
Hepatic Arterial Infusion Chemotherapy with Cisplatin versus Sorafenib for Intrahepatic Advanced Hepatocellular Carcinoma: A Propensity Score-Matched Analysis


 , , ,
, , ,  and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethical Approval
2.2. Diagnosis
2.3. Patients Receiving HAIC with Cisplatin
2.4. Patients Receiving Sorafenib
2.5. Treatment Outcome
2.6. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Univariate and Multivariate Analyses of OS
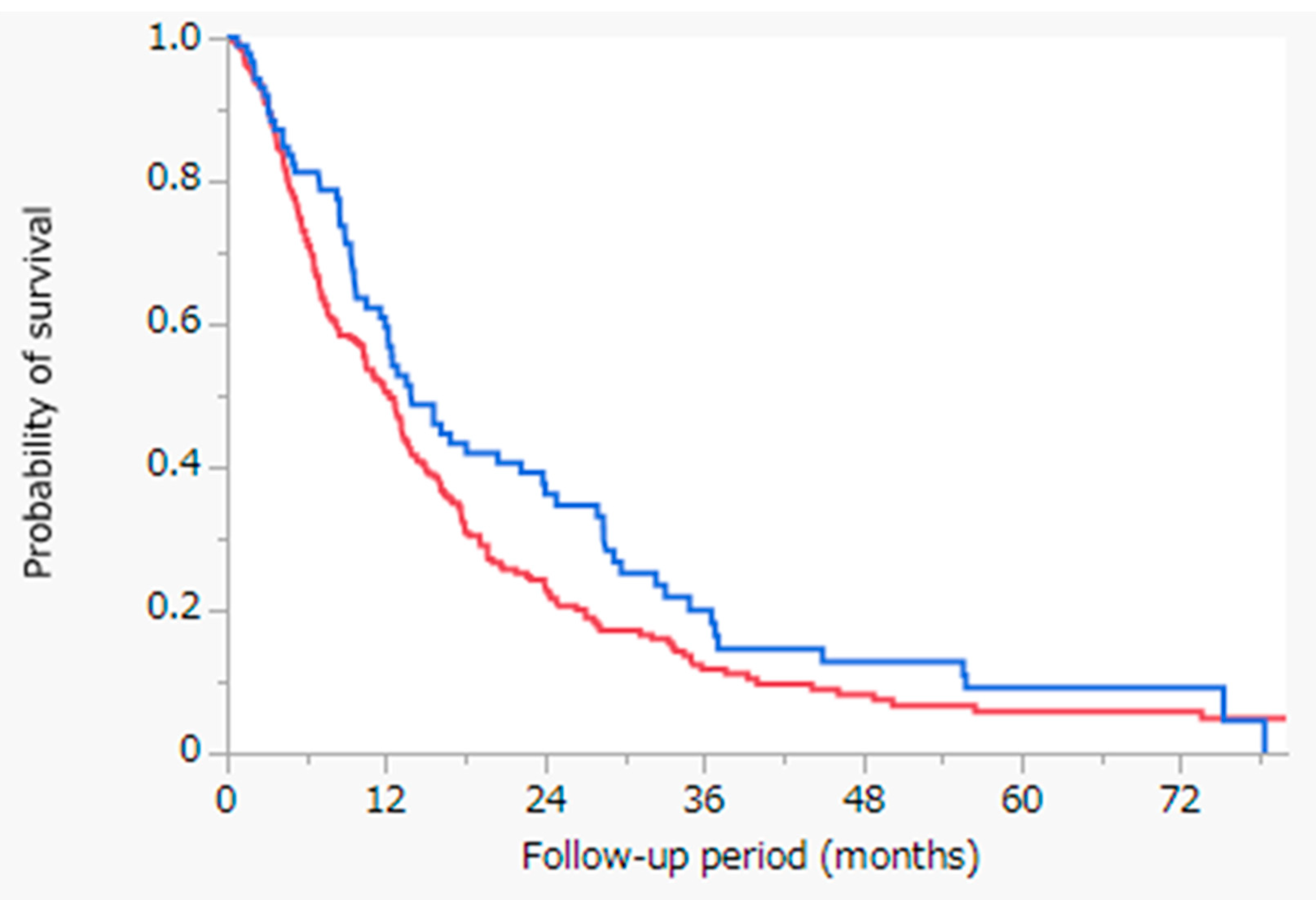
3.3. Survival Outcomes
3.4. Propensity Score-Matched Analysis
3.5. Characteristics of Patients Diagnosed with HCC Following Propensity Score-Matched Analysis
3.6. Transition of Treatment Following Propensity Score-Matched Analysis
3.7. Univariate and Multivariate Analyses of OS Following Propensity Score-Matched Analysis
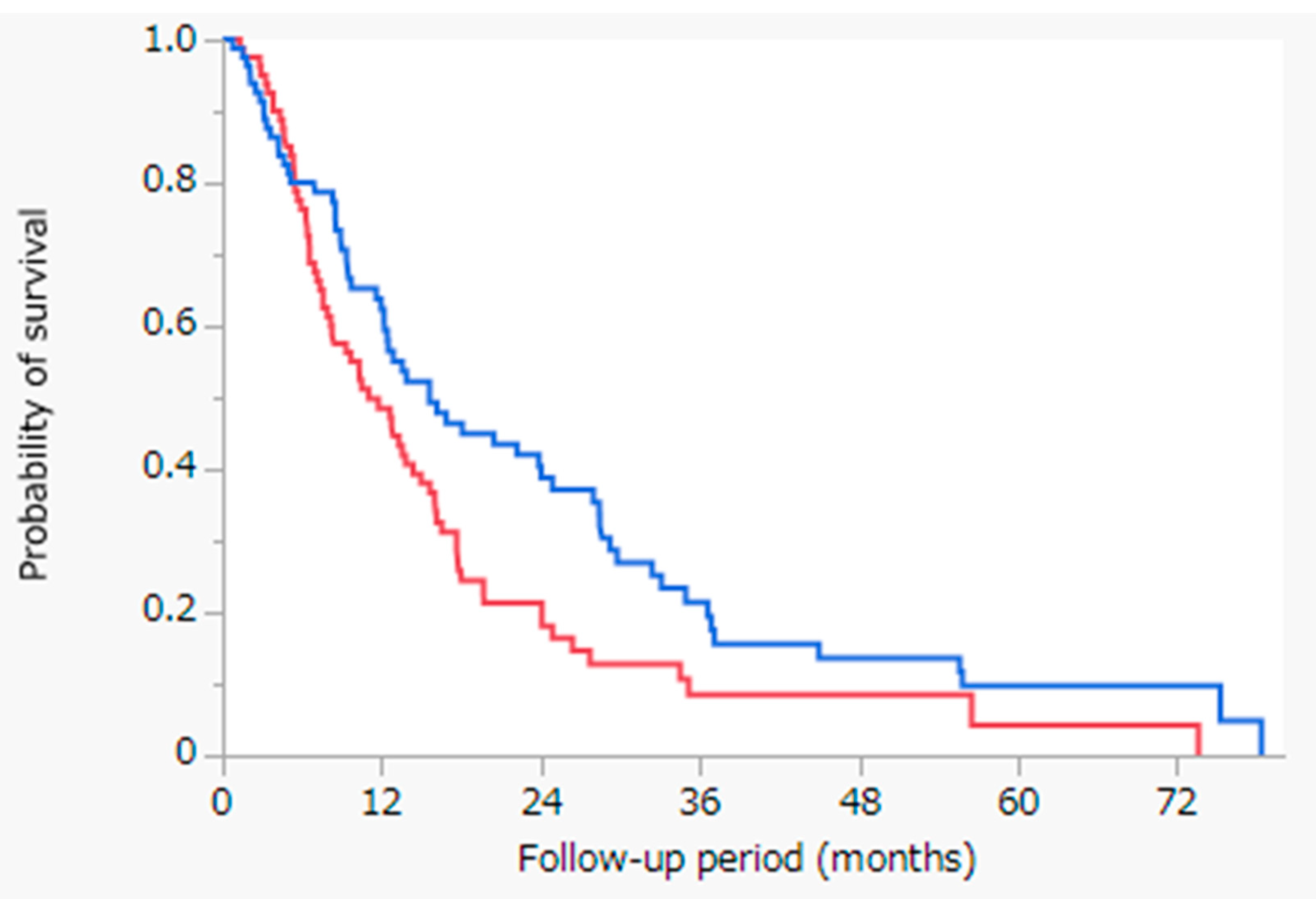
3.8. Survival Outcomes Following Propensity Score-Matched Analysis
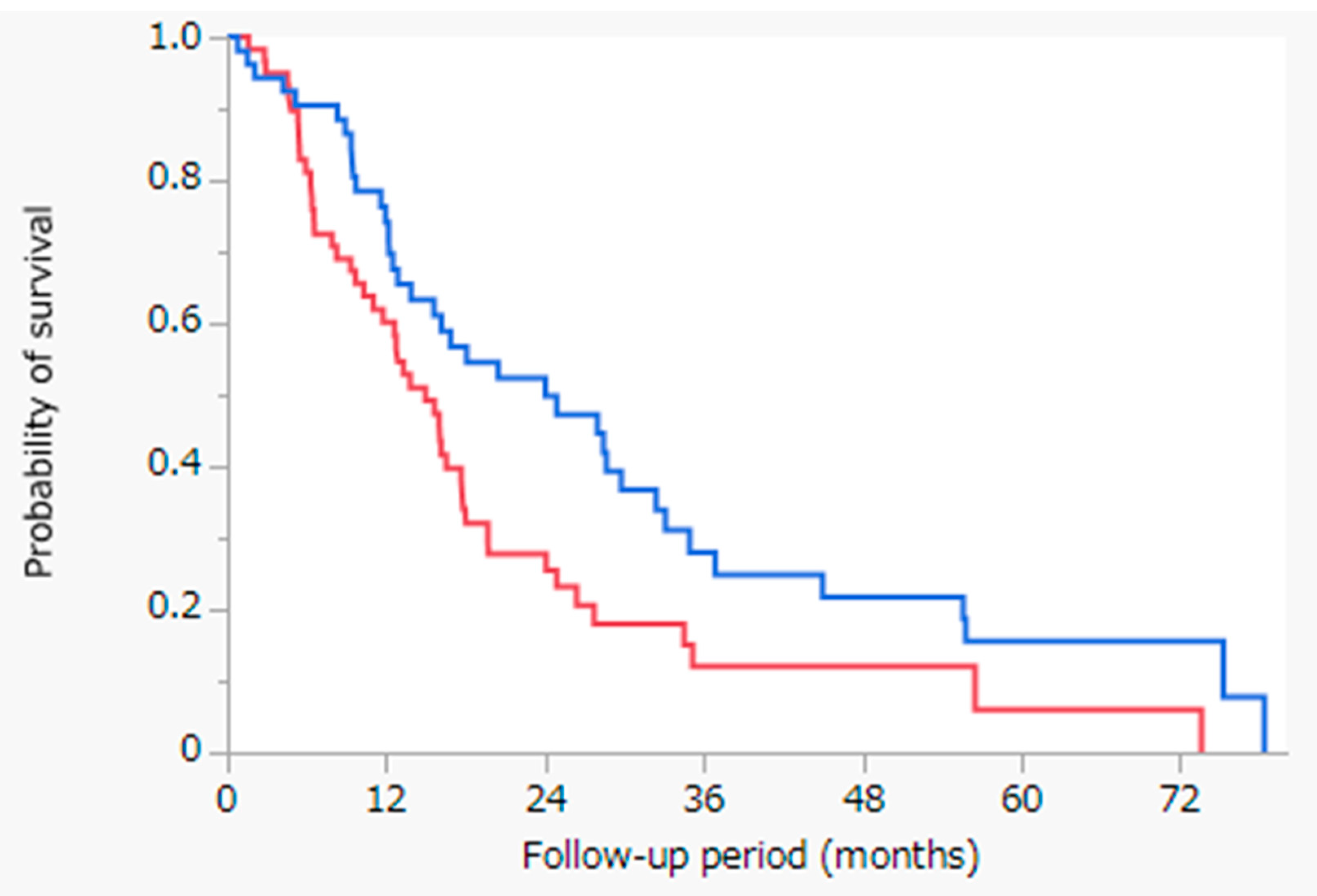
3.9. Survival Outcomes Having Child-Pugh Class A Following Propensity Score-Matched Analysis
3.10. Changes in Hepatic Reserve Factor before and 1 Month after Treatment Following Propensity Score-Matched Analysis
3.11. Adverse Events Following Propensity Score-Matched Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Me, J.F.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Singal, A.G.; Lampertico, P.; Nahon, P. Epidemiology and surveillance for hepatocellular carcinoma: New trends. J. Hepatol. 2020, 72, 250–261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Global Burden of Disease Liver Cancer Collaboration; Akinyemiju, T.; Abera, S.; Ahmed, M.; Alam, N.; Alemayohu, M.A.; Allen, C.; Al-Raddadi, R.; Alvis-Guzman, N.; Amoako, Y.; et al. The Burden of Primary Liver Cancer and Underlying Etiologies From 1990 to 2015 at the Global, Regional, and National Level. JAMA Oncol. 2017, 3, 1683–1691. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Naghavi, M.; Allen, C.; Barber, R.M.; Bhutta, Z.A.; Carter, A.; Casey, D.C.; Charlson, F.J.; Chen, A.Z.; Coates, M.M.; et al. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1459–1544. [Google Scholar] [CrossRef] [Green Version]
