
Anthracyclines Strike Back: Rediscovering Non-Pegylated Liposomal Doxorubicin in Current Therapeutic Scenarios of Breast Cancer

 ,
, 
 ,
, 
 , , ,
, , ,  , , , , ,
, , , , ,  ,
, 
 ,
,  , , , and
, , , and  add
Show full author list
add
Show full author list
Abstract
:Simple Summary
Abstract
1. Introduction
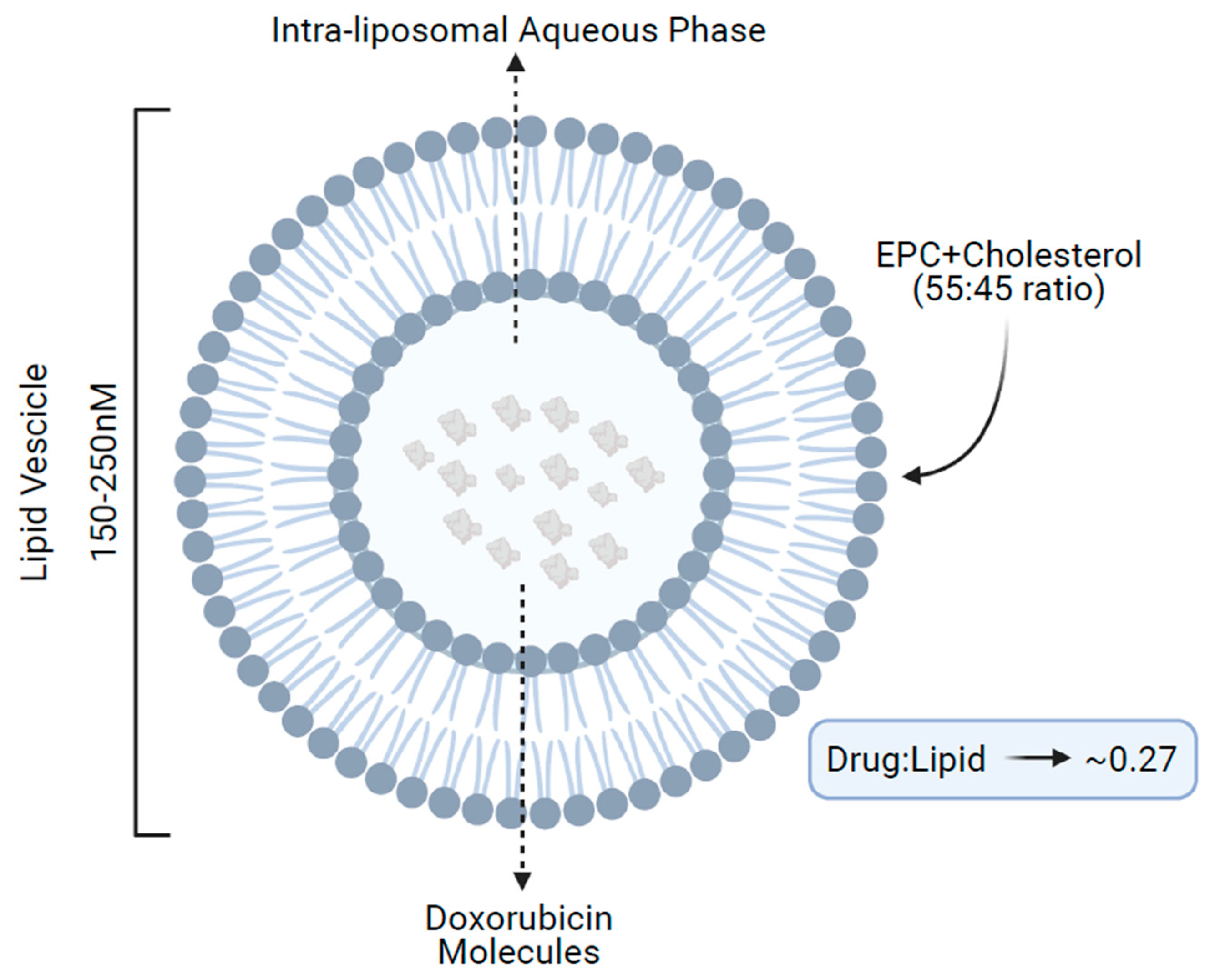
2. Structure and Mechanisms of Action
3. Current Therapeutic Indication, Efficacy, and Toxicity Profile
4. Additional Evidence in Metastatic HER2-Negative Disease
5. The Early-Stage Scenario
6. The HER2+ Disease: A Brief Overview
7. The Positioning of NPLD in the Current Therapeutic Algorithms
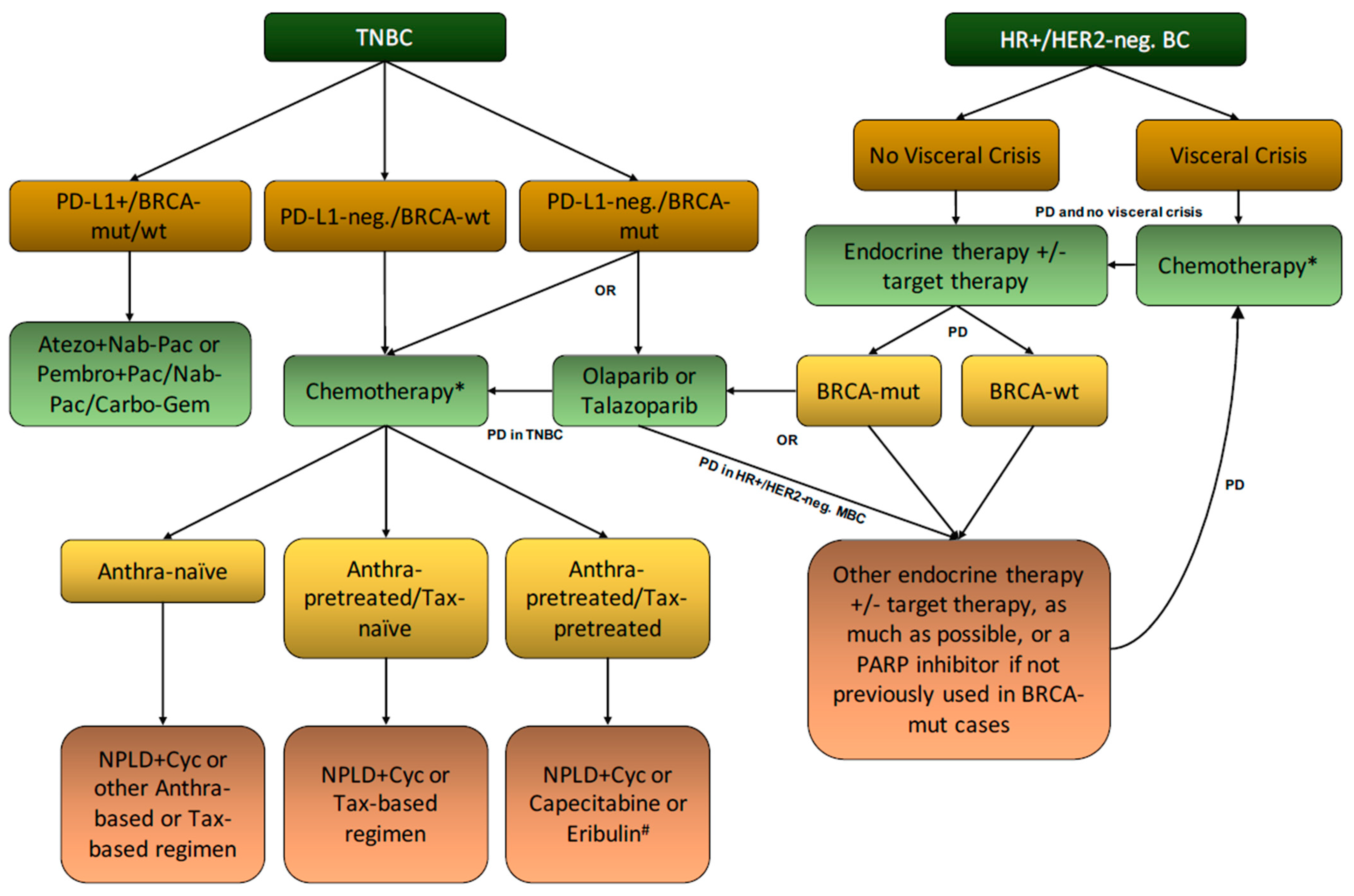
7.1. Metastatic Setting
- The reduced cardiotoxicity potentially allows clinicians to administer higher cumulative doses of doxorubicin if the liposomal formulation is adopted.
- The prescription caveats that limit the use of NPLD + cyclophosphamide to first-line settings and the possibility to still provide patients with very effective taxane-based regimens in the second and subsequent lines (i.e., nab-paclitaxel, paclitaxel, and docetaxel), if not used in the first-line setting.
7.2. Early-Stage Setting, Elderly Patients, and Main Limitations
7.3. Cardiac Monitoring
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cardinale, D.; Iacopo, F.; Cipolla, C.M. Cardiotoxicity of Anthracyclines. Front. Cardiovasc. Med. 2020, 7, 26. [Google Scholar] [CrossRef] [Green Version]
- Arciniegas Calle, M.C.; Sandhu, N.P.; Xia, H.; Cha, S.S.; Pellikka, P.A.; Ye, Z.; Herrmann, J.; Villarraga, H.R. Two-Dimensional Speckle Tracking Echocardiography Predicts Early Subclinical Cardiotoxicity Associated with Anthracycline-Trastuzumab Chemotherapy in Patients with Breast Cancer. BMC Cancer 2018, 18, 1037. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santoro, C.; Arpino, G.; Esposito, R.; Lembo, M.; Paciolla, I.; Cardalesi, C.; de Simone, G.; Trimarco, B.; De Placido, S.; Galderisi, M. 2D and 3D Strain for Detection of Subclinical Anthracycline Cardiotoxicity in Breast Cancer Patients: A Balance with Feasibility. Eur. Heart J. Cardiovasc. Imaging 2017, 18, 930–936. [Google Scholar] [CrossRef]
- Jain, K.K.; Casper, E.S.; Geller, N.L.; Hakes, T.B.; Kaufman, R.J.; Currie, V.; Schwartz, W.; Cassidy, C.; Petroni, G.R.; Young, C.W. A Prospective Randomized Comparison of Epirubicin and Doxorubicin in Patients with Advanced Breast Cancer. J. Clin. Oncol. 1985, 3, 818–826. [Google Scholar] [CrossRef] [PubMed]
- Hortobagyi, G.N.; Yap, H.Y.; Kau, S.W.; Fraschini, G.; Ewer, M.S.; Chawla, S.P.; Benjamin, R.S. A Comparative Study of Doxorubicin and Epirubicin in Patients with Metastatic Breast Cancer. Am. J. Clin. Oncol. 1989, 12, 57–62. [Google Scholar] [CrossRef] [PubMed]
- Perez, D.J.; Harvey, V.J.; Robinson, B.A.; Atkinson, C.H.; Dady, P.J.; Kirk, A.R.; Evans, B.D.; Chapman, P.J. A Randomized Comparison of Single-Agent Doxorubicin and Epirubicin as First-Line Cytotoxic Therapy in Advanced Breast Cancer. J. Clin. Oncol. 1991, 9, 2148–2152. [Google Scholar] [CrossRef] [PubMed]
- Wouters, K.A.; Kremer, L.C.M.; Miller, T.L.; Herman, E.H.; Lipshultz, S.E. Protecting against Anthracycline-Induced Myocardial Damage: A Review of the Most Promising Strategies. Br. J. Haematol. 2005, 131, 561–578. [Google Scholar] [CrossRef] [PubMed]
