
The Impact of Lifestyle Interventions in High-Risk Early Breast Cancer Patients: A Modeling Approach from a Single Institution Experience

 , , , , ,
, , , , ,  ,
,  add
Show full author list
add
Show full author list
Abstract
:Simple Summary
Abstract
1. Introduction
“If we were able to provide everyone with the right amount of nutrition and exercise, neither in excess nor in fault, we would have found the way to health”. Hippocrates, 460–377ac.
2. Materials and Methods
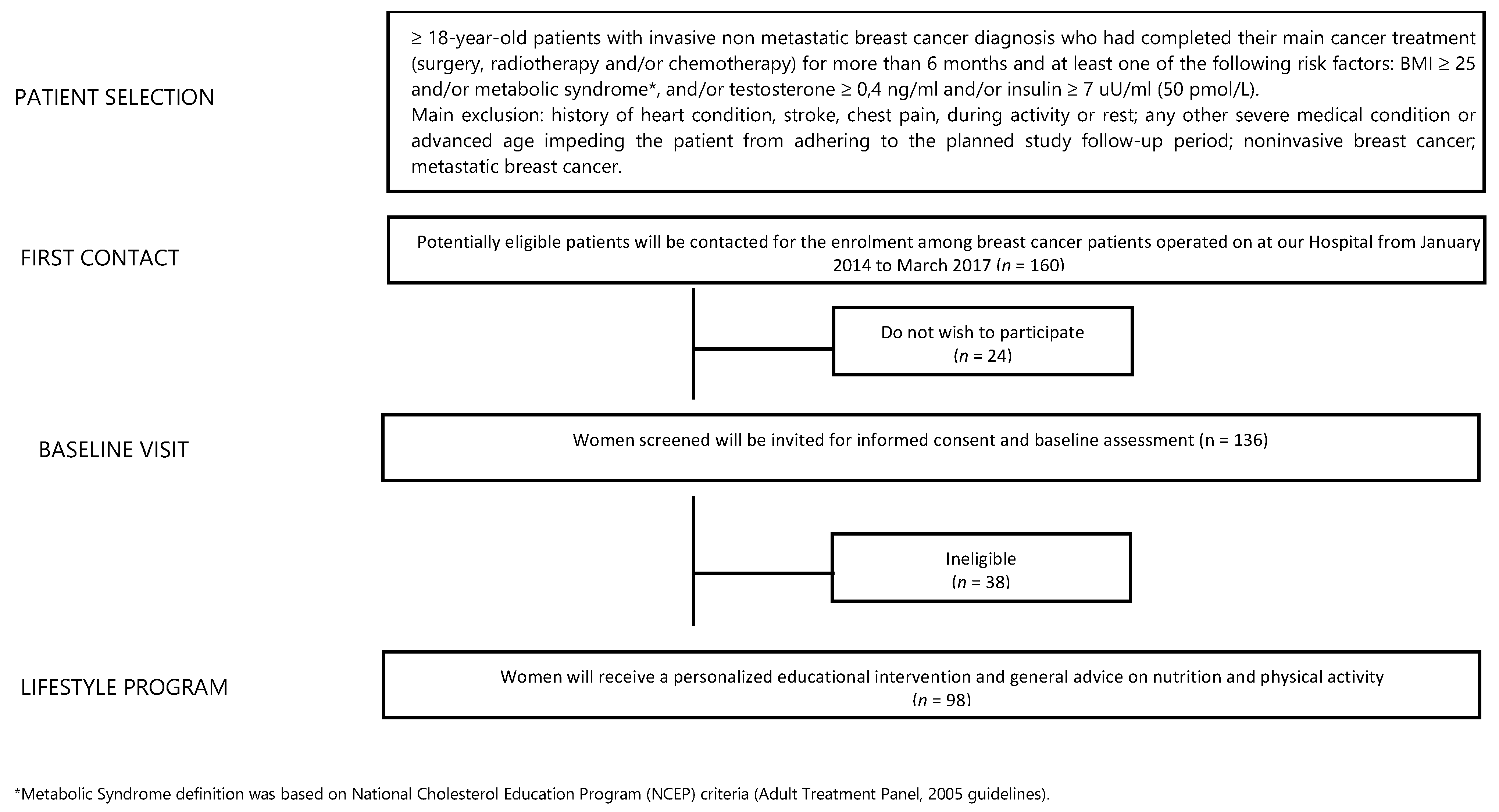
2.1. Study Population
2.2. Study Outcomes
2.3. Lifestyle Intervention
2.4. Assessments
2.5. Statistical Considerations
3. Results
3.1. Baseline Patients Characteristics
3.2. Primary Outcome: Body Weight Variation at T1, T2 and T3
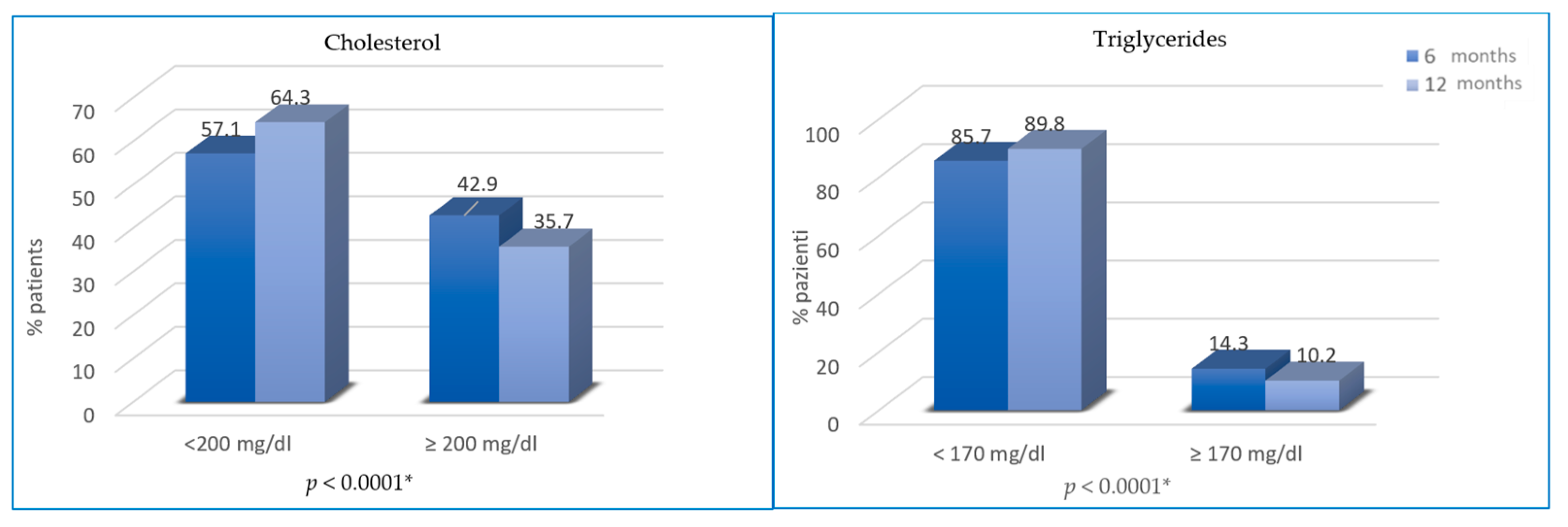
3.3. Secondary Outcomes at T2 and T3
3.4. Analysis of Variance (ANOVA)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Global Cancer Statistics 2020; Global Cancer Observatory (iarc.fr). Available online: https://gco.iarc.fr/ (accessed on 1 August 2021).
- Rebbeck, T.R.; Mitra, N.; Wan, F.; Sinilnikova, O.M.; Healey, S.; McGuffog, L.; Mazoyer, S.; Chenevix-Trench, G.; Easton, D.F.; Antoniou, A.C.; et al. Association of Type and Location ofBRCA1andBRCA2Mutations With Risk of Breast and Ovarian Cancer. JAMA 2015, 313, 1347–1361. [Google Scholar] [CrossRef] [Green Version]
- Kolak, A.; Kamińska, M.; Sygit, K.; Budny, A.; Surdyka, D.; Kukiełka-Budny, B.; Burdan, F. Primary and secondary prevention of breast cancer. Ann. Agric. Environ. Med. 2017, 24, 549–553. [Google Scholar] [CrossRef]
- Ghoncheh, M.; Pournamdar, Z.; Salehiniya, H. Incidence and Mortality and Epidemiology of Breast Cancer in the World. Asian Pac. J. Cancer Prev. 2016, 17, 43–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cancer-WHO | World Health Organization. Available online: www.who.int/en/news-room/fact-sheets/detail/cancer (accessed on 1 August 2021).
