Google Scholar] [CrossRef] [PubMed]
- Canellas, R.; Burk, K.S.; Parakh, A.; Sahani, D.V. Prediction of Pancreatic Neuroendocrine Tumor Grade Based on CT Features and Texture Analysis. AJR Am. J. Roentgenol. 2018, 210, 341–346. [Google Scholar] [CrossRef]
- Azoulay, A.; Cros, J.; Vullierme, M.-P.; de Mestier, L.; Couvelard, A.; Hentic, O.; Ruszniewski, P.; Sauvanet, A.; Vilgrain, V.; Ronot, M. Morphological Imaging and CT Histogram Analysis to Differentiate Pancreatic Neuroendocrine Tumor Grade 3 from Neuroendocrine Carcinoma. Diagn. Interv. Imaging 2020, 101, 821–830. [Google Scholar] [CrossRef] [PubMed]
- Bartoli, M.; Barat, M.; Dohan, A.; Gaujoux, S.; Coriat, R.; Hoeffel, C.; Cassinotto, C.; Chassagnon, G.; Soyer, P. CT and MRI of Pancreatic Tumors: An Update in the Era of Radiomics. Jpn. J. Radiol. 2020, 38, 1111–1124. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Carbonero, R.; Sorbye, H.; Baudin, E.; Raymond, E.; Wiedenmann, B.; Niederle, B.; Sedlackova, E.; Toumpanakis, C.; Anlauf, M.; Cwikla, J.B.; et al. ENETS Consensus Guidelines for High-Grade Gastroenteropancreatic Neuroendocrine Tumors and Neuroendocrine Carcinomas. Neuroendocrinology 2016, 103, 186–194. [Google Scholar] [CrossRef] [Green Version]
- Binderup, T.; Knigge, U.; Loft, A.; Mortensen, J.; Pfeifer, A.; Federspiel, B.; Hansen, C.P.; Hojgaard, L.; Kjaer, A. Functional Imaging of Neuroendocrine Tumors: A Head-to-Head Comparison of Somatostatin Receptor Scintigraphy, 123I-MIBG Scintigraphy, and 18F-FDG PET. J. Nucl. Med. 2010, 51, 704–712. [Google Scholar] [CrossRef] [Green Version]
- Zhang, P.; Yu, J.; Li, J.; Shen, L.; Li, N.; Zhu, H.; Zhai, S.; Zhang, Y.; Yang, Z.; Lu, M. Clinical and Prognostic Value of PET/CT Imaging with Combination of 68Ga-DOTATATE and 18F-FDG in Gastroenteropancreatic Neuroendocrine Neoplasms. Contrast Media Mol. Imaging 2018, 2018, 2340389. [Google Scholar] [CrossRef] [Green Version]
- Binderup, T.; Knigge, U.; Loft, A.; Federspiel, B.; Kjaer, A. 18F-Fluorodeoxyglucose Positron Emission Tomography Predicts Survival of Patients with Neuroendocrine Tumors. Clin. Cancer Res. 2010, 16, 978–985. [Google Scholar] [CrossRef] [Green Version]
- Chan, D.L.; Pavlakis, N.; Schembri, G.P.; Bernard, E.J.; Hsiao, E.; Hayes, A.; Barnes, T.; Diakos, C.; Khasraw, M.; Samra, J.; et al. Dual Somatostatin Receptor/FDG PET/CT Imaging in Metastatic Neuroendocrine Tumours: Proposal for a Novel Grading Scheme with Prognostic Significance. Theranostics 2017, 7, 1149–1158. [Google Scholar] [CrossRef]
- Kim, H.; An, S.; Lee, K.; Ahn, S.; Park, D.Y.; Kim, J.-H.; Kang, D.-W.; Kim, M.-J.; Chang, M.S.; Jung, E.S.; et al. Pancreatic High-Grade Neuroendocrine Neoplasms in the Korean Population: A Multicenter Study. Cancer Res. Treat. 2020, 52, 263–276. [Google Scholar] [CrossRef] [Green Version]