- Schettini, F.; Giuliano, M.; De Placido, S.; Arpino, G. Nab-Paclitaxel for the Treatment of Triple-Negative Breast Cancer: Rationale, Clinical Data and Future Perspectives. Cancer Treat. Rev. 2016, 50, 129–141. [Google Scholar] [CrossRef] [Green Version]
- Van Dalen, E.C.; Michiels, E.M.; Caron, H.N.; Kremer, L.C. Different Anthracycline Derivates for Reducing Cardiotoxicity in Cancer Patients. Cochrane Database Syst. Rev. 2010, 2010, CD005006. [Google Scholar] [CrossRef]
- Gabizon, A.; Shmeeda, H.; Barenholz, Y. Pharmacokinetics of Pegylated Liposomal Doxorubicin: Review of Animal and Human Studies. Clin. Pharmacokinet. 2003, 42, 419–436. [Google Scholar] [CrossRef] [PubMed]
- Giuliano, M.; Schettini, F.; Rognoni, C.; Milani, M.; Jerusalem, G.; Bachelot, T.; De Laurentiis, M.; Thomas, G.; De Placido, P.; Arpino, G.; et al. Endocrine Treatment versus Chemotherapy in Postmenopausal Women with Hormone Receptor-Positive, HER2-Negative, Metastatic Breast Cancer: A Systematic Review and Network Meta-Analysis. Lancet Oncol. 2019, 20, 1360–1369. [Google Scholar] [CrossRef] [Green Version]
- Rakshitha, V.; Nalini, K.; Sahana, N.; Deepak, P.; Jayashree, N.; Mohith, N.; Divyashree, R. Comparison of Safety and Toxicity of Liposomal versus Conventional Doxorubicin: An Updated Review. Int. J. Basic Clin. Pharmacol. 2019, 8, 1453–1459. [Google Scholar] [CrossRef]
- Bulbake, U.; Doppalapudi, S.; Kommineni, N.; Khan, W. Liposomal Formulations in Clinical Use: An Updated Review. Pharmaceutics 2017, 9, 12. [Google Scholar] [CrossRef]
- Rahman, A.; Carmichael, D.; Harris, M.; Roh, J.K. Comparative Pharmacokinetics of Free Doxorubicin and Doxorubicin Entrapped in Cardiolipin Liposomes. Cancer Res. 1986, 46, 2295–2299. [Google Scholar]
- Swenson, C.E.; Perkins, W.R.; Roberts, P.; Janoff, A.S. Liposome Technology and the Development of MyocetTM (Liposomal Doxorubicin Citrate). Breast 2001, 10, 1–7. [Google Scholar] [CrossRef]
- Batist, G.; Ramakrishnan, G.; Rao, C.S.; Chandrasekharan, A.; Gutheil, J.; Guthrie, T.; Shah, P.; Khojasteh, A.; Nair, M.K.; Hoelzer, K.; et al. Reduced Cardiotoxicity and Preserved Antitumor Efficacy of Liposome-Encapsulated Doxorubicin and Cyclophosphamide Compared with Conventional Doxorubicin and Cyclophosphamide in a Randomized, Multicenter Trial of Metastatic Breast Cancer. J. Clin. Oncol. 2001, 19, 1444–1454. [Google Scholar] [CrossRef] [PubMed]
- Chan, S.; Davidson, N.; Juozaityte, E.; Erdkamp, F.; Pluzanska, A.; Azarnia, N.; Lee, L.W. Phase III Trial of Liposomal Doxorubicin and Cyclophosphamide Compared with Epirubicin and Cyclophosphamide as First-Line Therapy for Metastatic Breast Cancer. Ann. Oncol. 2004, 15, 1527–1534. [Google Scholar] [CrossRef] [PubMed]
- Harris, L.; Batist, G.; Belt, R.; Rovira, D.; Navari, R.; Azarnia, N.; Welles, L.; Winer, E.; TLC D-99 Study Group. Liposome-Encapsulated Doxorubicin Compared with Conventional Doxorubicin in a Randomized Multicenter Trial as First-Line Therapy of Metastatic Breast Carcinoma. Cancer 2002, 94, 25–36. [Google Scholar] [CrossRef]
