Global Trends of Latent Prostate Cancer in Autopsy Studies


Abstract
:Simple Summary
Abstract
1. Introduction
2. Potential Biases in Methodology in Latent PC Studies
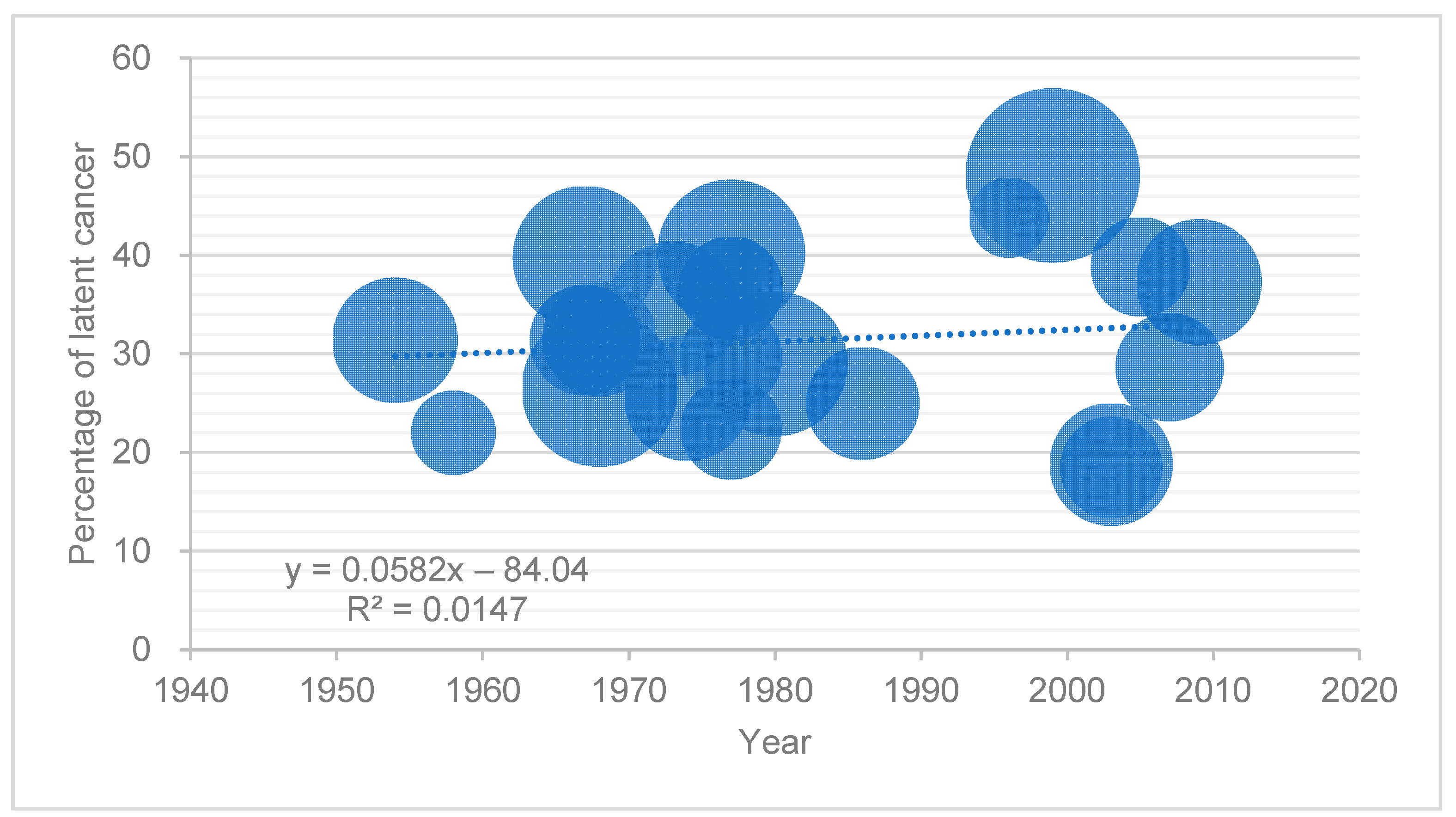
3. Prevalence of Latent PC in Western Countries
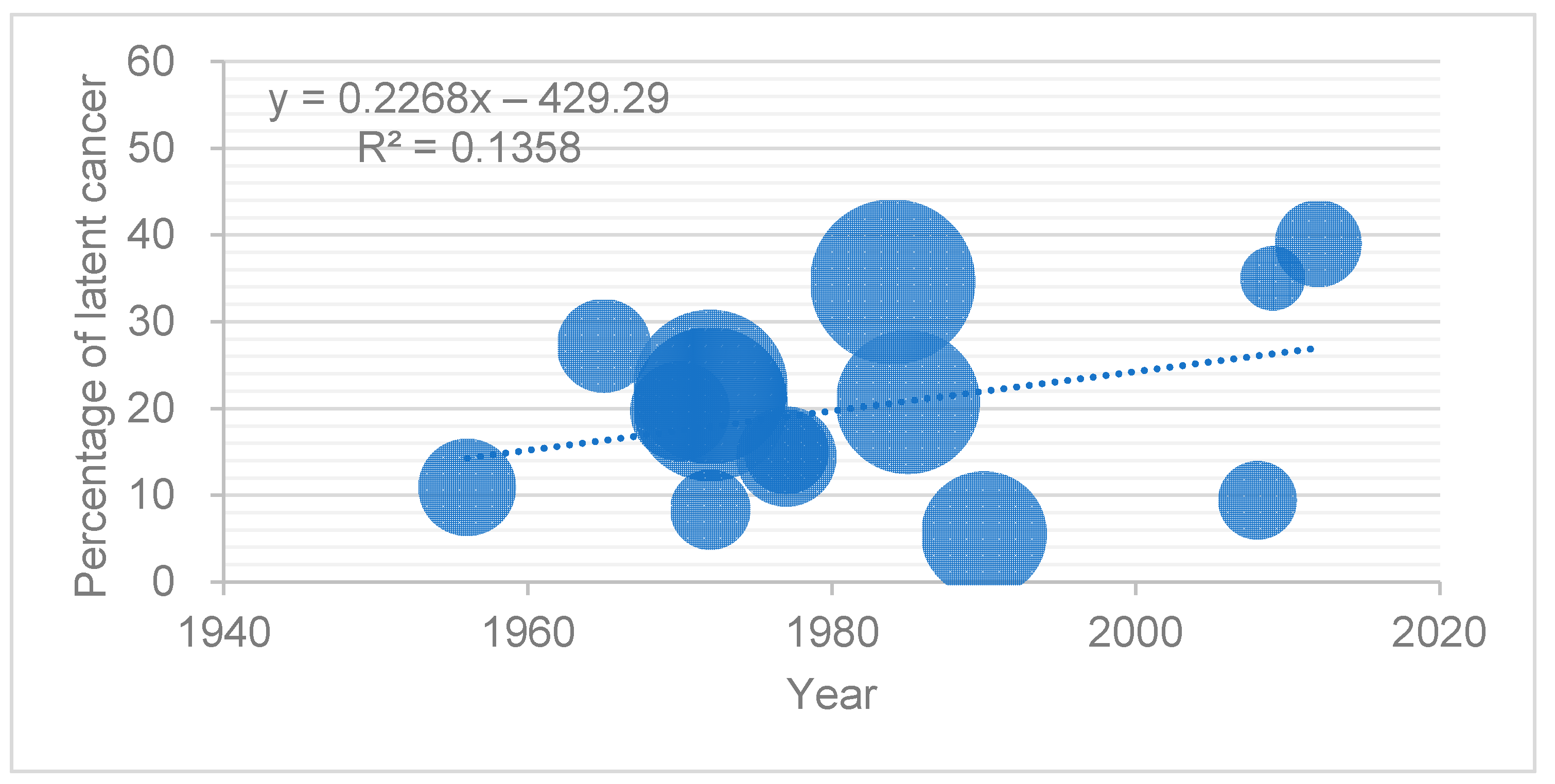
4. The prevalence of Latent PC in Asian and Other Countries
5. Pathological Findings from Latent PC
6. Limitations of Autopsy Studies
7. Learning from Latent PC and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: Globocan estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ito, K. Prostate cancer in asian men. Nat. Rev. Urol. 2014, 11, 197–212. [Google Scholar] [CrossRef] [PubMed]
- Yoshita, K.; Arai, Y.; Nozue, M.; Komatsu, K.; Ohnishi, H.; Saitoh, S.; Miura, K.; Group, N.D.R. Total energy intake and intake of three major nutrients by body mass index in japan: Nippon data80 and nippon data90. J. Epidemiol. 2010, 20 (Suppl. S3), S515–S523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iwasaki, M.; Mameri, C.P.; Hamada, G.S.; Tsugane, S. Cancer mortality among japanese immigrants and their descendants in the state of sao paulo, brazil, 1999–2001. JPN J. Clin Oncol. 2004, 34, 673–680. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mintz, E.R.; Smith, G.G. Autopsy findings in 100 cases of prostatic cancer. N. Engl. J. Med. 1934, 211, 479–487. [Google Scholar] [CrossRef]
- Bell, K.J.; Del Mar, C.; Wright, G.; Dickinson, J.; Glasziou, P. Prevalence of incidental prostate cancer: A systematic review of autopsy studies. Int. J. Cancer 2015, 137, 1749–1757. [Google Scholar] [CrossRef]
- Kimura, T.; Takahashi, H.; Okayasu, M.; Kido, M.; Inaba, H.; Kuruma, H.; Yamamoto, T.; Furusato, B.; Furusato, M.; Wada, T.; et al. Time trends in histological features of latent prostate cancer in japan. J. Urol. 2016, 195, 1415–1420. [Google Scholar] [CrossRef]
- Zlotta, A.R.; Egawa, S.; Pushkar, D.; Govorov, A.; Kimura, T.; Kido, M.; Takahashi, H.; Kuk, C.; Kovylina, M.; Aldaoud, N.; et al. Prevalence of prostate cancer on autopsy: Cross-sectional study on unscreened caucasian and asian men. J. Natl. Cancer Inst. 2013, 105, 1050–1058. [Google Scholar] [CrossRef] [Green Version]
- Rebbeck, T.R.; Haas, G.P. Temporal trends and racial disparities in global prostate cancer prevalence. Can. J. Urol. 2014, 21, 7496–7506. [Google Scholar] [PubMed]
- Moore, R.A. The morphology of small prostatic carcinoma. J. Urol. 1935, 33, 224–234. [Google Scholar] [CrossRef]