- Grandhi, M.S.; Kim, A.K.; Ronnekleiv-Kelly, S.; Kamel, I.R.; Ghasebeh, M.A.; Pawlik, T.M. Hepatocellular carcinoma: From diagnosis to treatment. Surg. Oncol. 2016, 25, 74–85. [Google Scholar] [CrossRef] [PubMed]
- Hartke, J.; Johnson, M.; Ghabril, M. The diagnosis and treatment of hepatocellular carcinoma. Semin. Diagn. Pathol. 2017, 34, 153–159. [Google Scholar] [CrossRef]
- Kokudo, N.; Takemura, N.; Hasegawa, K.; Takayama, T.; Kubo, S.; Shimada, M.; Nagano, H.; Hatano, E.; Izumi, N.; Kaneko, S.; et al. Clinical practice guidelines for hepatocellular carcinoma: The Japan Society of Hepatology 2017 (4th JSH-HCC guidelines) 2019 update. Hepatol. Res. 2019, 49, 1109–1113. [Google Scholar] [CrossRef]
- Iwamoto, H.; Niizeki, T.; Nagamatsu, H.; Ueshima, K.; Nomura, T.; Kuzuya, T.; Kasai, K.; Kooka, Y.; Hiraoka, A.; Sugimoto, R.; et al. Survival Benefit of Hepatic Arterial Infusion Chemotherapy over Sorafenib in the Treatment of Locally Progressed Hepatocellular Carcinoma. Cancers 2021, 13, 646. [Google Scholar] [CrossRef]
- Sung, P.S.; Yang, K.; Bae, S.H.; Oh, J.S.; Chun, H.J.; Nam, H.C.; Jang, J.W.; Choi, J.Y.; Yoon, S.K. Reduction of Intrahepatic Tumour by Hepatic Arterial Infusion Chemotherapy Prolongs Survival in Hepatocellular Carcinoma. Anticancer. Res. 2019, 39, 3909–3916. [Google Scholar] [CrossRef]
- Kang, M.K.; Gil Park, J.; Lee, H.J. Comparison of clinical outcomes between sorafenib and hepatic artery infusion chemotherapy in advanced hepatocellular carcinoma. Medicine 2018, 97, e0611. [Google Scholar] [CrossRef]
- Kodama, K.; Kawaoka, T.; Aikata, H.; Uchikawa, S.; Inagaki, Y.; Hatooka, M.; Morio, K.; Nakahara, T.; Murakami, E.; Tsuge, M.; et al. Comparison of clinical outcome of hepatic arterial infusion chemotherapy and sorafenib for advanced hepatocellular carcinoma according to macrovascular invasion and transcatheter arterial chemoembolization refractory status. J. Gastroenterol. Hepatol. 2018, 33, 1780–1786. [Google Scholar] [CrossRef]
