Non-Invasive Mapping for Effective Preoperative Guidance to Approach Highly Language-Eloquent Gliomas—A Large Scale Comparative Cohort Study Using a New Classification for Language Eloquence

 and
and 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Ethics
2.2. Eligibility Criteria
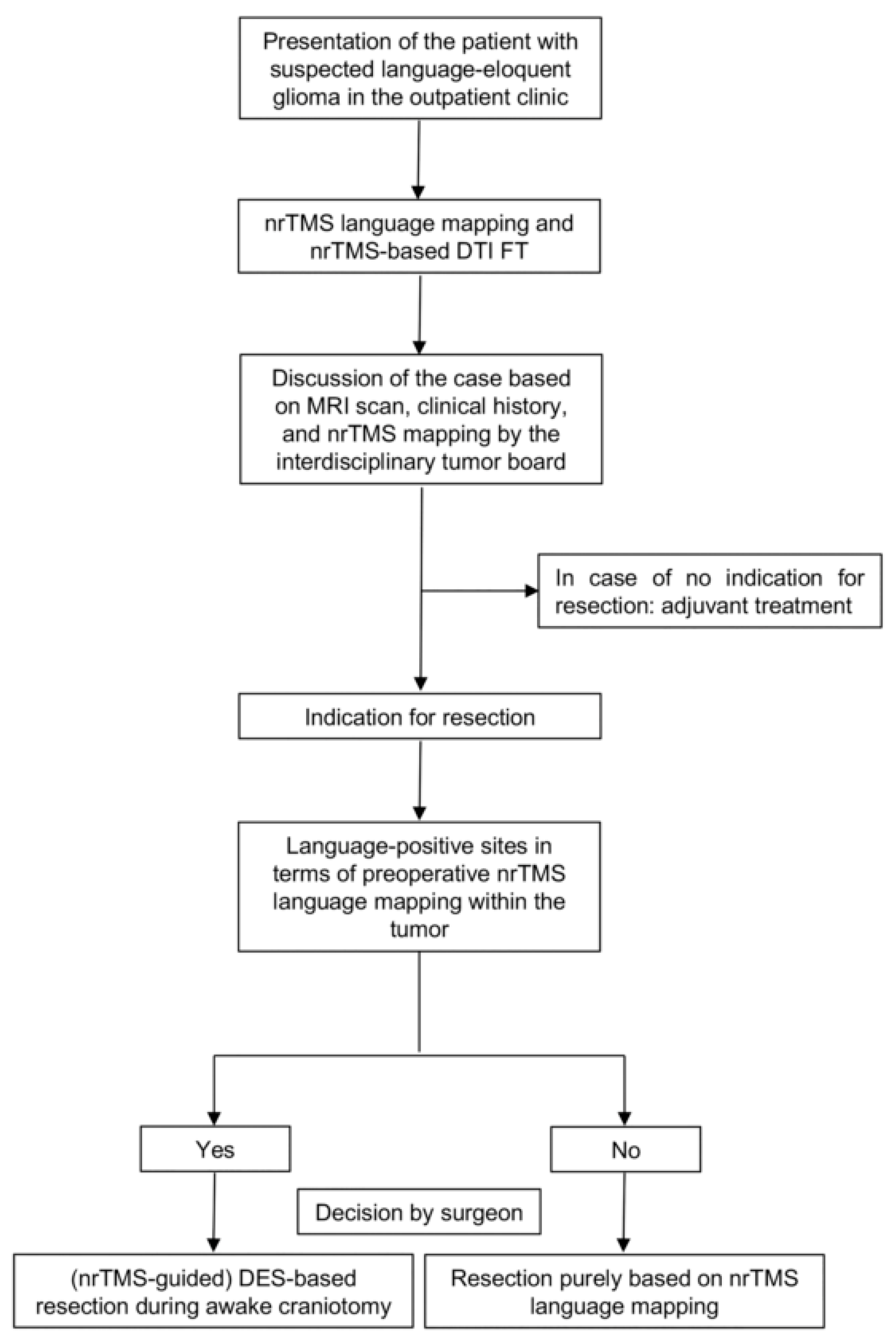
2.3. Study Protocol
2.4. Classification of Language Eloquence
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Functional and Radiological Outcome
3.3. Classification of Language Eloquence
4. Discussion
4.1. Feasibility of nrTMS-Based Glioma Resection
4.2. Differentiation through Classification of Language Eloquence
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Disclosure
References
- Capelle, L.; Fontaine, D.; Mandonnet, E.; Taillandier, L.; Golmard, J.L.; Bauchet, L.; Pallud, J.; Peruzzi, P.; Baron, M.H.; Kujas, M.; et al. Spontaneous and therapeutic prognostic factors in adult hemispheric World Health Organization Grade II gliomas: A series of 1097 cases: Clinical article. J. Neurosurg. 2013, 118, 1157–1168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanai, N.; Polley, M.Y.; McDermott, M.W.; Parsa, A.T.; Berger, M.S. An extent of resection threshold for newly diagnosed glioblastomas. J. Neurosurg. 2011, 115, 3–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Witt Hamer, P.C.; Robles, S.G.; Zwinderman, A.H.; Duffau, H.; Berger, M.S. Impact of intraoperative stimulation brain mapping on glioma surgery outcome: A meta-analysis. J. Clin. Oncol. 2012, 30, 2559–2565. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanai, N.; Mirzadeh, Z.; Berger, M.S. Functional outcome after language mapping for glioma resection. N. Engl. J. Med. 2008, 358, 18–27. [Google Scholar] [CrossRef] [PubMed]
