
Circulating Tissue Polypeptide-Specific Antigen in Pre-Diagnostic Pancreatic Cancer Samples

 , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethics Statement
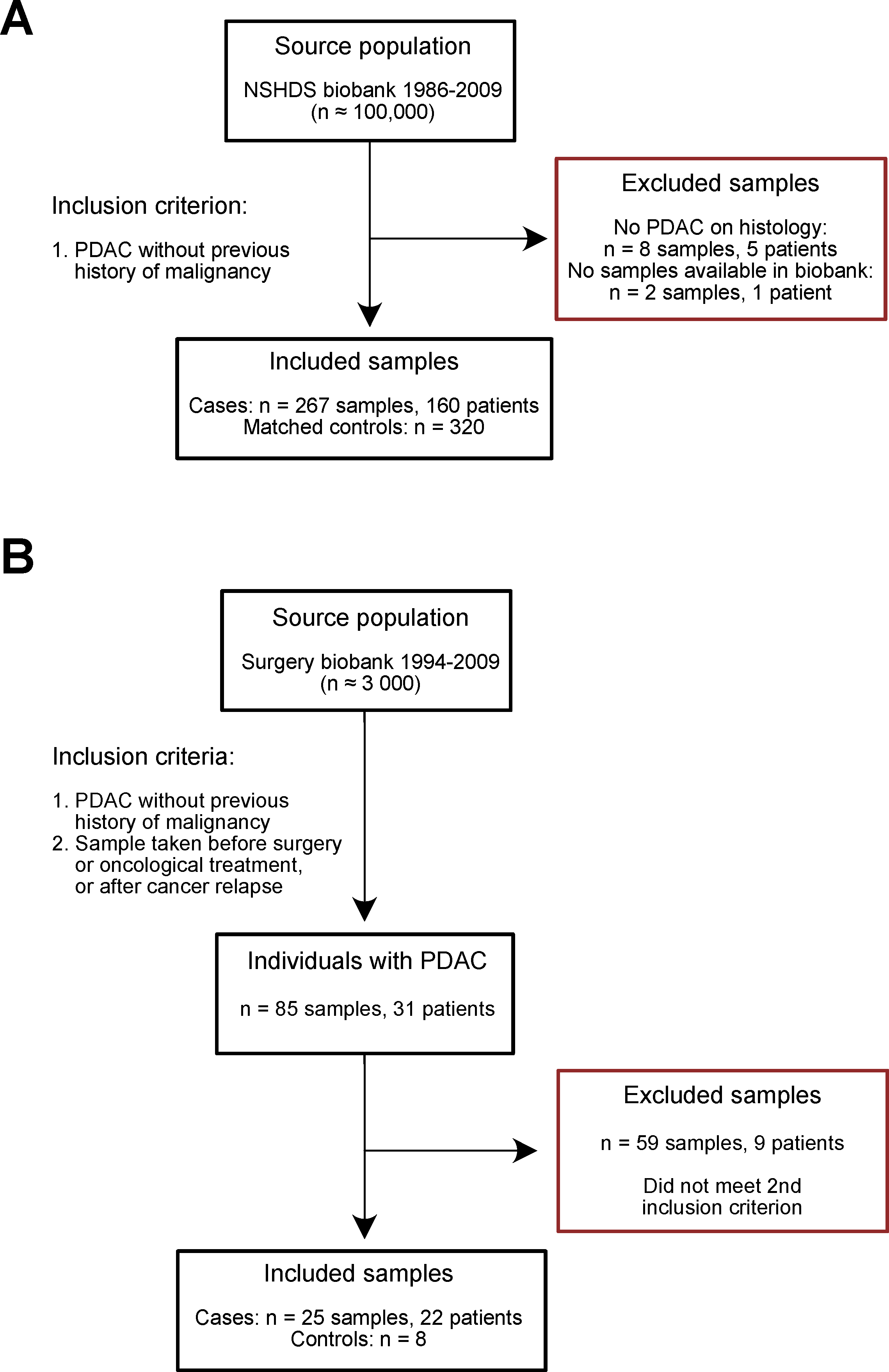
2.2. Study Design
2.3. Pre-Diagnostic Cohort
2.4. Diagnostic Cohort
2.5. ELISA
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wild, C.P.; Weiderpass, E.; Stewart, B.W. (Eds.) World Cancer Report: Cancer Research for Cancer Prevention; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2021. CA Cancer J. Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef]
- Yachida, S.; Jones, S.; Bozic, I.; Antal, T.; Leary, R.; Fu, B.; Kamiyama, M.; Hruban, R.H.; Eshleman, J.R.; Nowak, M.A.; et al. Distant metastasis occurs late during the genetic evolution of pancreatic cancer. Nature 2010, 467, 1114–1117. [Google Scholar] [CrossRef] [Green Version]
- Yu, J.; Blackford, A.L.; Dal Molin, M.; Wolfgang, C.L.; Goggins, M. Time to progression of pancreatic ductal adenocarcinoma from low-to-high tumour stages. Gut 2015, 64, 1783–1789. [Google Scholar] [CrossRef] [Green Version]
- Notta, F.; Chan-Seng-Yue, M.; Lemire, M.; Li, Y.; Wilson, G.W.; Connor, A.A.; Denroche, R.E.; Liang, S.B.; Brown, A.M.; Kim, J.C.; et al. A renewed model of pancreatic cancer evolution based on genomic rearrangement patterns. Nature 2016, 538, 378–382. [Google Scholar] [CrossRef] [PubMed]
- Cortes-Ciriano, I.; Lee, J.J.; Xi, R.; Jain, D.; Jung, Y.L.; Yang, L.; Gordenin, D.; Klimczak, L.J.; Zhang, C.Z.; Pellman, D.S.; et al. Comprehensive analysis of chromothripsis in 2,658 human cancers using whole-genome sequencing. Nat. Genet. 2020, 52, 331–341. [Google Scholar] [CrossRef] [Green Version]