- Llovet, J.M.; Ricci, S.; Mazzaferro, V.M.; Hilgard, P.; Gane, E.; Blanc, J.-F.; De Oliveira, A.C.; Santoro, A.; Raoul, J.-L.; Forner, A.; et al. Sorafenib in Advanced Hepatocellular Carcinoma. N. Engl. J. Med. 2008, 359, 378–390. [Google Scholar] [CrossRef] [PubMed]
- Cheng, A.-L.; Kang, Y.-K.; Chen, Z.; Tsao, C.-J.; Qin, S.; Kim, J.S.; Luo, R.; Feng, J.; Ye, S.; Yang, T.-S.; et al. Efficacy and safety of sorafenib in patients in the Asia-Pacific region with advanced hepatocellular carcinoma: A phase III randomised, double-blind, placebo-controlled trial. Lancet Oncol. 2008, 10, 25–34. [Google Scholar] [CrossRef]
- Finn, R.S.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.-Y.; Kudo, M.; Breder, V.; Merle, P.; Kaseb, A.O.; et al. Atezolizumab plus Bevacizumab in Unresectable Hepatocellular Carcinoma. N. Engl. J. Med. 2020, 382, 1894–1905. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, M.; Shimizu, S.; Sato, T.; Morimoto, M.; Kojima, Y.; Inaba, Y.; Hagihara, A.; Kudo, M.; Nakamori, S.; Kaneko, S.; et al. Sorafenib plus hepatic arterial infusion chemotherapy with cisplatin versus sorafenib for advanced hepatocellular carcinoma: Randomized phase II trial. Ann. Oncol. 2016, 27, 2090–2096. [Google Scholar] [CrossRef]
- Bruix, J.; Sherman, M.; Llovet, J.M.; Beaugrand, M.; Lencioni, R.; Burroughs, A.K.; Christensen, E.; Pagliaro, L.; Colombo, M.; Rodés, J. Clinical Management of Hepatocellular Carcinoma. Conclusions of the Barcelona-2000 EASL Conference. J. Hepatol. 2001, 35, 421–430. [Google Scholar] [CrossRef]
- Johnson, P.J.; Berhane, S.; Kagebayashi, C.; Satomura, S.; Teng, M.; Reeves, H.L.; O’Beirne, J.; Fox, R.; Skowronska, A.; Palmer, D.; et al. Assessment of Liver Function in Patients With Hepatocellular Carcinoma: A New Evidence-Based Approach—The ALBI Grade. J. Clin. Oncol. 2015, 33, 550–558. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Brú, C.; Bruix, J. Prognosis of Hepatocellular Carcinoma: The BCLC Staging Classification. Semin. Liver Dis. 1999, 19, 329–338. [Google Scholar] [CrossRef]
- Forner, A.; Reig, M.; Rodriguez-Lope, C.; Bruix, J. Current Strategy for Staging and Treatment: The BCLC Update and Future Prospects. Semin. Liver Dis. 2010, 30, 061–074. [Google Scholar] [CrossRef]