- Sigel, C.S.; Krauss Silva, V.W.; Reid, M.D.; Chhieng, D.; Basturk, O.; Sigel, K.M.; Daniel, T.D.; Klimstra, D.S.; Tang, L.H. Well Differentiated Grade 3 Pancreatic Neuroendocrine Tumors Compared with Related Neoplasms: A Morphologic Study: PanNET Morphologic Comparison. Cancer Cytopathol. 2018, 126, 326–335. [Google Scholar] [CrossRef] [PubMed]
- Faggiano, A.; Sabourin, J.-C.; Ducreux, M.; Lumbroso, J.; Duvillard, P.; Leboulleux, S.; Dromain, C.; Colao, A.; Schlumberger, M.; Baudin, E. Pulmonary and Extrapulmonary Poorly Differentiated Large Cell Neuroendocrine Carcinomas. Cancer 2007, 110, 265–274. [Google Scholar] [CrossRef] [PubMed]
- Welin, S.; Sorbye, H.; Sebjornsen, S.; Knappskog, S.; Busch, C.; Oberg, K. Clinical Effect of Temozolomide-Based Chemotherapy in Poorly Differentiated Endocrine Carcinoma after Progression on First-Line Chemotherapy. Cancer 2011, 117, 4617–4622. [Google Scholar] [CrossRef] [PubMed]
- Weynand, B.; Borbath, I.; Bernard, V.; Sempoux, C.; Gigot, J.-F.; Hubert, C.; Lannoy, V.; Deprez, P.H.; Jouret-Mourin, A. Pancreatic Neuroendocrine Tumour Grading on Endoscopic Ultrasound-Guided Fine Needle Aspiration: High Reproducibility and Inter-Observer Agreement of the Ki-67 Labelling Index. Cytopathology 2014, 25, 389–395. [Google Scholar] [CrossRef] [PubMed]
- Reid, M.D.; Bagci, P.; Ohike, N.; Saka, B.; Erbarut Seven, I.; Dursun, N.; Balci, S.; Gucer, H.; Jang, K.-T.; Tajiri, T.; et al. Calculation of the Ki67 Index in Pancreatic Neuroendocrine Tumors: A Comparative Analysis of Four Counting Methodologies. Mod. Pathol. 2015, 28, 686–694. [Google Scholar] [CrossRef]
- Shi, H.; Chen, L.; Zhang, Q.; Lin, Y.; Jiang, C.; Yao, H.; Hou, X.; Chen, M.; Lin, R.; Chen, J. Concordance Between the Ki-67 Index Cutoff Value of 55% and Differentiation in Neuroendocrine Tumor and Neuroendocrine Carcinoma in Grade 3 Pancreatic Neuroendocrine Neoplasms. Pancreas 2020, 49, 1378–1382. [Google Scholar] [CrossRef]
- Takizawa, N.; Ohishi, Y.; Hirahashi, M.; Takahashi, S.; Nakamura, K.; Tanaka, M.; Oki, E.; Takayanagi, R.; Oda, Y. Molecular Characteristics of Colorectal Neuroendocrine Carcinoma; Similarities with Adenocarcinoma Rather than Neuroendocrine Tumor. Hum. Pathol. 2015, 46, 1890–1900. [Google Scholar] [CrossRef]
- Girardi, D.M.; Silva, A.C.B.; Rêgo, J.F.M.; Coudry, R.A.; Riechelmann, R.P. Unraveling Molecular Pathways of Poorly Differentiated Neuroendocrine Carcinomas of the Gastroenteropancreatic System: A Systematic Review. Cancer Treat. Rev. 2017, 56, 28–35. [Google Scholar] [CrossRef]
- Woischke, C.; Schaaf, C.W.; Yang, H.-M.; Vieth, M.; Veits, L.; Geddert, H.; Märkl, B.; Stömmer, P.; Schaeffer, D.F.; Frölich, M.; et al. In-Depth Mutational Analyses of Colorectal Neuroendocrine Carcinomas with Adenoma or Adenocarcinoma Components. Mod. Pathol. 2017, 30, 95–103. [Google Scholar] [CrossRef]