- Koprowski, H.; Steplewski, Z.; Mitchell, K.; Herlyn, M.; Herlyn, D.; Fuhrer, P. Colorectal carcinoma antigens detected by hybridoma antibodies. Somat. Cell Genet. 1979, 5, 957–971. [Google Scholar] [CrossRef]
- Koprowski, H.; Herlyn, M.; Steplewski, Z.; Sears, H.F. Specific antigen in serum of patients with colon carcinoma. Science 1981, 212, 53–55. [Google Scholar] [CrossRef] [PubMed]
- DelVillano, B.C.; Zurawski, V.R., Jr. The carbohydrate antigenic determinant 19-9 (CA 19-9): A monoclonal antibody defined tumor marker. Lab. Res. Methods Biol. Med. 1983, 8, 269–282. [Google Scholar] [PubMed]
- Khomiak, A.; Brunner, M.; Kordes, M.; Lindblad, S.; Miksch, R.C.; Ohlund, D.; Regel, I. Recent Discoveries of Diagnostic, Prognostic and Predictive Biomarkers for Pancreatic Cancer. Cancers 2020, 12, 3234. [Google Scholar] [CrossRef]
- Mayers, J.R.; Wu, C.; Clish, C.B.; Kraft, P.; Torrence, M.E.; Fiske, B.P.; Yuan, C.; Bao, Y.; Townsend, M.K.; Tworoger, S.S.; et al. Elevation of circulating branched-chain amino acids is an early event in human pancreatic adenocarcinoma development. Nat. Med. 2014, 20, 1193–1198. [Google Scholar] [CrossRef]
- Katagiri, R.; Goto, A.; Nakagawa, T.; Nishiumi, S.; Kobayashi, T.; Hidaka, A.; Budhathoki, S.; Yamaji, T.; Sawada, N.; Shimazu, T.; et al. Increased Levels of Branched-Chain Amino Acid Associated With Increased Risk of Pancreatic Cancer in a Prospective Case-Control Study of a Large Cohort. Gastroenterology 2018, 155, 1474–1482.e1471. [Google Scholar] [CrossRef] [PubMed]
- Fest, J.; Vijfhuizen, L.S.; Goeman, J.J.; Veth, O.; Joensuu, A.; Perola, M.; Mannisto, S.; Ness-Jensen, E.; Hveem, K.; Haller, T.; et al. Search for Early Pancreatic Cancer Blood Biomarkers in Five European Prospective Population Biobanks Using Metabolomics. Endocrinology 2019, 160, 1731–1742. [Google Scholar] [CrossRef] [Green Version]
