
Development and Implementation of Multidisciplinary Liver Tumor Boards in the Veterans Affairs Health Care System: A 10-Year Experience

Abstract
:Simple Summary
Abstract
1. Background
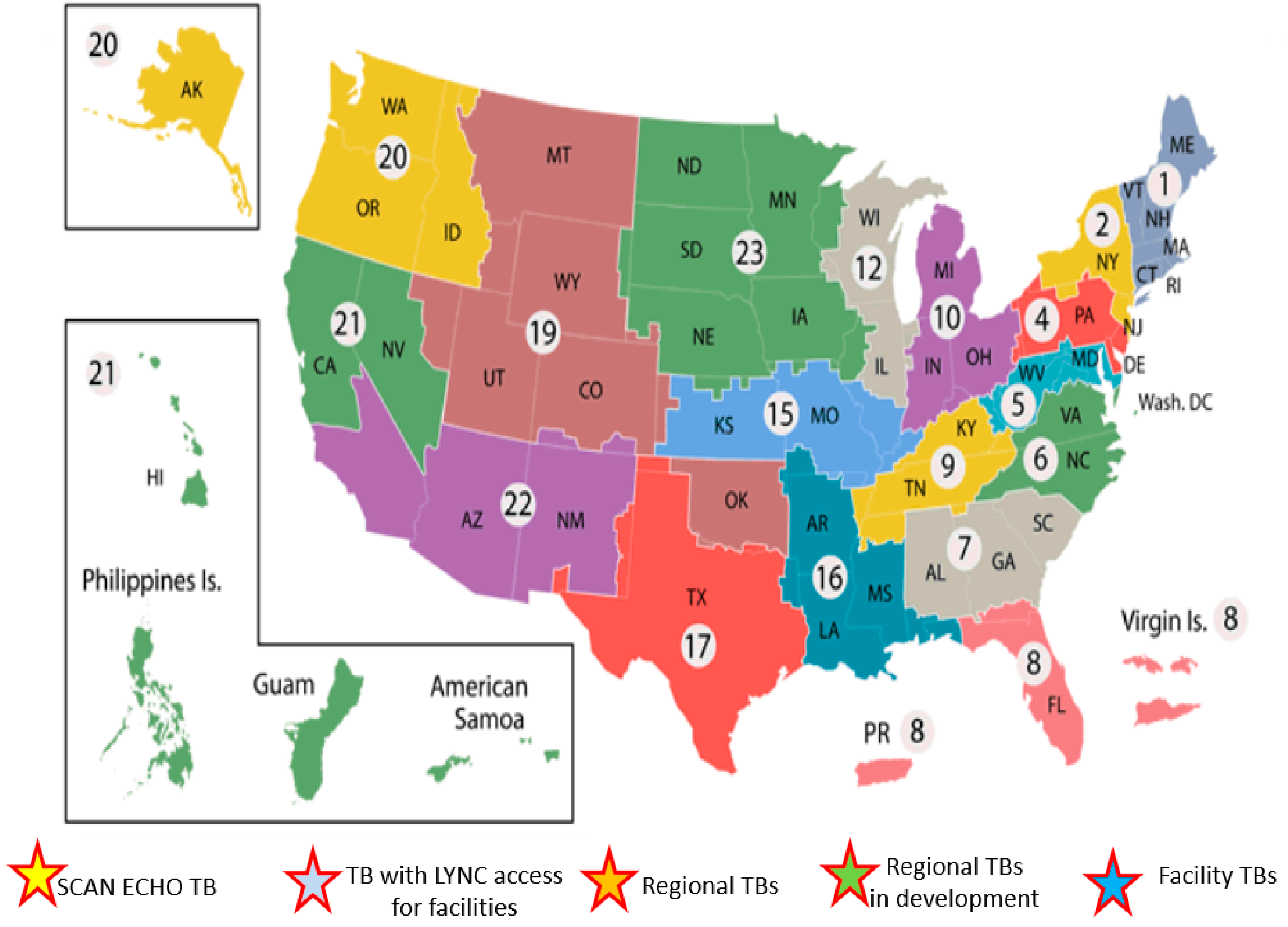
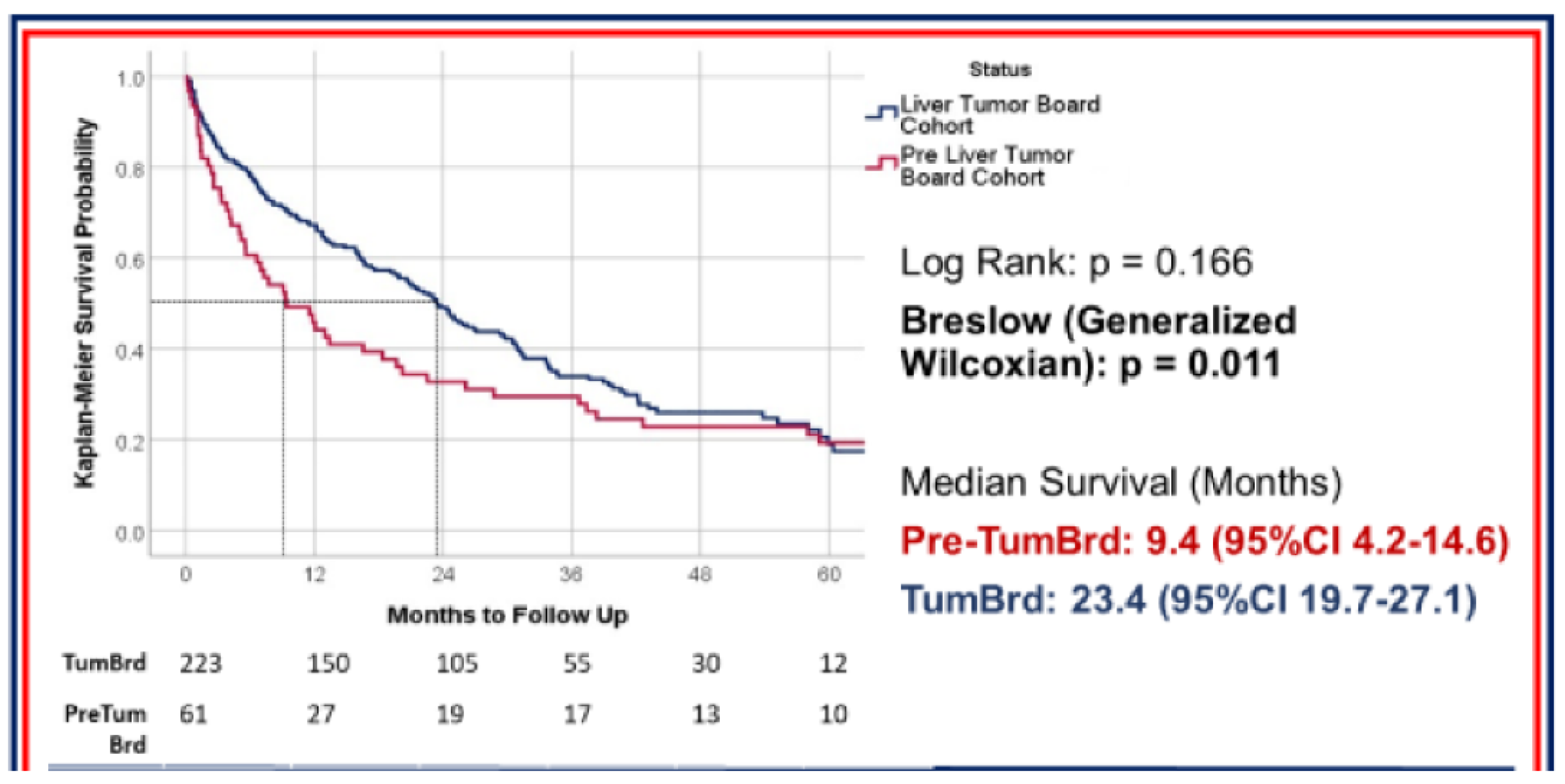
2. History of Liver Cancer Care at the VA
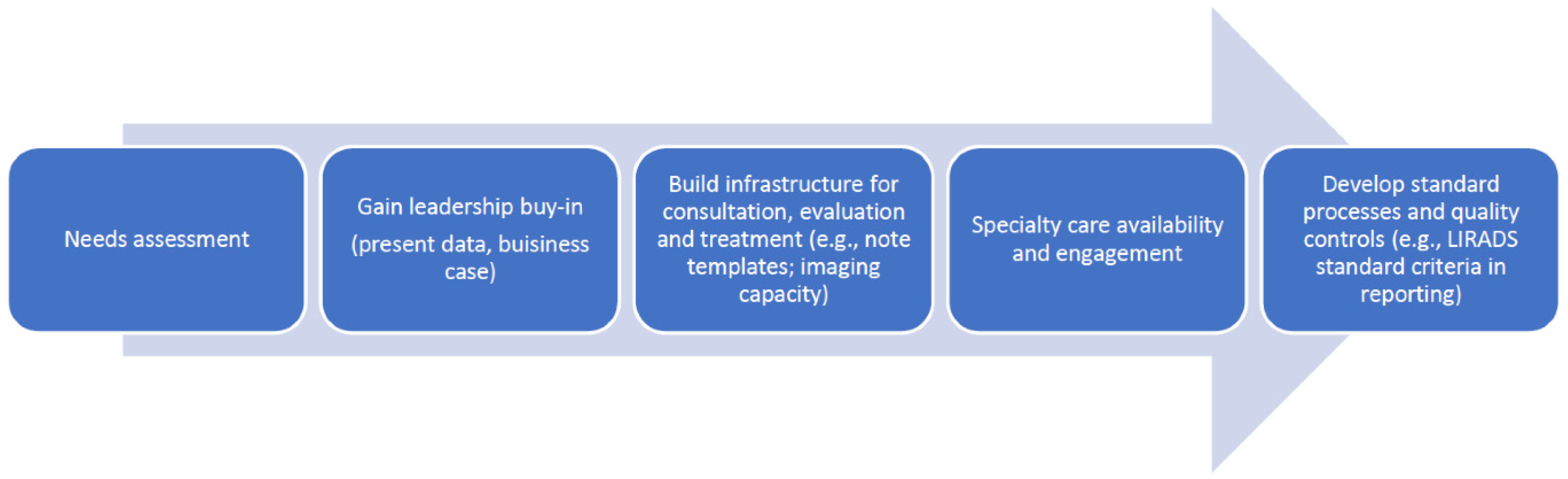
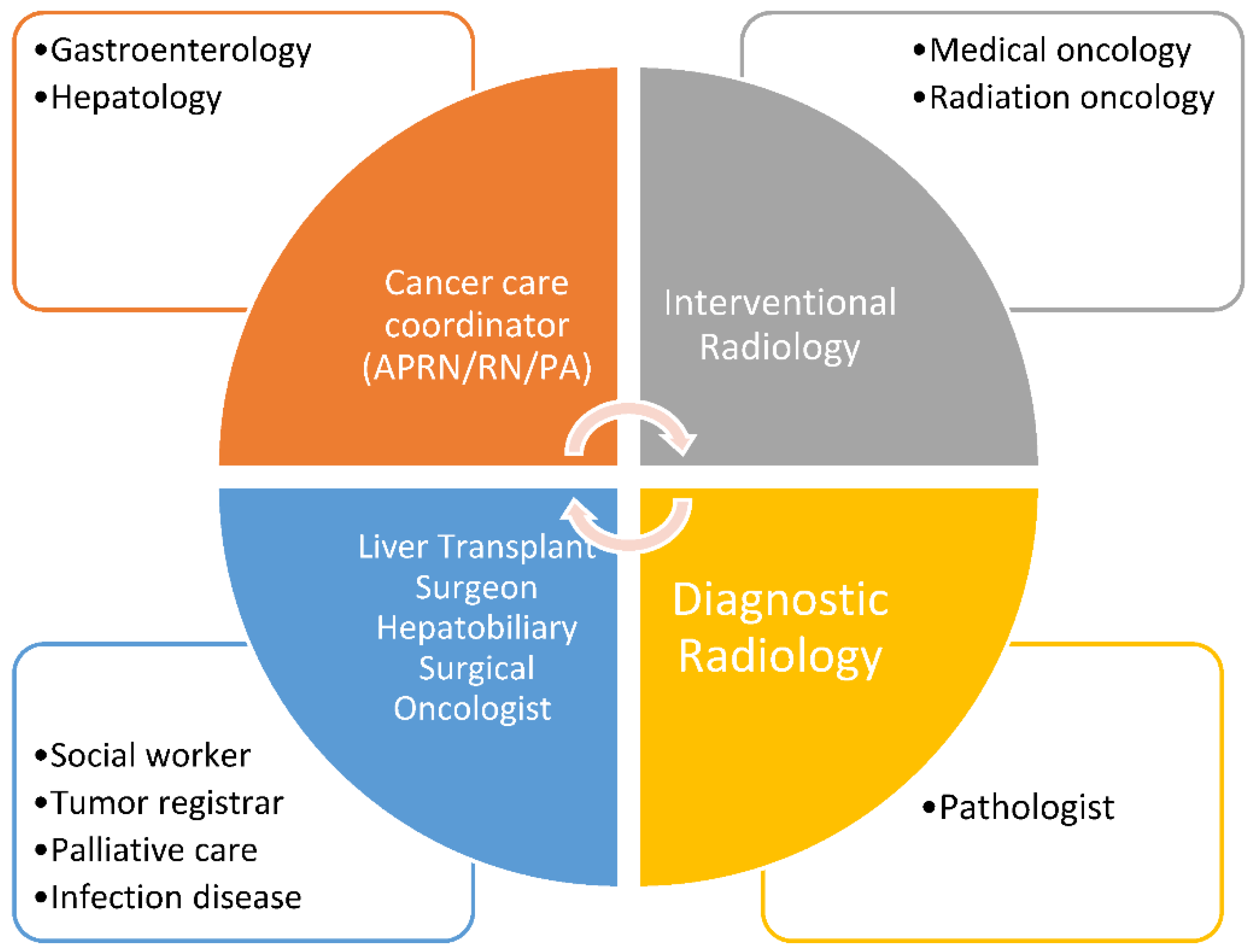
3. Components of Multidisciplinary Tumor Board
4. Discussion and Future Directions
Author Contributions
Funding
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ryerson, A.B.; Eheman, C.R.; Altekruse, S.F.; Ward, J.W.; Jemal, A.; Sherman, R.L.; Henley, S.J.; Holtzman, D.; Lake, A.; Noone, A.M.; et al. Annual Report to the Nation on the Status of Cancer, 1975-2012, featuring the increasing incidence of liver cancer. Cancer 2016, 122, 1312–1337. [Google Scholar] [CrossRef] [PubMed]
- Shiels, M.S.; O’Brien, T.R. Recent Decline in Hepatocellular Carcinoma Rates in the United States. Gastroenterology 2020, 158, 1503–1505.e2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Serper, M.; Taddei, T.; Mehta, R.; D’Addeo, K.; Dai, F.; Aytaman, A.; Baytarian, M.; Fox, R.; Hunt, K.; Goldberg, D.S.; et al. Association of Provider Specialty and Multidisciplinary Care With Hepatocellular Carcinoma Treatment and Mortality. Gastroenterology 2017, 152, 1954–1964. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agarwal, P.D.; Phillips, P.; Hillman, L.; Lucey, M.R.; Lee, F.; Mezrich, J.D.; Said, A. Multidisciplinary Management of Hepatocellular Carcinoma Improves Access to Therapy and Patient Survival. J. Clin. Gastroenterol. 2017, 51, 845–849. [Google Scholar] [CrossRef] [PubMed]
- Yan, S.-Y.; Zhang, Y.; Sun, C.; Cao, H.-X.; Li, G.-M.; Wang, Y.-Q.; Fan, J.-G. The clinical effect and relevant mechanism of combined sorafenib and radiofrequency ablation in the treatment of early small hepatocellular carcinoma. Oncol. Lett. 2016, 12, 951–955. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaba, R.C.; Kallwitz, E.R.; Parvinian, A.; Bui, J.T.; Von Roenn, N.M.; Berkes, J.L.; Cotler, S.J. Imaging surveillance and multidisciplinary review improves curative therapy access and survival in HCC patients. Ann. Hepatol. 2013, 12, 766–773. [Google Scholar] [CrossRef]
- Chang, T.T.; Sawhney, R.; Monto, A.; Ben Davoren, J.; Kirkland, J.; Stewart, L.; Corvera, C.U. Implementation of a multidisciplinary treatment team for hepatocellular cancer at a Veterans Affairs Medical Center improves survival. HPB 2008, 10, 