- Austin, P.C. The performance of different propensity score methods for estimating marginal hazard ratios. Stat. Med. 2012, 32, 2837–2849. [Google Scholar] [CrossRef] [Green Version]
- D’Agostino, R.B. Propensity score methods for bias reduction in the comparison of a treatment to a non-randomized control group. Stat. Med. 1998, 17, 2265–2281. [Google Scholar] [CrossRef]
- Johnson, S.R.; Tomlinson, G.; Hawker, G.A.; Granton, J.T.; Feldman, B.M. Propensity Score Methods for Bias Reduction in Observational Studies of Treatment Effect. Rheum. Dis. Clin. N. Am. 2018, 44, 203–213. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.; Won, J.H.; Kim, J.; Kwon, Y.; Cho, H.J.; Huh, J.; Kim, J.K. Hepatic Arterial Infusion Chemotherapy for Advanced Hepatocellular Carcinoma: Radiologic and Clinical Factors Predictive of Survival. Am. J. Roentgenol. 2021, 216, 1566–1573. [Google Scholar] [CrossRef] [PubMed]
- Bai, S.; Yang, P.; Xie, Z.; Li, J.; Lei, Z.; Xia, Y.; Qian, G.; Zhang, B.; Pawlik, T.M.; Lau, W.Y.; et al. Preoperative Estimated Risk of Microvascular Invasion is Associated with Prognostic Differences Following Liver Resection Versus Radiofrequency Ablation for Early Hepatitis B Virus-Related Hepatocellular Carcinoma. Ann. Surg. Oncol. 2021, 1–12. [Google Scholar] [CrossRef]
- Zhang, X.-P.; Chai, Z.-T.; Feng, J.-K.; Zhu, H.-M.; Zhang, F.; Hu, Y.-R.; Zhong, C.-Q.; Chen, Z.-H.; Wang, K.; Shi, J.; et al. Association of type 2 diabetes mellitus with incidences of microvascular invasion and survival outcomes in hepatitis B virus-related hepatocellular carcinoma after liver resection: A multicenter study. Eur. J. Surg. Oncol. (EJSO) 2021. [Google Scholar] [CrossRef]
- Obi, S.; Sato, S.; Kawai, T. Current Status of Hepatic Arterial Infusion Chemotherapy. Liver Cancer 2015, 4, 188–199. [Google Scholar] [CrossRef] [Green Version]
- Moriya, K.; Namisaki, T.; Sato, S.; Furukawa, M.; Douhara, A.; Kawaratani, H.; Kaji, K.; Shimozato, N.; Sawada, Y.; Saikawa, S.; et al. Bi-monthly hepatic arterial infusion chemotherapy as a novel strategy for advanced hepatocellular carcinoma in decompensated cirrhotic patients. Clin. Mol. Hepatol. 2019, 25, 381–389. [Google Scholar] [CrossRef] [Green Version]