- Stolzenberg-Solomon, R.; Derkach, A.; Moore, S.; Weinstein, S.J.; Albanes, D.; Sampson, J. Associations between metabolites and pancreatic cancer risk in a large prospective epidemiological study. Gut 2020, 69, 2008–2015. [Google Scholar] [CrossRef] [PubMed]
- Duell, E.J.; Lujan-Barroso, L.; Sala, N.; Deitz McElyea, S.; Overvad, K.; Tjonneland, A.; Olsen, A.; Weiderpass, E.; Busund, L.T.; Moi, L.; et al. Plasma microRNAs as biomarkers of pancreatic cancer risk in a prospective cohort study. Int. J. Cancer 2017, 141, 905–915. [Google Scholar] [CrossRef] [PubMed]
- Franklin, O.; Jonsson, P.; Billing, O.; Lundberg, E.; Ohlund, D.; Nystrom, H.; Lundin, C.; Antti, H.; Sund, M. Plasma Micro-RNA Alterations Appear Late in Pancreatic Cancer. Ann. Surg. 2018, 267, 775–781. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kucera, R.; Topolcan, O.; Fiala, O.; Kinkorova, J.; Treska, V.; Zednikova, I.; Slouka, D.; Simanek, V.; Safanda, M.; Babuska, V. The Role of TPS and TPA in the Diagnostics of Distant Metastases. Anticancer Res. 2016, 36, 773–777. [Google Scholar]
- Xie, S.; Ding, X.; Mo, W.; Chen, J. Serum tissue polypeptide-specific antigen is an independent predictor in breast cancer. Acta Histochem. 2014, 116, 372–376. [Google Scholar] [CrossRef]
- Eskelinen, M.; Kataja, V.; Hamalainen, E.; Kosma, V.M.; Penttila, I.; Alhava, E. Serum tumour markers CEA, AFP, CA 15-3, TPS and Neu in diagnosis of breast cancer. Anticancer Res. 1997, 17, 1231–1234. [Google Scholar]
- D’Alessandro, R.; Roselli, M.; Ferroni, P.; Mariotti, S.; Spila, A.; Aloe, S.; Carone, M.D.; Abbolito, M.R.; Carlini, S.; Perri, P.; et al. Serum tissue polypeptide specific antigen (TPS): A complementary tumor marker to CA 15-3 in the management of breast cancer. Breast Cancer Res. Treat. 2001, 68, 9–19. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.; Li, C.; Zhang, F.; Ma, X.; Gai, X. Clinical Value of Combined Determination of Serum B7-H4 with Carcinoembryonic Antigen, Osteopontin, or Tissue Polypeptide-Specific Antigen for the Diagnosis of Colorectal Cancer. Dis. Markers 2018, 2018, 4310790. [Google Scholar] [CrossRef]
- Carpelan-Holmstrom, M.; Haglund, C.; Lundin, J.; Alfthan, H.; Stenman, U.H.; Roberts, P.J. Independent prognostic value of preoperative serum markers CA 242, specific tissue polypeptide antigen and human chorionic gonadotrophin beta, but not of carcinoembryonic antigen or tissue polypeptide antigen in colorectal cancer. Br. J. Cancer 1996, 74, 925–929. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pasanen, P.A.; Eskelinen, M.; Partanen, K.; Pikkarainen, P.; Penttila, I.; Alhava, E. Diagnostic value of tissue polypeptide specific antigen in patients with pancreatic carcinoma. Tumour Biol. 1994, 15, 52–60. [Google Scholar] [CrossRef] [PubMed]
- Slesak, B.; Harlozinska-Szmyrka, A.; Knast, W.; Sedlaczek, P.; Einarsson, R.; van Dalen, A. TPS and CA 19-9 measurements in the follow-up of patients with pancreatic cancer and chronic pancreatitis. Int. J. Biol. Markers 2004, 19, 115–119. [Google Scholar] [CrossRef]
- Franklin, O.; Ohlund, D.; Lundin, C.; Oman, M.; Naredi, P.; Wang, W.; Sund, M. Combining conventional and stroma-derived tumour markers in pancreatic ductal adenocarcinoma. Cancer Biomark. 2015, 15, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ozkan, H.; Demirbas, S.; Ibis, M.; Akbal, E.; Koklu, S. Diagnostic validity of serum macrophage inhibitor cytokine and tissue polypeptide-specific antigen in pancreatobiliary diseases. Pancreatology 2011, 11, 295–300. [Google Scholar] [CrossRef]