- French Epirubicin Study Group. Epirubicin-Based Chemotherapy in Metastatic Breast Cancer Patients: Role of Dose-Intensity and Duration of Treatment. J. Clin. Oncol. 2000, 18, 3115–3124. [Google Scholar] [CrossRef]
- Xing, M.; Yan, F.; Yu, S.; Shen, P. Efficacy and Cardiotoxicity of Liposomal Doxorubicin-Based Chemotherapy in Advanced Breast Cancer: A Meta-Analysis of Ten Randomized Controlled Trials. PLoS ONE 2015, 10, e0133569. [Google Scholar] [CrossRef] [Green Version]
- Lorusso, V.; Giotta, F.; Bordonaro, R.; Maiello, E.; Del Prete, S.; Gebbia, V.; Filippelli, G.; Pisconti, S.; Cinieri, S.; Romito, S.; et al. Non-Pegylated Liposome-Encapsulated Doxorubicin Citrate plus Cyclophosphamide or Vinorelbine in Metastatic Breast Cancer Not Previously Treated with Chemotherapy: A Multicenter Phase III Study. Int. J. Oncol. 2014, 45, 2137–2142. [Google Scholar] [CrossRef] [Green Version]
- Schmid, P.; Krocker, J.; Kreienberg, R.; Klare, P.; Kittel, K.; Sommer, H.; Heinrich, G.; Steck, T.; Lichtenegger, W.; Elling, D.; et al. Non-Pegylated Liposomal Doxorubicin and Docetaxel in Metastatic Breast Cancer: Final Results of a Phase II Trial. Cancer Chemother. Pharmacol. 2009, 64, 401–406. [Google Scholar] [CrossRef] [PubMed]
- Fabi, A.; Ferretti, G.; Malaguti, P.; Gasparro, S.; Nisticò, C.; Arpino, G.; Papaldo, P.; Russillo, M.; Catania, G.; Schettini, F.; et al. Nanoparticle Albumin-Bound Paclitaxel/Liposomal-Encapsulated Doxorubicin in HER2-Negative Metastatic Breast Cancer Patients. Future Oncol. 2020, 16, 1629–1637. [Google Scholar] [CrossRef]
- Rosati, M.S.; Raimondi, C.; Baciarello, G.; Grassi, P.; Giovannoni, S.; Petrelli, E.; Basile, M.L.; Girolami, M.; Di Seri, M.; Frati, L. Weekly Combination of Non-Pegylated Liposomal Doxorubicin and Taxane in First-Line Breast Cancer: WALT Trial (Phase I-II). Ann. Oncol. 2011, 22, 315–320. [Google Scholar] [CrossRef]
- Curtit, E.; Nouyrigat, P.; Dohollou, N.; Levy, E.; Lortholary, A.; Gligorov, J.; Facchini, T.; Jaubert, D.; Maille, N.; Pivot, X.; et al. Myotax: A Phase II Trial of Docetaxel plus Non-Pegylated Liposomal Doxorubicin as First-Line Therapy of Metastatic Breast Cancer Previously Treated with Adjuvant Anthracyclines. Eur. J. Cancer 2011, 47, 2396–2402. [Google Scholar] [CrossRef]
- Venturini, M.; Bighin, C.; Puglisi, F.; Olmeo, N.; Aitini, E.; Colucci, G.; Garrone, O.; Paccagnella, A.; Marini, G.; Crinò, L.; et al. A Multicentre Phase II Study of Non-Pegylated Liposomal Doxorubicin in Combination with Trastuzumab and Docetaxel as First-Line Therapy in Metastatic Breast Cancer. Breast 2010, 19, 333–338. [Google Scholar] [CrossRef] [PubMed]
- Lockman, P.R.; Mittapalli, R.K.; Taskar, K.S.; Rudraraju, V.; Gril, B.; Bohn, K.A.; Adkins, C.E.; Roberts, A.; Thorsheim, H.R.; Gaasch, J.A.; et al. Heterogeneous Blood-Tumor Barrier Permeability Determines Drug Efficacy in Experimental Brain Metastases of Breast Cancer. Clin. Cancer Res. 2010, 16, 5664–5678. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Angeli, E.; Nguyen, T.T.; Janin, A.; Bousquet, G. How to Make Anticancer Drugs Cross the Blood-Brain Barrier to Treat Brain Metastases. Int. J. Mol. Sci. 2019, 21, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmid, P.; Krocker, J.; Schulz, C.-O.; Michniewicz, K.; Dieing, A.; Eggemann, H.; Heilmann, V.; Blohmer, J.-U.; Sezer, O.; Elling, D.; et al. Primary Chemotherapy with Gemcitabine, Liposomal Doxorubicin and Docetaxel in Patients with Locally Advanced Breast Cancer: Results of a Phase I Trial. Anti-Cancer Drugs 2005, 16, 21–29. [Google Scholar] [CrossRef]