- Andrews, G.S. Latent carcinoma of the prostate. J. Clin. Pathol 1949, 2, 197–208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edwards, C.N.; Steinthorsson, E.; Nicholson, D. An autopsy study of latent prostatic cancer. Cancer 1953, 6, 531–554. [Google Scholar] [CrossRef]
- Franks, L.M. Latent carcinoma. Ann. R Coll. Surg. Engl. 1954, 15, 236–249. [Google Scholar] [PubMed]
- Viitanen, I.; Von Hellens, A. Latent carcinoma of the prostate in finland; preliminary report. Acta Pathol. Microbiol. Scand. 1958, 44, 64–67. [Google Scholar] [CrossRef] [PubMed]
- Halpert, B.; Schmalhorst, W.R. Carcinoma of the prostate in patients 70 to 79 years old. Cancer 1966, 19, 695–698. [Google Scholar] [CrossRef]
- Liavag, I. The localization of prostatic carcinoma. An autopsy study. Scand. J. Urol. Nephrol. 1968, 2, 65–71. [Google Scholar] [CrossRef]
- Lundberg, S.; Berge, T. Prostatic carcinoma. An autopsy study. Scand. J. Urol. Nephrol. 1970, 4, 93–97. [Google Scholar] [CrossRef]
- Harbitz, T.B. Testis weight and the histology of the prostate in elderly men. An analysis in an autopsy series. Acta Pathol. Microbiol. Scand. A 1973, 81, 148–158. [Google Scholar] [CrossRef]
- Akazaki, K.; Stemmerman, G.N. Comparative study of latent carcinoma of the prostate among japanese in Japan and Hawaii. J. Natl. Cancer Inst. 1973, 50, 1137–1144. [Google Scholar] [CrossRef]
- Breslow, N.; Chan, C.W.; Dhom, G.; Drury, R.A.; Franks, L.M.; Gellei, B.; Lee, Y.S.; Lundberg, S.; Sparke, B.; Sternby, N.H.; et al. Latent carcinoma of prostate at autopsy in seven areas. The international agency for research on cancer, lyons, france. Int. J. Cancer 1977, 20, 680–688. [Google Scholar] [CrossRef]
- Holund, B. Latent prostatic cancer in a consecutive autopsy series. Scand. J. Urol. Nephrol. 1980, 14, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Guileyardo, J.M.; Johnson, W.D.; Welsh, R.A.; Akazaki, K.; Correa, P. Prevalence of latent prostate carcinoma in two U.S. populations. J. Natl. Cancer Inst. 1980, 65, 311–316. [Google Scholar] [CrossRef] [PubMed]
- Yatani, R.; Chigusa, I.; Akazaki, K.; Stemmermann, G.N.; Welsh, R.A.; Correa, P. Geographic pathology of latent prostatic carcinoma. Int. J. Cancer 1982, 29, 611–616. [Google Scholar] [CrossRef] [PubMed]
- Stemmermann, G.N.; Nomura, A.M.; Chyou, P.H.; Yatani, R. A prospective comparison of prostate cancer at autopsy and as a clinical event: The Hawaii Japanese experience. Cancer Epidemiol. Biomark. Prev. 1992, 1, 189–193. [Google Scholar] [PubMed]