- Buja, A.; Pierbon, M.; Lago, L.; Grotto, G.; Baldo, V. Breast Cancer Primary Prevention and Diet: An Umbrella Review. Int. J. Environ. Res. Public Health 2020, 17, 4731. [Google Scholar] [CrossRef] [PubMed]
- Turati, F.; Carioli, G.; Bravi, F.; Ferraroni, M.; Serraino, D.; Montella, M.; Giacosa, A.; Toffolutti, F.; Negri, E.; Levi, F.; et al. Mediterranean Diet and Breast Cancer Risk. Nutrients 2018, 10, 326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwingshackl, L.; Schwedhelm, C.; Galbete, C.; Hoffmann, G. Adherence to Mediterranean Diet and Risk of Cancer: An Updated Systematic Review and Meta-Analysis. Nutrients 2017, 9, 1063. [Google Scholar] [CrossRef]
- Most, J.; Tosti, V.; Redman, L.M.; Fontana, L. Calorie restriction in humans: An update. Ageing Res. Rev. 2017, 39, 36–45. [Google Scholar] [CrossRef] [PubMed]
- Jiralerspong, S.; Goodwin, P. Obesity and Breast Cancer Prognosis: Evidence, Challenges, and Opportunities. J. Clin. Oncol. 2016, 34, 4203–4216. [Google Scholar] [CrossRef]
- Ewertz, M.; Jensen, M.-B.; Gunnarsdóttir, K.; Højris, I.; Jakobsen, E.H.; Nielsen, D.; Stenbygaard, L.E.; Tange, U.B.; Cold, S. Effect of Obesity on Prognosis After Early-Stage Breast Cancer. J. Clin. Oncol. 2011, 29, 25–31. [Google Scholar] [CrossRef]
- O’Flanagan, C.H.; Smith, L.A.; McDonell, S.; Hursting, S.D. When less may be more: Calorie restriction and response to cancer therapy. BMC Med. 2017, 15, 106. [Google Scholar] [CrossRef]
- Denduluri, S.K.; Idowu, O.; Wang, Z.; Liao, Z.; Yan, Z.; Mohammed, M.K.; Ye, J.; Wei, Q.; Wang, J.; Zhao, L.; et al. Insulin-like growth factor (IGF) signaling in tumorigenesis and the development of cancer drug resistance. Genes Dis. 2015, 2, 13–25. [Google Scholar] [CrossRef] [Green Version]
- Goss, P.E.; Ingle, J.N.; Pritchard, K.I.; Robert, N.J.; Muss, H.; Gralow, J.; Gelmon, K.; Whelan, T.; Strasser-Weippl, K.; Rubin, S.; et al. Extending Aromatase-Inhibitor Adjuvant Therapy to 10 Years. N. Engl. J. Med. 2016, 375, 209–219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pfeiler, G.; Königsberg, R.; Fesl, C.; Mlineritsch, B.; Stoeger, H.; Singer, C.F.; Pöstlberger, S.; Steger, G.G.; Seifert, M.; Dubsky, P.; et al. Impact of Body Mass Index on the Efficacy of Endocrine Therapy in Premenopausal Patients with Breast Cancer: An Analysis of the Prospective ABCSG-12 Trial. J. Clin. Oncol. 2011, 29, 2653–2659. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andrikopoulou, A.; Fiste, O.; Liontos, M.; Dimopoulos, M.-A.; Zagouri, F. Aromatase and CDK4/6 Inhibitor-Induced Musculoskeletal Symptoms: A Systematic Review. Cancers 2021, 13, 465. [Google Scholar] [CrossRef] [PubMed]
- Beckwée, D.; Leysen, L.; Meuwis, K.; Adriaenssens, N. Prevalence of aromatase inhibitor-induced arthralgia in breast cancer: A systematic review and meta-analysis. Support. Care Cancer 2017, 25, 1673–1686. [Google Scholar] [CrossRef] [PubMed]
- Crew, K.D.; Greenlee, H.; Capodice, J.; Raptis, G.; Brafman, L.; Fuentes, D.; Sierra, A.; Hershman, D.L. Prevalence of Joint Symptoms in Postmenopausal Women Taking Aromatase Inhibitors for Early-Stage Breast Cancer. J. Clin. Oncol. 2007, 25, 3877–3883. [Google Scholar] [CrossRef]
- Sestak, I.; Cuzick, J.; Sapunar, F.; Eastell, R.; Forbes, J.F.; Bianco, A.R.; Buzdar, A.U. Risk factors for joint symptoms in patients enrolled in the ATAC trial: A retrospective, exploratory analysis. Lancet Oncol. 2008, 9, 866–872. [Google Scholar] [CrossRef] [Green Version]