- Kudo, M.; Ueshima, K.; Yokosuka, O.; Ogasawara, S.; Obi, S.; Izumi, N.; Aikata, H.; Nagano, H.; Hatano, E.; Sasaki, Y.; et al. Sorafenib plus low-dose cisplatin and fluorouracil hepatic arterial infusion chemotherapy versus sorafenib alone in patients with advanced hepatocellular carcinoma (SILIUS): A randomised, open label, phase 3 trial. Lancet Gastroenterol. Hepatol. 2018, 3, 424–432. [Google Scholar] [CrossRef]
- He, M.; Li, Q.; Zou, R.; Shen, J.; Fang, W.; Tan, G.; Zhou, Y.; Wu, X.; Xu, L.; Wei, W.; et al. Sorafenib Plus Hepatic Arterial Infusion of Oxaliplatin, Fluorouracil, and Leucovorin vs Sorafenib Alone for Hepatocellular Carcinoma With Portal Vein Invasion. JAMA Oncol. 2019, 5, 953–960. [Google Scholar] [CrossRef] [PubMed]
- Zhuang, B.-W.; Li, W.; Xie, X.-H.; Hu, H.-T.; Lu, M.-D.; Xie, X.-Y. Sorafenib versus hepatic arterial infusion chemotherapy for advanced hepatocellular carcinoma: A systematic review and meta-analysis. Jpn. J. Clin. Oncol. 2019, 49, 845–855. [Google Scholar] [CrossRef] [PubMed]
- Lyu, N.; Kong, Y.; Mu, L.; Lin, Y.; Li, J.; Liu, Y.; Zhang, Z.; Zheng, L.; Deng, H.; Li, S.; et al. Hepatic arterial infusion of oxaliplatin plus fluorouracil/leucovorin vs. sorafenib for advanced hepatocellular carcinoma. J. Hepatol. 2018, 69, 60–69. [Google Scholar] [CrossRef] [PubMed]
- Ueshima, K.; Ogasawara, S.; Ikeda, M.; Yasui, Y.; Terashima, T.; Yamashita, T.; Obi, S.; Sato, S.; Aikata, H.; Ohmura, T.; et al. Hepatic Arterial Infusion Chemotherapy versus Sorafenib in Patients with Advanced Hepatocellular Carcinoma. Liver Cancer 2020, 9, 583–595. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | HAIC (n = 88) | Sorafenib (n = 243) | p-Value |
|---|---|---|---|
| Age (years) | 73.8 ± 9.6 | 72.4 ± 9.5 | 0.2515 |
| 75.2 (47.8–88.6) | 72.8 (35.7–94.4) | ||
| Sex (male/female) | 61 (69%)/27 (31%) | 193 (79%)/50 (21%) | 0.0545 |
| Etiology (HBV/HCV/HBV + HCV/both negative) | 6 (7%)/71 (81%)/0 (0%)/11 (12%) | 37 (15%)/153 (63%)/3 (1%)/50 (21%) | 0.0196 |