- Banfi, G.; Zerbi, A.; Pastori, S.; Parolini, D.; Dicarlo, V.; Bonini, P. Behavior of Tumor-Markers Ca19.9, Ca195, Cam43, Ca242, and Tps in the Diagnosis and Follow-up of Pancreatic-Cancer. Clin. Chem. 1993, 39, 420–423. [Google Scholar] [CrossRef]
- Pasanen, P.A.; Eskelinen, M.; Partanen, K.; Pikkarainen, P.; Penttila, I.; Alhava, E. A Prospective-Study of Serum Tumor-Markers Carcinoembryonic Antigen, Carbohydrate Antigen-50 and Antigen-242, Tissue Polypeptide Antigen and Tissue Polypeptide Specific Antigen in the Diagnosis of Pancreatic-Cancer with Special Reference to Multivariate Diagnostic Score. Brit. J. Cancer 1994, 69, 562–565. [Google Scholar] [CrossRef] [Green Version]
- Talar-Wojnarowska, R.; Gasiorowska, A.; Olakowski, M.; Lekstan, A.; Lampe, P.; Malecka-Panas, E. Clinical value of serum neopterin, tissue polypeptide-specific antigen and CA19-9 levels in differential diagnosis between pancreatic cancer and chronic pancreatitis. Pancreatology 2010, 10, 689–694. [Google Scholar] [CrossRef]
- Plebani, M.; Basso, D.; Del Favero, G.; Ferrara, C.; Meggiato, T.; Fogar, P.; Mangano, F.; Ricciardi, G.; Burlina, A. Clinical utility of TPS, TPA and CA 19-9 measurement in pancreatic cancer. Oncology 1993, 50, 436–440. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P.; Initiative, S. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020. [Google Scholar]
- Therneau, T. A Package for Survival Analysis in R; CRAN: Vienna, Austria, 2020. [Google Scholar]
- Therneau, T.; Grambsch, P. Modeling Survival Data: Extending the Cox Model; Springer: New York, NY, USA, 2000. [Google Scholar]
- Chongsuvivatwong, V. epiDisplay: Epidemiological Data Display Package; CRAN: Vienna, Austria, 2018. [Google Scholar]
- Wickham, H. ggplot2: Elegant Graphics for Data Analysis; Springer: New York, NY, USA, 2016. [Google Scholar]