- Tang, L.H.; Untch, B.R.; Reidy, D.L.; O’Reilly, E.; Dhall, D.; Jih, L.; Basturk, O.; Allen, P.J.; Klimstra, D.S. Well-Differentiated Neuroendocrine Tumors with a Morphologically Apparent High-Grade Component: A Pathway Distinct from Poorly Differentiated Neuroendocrine Carcinomas. Clin. Cancer Res. 2016, 22, 1011–1017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uccella, S.; La Rosa, S.; Metovic, J.; Marchiori, D.; Scoazec, J.-Y.; Volante, M.; Mete, O.; Papotti, M. Genomics of High-Grade Neuroendocrine Neoplasms: Well-Differentiated Neuroendocrine Tumor with High-Grade Features (G3 NET) and Neuroendocrine Carcinomas (NEC) of Various Anatomic Sites. Endocr. Pathol. 2021, 32, 192–210. [Google Scholar] [CrossRef]
- Koh, J.; Nam, S.K.; Kwak, Y.; Kim, G.; Kim, K.-K.; Lee, B.-C.; Ahn, S.-H.; Park, D.J.; Kim, H.-H.; Park, K.U.; et al. Comprehensive Genetic Features of Gastric Mixed Adenoneuroendocrine Carcinomas and Pure Neuroendocrine Carcinomas. J. Pathol. 2021, 253, 94–105. [Google Scholar] [CrossRef]
- Yachida, S.; Vakiani, E.; White, C.M.; Zhong, Y.; Saunders, T.; Morgan, R.; de Wilde, R.F.; Maitra, A.; Hicks, J.; Demarzo, A.M.; et al. Small Cell and Large Cell Neuroendocrine Carcinomas of the Pancreas Are Genetically Similar and Distinct from Well-Differentiated Pancreatic Neuroendocrine Tumors. Am. J. Surg. Pathol. 2012, 36, 173–184. [Google Scholar] [CrossRef]
- Jesinghaus, M.; Konukiewitz, B.; Keller, G.; Kloor, M.; Steiger, K.; Reiche, M.; Penzel, R.; Endris, V.; Arsenic, R.; Hermann, G.; et al. Colorectal Mixed Adenoneuroendocrine Carcinomas and Neuroendocrine Carcinomas Are Genetically Closely Related to Colorectal Adenocarcinomas. Mod. Pathol. 2017, 30, 610–619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diaz, L.A.; Bardelli, A. Liquid Biopsies: Genotyping Circulating Tumor DNA. J. Clin. Oncol. 2014, 32, 579–586. [Google Scholar] [CrossRef]
- Gerard, L.; Garcia, J.; Gauthier, A.; Lopez, J.; Durand, A.; Hervieu, V.; Lemelin, A.; Chardon, L.; Landel, V.; Gibert, B.; et al. CtDNA in Neuroendocrine Carcinoma of Gastroenteropancreatic Origin or of Unknown Primary: The CIRCAN-NEC Pilot Study. Neuroendocrinology 2020. [Google Scholar] [CrossRef]
- Shafqat, H.; Ali, S.; Salhab, M.; Olszewski, A.J. Survival of Patients with Neuroendocrine Carcinoma of the Colon and Rectum: A Population-Based Analysis. Dis. Colon Rectum 2015, 58, 294–303. [Google Scholar] [CrossRef] [PubMed]
- Yachida, S.; Matsushita, K.; Usuki, H.; Wanibuchi, H.; Maeba, T.; Maeta, H. Long-Term Survival after Resection for Small Cell Carcinoma of the Esophagus. Ann. Thorac. Surg. 2001, 72, 596–597. [Google Scholar] [CrossRef]
- Nishimaki, T.; Suzuki, T.; Nakagawa, S.; Watanabe, K.; Aizawa, K.; Hatakeyama, K. Tumor Spread and Outcome of Treatment in Primary Esophageal Small Cell Carcinoma. J. Surg. Oncol. 1997, 64, 130–134. [Google Scholar] [CrossRef]