- Sakr, W.A.; Haas, G.P.; Cassin, B.F.; Pontes, J.E.; Crissman, J.D. The frequency of carcinoma and intraepithelial neoplasia of the prostate in young male patients. J. Urol. 1993, 150, 379–385. [Google Scholar] [CrossRef]
- Brawn, P.N.; Jay, D.W.; Foster, D.M.; Kuhl, D.; Speights, V.O.; Johnson, F.H.; Riggs, M.; Lind, M.L.; Coffield, K.S.; Weaver, B. Prostatic acid phosphatase levels (enzymatic method) from completely sectioned, clinically benign, whole prostates. Prostate 1996, 28, 295–299. [Google Scholar] [CrossRef]
- Billis, A. Latent carcinoma and atypical lesions of prostate an autopsy study. Urology 1986, 28, 324–329. [Google Scholar] [CrossRef]
- Sanchez-Chapado, M.; Olmedilla, G.; Cabeza, M.; Donat, E.; Ruiz, A. Prevalence of prostate cancer and prostatic intraepithelial neoplasia in caucasian mediterranean males: An autopsy study. Prostate 2003, 54, 238–247. [Google Scholar] [CrossRef] [PubMed]
- Soos, G.; Tsakiris, I.; Szanto, J.; Turzo, C.; Haas, P.G.; Dezso, B. The prevalence of prostate carcinoma and its precursor in hungary: An autopsy study. Eur. Urol. 2005, 48, 739–744. [Google Scholar] [CrossRef]
- Stamatiou, K.; Alevizos, A.; Perimeni, D.; Sofras, F.; Agapitos, E. Frequency of impalpable prostate adenocarcinoma and precancerous conditions in greek male population: An autopsy study. Prostate Cancer Prostatic Dis. 2006, 9, 45–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haas, G.P.; Delongchamps, N.B.; Jones, R.F.; Chandan, V.; Serio, A.M.; Vickers, A.J.; Jumbelic, M.; Threatte, G.; Korets, R.; Lilja, H.; et al. Needle biopsies on autopsy prostates: Sensitivity of cancer detection based on true prevalence. J. Natl. Cancer Inst. 2007, 99, 1484–1489. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polat, K.; Tüzel, E.; Aktepe, F.; Akdoğan, B.; Güler, C.; Uzun, I. Investigation of the incidence of latent prostate cancer and high-grade prostatic intraepithelial neoplasia in an autopsy series of Turkish males. Turk. J. Urol. 2009, 35, 96–100. [Google Scholar]
- Powell, I.J.; Bock, C.H.; Ruterbusch, J.J.; Sakr, W. Evidence supports a faster growth rate and/or earlier transformation to clinically significant prostate cancer in black than in white american men, and influences racial progression and mortality disparity. J. Urol. 2010, 183, 1792–1796. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jahn, J.L.; Giovannucci, E.L.; Stampfer, M.J. The high prevalence of undiagnosed prostate cancer at autopsy: Implications for epidemiology and treatment of prostate cancer in the prostate-specific antigen-era. Int. J. Cancer 2015, 137, 2795–2802. [Google Scholar] [CrossRef]