- Ille, S.; Sollmann, N.; Hauck, T.; Maurer, S.; Tanigawa, N.; Obermueller, T.; Negwer, C.; Droese, D.; Boeckh-Behrens, T.; Meyer, B.; et al. Impairment of preoperative language mapping by lesion location: A functional magnetic resonance imaging, navigated transcranial magnetic stimulation, and direct cortical stimulation study. J. Neurosurg. 2015, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Picht, T.; Krieg, S.M.; Sollmann, N.; Rosler, J.; Niraula, B.; Neuvonen, T.; Savolainen, P.; Lioumis, P.; Makela, J.P.; Deletis, V.; et al. A comparison of language mapping by preoperative navigated transcranial magnetic stimulation and direct cortical stimulation during awake surgery. Neurosurgery 2013, 72, 808–819. [Google Scholar] [CrossRef] [Green Version]
- Tarapore, P.E.; Findlay, A.M.; Honma, S.M.; Mizuiri, D.; Houde, J.F.; Berger, M.S.; Nagarajan, S.S. Language mapping with navigated repetitive TMS: Proof of technique and validation. Neuroimage 2013, 82, 260–272. [Google Scholar] [CrossRef] [Green Version]
- Raffa, G.; Quattropani, M.C.; Scibilia, A.; Conti, A.; Angileri, F.F.; Esposito, F.; Sindorio, C.; Cardali, S.M.; Germano, A.; Tomasello, F. Surgery of language-eloquent tumors in patients not eligible for awake surgery: The impact of a protocol based on navigated transcranial magnetic stimulation on presurgical planning and language outcome, with evidence of tumor-induced intra-hemispheric plasticity. Clin. Neurol. Neurosurg. 2018, 168, 127–139. [Google Scholar] [CrossRef]
- Ille, S.; Engel, L.; Kelm, A.; Meyer, B.; Krieg, S.M. Language-Eloquent White Matter Pathway Tractography and the Course of Language Function in Glioma Patients. Front. Oncol. 2018, 8, 572. [Google Scholar] [CrossRef]
- Raffa, G.; Bahrend, I.; Schneider, H.; Faust, K.; Germano, A.; Vajkoczy, P.; Picht, T. A Novel Technique for Region and Linguistic Specific nTMS-based DTI Fiber Tracking of Language Pathways in Brain Tumor Patients. Front. Neurosci. 2016, 10, 552. [Google Scholar] [CrossRef]