- Basturk, O.; Tang, L.; Hruban, R.H.; Adsay, V.; Yang, Z.; Krasinskas, A.M.; Vakiani, E.; La Rosa, S.; Jang, K.-T.; Frankel, W.L.; et al. Poorly Differentiated Neuroendocrine Carcinomas of the Pancreas: A Clinicopathologic Analysis of 44 Cases. Am. J. Surg. Pathol. 2014, 38, 437–447. [Google Scholar] [CrossRef]
- Haugvik, S.-P.; Janson, E.T.; Österlund, P.; Langer, S.W.; Falk, R.S.; Labori, K.J.; Vestermark, L.W.; Grønbæk, H.; Gladhaug, I.P.; Sorbye, H. Surgical Treatment as a Principle for Patients with High-Grade Pancreatic Neuroendocrine Carcinoma: A Nordic Multicenter Comparative Study. Ann. Surg. Oncol. 2016, 23, 1721–1728. [Google Scholar] [CrossRef]
- Shen, C.; Chen, H.; Chen, H.; Yin, Y.; Han, L.; Chen, J.; Tang, S.; Yin, X.; Zhou, Z.; Zhang, B.; et al. Surgical Treatment and Prognosis of Gastric Neuroendocrine Neoplasms: A Single-Center Experience. BMC Gastroenterol. 2016, 16, 111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Casas, F.; Ferrer, F.; Farrus, B.; Casals, J.; Biete, A. Primary Small Cell Carcinoma of the Esophagus: A Review of the Literature with Emphasis on Therapy and Prognosis. Cancer 1997, 80, 1366–1372. [Google Scholar] [CrossRef]
- Pellat, A.; Walter, T.; Augustin, J.; Hautefeuille, V.; Hentic, O.; Do Cao, C.; Lièvre, A.; Coriat, R.; Hammel, P.; Dubreuil, O.; et al. Chemotherapy in Resected Neuroendocrine Carcinomas of the Digestive Tract: A National Study from the French Group of Endocrine Tumours (GTE). Neuroendocrinology 2019, 110, 404–412. [Google Scholar] [CrossRef]
- Pignon, J.P.; Arriagada, R.; Ihde, D.C.; Johnson, D.H.; Perry, M.C.; Souhami, R.L.; Brodin, O.; Joss, R.A.; Kies, M.S.; Lebeau, B.; et al. A Meta-Analysis of Thoracic Radiotherapy for Small-Cell Lung Cancer. N. Engl. J. Med. 1992, 327, 1618–1624. [Google Scholar] [CrossRef]
- Sørensen, M.; Pijls-Johannesma, M.; Felip, E.; ESMO Guidelines Working Group. Small-Cell Lung Cancer: ESMO Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up. Ann. Oncol. 2010, 21 (Suppl. 5), v120–v125. [Google Scholar] [CrossRef] [PubMed]
- Ku, G.Y.; Minsky, B.D.; Rusch, V.W.; Bains, M.; Kelsen, D.P.; Ilson, D.H. Small-Cell Carcinoma of the Esophagus and Gastroesophageal Junction: Review of the Memorial Sloan-Kettering Experience. Ann. Oncol. 2008, 19, 533–537. [Google Scholar] [CrossRef] [PubMed]
- Brieau, B.; Lepere, C.; Walter, T.; Lecomte, T.; Guimbaud, R.; Manfredi, S.; Tougeron, D.; Desseigne, F.; Lourenco, N.; Afchain, P.; et al. Radiochemotherapy Versus Surgery in Nonmetastatic Anorectal Neuroendocrine Carcinoma: A Multicenter Study by the Association Des Gastro-Enterologues Oncologues. Medicine 2015, 94, e1864. [Google Scholar] [CrossRef]
- Yoshida, T.; Hijioka, S.; Hosoda, W.; Ueno, M.; Furukawa, M.; Kobayashi, N.; Ikeda, M.; Ito, T.; Kodama, Y.; Morizane, C.; et al. Surgery for Pancreatic Neuroendocrine Tumor G3 and Carcinoma G3 Should Be Considered Separately. Ann. Surg. Oncol. 2019, 26, 1385–1393. [Google Scholar] [CrossRef] [PubMed]