| Child-Pugh class (A/B) | 56 (64%)/32 (36%) | 196 (81%)/47 (19%) | 0.0013 |
| Macrovascular invasion (yes/no) | 13 (15%)/75 (85%) | 65 (27%)/178 (73%) | 0.0233 |
| BCLC stage (B/C) | 71 (81%)/17 (19%) | 178 (73%)/65 (27%) | 0.1665 |
| Albumin (g/dL) | 3.4 ± 0.5 | 3.6 ± 0.5 | 0.0009 |
| 3.5 (2.2–4.4) | 3.6 (2.1–4.8) | ||
| Total bilirubin level (mg/dL) | 1.0 ± 0.5 | 0.9 ± 0.5 | 0.2451 |
| 0.9 (0.3–2.7) | 0.9 (0.2–3.4) | ||
| ALBI score | −2.08 ± 0.48 | −2.28 ± 0.47 | 0.0006 |
| −2.11 (−2.99–−0.83) | −2.31 (−3.28–−1.02) | ||
| Prothrombin time (%) | 75.3 ± 11.0 | 85.0 ± 16.4 | <0.0001 |
| 74.5 (44.6–105.5) | 84.4 (23.0–130.0) | ||
| AFP (ng/mL) | 4399 ± 24,315 | 7275 ± 49,351 | 0.6009 |
| 108 (2–222,500) | 93 (1–720,500) | ||
| DCP (mAU/mL) | 8914 ± 38,872 | 9824 ± 31,329 | 0.8276 |
| 290 (6–344,000) | 548 (8–335,810) |
| (A) | ||||
| Variable | Univariate Analysis | Multivariate Analysis | ||
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| Age (≥75.3 years) | 0.799 (0.492–1.297) | 0.3633 | 0.588 (0.331–1.043) | 0.0669 |
| Sex (Male) | 0.926 (0.551–1.557) | 0.7727 | 1.023 (0.576–1.814) | 0.9388 |
| Etiology (HCV) | 1.116 (0.596–2.090) | 0.7279 | 1.407 (0.709–2.795) | 0.3147 |
| Child-Pugh class (B) | 2.752 (1.657–4.571) | 0.0002 | 2.848 (1.318–6.152) | 0.0059 |
| Macrovascular invasion (Yes) | 4.305 (2.196–8.437) | 0.0002 | 1.747 (0.485–6.297) | 0.3810 |
| BCLC stage (C) | 4.027 (2.152–7.536) | <0.0001 | 2.680 (0.847–8.478) | 0.1240 |
| ALBI score (≥−2.11) | 1.683 (1.037–2.730) | 0.0349 | 0.781 (0.380–1.605) | 0.4960 |
| AFP (≥108 ng/mL) | 1.646 (1.008–2.688) | 0.0472 | 1.776 (0.973–3.243) | 0.0598 |
| DCP (≥290 mAU/mL) | 1.593 (0.971–2.615) | 0.0680 | 1.682 (0.978–2.894) | 0.0619 |
| (B) | ||||
| Variable | Univariate Analysis | Multivariate Analysis | ||
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| Age (≥72.8 years) | 1.141 (0.868–1.501) | 0.3438 | 1.269 (0.938–1.718) | 0.1224 |
| Sex (Male) | 0.714 (0.506–1.008) | 0.0639 | 0.884 (0.599–1.305) | 0.5390 |
| Etiology (HCV) | 1.169 (0.878–1.557) | 0.2809 | 0.974 (0.711–1.335) | 0.8715 |