- Ille, S.; Gempt, J.; Meyer, B.; Krieg, S.M. nTMS guidance of awake surgery for highly eloquent gliomas. Neurosurg. Focus 2018, 45, V9. [Google Scholar] [CrossRef] [PubMed]
- Ille, S.; Sollmann, N.; Butenschoen, V.M.; Meyer, B.; Ringel, F.; Krieg, S.M. Resection of highly language-eloquent brain lesions based purely on rTMS language mapping without awake surgery. Acta Neurochir. 2016, 158, 2265–2275. [Google Scholar] [CrossRef] [PubMed]
- Hendrix, P.; Senger, S.; Simgen, A.; Griessenauer, C.J.; Oertel, J. Preoperative rTMS Language Mapping in Speech-Eloquent Brain Lesions Resected Under General Anesthesia: A Pair-Matched Cohort Study. World Neurosurg. 2017, 100, 425–433. [Google Scholar] [CrossRef] [PubMed]
- Duffau, H.; Moritz-Gasser, S.; Mandonnet, E. A re-examination of neural basis of language processing: Proposal of a dynamic hodotopical model from data provided by brain stimulation mapping during picture naming. Brain Lang. 2014, 131, 1–10. [Google Scholar] [CrossRef]
- Chang, E.F.; Raygor, K.P.; Berger, M.S. Contemporary model of language organization: An overview for neurosurgeons. J. Neurosurg. 2015, 122, 250–261. [Google Scholar] [CrossRef]
- Ille, S.; Picht, T.; Shiban, E.; Meyer, B.; Vajkoczy, P.; Krieg, S.M. The impact of nTMS mapping on treatment of brain AVMs. Acta Neurochir. 2018, 160, 567–578. [Google Scholar] [CrossRef]
- Rossini, P.M.; Burke, D.; Chen, R.; Cohen, L.G.; Daskalakis, Z.; Di Iorio, R.; Di Lazzaro, V.; Ferreri, F.; Fitzgerald, P.B.; George, M.S.; et al. Non-invasive electrical and magnetic stimulation of the brain, spinal cord, roots and peripheral nerves: Basic principles and procedures for routine clinical and research application. An updated report from an I.F.C.N. Committee. Clin. Neurophysiol. 2015, 126, 1071–1107. [Google Scholar] [CrossRef]