- Konety, B.R.; Bird, V.Y.; Deorah, S.; Dahmoush, L. Comparison of the incidence of latent prostate cancer detected at autopsy before and after the prostate specific antigen era. J. Urol. 2005, 174, 1785–1788; discussion 1788. [Google Scholar] [CrossRef] [PubMed]
- Karube, K. Study of latent carcinoma of the prostate in the japanese based on necropsy material. Tohoku J. Exp. Med. 1961, 74, 265–285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, Y.S.; Shanmugaratnam, K. Latent prostate carcinoma in Singapore Chinese. Singap. Med. J. 1972, 13, 1–6. [Google Scholar]
- Bean, M.A.; Yatani, R.; Liu, P.I.; Fukazawa, K.; Ashley, F.W.; Fujita, S. Prostatic carcinoma at autopsy in hiroshima and nagasaki japanese. Cancer 1973, 32, 498–506. [Google Scholar] [CrossRef]
- Yatani, R.; Shiraishi, T.; Nakakuki, K.; Kusano, I.; Takanari, H.; Hayashi, T.; Stemmermann, G.N. Trends in frequency of latent prostate carcinoma in japan from 1965–1979 to 1982–1986. J. Natl. Cancer Inst. 1988, 80, 683–687. [Google Scholar] [CrossRef]
- Takahashi, S.; Shirai, T.; Hasegawa, R.; Imaida, K.; Ito, N. Latent prostatic carcinomas found at autopsy in men over 90 years old. JPN J. Clin. Oncol. 1992, 22, 117–121. [Google Scholar] [CrossRef]
- Gu, F.-L.; Xia, T.-L.; Kong, X.-T. Preliminary study of the frequency ofbenign prostatic hyperplasia and prostatic cancer in china. Urology 1994, 44, 688–691. [Google Scholar] [CrossRef]
- Zare-Mirzaie, A.; Balvayeh, P.; Imamhadi, M.A.; Lotfi, M. The frequency of latent prostate carcinoma in autopsies of over 50 years old males, the Iranian experience. Med. J. Islam. Repub. Iran. 2012, 26, 73–77. [Google Scholar] [PubMed]
- Inaba, H.; Kimura, T.; Onuma, H.; Sato, S.; Kido, M.; Yamamoto, T.; Fukuda, Y.; Takahashi, H.; Egawa, S. Tumor location and pathological features of latent and incidental prostate cancer in contemporary japanese men. J. Urol. 2020, 204, 267–272. [Google Scholar] [CrossRef] [PubMed]
- Billis, A.; Souza, C.A.F.; Piovesan, H. Histologic carcinoma of the prosate in autopsies frequency, origin, extension, grading and terminology. Braz. J. Urol. 2002, 28, 197–205. [Google Scholar]
- Kimura, T.; Egawa, S. Epidemiology of prostate cancer in asian countries. Int. J. Urol. 2018, 25, 524–531. [Google Scholar] [CrossRef] [Green Version]