| Child-Pugh class (B) | 2.541 (1.805–3.578) | <0.0001 | 1.794 (1.195–2.692) | 0.0058 |
| Macrovascular invasion (Yes) | 1.388 (1.022–1.886) | 0.0401 | 1.085 (0.772–1.526) | 0.6397 |
| BCLC stage (C) | 1.388 (1.022–1.886) | 0.0401 | 1.085 (0.772–1.526) | 0.6397 |
| ALBI score (≥−2.31) | 2.077 (1.567–2.753) | <0.0001 | 1.655 (1.179–2.323) | 0.0039 |
| AFP (≥93 ng/mL) | 2.289 (1.725–3.036) | <0.0001 | 2.091 (1.512–2.893) | < 0.0001 |
| DCP (≥548 mAU/mL) | 1.912 (1.446–2.529) | <0.0001 | 1.260 (0.920–1.726) | 0.1483 |
| Variable | HAIC (n = 83) | Sorafenib (n = 83) | p-Value |
|---|---|---|---|
| Age (years) | 73.7± 9.6 | 73.2 ± 10.0 | 0.7394 |
| 74.8 (47.8–88.6) | 74.3 (35.7–91.6) | ||
| Sex (male/female) | 56 (67%)/27 (33%) | 60 (72%)/23 (28%) | 0.4986 |
| Etiology (HBV/HCV/HBV + HCV/both negative) | 6 (7%)/67 (81%)/0 (0%)/10 (12%) | 7 (9%)/65 (78%)/0 (0%)/11 (13%) | 0.9225 |
| Child-Pugh class (A/B) | 53 (64%)/30 (36%) | 59 (71%)/24 (29%) | 0.3202 |
| Macrovascular invasion (yes/no) | 12 (14%)/71 (86%) | 9 (11%)/74 (89%) | 0.4836 |
| BCLC stage (B/C) | 71 (86%)/12 (14%) | 74 (89%)/9 (11%) | 0.4836 |
| Albumin level (g/dL) | 3.4 ± 0.5 | 3.5 ± 0.5 | 0.4229 |
| 3.5 (2.2–4.4) | 3.5 (2.6–4.6) | ||
| Total bilirubin (mg/dL) | 1.0 ± 0.5 | 1.0 ± 0.4 | 0.7646 |
| 0.9 (0.3–2.7) | 1.0 (0.3–2.9) | ||
| ALBI score | −2.09 ± 0.48 | −2.14 ± 0.44 | 0.4712 |
| −2.11 (−2.99–−0.83) | −2.16 (−3.23–−1.26) | ||
| Prothrombin time (%) | 75.0 ± 10.4 | 76.1 ± 12.0 | 0.5602 |
| 74.5 (44.6–100.7) | 78.0 (39.0–97.0) | ||
| AFP (ng/mL) | 4462 ± 25,019 | 4396 ± 19,661 | 0.9849 |
| 75 (2–222,500) | 100 (3–177,630) | ||
| DCP (mAU/mL) | 8562 ± 39,732 | 7898 ± 20,603 | 0.8928 |
| 316 (6–344,000) | 582 (11–112,000) |
| Variable | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| Age (≥74.4 years) | 0.887 (0.629–1.251) | 0.4942 | 0.855 (0.589–1.242) | 0.4103 |
| Sex (male) | 0.785 (0.541–1.139) | 0.2096 | 0.922 (0.612–1.388) | 0.6976 |
| Etiology (HCV) | 1.234 (0.811–1.952) | 0.3354 | 1.397 (0.871–2.328) | 0.1702 |
| Child-Pugh class (B) | 2.615 (1.799–3.761) | <0.0001 | 1.783 (1.136–2.807) | 0.0119 |
| Macrovascular invasion (Yes) | 2.813 (1.699–4.655) | 0.0003 | 2.035 (1.136–3.557) | 0.0180 |