- Garnier, S. Viridis: Default Color Maps from ‘Matplotlib’; CRAN: Vienna, Austria, 2018. [Google Scholar]
- Garnier, S.; Ross, N.; Rudis, R.; Camargo, P.A.; Sciaini, M.; Scherer, C. Viridis—Colorblind-Friendly Color Maps for R. R Package Version 0.6.2. 2021. Available online: https://sjmgarnier.github.io/viridis/ (accessed on 20 October 2021). [CrossRef]
- Zhang, J.; Wei, Q.; Dong, D.; Ren, L. The role of TPS, CA125, CA15-3 and CEA in prediction of distant metastasis of breast cancer. Clin. Chim. Acta 2021, 523, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Ansari, D.; Bauden, M.; Bergstrom, S.; Rylance, R.; Marko-Varga, G.; Andersson, R. Relationship between tumour size and outcome in pancreatic ductal adenocarcinoma. Br. J. Surg. 2017, 104, 600–607. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Cases (n = 160) | Controls (n = 320) |
|---|---|---|
| Mean age at blood sample collection (years) | 55 | 55 |
| Sex | ||
| Men, n | 57 | 114 |
| Women, n | 103 | 206 |
| TNM stage at diagnosis (7th ed of AJCC staging) | ||
| Stage I | 12 | NA |
| Stage II | 11 | NA |
| Stage III | 37 | NA |
| Stage IV | 100 | NA |
| Grade at diagnosis | ||
| Low | 33 | NA |
| Intermediate | 44 | NA |
| High | 4 | NA |
| Information missing | 79 | NA |
| Surgical treatment | ||
| None | 111 | NA |
| Curative | 23 | NA |
| Palliative | 25 | NA |
| Information missing | 1 | NA |
| Variable | Cases (n = 22) | Controls (n = 52) |
|---|---|---|
| Mean age at blood sample collection (years) * | 61 | 52 |
| Sex # | ||
| Men, n | 9 | 21 |
| Women, n | 13 | 31 |
| TNM stage (7th ed of AJCC staging) | ||
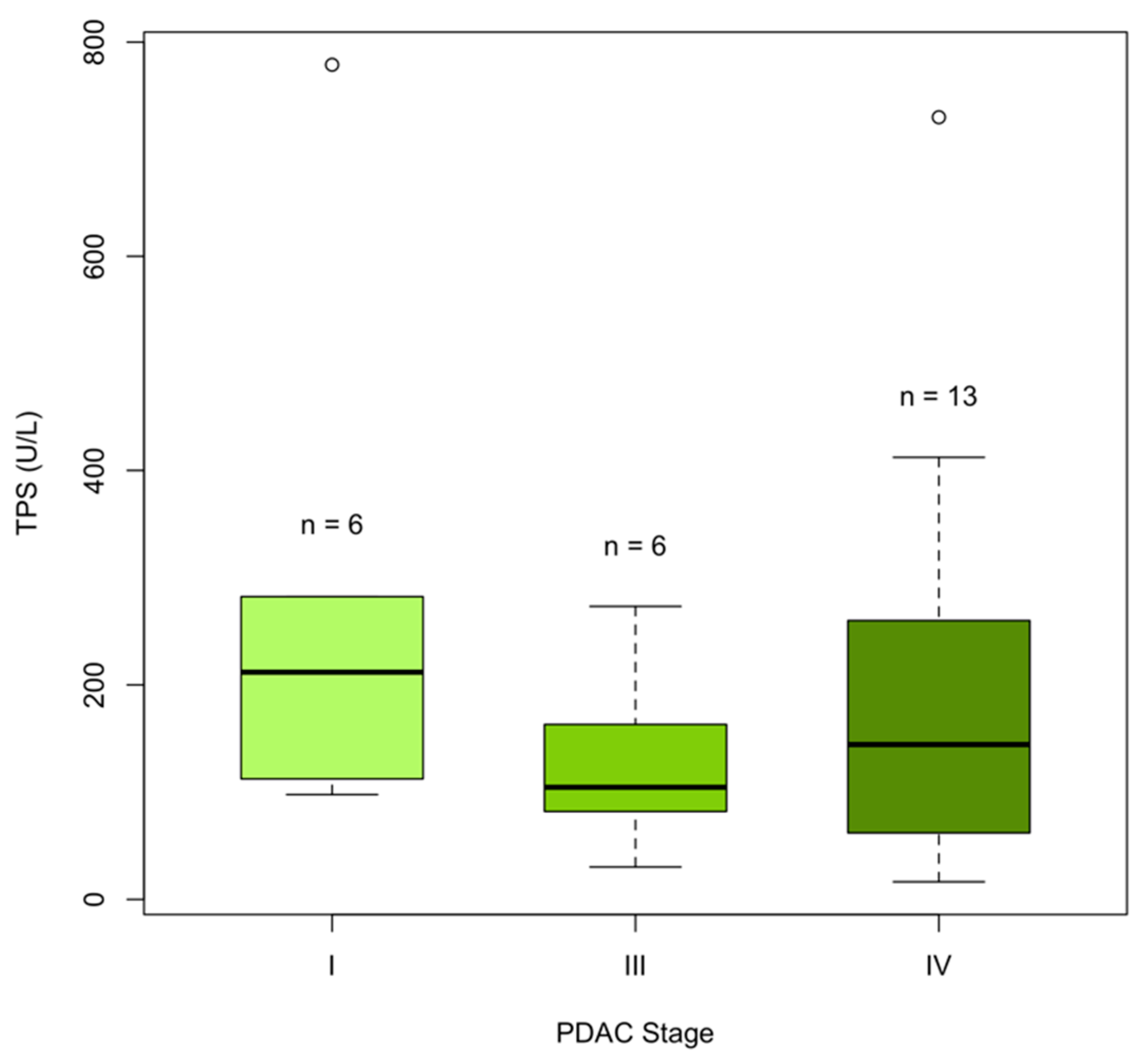
| Stage I | 6 | NA |
| Stage II | 0 | NA |
| Stage III | 6 | NA |
| Stage IV | 10 | NA |
| Surgical treatment | ||
| None | 11 | NA |
| Curative | 7 | NA |