- Cook, L.S.; Goldoft, M.; Schwartz, S.M.; Weiss, N.S. Incidence of adenocarcinoma of the prostate in asian immigrants to the united states and their descendants. J. Urol. 1999, 161, 152–155. [Google Scholar] [CrossRef]
- Epstein, J.I.; Walsh, P.C.; Carmichael, M.; Brendler, C.B. Pathologic and clinical findings to predict tumor extent of nonpalpable (stage t1c) prostate cancer. JAMA 1994, 271, 368–374. [Google Scholar] [CrossRef] [PubMed]
- Stamey, T.A.; Freiha, F.S.; McNeal, J.E.; Redwine, E.A.; Whittemore, A.S.; Schmid, H.P. Localized prostate cancer. Relationship of tumor volume to clinical significance for treatment of prostate cancer. Cancer 1993, 71, 933–938. [Google Scholar] [CrossRef]
- Chen, Y.; Yan, W. Implications from autopsy studies of latent prostate cancer. Nat. Rev. Urol. 2020, 17, 428–429. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, H.; Epstein, J.I.; Wakui, S.; Yamamoto, T.; Furusato, B.; Zhang, M. Differences in prostate cancer grade, stage, and location in radical prostatectomy specimens from united states and japan. Prostate 2014, 74, 321–325. [Google Scholar] [CrossRef]
- Hashine, K.; Ueno, Y.; Shinomori, K.; Ninomiya, I.; Teramoto, N.; Yamashita, N. Correlation between cancer location and oncological outcome after radical prostatectomy. Int. J. Urol. 2012, 19, 855–860. [Google Scholar] [CrossRef] [PubMed]
- Takashima, R.; Egawa, S.; Kuwao, S.; Baba, S. Anterior distribution of stage t1c nonpalpable tumors in radical prostatectomy specimens. Urology 2002, 59, 692–697. [Google Scholar] [CrossRef]
- Koppie, T.M.; Bianco, F.J., Jr.; Kuroiwa, K.; Reuter, V.E.; Guillonneau, B.; Eastham, J.A.; Scardino, P.T. The clinical features of anterior prostate cancers. BJU Int. 2006, 98, 1167–1171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Ahmadie, H.A.; Tickoo, S.K.; Olgac, S.; Gopalan, A.; Scardino, P.T.; Reuter, V.E.; Fine, S.W. Anterior-predominant prostatic tumors: Zone of origin and pathologic outcomes at radical prostatectomy. Am. J. Surg. Pathol. 2008, 32, 229–235. [Google Scholar] [CrossRef] [PubMed]
- Hossack, T.; Patel, M.I.; Huo, A.; Brenner, P.; Yuen, C.; Spernat, D.; Mathews, J.; Haynes, A.M.; Sutherland, R.; del Prado, W.; et al. Location and pathological characteristics of cancers in radical prostatectomy specimens identified by transperineal biopsy compared to transrectal biopsy. J. Urol. 2012, 188, 781–785. [Google Scholar] [CrossRef] [PubMed]