- Southwell, D.G.; Birk, H.S.; Han, S.J.; Li, J.; Sall, J.W.; Berger, M.S. Resection of gliomas deemed inoperable by neurosurgeons based on preoperative imaging studies. J. Neurosurg. 2018, 129, 567–575. [Google Scholar] [CrossRef] [Green Version]
- Bloch, O.; Han, S.J.; Cha, S.; Sun, M.Z.; Aghi, M.K.; McDermott, M.W.; Berger, M.S.; Parsa, A.T. Impact of extent of resection for recurrent glioblastoma on overall survival: Clinical article. J. Neurosurg. 2012, 117, 1032–1038. [Google Scholar] [CrossRef]
- Krieg, S.; Lioumis, P.; Mäkelä, J.; Wilenus, J.; Karhu, J.; Hannula, H.; Savolainen, P.; Weiss Lucas, C.; Seidel, K.; Laakso, A.; et al. Protocol for Motor and Language Mapping by Navigated TMS in Patients and Healthy Volunteers; workshop report. Acta Neurochir. 2017, 159, 1187–1195. [Google Scholar] [CrossRef] [Green Version]
- Negwer, C.; Ille, S.; Hauck, T.; Sollmann, N.; Maurer, S.; Kirschke, J.S.; Ringel, F.; Meyer, B.; Krieg, S.M. Visualization of subcortical language pathways by diffusion tensor imaging fiber tracking based on rTMS language mapping. Brain Imaging Behav. 2016. [Google Scholar] [CrossRef]
- Duffau, H. The usefulness of the asleep-awake-asleep glioma surgery. Acta Neurochir. 2014, 156, 1493–1494. [Google Scholar] [CrossRef]
- Hervey-Jumper, S.L.; Li, J.; Lau, D.; Molinaro, A.M.; Perry, D.W.; Meng, L.; Berger, M.S. Awake craniotomy to maximize glioma resection: Methods and technical nuances over a 27-year period. J. Neurosurg. 2015, 123, 325–339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ius, T.; Angelini, E.; Thiebaut de Schotten, M.; Mandonnet, E.; Duffau, H. Evidence for potentials and limitations of brain plasticity using an atlas of functional resectability of WHO grade II gliomas: Towards a “minimal common brain”. Neuroimage 2011, 56, 992–1000. [Google Scholar] [CrossRef] [PubMed]