| BCLC stage (C) | 2.813 (1.699–4.655) | 0.0003 | 2.035 (1.164–3.557) | 0.0180 |
| ALBI score (≥−2.14) | 2.121 (1.500–3.009) | <0.0001 | 1.501 (0.968–2.308) | 0.0692 |
| AFP (≥97 ng/mL) | 1.954 (1.378–2.777) | 0.0002 | 1.587 (1.089–2.316) | 0.0164 |
| DCP (≥491 mAU/mL) | 2.061 (1.448–2.939) | <0.0001 | 1.597 (1.091–2.339) | 0.0162 |
| Treatment (HAIC) | 0.653 (0.460–0.925) | 0.0164 | 0.604 (0.413–0.883) | 0.0090 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zaizen, Y.; Nakano, M.; Fukumori, K.; Yano, Y.; Takaki, K.; Niizeki, T.; Kuwaki, K.; Fukahori, M.; Sakaue, T.; Yoshimura, S.; et al. Hepatic Arterial Infusion Chemotherapy with Cisplatin versus Sorafenib for Intrahepatic Advanced Hepatocellular Carcinoma: A Propensity Score-Matched Analysis. Cancers 2021, 13, 5282. https://doi.org/10.3390/cancers13215282
Zaizen Y, Nakano M, Fukumori K, Yano Y, Takaki K, Niizeki T, Kuwaki K, Fukahori M, Sakaue T, Yoshimura S, et al. Hepatic Arterial Infusion Chemotherapy with Cisplatin versus Sorafenib for Intrahepatic Advanced Hepatocellular Carcinoma: A Propensity Score-Matched Analysis. Cancers. 2021; 13(21):5282. https://doi.org/10.3390/cancers13215282
Chicago/Turabian StyleZaizen, Yuki, Masahito Nakano, Kazuta Fukumori, Yoichi Yano, Kota Takaki, Takashi Niizeki, Kotaro Kuwaki, Masaru Fukahori, Takahiko Sakaue, Sohei Yoshimura, and et al. 2021. "Hepatic Arterial Infusion Chemotherapy with Cisplatin versus Sorafenib for Intrahepatic Advanced Hepatocellular Carcinoma: A Propensity Score-Matched Analysis" Cancers 13, no. 21: 5282. https://doi.org/10.3390/cancers13215282
APA StyleZaizen, Y., Nakano, M., Fukumori, K., Yano, Y., Takaki, K., Niizeki, T., Kuwaki, K., Fukahori, M., Sakaue, T., Yoshimura, S., Nakazaki, M., Kuromatsu, R., Okamura, S., Iwamoto, H., Shimose, S., Shirono, T., Noda, Y., Kamachi, N., Koga, H., & Torimura, T. (2021). Hepatic Arterial Infusion Chemotherapy with Cisplatin versus Sorafenib for Intrahepatic Advanced Hepatocellular Carcinoma: A Propensity Score-Matched Analysis. Cancers, 13(21), 5282. https://doi.org/10.3390/cancers13215282