- Mygatt, J.; Sesterhenn, I.; Rosner, I.; Chen, Y.; Cullen, J.; Morris-Gore, T.; Barton, J.; Dobi, A.; Srivastava, S.; McLeod, D.; et al. Anterior tumors of the prostate: Clinicopathological features and outcomes. Prostate Cancer Prostatic Dis. 2014, 17, 75–80. [Google Scholar] [CrossRef] [PubMed]
- McNeal, J.E. Cancer volume and site of origin of adenocarcinoma in the prostate: Relationship to local and distant spread. Hum. Pathol. 1992, 23, 258–266. [Google Scholar] [CrossRef]
- Igawa, M.; Urakami, S.; Shiina, H.; Ishibe, T.; Usui, T.; Chodak, G.W. Association of nm23 protein levels in human prostates with proliferating cell nuclear antigen expression at autopsy. Eur. Urol. 1996, 30, 383–387. [Google Scholar] [CrossRef]
- Watanabe, M.; Shiraishi, T.; Yatani, R.; Nomura, A.M.; Stemmermann, G.N. International comparison on ras gene mutations in latent prostate carcinoma. Int. J. Cancer 1994, 58, 174–178. [Google Scholar] [CrossRef]
- Alipov, G.; Nakayama, T.; Ito, M.; Kawai, K.; Naito, S.; Nakashima, M.; Niino, D.; Sekine, I. Overexpression of ets-1 proto-oncogene in latent and clinical prostatic carcinomas. Histopathology 2005, 46, 202–208. [Google Scholar] [CrossRef] [PubMed]
- Maekawa, S.; Suzuki, M.; Arai, T.; Suzuki, M.; Kato, M.; Morikawa, T.; Kasuya, Y.; Kume, H.; Kitamura, T.; Homma, Y. Tmprss2 met160val polymorphism: Significant association with sporadic prostate cancer, but not with latent prostate cancer in Japanese men. Int. J. Urol. 2014, 21, 1234–1238. [Google Scholar] [CrossRef] [PubMed]
- Allsbrook, W.C., Jr.; Mangold, K.A.; Johnson, M.H.; Lane, R.B.; Lane, C.G.; Amin, M.B.; Bostwick, D.G.; Humphrey, P.A.; Jones, E.C.; Reuter, V.E.; et al. Interobserver reproducibility of gleason grading of prostatic carcinoma: Urologic pathologists. Hum. Pathol. 2001, 32, 74–80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dehner, L.P. The medical autopsy: Past, present, and dubious future. Mo. Med. 2010, 107, 94–100. [Google Scholar] [PubMed]
- Nemetz, P.N.; Tanglos, E.; Sands, L.P.; Fisher, W.P., Jr.; Newman, W.P., 3rd; Burton, E.C. Attitudes toward the autopsy—An 8-state survey. MedGenMed 2006, 8, 80. [Google Scholar] [PubMed]
- Xiao, J.; Krueger, G.R.; Buja, L.M.; Covinsky, M. The impact of declining clinical autopsy: Need for revised healthcare policy. Am. J. Med. Sci. 2009, 337, 41–46. [Google Scholar] [CrossRef] [PubMed]
- Japanese Pathological Society. Annual of the Pathological Autopsy Cases in Japan. Available online: http://pathology.or.jp/kankoubutu/autopsy-index.html (accessed on 19 January 2021).