- Schmid, P.; Krocker, J.; Jehn, C.; Michniewicz, K.; Lehenbauer-Dehm, S.; Eggemann, H.; Heilmann, V.; Kümmel, S.; Schulz, C.O.; Dieing, A.; et al. Primary Chemotherapy with Gemcitabine as Prolonged Infusion, Non-Pegylated Liposomal Doxorubicin and Docetaxel in Patients with Early Breast Cancer: Final Results of a Phase II Trial. Ann. Oncol. 2005, 16, 1624–1631. [Google Scholar] [CrossRef] [PubMed]
- Coltelli, L.; Fontana, A.; Lucchesi, S.; Ginocchi, L.; Bocci, G.; Filidei, M.; Scalese, M.; Arrighi, G.; Finale, C.; Marcucci, L.; et al. Cardiac Safety of Adjuvant Non-Pegylated Liposomal Doxorubicin Combined with Cyclophosphamide and Followed by Paclitaxel in Older Breast Cancer Patients. Breast 2017, 31, 186–191. [Google Scholar] [CrossRef]
- Vici, P.; Pizzuti, L.; Gamucci, T.; Sergi, D.; Conti, F.; Zampa, G.; Del Medico, P.; De Vita, R.; Pozzi, M.; Botti, C.; et al. Non-Pegylated Liposomal Doxorubicin-Cyclophosphamide in Sequential Regimens with Taxanes as Neoadjuvant Chemotherapy in Breast Cancer Patients. J. Cancer 2014, 5, 398–405. [Google Scholar] [CrossRef] [Green Version]
- Davidson, N.; Camburn, T.; Keary, I.; Houghton, D. Substituting Doxorubicin with Nonpegylated Liposomal Doxorubicin for the Treatment of Early Breast Cancer: Results of a Retrospective Study. Int. J. Breast Cancer 2014, 2014, 984067. [Google Scholar] [CrossRef]
- Von Minckwitz, G.; Schneeweiss, A.; Loibl, S.; Salat, C.; Denkert, C.; Rezai, M.; Blohmer, J.U.; Jackisch, C.; Paepke, S.; Gerber, B.; et al. Neoadjuvant Carboplatin in Patients with Triple-Negative and HER2-Positive Early Breast Cancer (GeparSixto; GBG 66): A Randomised Phase 2 Trial. Lancet Oncol. 2014, 15, 747–756. [Google Scholar] [CrossRef]
- Brain, E.G.C.; Mertens, C.; Girre, V.; Rousseau, F.; Blot, E.; Abadie, S.; Uwer, L.; Bourbouloux, E.; Van Praagh-Doreau, I.; Mourey, L.; et al. Impact of Liposomal Doxorubicin-Based Adjuvant Chemotherapy on Autonomy in Women over 70 with Hormone-Receptor-Negative Breast Carcinoma: A French Geriatric Oncology Group (GERICO) Phase II Multicentre Trial. Crit. Rev. Oncol. Hematol. 2011, 80, 160–170. [Google Scholar] [CrossRef]
- Brain, E.; Girre, V.; Rollot, F.; Bonnetain, F.; Debled, M.; Lacroix, M.; Baffert, S.; Latouche, A.; Falandry, C.; Peyro Saint Paul, H.P.; et al. ASTER 70s: Benefit of Adjuvant Chemotherapy for Estrogen Receptor-Positive HER2-Negative Breast Cancer in Women over 70 According to Genomic Grade—A French GERICO/UCBG UNICANCER Multicenter Phase III Trial. JCO 2012, 30, TPS667. [Google Scholar] [CrossRef]
- Gradishar, W.J.; Moran, M.S.; Abraham, J.; Aft, R.; Agnese, D.; Allison, K.H.; Blair, S.L.; Burstein, H.J.; Dang, C.; Elias, A.D.; et al. NCCN Guidelines® Insights: Breast Cancer, Version 4.2021. J. Natl. Compr. Cancer Netw. 2021, 19, 484–493. [Google Scholar] [CrossRef]