- Zappa, M.; Abdel-Rehim, M.; Hentic, O.; Vullierme, M.-P.; Ruszniewski, P.; Vilgrain, V. Liver-Directed Therapies in Liver Metastases from Neuroendocrine Tumors of the Gastrointestinal Tract. Target. Oncol. 2012, 7, 107–116. [Google Scholar] [CrossRef] [PubMed]
- de Baere, T.; Deschamps, F.; Tselikas, L.; Ducreux, M.; Planchard, D.; Pearson, E.; Berdelou, A.; Leboulleux, S.; Elias, D.; Baudin, E. GEP-NETS Update: Interventional Radiology: Role in the Treatment of Liver Metastases from GEP-NETs. Eur. J. Endocrinol. 2015, 172, R151–R166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barat, M.; Cottereau, A.-S.; Kedra, A.; Dermine, S.; Palmieri, L.-J.; Coriat, R.; Dautry, R.; Tselikas, L.; Soyer, P.; Dohan, A. The Role of Interventional Radiology for the Treatment of Hepatic Metastases from Neuroendocrine Tumor: An Updated Review. J. Clin. Med. 2020, 9, 2302. [Google Scholar] [CrossRef] [PubMed]
- Du, S.; Ni, J.; Weng, L.; Ma, F.; Li, S.; Wang, W.; Sang, X.; Lu, X.; Zhong, S.; Mao, Y. Aggressive Locoregional Treatment Improves the Outcome of Liver Metastases from Grade 3 Gastroenteropancreatic Neuroendocrine Tumors. Medicin 2015, 94, e1429. [Google Scholar] [CrossRef] [PubMed]
- Nakano, K.; Takahashi, S.; Yuasa, T.; Nishimura, N.; Mishima, Y.; Sakajiri, S.; Yokoyama, M.; Tsuyama, N.; Ishikawa, Y.; Hatake, K. Feasibility and Efficacy of Combined Cisplatin and Irinotecan Chemotherapy for Poorly Differentiated Neuroendocrine Carcinomas. Jpn. J. Clin. Oncol. 2012, 42, 697–703. [Google Scholar] [CrossRef] [Green Version]
- Hainsworth, J.D.; Spigel, D.R.; Litchy, S.; Greco, F.A. Phase II Trial of Paclitaxel, Carboplatin, and Etoposide in Advanced Poorly Differentiated Neuroendocrine Carcinoma: A Minnie Pearl Cancer Research Network Study. J. Clin. Oncol. 2006, 24, 3548–3554. [Google Scholar] [CrossRef]
- Mani, M.A.; Shroff, R.T.; Jacobs, C.; Wolff, R.A.; Ajani, J.A.; Yao, J.C.; Phan, A.T. A Phase II Study of Irinotecan and Cisplatin for Metastatic or Unresectable High Grade Neuroendocrine Carcinoma. J. Clin. Oncol. 2008, 26, 15550. [Google Scholar] [CrossRef]
- Lu, Z.H.; Li, J.; Lu, M.; Zhang, X.T.; Li, J.; Zhou, J.; Wang, X.C.; Gong, J.F.; Gao, J.; Li, Y.; et al. Feasibility and Efficacy of Combined Cisplatin plus Irinotecan Chemotherapy for Gastroenteropancreatic Neuroendocrine Carcinomas. Med. Oncol. 2013, 30, 664. [Google Scholar] [CrossRef]
- Ramella Munhoz, R.; de Mendonca Rego, J.F.; de Celis Ferrari, A.R.; Ignez Braghiroli, M.; Mendonca Bariani, G.; Marcelo Hoff, P.; Perego Costa, F.; Eduardo Flesch Pfiffer, T.; Riechelmann, R. Combination of Irinotecan and a Platinum Agent for Poorly Differentiated Neuroendocrine Carcinomas. Rare tumors 2013, 5, e39. [Google Scholar] [CrossRef]