405–411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor, C.; Munro, A.J.; Glynne-Jones, R.; Griffith, C.; Trevatt, P.; Richards, M.; Ramirez, A.J. Multidisciplinary team working in cancer: What is the evidence? BMJ 2010, 340, c951. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siddique, O.; Yoo, E.R.; Perumpail, R.B.; Perumpail, B.J.; Liu, A.; Cholankeril, G.; Ahmed, A. The importance of a multidisciplinary approach to hepatocellular carcinoma. J. Multidiscip. Health 2017, 10, 95–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yopp, A.C.; Mansour, J.C.; Beg, M.S.; Arenas, J.; Trimmer, C.; Reddick, M.; Pedrosa, I.; Khatri, G.; Yakoo, T.; Meyer, J.J.; et al. Establishment of a Multidisciplinary Hepatocellular Carcinoma Clinic is Associated with Improved Clinical Outcome. Ann. Surg. Oncol. 2014, 21, 1287–1295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: Hepatobiliary Cancers; Version 3; National Comprehensive Cancer Network: Plymouth Meeting, PA, USA, 2017. [Google Scholar]
- American College of Radiology ACo. Liver Imaging Reporting Data System. Available online: https://www.acr.org/QualitySafety/Resources/LIRADS (accessed on 3 January 2021).
- Available online: https://www.hepatitis.va.gov/pdf/HCC-multidisciplinary-management-best-practices.pdf (accessed on 3 January 2021).