- Cardoso, F.; Paluch-Shimon, S.; Senkus, E.; Curigliano, G.; Aapro, M.S.; André, F.; Barrios, C.H.; Bergh, J.; Bhattacharyya, G.S.; Biganzoli, L.; et al. 5th ESO-ESMO International Consensus Guidelines for Advanced Breast Cancer (ABC 5). Ann. Oncol. 2020, 31, 1623–1649. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, F.; Kyriakides, S.; Ohno, S.; Penault-Llorca, F.; Poortmans, P.; Rubio, I.T.; Zackrisson, S.; Senkus, E. ESMO Guidelines Committee Early Breast Cancer: ESMO Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up. Ann. Oncol. 2019, 30, 1674. [Google Scholar] [CrossRef] [Green Version]
- Gavilá, J.; Oliveira, M.; Pascual, T.; Perez-Garcia, J.; Gonzàlez, X.; Canes, J.; Paré, L.; Calvo, I.; Ciruelos, E.; Muñoz, M.; et al. Safety, Activity, and Molecular Heterogeneity Following Neoadjuvant Non-Pegylated Liposomal Doxorubicin, Paclitaxel, Trastuzumab, and Pertuzumab in HER2-Positive Breast Cancer (Opti-HER HEART): An Open-Label, Single-Group, Multicenter, Phase 2 Trial. BMC Med. 2019, 17, 8. [Google Scholar] [CrossRef]
- Antón, A.; Ruiz, A.; Plazaola, A.; Calvo, L.; Seguí, M.A.; Santaballa, A.; Muñoz, M.; Sánchez, P.; Miguel, A.; Carrasco, E.; et al. Phase II Clinical Trial of Liposomal-Encapsulated Doxorubicin Citrate and Docetaxel, Associated with Trastuzumab, as Neoadjuvant Treatment in Stages II and IIIA HER2-Overexpressing Breast Cancer Patients. GEICAM 2003-03 Study. Ann. Oncol. 2011, 22, 74–79. [Google Scholar] [CrossRef]
- Saracchini, S.; Foltran, L.; Tuccia, F.; Bassini, A.; Sulfaro, S.; Micheli, E.; Del Conte, A.; Bertola, M.; Gion, M.; Lorenzon, M.; et al. Phase II Study of Liposome-Encapsulated Doxorubicin plus Cyclophosphamide, Followed by Sequential Trastuzumab plus Docetaxel as Primary Systemic Therapy for Breast Cancer Patients with HER2 Overexpression or Amplification. Breast 2013, 22, 1101–1107. [Google Scholar] [CrossRef] [PubMed]
- Tarantino, P.; Tolaney, S.M.; Harbeck, N.; Cortes, J.; Curigliano, G. Anthracyclines for Human Epidermal Growth Factor Receptor 2-Positive Breast Cancer: Are We Ready to Let Them Go? J. Clin. Oncol. 2021, JCO2101059. [Google Scholar] [CrossRef] [PubMed]
- Amadori, D.; Milandri, C.; Comella, G.; Saracchini, S.; Salvagni, S.; Barone, C.; Bordonaro, R.; Gebbia, V.; Barbato, A.; Serra, P.; et al. A Phase I/II Trial of Non-Pegylated Liposomal Doxorubicin, Docetaxel and Trastuzumab as First-Line Treatment in HER-2-Positive Locally Advanced or Metastatic Breast Cancer. Eur. J. Cancer 2011, 47, 2091–2098. [Google Scholar] [CrossRef] [PubMed]
- Cortes, J.; Di Cosimo, S.; Climent, M.A.; Cortés-Funes, H.; Lluch, A.; Gascón, P.; Mayordomo, J.I.; Gil, M.; Benavides, M.; Cirera, L.; et al. Nonpegylated Liposomal Doxorubicin (TLC-D99), Paclitaxel, and Trastuzumab in HER-2-Overexpressing Breast Cancer: A Multicenter Phase I/II Study. Clin. Cancer Res. 2009, 15, 307–314. [Google Scholar] [CrossRef] [Green Version]
- Baselga, J.; Manikhas, A.; Cortés, J.; Llombart, A.; Roman, L.; Semiglazov, V.F.; Byakhov, M.; Lokanatha, D.; Forenza, S.; Goldfarb, R.H.; et al. Phase III Trial of Nonpegylated Liposomal Doxorubicin in Combination with Trastuzumab and Paclitaxel in HER2-Positive Metastatic Breast Cancer. Ann. Oncol. 2014, 25, 592–598. [Google Scholar] [CrossRef]