- Okuma, H.S.; Iwasa, S.; Shoji, H.; Takashima, A.; Okita, N.; Honma, Y.; Kato, K.; Hamaguchi, T.; Yamada, Y.; Shimada, Y. Irinotecan plus Cisplatin in Patients with Extensive-Disease Poorly Differentiated Neuroendocrine Carcinoma of the Esophagus. Anticancer. Res. 2014, 34, 5037–5041. [Google Scholar]
- Olsen, I.H.; Sorensen, J.B.; Federspiel, B.; Kjaer, A.; Hansen, C.P.; Knigge, U.; Langer, S.W. Temozolomide as Second or Third Line Treatment of Patients with Neuroendocrine Carcinomas. Sci. World J. 2012, 2012, 170496. [Google Scholar] [CrossRef] [Green Version]
- Sahu, A.; Jefford, M.; Lai-Kwon, J.; Thai, A.; Hicks, R.J.; Michael, M. CAPTEM in Metastatic Well-Differentiated Intermediate to High Grade Neuroendocrine Tumors: A Single Centre Experience. J. Oncol. 2019, 2019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bajetta, E.; Catena, L.; Procopio, G.; De Dosso, S.; Bichisao, E.; Ferrari, L.; Martinetti, A.; Platania, M.; Verzoni, E.; Formisano, B.; et al. Are Capecitabine and Oxaliplatin (XELOX) Suitable Treatments for Progressing Low-Grade and High-Grade Neuroendocrine Tumours? Cancer Chemother. Pharmacol. 2007, 59, 637–642. [Google Scholar] [CrossRef]
- Hentic, O.; Hammel, P.; Couvelard, A.; Rebours, V.; Zappa, M.; Palazzo, M.; Maire, F.; Goujon, G.; Gillet, A.; Levy, P.; et al. FOLFIRI Regimen: An Effective Second-Line Chemotherapy after Failure of Etoposide-Platinum Combination in Patients with Neuroendocrine Carcinomas Grade 3. Endocr. Relat. Cancer 2012, 19, 751–757. [Google Scholar] [CrossRef] [Green Version]
- Hadoux, J.; Malka, D.; Planchard, D.; Scoazec, J.Y.; Caramella, C.; Guigay, J.; Boige, V.; Leboulleux, S.; Burtin, P.; Berdelou, A.; et al. Post-First-Line FOLFOX Chemotherapy for Grade 3 Neuroendocrine Carcinoma. Endocr. Relat. Cancer 2015, 22, 289–298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sorbye, H.; Kong, G.; Grozinsky-Glasberg, S. PRRT in High-Grade Gastroenteropancreatic Neuroendocrine Neoplasms (WHO G3). Endocr. Relat. Cancer 2020, 27, R67–R77. [Google Scholar] [CrossRef] [PubMed]
- Ostwal, V.; Basu, S.; Bhargava, P.; Shah, M.; Parghane, R.V.; Srinivas, S.; Chaudhari, V.; Bhandare, M.S.; Shrikhande, S.V.; Ramaswamy, A. Capecitabine-Temozolomide (CAPTEM) in Advanced Grade 2 and Grade 3 Neuroendocrine Neoplasms (NENs)—Benefits of Chemotherapy in NENs with Significant 18FDG Uptake. Neuroendocrinology 2020. [Google Scholar] [CrossRef]
- Raymond, E.; Dahan, L.; Raoul, J.-L.; Bang, Y.-J.; Borbath, I.; Lombard-Bohas, C.; Valle, J.; Metrakos, P.; Smith, D.; Vinik, A.; et al. Sunitinib Malate for the Treatment of Pancreatic Neuroendocrine Tumors. N. Engl. J. Med. 2011, 364, 501–513. [Google Scholar] [CrossRef] [Green Version]