- De Witt Hamer, P.C.; Hendriks, E.J.; Mandonnet, E.; Barkhof, F.; Zwinderman, A.H.; Duffau, H. Resection probability maps for quality assessment of glioma surgery without brain location bias. PLoS ONE 2013, 8, e73353. [Google Scholar] [CrossRef] [PubMed]
- Tate, M.C.; Herbet, G.; Moritz-Gasser, S.; Tate, J.E.; Duffau, H. Probabilistic map of critical functional regions of the human cerebral cortex: Broca’s area revisited. Brain A J. Neurol. 2014, 137, 2773–2782. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Classification | Points | ||
|---|---|---|---|
| High | Cortical | Opercular inferior frontal gyrus | 3 |
| Posterior supramarginal gyrus | |||
| Angular gyrus | |||
| Posterior middle frontal gyrus | |||
| Posterior superior temporal gyrus | |||
| Middle superior temporal gyrus | |||
| Subcortical | Arcuate fasciculus/deep superior longitudinal fasciculus | ||
| Superior longitudinal fasciculus II & III | |||
| Inferior fronto-occipital fasciculus | |||
| Uncinate fasciculus | |||
| Clinical | Preoperative language deficit * due to tumor growth | 2 | |
| Postoperative language deficit * after prior resection ** | |||
| Moderate | Cortical | Triangular inferior frontal gyrus | 2 |
| Anterior supramarginal gyrus | |||
| Middle middle frontal gyrus | |||
| Posterior middle temporal gyrus | |||
| Middle middle temporal gyrus | |||
| Posterior superior frontal gyrus | |||
| <5 mm to Co3 | |||
| Subcortical | Middle longitudinal fasciculus | ||
| Inferior longitudinal fasciculus | |||
| 5–10 mm to S3 | |||
| Clinical | Focal seizure accompanied by language deficit | 1 | |
| Low | Cortical | >5 mm to Co3 | 0 |
| Not within Co2 | |||
| Subcortical | >10 mm to S3 | ||
| >5 mm to S2 | |||