- Baselga, J.; Cortés, J.; Kim, S.-B.; Im, S.-A.; Hegg, R.; Im, Y.-H.; Roman, L.; Pedrini, J.L.; Pienkowski, T.; Knott, A.; et al. Pertuzumab plus Trastuzumab plus Docetaxel for Metastatic Breast Cancer. N. Engl. J. Med. 2012, 366, 109–119. [Google Scholar] [CrossRef] [Green Version]
- Schettini, F.; Conte, B.; Buono, G.; De Placido, P.; Parola, S.; Griguolo, G.; Fabi, A.; Bighin, C.; Riccardi, F.; Cianniello, D.; et al. T-DM1 versus Pertuzumab, Trastuzumab and a Taxane as First-Line Therapy of Early-Relapsed HER2-Positive Metastatic Breast Cancer: An Italian Multicenter Observational Study. ESMO Open 2021, 6, 100099. [Google Scholar] [CrossRef]
- Verma, S.; Miles, D.; Gianni, L.; Krop, I.E.; Welslau, M.; Baselga, J.; Pegram, M.; Oh, D.-Y.; Diéras, V.; Guardino, E.; et al. Trastuzumab Emtansine for HER2-Positive Advanced Breast Cancer. N. Engl. J. Med. 2012, 367, 1783–1791. [Google Scholar] [CrossRef] [Green Version]
- López-Miranda, E.; Pérez-García, J.M.; Di Cosimo, S.; Brain, E.; Ravnik, M.; Escrivá-de-Romaní, S.; Vidal, M.; Gligorov, J.; Borštnar, S.; Calabuig, L.; et al. Trastuzumab Emtansine Plus Non-Pegylated Liposomal Doxorubicin in HER2-Positive Metastatic Breast Cancer (Thelma): A Single-Arm, Multicenter, Phase Ib Trial. Cancers 2020, 12, 3509. [Google Scholar] [CrossRef]
- Moy, B.; Rumble, R.B.; Come, S.E.; Davidson, N.E.; Di Leo, A.; Gralow, J.R.; Hortobagyi, G.N.; Yee, D.; Smith, I.E.; Chavez-MacGregor, M.; et al. Chemotherapy and Targeted Therapy for Patients With Human Epidermal Growth Factor Receptor 2-Negative Metastatic Breast Cancer That is Either Endocrine-Pretreated or Hormone Receptor-Negative: ASCO Guideline Update. J. Clin. Oncol. 2021. epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Schettini, F.; Giudici, F.; Bernocchi, O.; Sirico, M.; Corona, S.P.; Giuliano, M.; Locci, M.; Paris, I.; Scambia, G.; De Placido, S.; et al. Poly (ADP-Ribose) Polymerase Inhibitors in Solid Tumours: Systematic Review and Meta-Analysis. Eur. J. Cancer 2021, 149, 134–152. [Google Scholar] [CrossRef]
- Militello, A.M.; Zielli, T.; Boggiani, D.; Michiara, M.; Naldi, N.; Bortesi, B.; Zanelli, P.; Uliana, V.; Giuliotti, S.; Musolino, A. Mechanism of Action and Clinical Efficacy of CDK4/6 Inhibitors in BRCA-Mutated, Estrogen Receptor-Positive Breast Cancers: Case Report and Literature Review. Front. Oncol. 2019, 9, 759. [Google Scholar] [CrossRef] [Green Version]
- Schettini, F.; Giudici, F.; Giuliano, M.; Cristofanilli, M.; Arpino, G.; Del Mastro, L.; Puglisi, F.; De Placido, S.; Paris, I.; De Placido, P.; et al. Overall Survival of CDK4/6-Inhibitors-Based Treatments in Clinically Relevant Subgroups of Metastatic Breast Cancer: Systematic Review and Meta-Analysis. J. Natl. Cancer Inst. 2020, 112, 1089–1097. [Google Scholar] [CrossRef]
- Nanni, O.; Amadori, D.; De Censi, A.; Rocca, A.; Freschi, A.; Bologna, A.; Gianni, L.; Rosetti, F.; Amaducci, L.; Cavanna, L.; et al. Metformin plus Chemotherapy versus Chemotherapy Alone in the First-Line Treatment of HER2-Negative Metastatic Breast Cancer. The MYME Randomized, Phase 2 Clinical Trial. Breast Cancer Res. Treat. 2019, 174, 433–442. [Google Scholar] [CrossRef] [PubMed]
- Mbuagbaw, L.; Rochwerg, B.; Jaeschke, R.; Heels-Andsell, D.; Alhazzani, W.; Thabane, L.; Guyatt, G.H. Approaches to Interpreting and Choosing the Best Treatments in Network Meta-Analyses. Syst. Rev. 2017, 6, 79. [Google Scholar] [CrossRef] [Green Version]