| Palliative | 4 | NA |
| Stratum (Number of Samples) | Crude Estimate a | Crude OR (95% CI) | Adjusted Estimate a | Adjusted OR (95% CI) |
|---|---|---|---|---|
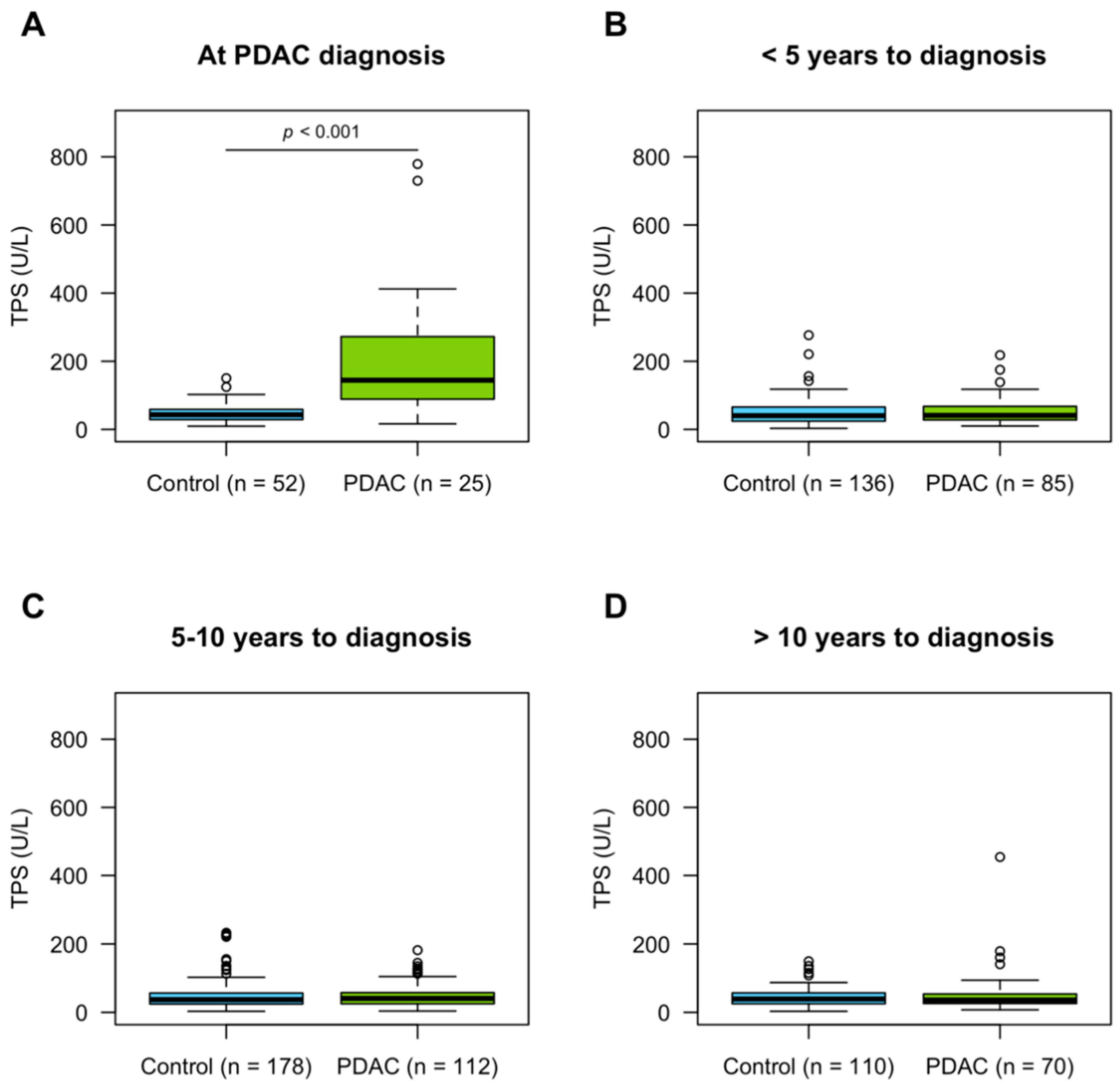
| At diagnosis (25 PDAC, 52 controls) | 0.033 (p < 0.001) | 1.03 (1.02–1.05) | 0.030 (p < 0.001) | 1.03 (1.01–1.05) |
| <5 years to diagnosis (85 PDAC, 136 controls) | 0.002 | 1.00 (0.99–1.01) | 0.006 | 1.01 (1.00–1.02) |
| 5–10 years to diagnosis (112 PDAC, 178 controls) | 0.0003 | 1.00 (0.99–1.01) | −0.004 | 1.00 (0.99–1.00) |
| >10 years to diagnosis (70 PDAC, 110 controls) | 0.004 | 1.00 (1.00–1.01) | 0.005 | 1.00 (1.00–1.01) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Borgmästars, E.; Lundberg, E.; Öhlund, D.; Nyström, H.; Franklin, O.; Lundin, C.; Jonsson, P.; Sund, M. Circulating Tissue Polypeptide-Specific Antigen in Pre-Diagnostic Pancreatic Cancer Samples. Cancers 2021, 13, 5321. https://doi.org/10.3390/cancers13215321
Borgmästars E, Lundberg E, Öhlund D, Nyström H, Franklin O, Lundin C, Jonsson P, Sund M. Circulating Tissue Polypeptide-Specific Antigen in Pre-Diagnostic Pancreatic Cancer Samples. Cancers. 2021; 13(21):5321. https://doi.org/10.3390/cancers13215321
Chicago/Turabian StyleBorgmästars, Emmy, Erik Lundberg, Daniel Öhlund, Hanna Nyström, Oskar Franklin, Christina Lundin, Pär Jonsson, and Malin Sund. 2021. "Circulating Tissue Polypeptide-Specific Antigen in Pre-Diagnostic Pancreatic Cancer Samples" Cancers 13, no. 21: 5321. https://doi.org/10.3390/cancers13215321
APA StyleBorgmästars, E., Lundberg, E., Öhlund, D., Nyström, H., Franklin, O., Lundin, C., Jonsson, P., & Sund, M. (2021). Circulating Tissue Polypeptide-Specific Antigen in Pre-Diagnostic Pancreatic Cancer Samples. Cancers, 13(21), 5321. https://doi.org/10.3390/cancers13215321