- Duregon, E.; Schneider, J.; DeMarzo, A.M.; Hooper, J.E. Rapid research autopsy is a stealthy but growing contributor to cancer research. Cancer 2019, 125, 2915–2919. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Author | Year Published | Country/Ethnicity | Duration of Study | Study Population | No. of Cases | Age | No. of Cancers | % | Pathology Section Width (mm) | Ref. No. |
|---|---|---|---|---|---|---|---|---|---|---|
| Moore | 1935 | Austria | 1931–1932 | Hospital | 304 | Range, 21–90 | 52 | 16.7 | 4 | [10] |
| Andrews | 1949 | UK | NA | Hospital | 142 | Range, 40–79 | 17 | 12.0 | 4 | [11] |
| Edwards | 1953 | Canada | 1942–1945 | Hospital | 173 | Mean, 64.1 | 35 | 16.7 | 4 | [12] |
| Franks | 1954 | US | NA | Forensic | 220 | NA | 69 | 31.4 | 4 | [13] |
| Viitanen | 1958 | Finland | NA | Hospital | 100 | ≥50 | 22 | 22.0 | 5 | [14] |
| Halpert | 1965 | US/Black | NA | Hospital | 30 | Range, 70–79 | 13 | 43.3 | 4 | [15] |
| Halpert | 1965 | US/Caucasian | NA | Hospital | 70 | Range, 70–79 | 41 | 58.6 | 4 | [15] |
| Liavag | 1968 | Norway | NA | Hospital | 340 | ≥40 | 90 | 26.5 | 4 | [16] |
| Lundberg | 1970 | Sweden | 1967 | Hospital | 292 | NA | 116 | 39.7 | 5 | [17] |
| Harbitz | 1973 | Norway | 1967–1968 | Hospital | 172 | ≥40 | 54 | 31.4 | 4–6 | [18] |
| Akazaki | 1973 | US/men of Japanese ancestry | 1969–1972 | Hospital | 158 | ≥50 | 46 | 29.1 | 3 | [19] |
| Breslow | 1977 | Germany | NA | Hospital | 145 | Mean, 65 | 43 | 29.7 | 5 | [20] |
| Breslow | 1977 | Israel | NA | Hospital | 143 | Mean, 65 | 32 | 22.4 | 5 | [20] |
| Breslow | 1977 | Sweden | NA | Hospital | 306 | Mean, 65 | 123 | 40.2 | 5 | [20] |
| Hølund | 1980 | Denmark | 1971–1977 | Hospital | 223 | Range, 36–94 | 57 | 25.6 | 3 | [21] |
| Gulleyardo | 1980 | US/Black | NA | Hospital | 207 | NA | 65 | 31.4 | 3 | [22] |
| Gulleyardo | 1980 | US/Caucasian | NA | Hospital | 293 | NA | 85 | 29 | 3 | [22] |
| Yatani | 1982 | Colombia | 1967–1970 | Hospital | 182 | Mean, 64.4 | NA | 31.5 | 3 | [23] |
| Yatani | 1982 | US/Black | 1969–1978 | Hospital | 178 | Mean, 63.6 | NA | 36.9 | 3 | [23] |
| Yatani | 1982 | US/Caucasian | 1969–1978 | Hospital | 253 | Mean, 63.2 | NA | 34.6 | 3 | [23] |
| Yatani | 1982 | US/men of Japanese ancestry | 1969–1978 | Hospital | 417 | Mean, 70.1 | NA | 25.6 | 3 | [23] |
| Stemmermann | 1992 | US/men of Japanese ancestry | 1970–1990 | Hospital | 293 | Mean, 67.9 | 80 | 27.3 | 3 | [24] |
| Sakr | 1993 | US/Black | NA | Forensic | 98 | 10–50 | 19 | 19.4 | 3–4 | [25] |
| Sakr | 1993 | US/Caucasian | NA | Forensic | 54 | 10–50 | 14 | 25.9 | 3–4 | [25] |
| Brawn | 1996 | US/Black | NA | Hospital | 15 | ≥50 | 5 | 33.3 | 3 | [26] |
| Brawn | 1996 | US/Caucasian | NA | Hospital | 89 | ≥50 | 39 | 43.8 | 3 | [26] |
| Sanchez-Chapado | 2003 | Spain | NA | Forensic | 146 | Mean, 48.5 | 27 | 18.5 | 3-4 | [28] |
| Soos | 2005 | Hungary | NA | Hospital | 139 | 18–95 | 54 | 38.8 | 4 | [29] |
| Stamtiou | 2007 | Greece | 2002–2004 | Hospital | 212 | ≥30 | 40 | 18.8 | 4 | [30] |