- Available online: https://www.hepatitis.va.gov/pdf/HCC-patient-modules.pdf (accessed on 3 January 2021).
- Horowitz, J.; Lerer, R.; Nelson, E.; Silver, B.; Zahiruddin, A.; Kalra, A.; Al-Ani, F.; Hunt, K.K.; Lancellotti, F.; Schwartz, D. Effects of a multifacility, multispecialty tumor board on timeliness of care and survival in HCC. Hepatology 2019, 70, 133A. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Elements of MDLTB | Key Questions and Possible Solutions |
|---|---|
| Governance, Recording and Documentation | Where will MDLTB meet? When will MDLTB meet? Who will present cases? Who will record findings, discussion, and recommendations? |
| Clinical documentation and coordination | MDLTB Common Data Elements Getting data into clinical record
|
| Agenda creation and submission | Who will create agenda? Will pre-review be required, who will do? How will incomplete submissions be handled?
|
Getting data into clinical record
| |
| Case submission | Who will have access to submit?
How will data be submitted?
Cutoff date/time |
| Follow up | Computerized Patient Record System (CPRS) orders at Hub – who is going to be responsible?
|
| Audit and feedback | What outcomes are important for MDLTB to track?
How sentinel events will be reported/discussed Reporting requirements (if any) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rabiee, A.; Taddei, T.; Aytaman, A.; Rogal, S.S.; Kaplan, D.E.; Morgan, T.R. Development and Implementation of Multidisciplinary Liver Tumor Boards in the Veterans Affairs Health Care System: A 10-Year Experience. Cancers 2021, 13, 4849. https://doi.org/10.3390/cancers13194849
Rabiee A, Taddei T, Aytaman A, Rogal SS, Kaplan DE, Morgan TR. Development and Implementation of Multidisciplinary Liver Tumor Boards in the Veterans Affairs Health Care System: A 10-Year Experience. Cancers. 2021; 13(19):4849. https://doi.org/10.3390/cancers13194849
Chicago/Turabian StyleRabiee, Atoosa, Tamar Taddei, Ayse Aytaman, Shari S. Rogal, David E. Kaplan, and Timothy R. Morgan. 2021. "Development and Implementation of Multidisciplinary Liver Tumor Boards in the Veterans Affairs Health Care System: A 10-Year Experience" Cancers 13, no. 19: 4849. https://doi.org/10.3390/cancers13194849
APA StyleRabiee, A., Taddei, T., Aytaman, A., Rogal, S. S., Kaplan, D. E., & Morgan, T. R. (2021). Development and Implementation of Multidisciplinary Liver Tumor Boards in the Veterans Affairs Health Care System: A 10-Year Experience. Cancers, 13(19), 4849. https://doi.org/10.3390/cancers13194849