- Gradishar, W.J.; Krasnojon, D.; Cheporov, S.; Makhson, A.N.; Manikhas, G.M.; Clawson, A.; Bhar, P. Significantly Longer Progression-Free Survival with Nab-Paclitaxel Compared with Docetaxel as First-Line Therapy for Metastatic Breast Cancer. J. Clin. Oncol. 2009, 27, 3611–3619. [Google Scholar] [CrossRef] [PubMed]
- Gradishar, W.J.; Tjulandin, S.; Davidson, N.; Shaw, H.; Desai, N.; Bhar, P.; Hawkins, M.; O’Shaughnessy, J. Phase III Trial of Nanoparticle Albumin-Bound Paclitaxel Compared with Polyethylated Castor Oil-Based Paclitaxel in Women with Breast Cancer. J. Clin. Oncol. 2005, 23, 7794–7803. [Google Scholar] [CrossRef]
- Gradishar, W.J.; Krasnojon, D.; Cheporov, S.; Makhson, A.N.; Manikhas, G.M.; Clawson, A.; Bhar, P.; McGuire, J.R.; Iglesias, J. Phase II Trial of Nab-Paclitaxel Compared with Docetaxel as First-Line Chemotherapy in Patients with Metastatic Breast Cancer: Final Analysis of Overall Survival. Clin. Breast Cancer 2012, 12, 313–321. [Google Scholar] [CrossRef]
- Rigacci, L.; Annibali, O.; Kovalchuk, S.; Bonifacio, E.; Pregnolato, F.; Angrilli, F.; Vitolo, U.; Pozzi, S.; Broggi, S.; Luminari, S.; et al. Nonpeghylated Liposomal Doxorubicin Combination Regimen (R-COMP) for the Treatment of Lymphoma Patients with Advanced Age or Cardiac Comorbidity. Hematol. Oncol. 2020, 38, 478–486. [Google Scholar] [CrossRef]
- Luminari, S.; Viel, E.; Ferreri, A.J.M.; Zaja, F.; Chimienti, E.; Musuraca, G.; Tucci, A.; Balzarotti, M.; Tani, M.; Salvi, F.; et al. Nonpegylated Liposomal Doxorubicin Combination Regimen in Patients with Diffuse Large B-Cell Lymphoma and Cardiac Comorbidity. Results of the HEART01 Phase II Trial Conducted by the Fondazione Italiana Linfomi. Hematol. Oncol. 2018, 36, 68–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szmit, S.; Grela-Wojewoda, A.; Talerczyk, M.; Kufel-Grabowska, J.; Streb, J.; Smok-Kalwat, J.; Iżycki, D.; Chmielowska, E.; Wilk, M.; Sosnowska-Pasiarska, B. Predictors of New-Onset Heart Failure and Overall Survival in Metastatic Breast Cancer Patients Treated with Liposomal Doxorubicin. Sci. Rep. 2020, 10, 18481. [Google Scholar] [CrossRef] [PubMed]
- Szmit, S.; Jurczak, W.; Zaucha, J.M.; Długosz-Danecka, M.; Sosnowska-Pasiarska, B.; Chmielowska, E.; Joks, M.; Drozd-Sokołowska, J.; Knopińska-Posłuszny, W.; Spychałowicz, W.; et al. Acute Decompensated Heart Failure as a Reason of Premature Chemotherapy Discontinuation May Be Independent of a Lifetime Doxorubicin Dose in Lymphoma Patients with Cardiovascular Disorders. Int. J. Cardiol. 2017, 235, 147–153. [Google Scholar] [CrossRef]
- Aapro, M.; Bernard-Marty, C.; Brain, E.G.; Batist, G.; Erdkamp, F.; Krzemieniecki, K.; Leonard, R.; Lluch, A.; Monfardini, S.; Ryberg, M.; et al. Anthracycline cardiotoxicity in the elderly cancer patient: A SIOG expert position paper. Ann. Oncol. 2011, 22, 257–267. [Google Scholar] [CrossRef] [PubMed]
- European Commission Myocet’s Summary of Product Characteristics. Annex I. Available online: https://ec.europa.eu/health/documents/community-register/2015/20150127130862/anx_130862_en.pdf (accessed on 31 August 2021).