| Haas | 2007 | US (92% Caucasian) | NA | Hospital | 164 | Median, 64 | 47 | 28.7 | 4 | [31] |
| Polat | 2009 | Turkey | NA | Hospital | 114 | Mean, 55 | 11 | 9.6 | 4 | [32] |
| Powell | 2010 | US/Black | 1993–2004 | Forensic | 630 | 20–79 | NA | 35.1 | 2.5 | [33] |
| Powell | 2010 | US/Caucasian | 1993–2004 | Forensic | 426 | 20–79 | NA | 48.1 | 2.5 | [33] |
| Zlotta | 2013 | Russia | 2008–2011 | Hospital | 220 | Mean, 62.5 | 82 | 37.3 | 4 | [8] |
| Author | Year Published | Country/Ethnicity | Duration of Study | Study Population | No. of Cases | Age | No. of Cancers | % | Pathology Section Width (mm) | Ref. No. |
|---|---|---|---|---|---|---|---|---|---|---|
| Karube | 1961 | Japan | 1954–1959 | Hospital | 229 | ≥40 | 25 | 10.9 | 4–5 | [36] |
| Lee | 1972 | Singapore | NA | Hospital | 156 | Range, 42–87 | 13 | 8.3 | 4 | [37] |
| Akazaki | 1973 | Japan | 1969–1972 | Hospital | 239 | ≥50 | 47 | 19.7 | 3 | [19] |
| Bean | 1973 | Japan | 1961–1969 | Hospital | 213 | ≥50 | 58 | 27.2 | 5 | [38] |
| Breslow | 1977 | Hong Kong | NA | Hospital | 173 | Mean, 65 | 26 | 15.0 | 5 | [20] |
| Breslow | 1977 | Jamaica | NA | Hospital | 168 | Mean, 65 | 55 | 32.7 | 5 | [20] |
| Breslow | 1977 | Singapore | NA | Hospital | 242 | Mean, 65 | 35 | 14.5 | 5 | [20] |
| Breslow | 1977 | Uganda | NA | Hospital | 150 | Mean, 65 | 36 | 24.0 | 5 | [20] |
| Yatani | 1982 | Japan | 1965–1979 | Hospital | 576 | Mean, 67.7 | NA | 20.5 | 3 | [23] |
| Billis | 1986 | Brazil | NA | Hospital | 180 | Range, 40–88 | 45 | 25.0 | 3–5 | [27] |
| Yatani | 1988 | Japan | 1965–1979 | Hospital | 576 | Mean, 67.6 | NA | 22.5 | 3 | [39] |
| Yatani | 1988 | Japan | 1982–1986 | Hospital | 660 | Mean, 68.7 | NA | 34.6 | 3 | [39] |
| Takahashi | 1992 | Japan | NA | Hospital | 29 | ≥90 | 17 | 58.6 | 3–4 | [40] |
| Gu | 1994 | China | 1989–1992 | Hospital | 381 (including 60 RCP) | NA | 21 | 5.5 | 5 | [41] |
| Zare–Mirzaie | 2012 | Iran | 2008–2009 | Hospital | 149 | Mean, 64.5 | 14 | 9.4 | 4 | [42] |
| Zlotta | 2013 | Japan | 2008–2011 | Hospital | 100 | Mean, 68.5 | 35 | 35.0 | 4 | [8] |
| Kimura | 2016 | Japan | 1983–1987 | Hospital | 501 | Mean, 63.5 | 104 | 20.8 | 5 | [7] |
| Inaba | 2020 | Japan | 2009–2017 | Hospital | 182 | Median, 72 | 71 | 39.0 | 5 | [43] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kimura, T.; Sato, S.; Takahashi, H.; Egawa, S. Global Trends of Latent Prostate Cancer in Autopsy Studies. Cancers 2021, 13, 359. https://doi.org/10.3390/cancers13020359
Kimura T, Sato S, Takahashi H, Egawa S. Global Trends of Latent Prostate Cancer in Autopsy Studies. Cancers. 2021; 13(2):359. https://doi.org/10.3390/cancers13020359
Chicago/Turabian StyleKimura, Takahiro, Shun Sato, Hiroyuki Takahashi, and Shin Egawa. 2021. "Global Trends of Latent Prostate Cancer in Autopsy Studies" Cancers 13, no. 2: 359. https://doi.org/10.3390/cancers13020359
APA StyleKimura, T., Sato, S., Takahashi, H., & Egawa, S. (2021). Global Trends of Latent Prostate Cancer in Autopsy Studies. Cancers, 13(2), 359. https://doi.org/10.3390/cancers13020359