- Yao, J.C.; Shah, M.H.; Ito, T.; Bohas, C.L.; Wolin, E.M.; Van Cutsem, E.; Hobday, T.J.; Okusaka, T.; Capdevila, J.; de Vries, E.G.; et al. Everolimus for Advanced Pancreatic Neuroendocrine Tumors. N. Engl. J. Med. 2011, 364, 514–523. [Google Scholar] [CrossRef] [Green Version]
- Yao, J.C.; Fazio, N.; Singh, S.; Buzzoni, R.; Carnaghi, C.; Wolin, E.; Tomasek, J.; Raderer, M.; Lahner, H.; Voi, M.; et al. Everolimus for the Treatment of Advanced, Non-Functional Neuroendocrine Tumours of the Lung or Gastrointestinal Tract (RADIANT-4): A Randomised, Placebo-Controlled, Phase 3 Study. Lancet 2016, 387, 968–977. [Google Scholar] [CrossRef]
- Pellat, A.; Netter, J.; Perkins, G.; Cohen, R.; Coulet, F.; Parc, Y.; Svrcek, M.; Duval, A.; André, T. Lynch syndrome: What is new? Bull. Cancer 2019, 106, 647–655. [Google Scholar] [CrossRef] [PubMed]
- Panzuto, F.; Rinzivillo, M.; Spada, F.; Antonuzzo, L.; Ibrahim, T.; Campana, D.; Fazio, N.; Delle Fave, G. Everolimus in Pancreatic Neuroendocrine Carcinomas G3. Pancreas 2017, 46, 302–305. [Google Scholar] [CrossRef] [PubMed]
- Weber, M.M.; Fottner, C. Immune Checkpoint Inhibitors in the Treatment of Patients with Neuroendocrine Neoplasia. Oncol. Res. Treat. 2018, 41, 306–312. [Google Scholar] [CrossRef] [PubMed]
- Nghiem, P.T.; Bhatia, S.; Lipson, E.J.; Kudchadkar, R.R.; Miller, N.J.; Annamalai, L.; Berry, S.; Chartash, E.K.; Daud, A.; Fling, S.P.; et al. PD-1 Blockade with Pembrolizumab in Advanced Merkel-Cell Carcinoma. N. Engl. J. Med. 2016, 374, 2542–2552. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, H.L.; Russell, J.; Hamid, O.; Bhatia, S.; Terheyden, P.; D’Angelo, S.P.; Shih, K.C.; Lebbé, C.; Linette, G.P.; Milella, M.; et al. Avelumab in Patients with Chemotherapy-Refractory Metastatic Merkel Cell Carcinoma: A Multicentre, Single-Group, Open-Label, Phase 2 Trial. Lancet Oncol. 2016, 17, 1374–1385. [Google Scholar] [CrossRef] [Green Version]
- Vijayvergia, N.; Dasari, A.; Deng, M.; Litwin, S.; Al-Toubah, T.; Alpaugh, R.K.; Dotan, E.; Hall, M.J.; Ross, N.M.; Runyen, M.M.; et al. Pembrolizumab Monotherapy in Patients with Previously Treated Metastatic High-Grade Neuroendocrine Neoplasms: Joint Analysis of Two Prospective, Non-Randomised Trials. Br. J. Cancer 2020, 122, 1309–1314. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Well-Differentiated NEN 1 | Ki−67 Index (%) | Mitotic Index (HPF 2) |
|---|---|---|
| NET 3 G-1 (low-grade) | <3 | <2/10 |
| NET G-2 (intermediate-grade) | 3–20 | 2–20/10 |
| NET G-3 (high-grade) | >20 | >20/10 |
| Poorly differentiated NEN | ||
| NEC 4 G-3 Small-cell type, Large-cell type | >20 | >20/10 |
| Mixed Neuroendocrine–nonneuroendocrine neoplasm (MiNEN) | ||
| Study (First Author, Year) | Tumor Site | Chemotherapy Regimen | Patients (Number) | Response Rate (%) | Median OS 1 (Months) |
|---|---|---|---|---|---|
| Moertel, 1991 [36] | Digestive Lung Unknown | Cisplatin/etoposide | 18 | 67 | 19 |