- Seicean, S.; Seicean, A.; Alan, N.; Plana, J.C.; Budd, G.T.; Marwick, T.H. Cardioprotective Effect of β-Adrenoceptor Blockade in Patients with Breast Cancer Undergoing Chemotherapy: Follow-up Study of Heart Failure. Circ. Heart Fail. 2013, 6, 420–426. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Study Characteristics | Trial 1 | Trial 2 | Trial 3 |
|---|---|---|---|
| First Author | Batist G | Harris L | Chan S |
| Year | 2001 | 2002 | 2004 |
| Journal | J Clin Oncol | Cancer | Ann Oncol |
| Phase | III | III | III |
| Randomization | Yes | Yes | Yes |
| Study population | HER2-neg. MBC | HER2-neg. MBC | HER2-neg. MBC |
| Arm A | NPLD + Cyc | NPLD | NPLD + Cyc |
| Doses Arm A | 60 mg/m2 + 600 mg/m2 | 75 mg/m2 | 75 mg/m2 + 600 mg/m2 |
| Arm B | AC | Doxorubicin | EC |
| Doses Arm B | 60 mg/m2 + 600 mg/m2 | 75 mg/m2 | 75 mg/m2 + 600 mg/m2 |
| N Arm A | 142 | 108 | 80 |
| N Arm B | 155 | 116 | 80 |
| RR Arm A | 43% (95% CI: 35–52%) | 26% (95% CI: NR) | 46% (95% CI: 35–58%) |
| RR Arm B | 43% (95% CI: 35–51%) | 26% (95% CI: NR) | 39% (95% CI: 28–50%) |
| mTTP Arm A | 5.10 | 3.80 | 7.70 |
| mTTP Arm B | 5.50 | 4.30 | 5.60 |
| HR (B vs. A) | 1.03 | 0.92 * | 1.52 |
| P | 0.82 | 0.59 | 0.02 |
| mOS Arm A | 19.00 | 16.00 | 18.30 |
| mOS Arm B | 16.00 | 20.00 | 16.00 |
| HR (B vs. A) | 1.04 | 0.76 * | 1.15 |
| P | 0.79 | 0.09 | 0.50 |
| ADVERSE REACTIONS WHO GRADE ≥3 | NPLD + CYC | NPLD |
|---|---|---|
| non-hematologic non-cardiac events | % pt | % pt |
| Allergic reactions | - | 4.0 |
| Alopecia * | 62.0 | - |
| Arthralgia | - | 4.0 |
| Constipation | 1.0 | - |
| Diarrhea | 1.0–3.0 | 1.0 |
| Fatigue/asthenia | 0.0–6.0 | 14.0 |
| Febrile neutropenia | 5.0–9.0 | 0.0–11.0 |
| Hand-foot syndrome | - | 10.0 |
| Infection | 7.0–11.0 | 5.0 |
| Nausea/vomiting | 2.0–21.0 | 13.0 |
| Skin reaction/rash | 0.0 | 1.0 |
| Stomatitis/mucositis | 4.0–7.0 | 9.0 |
| Hematologic and biochemical events | ||
| Decreased hemoglobin/anemia | 3.0–25.0 | 22.0 |
| Thrombocytopenia | 2.0–22.0 | 13.0 |
| Neutropenia | 61.0–87.0 | 50.0 |
| Leukopenia | 16.0 | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schettini, F.; Giuliano, M.; Lambertini, M.; Bartsch, R.; Pinato, D.J.; Onesti, C.E.; Harbeck, N.; Lüftner, D.; Rottey, S.; van Dam, P.A.; et al. Anthracyclines Strike Back: Rediscovering Non-Pegylated Liposomal Doxorubicin in Current Therapeutic Scenarios of Breast Cancer. Cancers 2021, 13, 4421. https://doi.org/10.3390/cancers13174421
Schettini F, Giuliano M, Lambertini M, Bartsch R, Pinato DJ, Onesti CE, Harbeck N, Lüftner D, Rottey S, van Dam PA, et al. Anthracyclines Strike Back: Rediscovering Non-Pegylated Liposomal Doxorubicin in Current Therapeutic Scenarios of Breast Cancer. Cancers. 2021; 13(17):4421. https://doi.org/10.3390/cancers13174421
Chicago/Turabian StyleSchettini, Francesco, Mario Giuliano, Matteo Lambertini, Rupert Bartsch, David James Pinato, Concetta Elisa Onesti, Nadia Harbeck, Diana Lüftner, Sylvie Rottey, Peter A. van Dam, and et al. 2021. "Anthracyclines Strike Back: Rediscovering Non-Pegylated Liposomal Doxorubicin in Current Therapeutic Scenarios of Breast Cancer" Cancers 13, no. 17: 4421. https://doi.org/10.3390/cancers13174421
APA StyleSchettini, F., Giuliano, M., Lambertini, M., Bartsch, R., Pinato, D. J., Onesti, C. E., Harbeck, N., Lüftner, D., Rottey, S., van Dam, P. A., Zaman, K., Mustacchi, G., Gligorov, J., Awada, A., Campone, M., Wildiers, H., Gennari, A., Tjan-Heijnen, V. C. G., Cortes, J., ... Generali, D. (2021). Anthracyclines Strike Back: Rediscovering Non-Pegylated Liposomal Doxorubicin in Current Therapeutic Scenarios of Breast Cancer. Cancers, 13(17), 4421. https://doi.org/10.3390/cancers13174421