| Clinical | No clinical history of language impairment | ||
| Grading | Cases | nrTMS | Awake | p-Value | |
|---|---|---|---|---|---|
| 36 (36.0) | 40 (85.1) | ||||
| Grading high | Rating | Co3 | 18 (50.0) | 34 (85.0) | 0.0228 |
| Co2 | 17 (47.2) | 6 (15.0) | |||
| S3 | 32 (88.9) | 36 (90.0) | |||
| S2 | 4 (11.1) | 4 (10.0) | |||
| Cl2 | 25 (69.4) | 28 (70.0) | |||
| Cl1 | 13 (36.1) | 6 (15.0) | |||
| Sum of points | 6 | 11 (30.6) | 10 (25.0) | 0.2022 | |
| 7 | 14 (38.9) | 10 (25.0) | |||
| 8 | 8 (22.2) | 18 (45.0) | |||
| 9 | 3 (8.3) | 2 (5.0) | |||
| Outcome | no new | 25 (69.4) | 22 (55.0) | 0.4205 | |
| transient | 7 (19.4) | 14 (35.0) | |||
| permanent | 2 (5.6) | 3 (7.5) | |||
| complication | 2 (5.6) | 1 (2.5) | |||
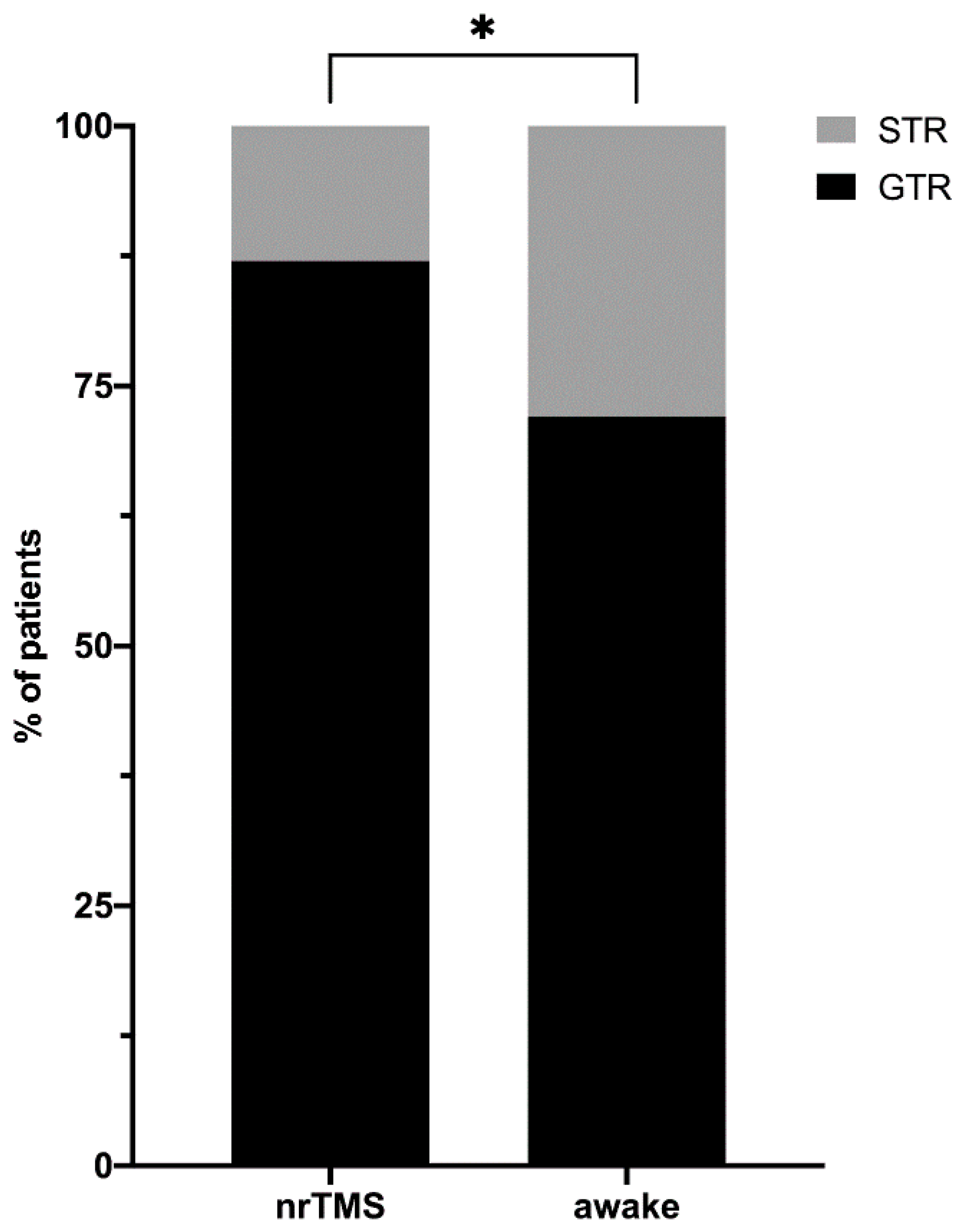
| EOR | GTR | 30 (83.3) | 28 (70.0) | 0.1903 | |
| STR | 6 (16.7) | 12 (30.0) | |||
| Cases | 53 (53.0) | 7 (14.9) | |||
| Grading moderate | Rating | Co3 | 4 (7.5) | 0 | 0.2474 |
| Co2 | 25 (47.2) | 7 (100) | |||
| S3 | 27 (50.9) | 5 (71.4) | |||
| S2 | 21 (39.6) | 1 (14.3) | |||
| Cl2 | 10 (18.9) | 1 (14.3) | |||
| Cl1 | 12 (22.6) | 0 | |||
| Sum of points | 3 | 15 (28.3) | 0 | 0.1725 | |
| 4 | 18 (34.0) | 2 (28.6) | |||
| 5 | 20 (37.7) | 5 (71.4) | |||
| Outcome | no new | 36 (67.9) | 6 (85.7) | 0.9253 | |
| transient | 10 (18.9) | 1 (14.3) | |||
| permanent | 1 (1.9) | 0 | |||
| complication | 6 (11.3) | 0 | |||
| EOR | GTR | 46 (86.8) | 6 (85.7) | >0.9999 | |
| STR | 7 (13.2) | 1 (14.3) | |||
| Classification | nrTMS | Awake | p-Value | |
|---|---|---|---|---|
| Rating | Co3 | 22 (22.0) | 34 (72.3) | <0.0001 |
| Co2 | 44 (44.0) | 13 (27.7) | ||
| S3 | 59 (59.0) | 41 (87.2) | ||
| S2 | 31 (31.0) | 5 (10.6) | ||
| Cl2 | 35 (35.0) | 29 (61.7) | ||
| Cl1 | 28 (28.0) | 6 (12.8) | ||
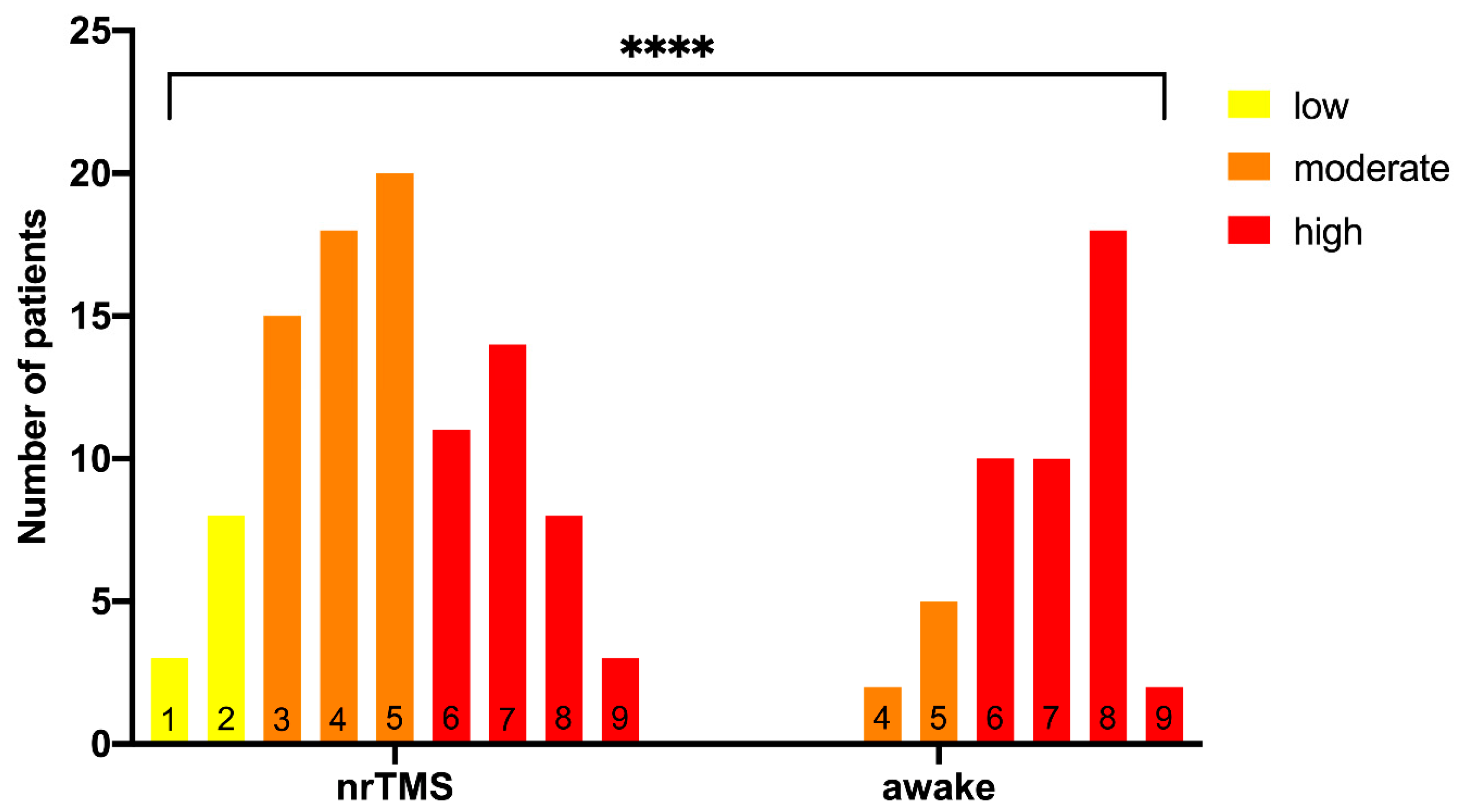