| Mitry, 1999 [34] | Digestive Lung Head and neck Uterus Unknown | Cisplatin/etoposide | 41 | 41.5 | 15 |
| Hainsworth, 2006 [86] | Digestive Lung Skin Thyroid Endometrium Prostate Sinus Unknown | Paclitaxel/carboplatin/ etoposide | 78 | 42 | 14.5 |
| Mani, 2008 [87] | NA | Cisplatin/irinotecan | 20 | 58 | NA 2 |
| Iwasa, 2010 [35] | Digestive (hepatobiliary tract, pancreas) | Cisplatin/etoposide | 21 | 14 | 5.8 |
| Nakano, 2012 [85] | Digestive Urinary tract Head, neck Gynecologic Unknown | Cisplatin/irinotecan | 44 | 50 | 16 |
| Sorbye, 2013 [25] | Digestive | Cisplatin/etoposide | 129 | 31 | 12 |
| Carboplatin/etoposide | 67 | 30 | 11 | ||
| Carboplatin/etoposide/ | 28 | 44 | 10 | ||
| Vincristine | |||||
| Other | 28 | NA | NA | ||
| Lu, 2013 [88] | Digestive | Cisplatin/irinotecan | 16 | 51.1 | 10.6 |
| Munhoz, 2013 [89] | Digestive Nasopharynx Prostate Unknown | Cisplatin or caboplatin/irinotecan | 28 | 46.4 | 11.7 |
| Yamaguchi, 2014 [37] | Digestive | Cisplatin/etoposide Cisplatin/irinotecan | 46 160 | 28 50 | 7.3 13 |
| Okuma, 2014 [90] | Oesophagus | Cisplatin/irinotecan | 12 | 50 | 12.6 |
| Walter, 2017 [21] | Digestive | Cisplatin or caboplatin/etoposide | 152 | 50 | 11.6 |
| Study (First Author, Year) | Tumor Site | Chemotherapy Regimen | Patients (Number) | Response Rate (%) | Median OS 1 (Months) |
|---|---|---|---|---|---|
| Bajetta, 2006 [93] | Digestive Lung Other | Capecitabine/oxaliplatin (XELOX) | 13 | 23 | 5 |
| Welin, 2011 [54] | Digestive Lung Unknown | Temozolomide ± capecitabine ± bevacizumab | 25 | 33 | 22 |
| Olsen, 2012 [91] | Digestive Lung Prostate Kidney Unknown | Temozolomide | 28 | 0 | 3.5 |
| Hentic, 2012 [94] | Digestive | 5-FU/irinotecan (FOLFIRI) | 19 | 31 | 18 |
| Sorbye, 2013 [25] | Digestive | Various combinations (temozolomide-based or taxotere-based) | 100 | 18 | 19 |
| Hadoux, 2015 [95] | Digestive Thoracic Other Unknown | 5-FU/oxaliplatin (FOLFOX) | 20 | 29 | 9.9 |
| Walter, 2017 [21] | Digestive | 5-FU/irinotecan (FOLFIRI) | 72 | 24 | 5.9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pellat, A.; Cottereau, A.S.; Terris, B.; Coriat, R. Neuroendocrine Carcinomas of the Digestive Tract: What Is New? Cancers 2021, 13, 3766. https://doi.org/10.3390/cancers13153766
Pellat A, Cottereau AS, Terris B, Coriat R. Neuroendocrine Carcinomas of the Digestive Tract: What Is New? Cancers. 2021; 13(15):3766. https://doi.org/10.3390/cancers13153766
Chicago/Turabian StylePellat, Anna, Anne Ségolène Cottereau, Benoit Terris, and Romain Coriat. 2021. "Neuroendocrine Carcinomas of the Digestive Tract: What Is New?" Cancers 13, no. 15: 3766. https://doi.org/10.3390/cancers13153766
APA StylePellat, A., Cottereau, A. S., Terris, B., & Coriat, R. (2021). Neuroendocrine Carcinomas of the Digestive Tract: What Is New? Cancers, 13(15), 3766. https://doi.org/10.3390/cancers13153766