- Dieli-Conwright, C.; Orozco, B. Exercise after breast cancer treatment: Current perspectives. Breast Cancer 2015, 7, 353–362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lahart, I.; Metsios, G.S.; Nevill, A.; Carmichael, A.R. Physical activity, risk of death and recurrence in breast cancer survivors: A systematic review and meta-analysis of epidemiological studies. Acta Oncol. 2015, 54, 635–654. [Google Scholar] [CrossRef]
- American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription, 10th ed.; Wolters Kluwer Health: Philadelphia, PA, USA, 2018. [Google Scholar]
- Campbell, K.L.; Winters-Stone, K.M.; Wiskemann, J.; May, A.M.; Schwartz, A.L.; Courneya, K.S.; Zucker, D.S.; Matthews, C.E.; Ligibel, J.A.; Gerber, L.H.; et al. Exercise Guidelines for Cancer Survivors: Consensus Statement from International Multidisciplinary Roundtable. Med. Sci. Sports Exerc. 2019, 51, 2375–2390. [Google Scholar] [CrossRef] [Green Version]
- Irwin, M.; Cartmel, B.; Gross, C.; Li, F.; Yao, X.; Fiellin, M.; Ercolano, E.; Harrigan, M.; Zhou, Y.; Sanft, T.B.; et al. Effect of exercise on weight, body fat, and serum inflammatory biomarkers in breast cancer survivors with aromatase inhibitor arthralgias: The hormones and physical exercise (HOPE) study. J. Clin. Oncol. 2014, 32, 9536. [Google Scholar] [CrossRef]
- Ruiz, R.B.; Hernández, P.S. Diet and cancer: Risk factors and epidemiological evidence. Maturitas 2014, 77, 202–208. [Google Scholar] [CrossRef] [PubMed]
- Friedenreich, C.M.; Neilson, H.K.; Farris, M.S.; Courneya, K.S. Physical Activity and Cancer Outcomes: A Precision Medicine Approach. Clin. Cancer Res. 2016, 22, 4766–4775. [Google Scholar] [CrossRef] [Green Version]
- Craig, C.L.; Marshall, A.L.; Sjostrom, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International Physical Activity Questionnaire: 12-Country Reliability and Validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [Green Version]
- Lee, P.H.; Macfarlane, D.J.; Lam, T.; Stewart, S.M. Validity of the international physical activity questionnaire short form (IPAQ-SF): A systematic review. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmidt, K.; Vogt, L.; Thiel, C.; Jäger, E.; Banzer, W. Validity of the Six-Minute Walk Test in Cancer Patients. Int. J. Sport Med. 2013, 34, 631–636. [Google Scholar] [CrossRef] [PubMed]
- Picon-Ruiz, M.; Morata-Tarifa, C.; Valle-Goffin, J.J.; Friedman, E.R.; Slingerland, J.M. Obesity and adverse breast cancer risk and outcome: Mechanistic insights and strategies for intervention. CA Cancer J. Clin. 2017, 67, 378–397. [Google Scholar] [CrossRef] [PubMed]
- Wani, B.; Aziz, S.A.; Ganaie, M.A.; Mir, M.H. Metabolic syndrome and breast cancer risk. Indian J. Med. Paediatr. Oncol. 2017, 38, 434–439. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Schoufour, J.; Wang, D.D.; Dhana, K.; Pan, A.; Liu, X.; Song, M.; Liu, G.; Shin, H.J.; Sun, Q.; et al. Healthy lifestyle and life expectancy free of cancer, cardiovascular disease, and type 2 diabetes: Prospective cohort study. BMJ 2020, 368, l6669. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ambrignani, M.G.; Parrini, I.; Grosseto, D.; Lestuzzi, C.; Mistrangelo, M.; Passaretti, B. A nome dell’Area Prevenzione Cardiovascolare ANMCO e della Task Force Cardioncologia ANMCO. Stili di vita, fattori di rischio e prevenzione delle malattie oncologiche: Il ruolo del cardiologo Lifestyle, risk factors and prevention of cancer: Role of the cardiologist. G Ital. Cardiol. 2019, 20, 20–31. [Google Scholar] [CrossRef]