| Sum of points | 1 | 3 (3.0) | <0.0001 | |
| 2 | 8 (8.0) | |||
| 3 | 15 (15.0) | |||
| 4 | 18 (18.0) | 2 (4.3) | ||
| 5 | 20 (20.0) | 5 (10.6) | ||
| 6 | 11 (11.0) | 10 (21.3) | ||
| 7 | 14 (14.0) | 10 (21.3) | ||
| 8 | 8 (8.0) | 18 (38.3) | ||
| 9 | 3 (3.0) | 2 (4.3) | ||
| Grading | high | 36 (36.0) | 40 (85.1) | <0.0001 |
| moderate | 53 (53.0) | 7 (14.9) | ||
| low | 11 (11.0) | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ille, S.; Schroeder, A.; Albers, L.; Kelm, A.; Droese, D.; Meyer, B.; Krieg, S.M. Non-Invasive Mapping for Effective Preoperative Guidance to Approach Highly Language-Eloquent Gliomas—A Large Scale Comparative Cohort Study Using a New Classification for Language Eloquence. Cancers 2021, 13, 207. https://doi.org/10.3390/cancers13020207
Ille S, Schroeder A, Albers L, Kelm A, Droese D, Meyer B, Krieg SM. Non-Invasive Mapping for Effective Preoperative Guidance to Approach Highly Language-Eloquent Gliomas—A Large Scale Comparative Cohort Study Using a New Classification for Language Eloquence. Cancers. 2021; 13(2):207. https://doi.org/10.3390/cancers13020207
Chicago/Turabian StyleIlle, Sebastian, Axel Schroeder, Lucia Albers, Anna Kelm, Doris Droese, Bernhard Meyer, and Sandro M. Krieg. 2021. "Non-Invasive Mapping for Effective Preoperative Guidance to Approach Highly Language-Eloquent Gliomas—A Large Scale Comparative Cohort Study Using a New Classification for Language Eloquence" Cancers 13, no. 2: 207. https://doi.org/10.3390/cancers13020207
APA StyleIlle, S., Schroeder, A., Albers, L., Kelm, A., Droese, D., Meyer, B., & Krieg, S. M. (2021). Non-Invasive Mapping for Effective Preoperative Guidance to Approach Highly Language-Eloquent Gliomas—A Large Scale Comparative Cohort Study Using a New Classification for Language Eloquence. Cancers, 13(2), 207. https://doi.org/10.3390/cancers13020207