- Rinnerthaler, G.; Gampenrieder, S.P.; Greil, R. SABCS 2017: Lifestyle factors, hormone receptor-positive advanced disease, liquid biopsies, and prognosis. Memo 2018, 11, 208–212. [Google Scholar] [CrossRef] [PubMed]
- Runowicz, C.D.; Leach, C.R.; Henry, N.L.; Henry, K.S.; Mackey, H.T.; Cowens-Alvarado, R.L.; Cannady, R.S.; Pratt-Chapman, M.; Edge, S.B.; Jacobs, L.A.; et al. American Cancer Society/American Society of Clinical Oncology Breast Cancer Survivorship Care Guideline. CA Cancer J. Clin. 2016, 66, 43–73. [Google Scholar] [CrossRef] [PubMed]
- Ormel, H.; Van Der Schoot, G.; Sluiter, W.; Jalving, M.; Gietema, J.; Walenkamp, A. Predictors of adherence to exercise interventions during and after cancer treatment: A systematic review. Psycho-Oncology 2018, 27, 713–724. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, M.A.; Bayes, S.; Galvão, D.A.; Singh, F.; Spry, N.A.; Davis, M.; Chee, R.; Zissiadis, Y.; Hart, N.H.; Taaffe, D.R.; et al. If you build it, will they come? Evaluation of a co-located exercise clinic and cancer treatment centre using the REAIM framework. Eur. J. Cancer Care 2020, 29, e13251. [Google Scholar] [CrossRef] [PubMed]
- Rodulfo, J.I.A. Sedentary lifestyle a disease from xxi century. Clin. Investig. Arterioscler. 2019, 31, 233–240. [Google Scholar] [CrossRef]
- Irwin, M.L.; Smith, A.W.; McTiernan, A.; Ballard-Barbash, R.; Cronin, K.; Gilliland, F.D.; Baumgartner, R.N.; Baumgartner, K.B.; Bernstein, L. Influence of Pre- and Postdiagnosis Physical Activity on Mortality in Breast Cancer Survivors: The Health, Eating, Activity, and Lifestyle Study. J. Clin. Oncol. 2008, 26, 3958–3964. [Google Scholar] [CrossRef]
- Irwin, M.L.; McTierman, A.; Bernstein, L.; Gilliland, F.D.; Baumgartner, R.; Baumgartner, K.; Ballard-Barbash, R. Physical activity levels among breast cancer survivors. Med. Sci. Sports Exerc. 2004, 36, 1484–1491. [Google Scholar]
- Natalucci, V.; Villarini, M.; Emili, R.; Acito, M.; Vallorani, L.; Barbieri, E.; Villarini, A. Special Attention to Physical Activity in Breast Cancer Patients during the First Wave of COVID-19 Pandemic in Italy: The DianaWeb Cohort. J. Pers. Med. 2021, 11, 381. [Google Scholar] [CrossRef]
- Meyer, J.; McDowell, C.; Lansing, J.; Brower, C.; Smith, L.; Tully, M.; Herring, M. Changes in Physical Activity and Sedentary Behavior in Response to COVID-19 and Their Associations with Mental Health in 3052 US Adults. Int. J. Environ. Res. Public Health 2020, 17, 6469. [Google Scholar] [CrossRef]
- Rock, C.L.; Demark-Wahnefried, W. Can Lifestyle Modification Increase Survival in Women Diagnosed with Breast Cancer? J. Nutr. 2002, 132, 3504S–3509S. [Google Scholar] [CrossRef]
- Esposito, K.; Chiodini, P.; Capuano, A.; Bellastella, G.; Maiorino, M.I.; Rafaniello, C.; Giugliano, D. Metabolic syndrome and postmenopausal breast cancer: Systematic review and meta-analysis. Menopause 2013, 20, 1301–1309. [Google Scholar] [CrossRef] [PubMed]
- Villarini, A.; Pasanisi, P.; Traina, A.; Mano, M.P.; Bonanni, B.; Panico, S.; Scipioni, C.; Galasso, R.; Paduos, A.; Simeoni, M.; et al. Lifestyle and breast cancer recurrences: The DIANA-5 trial. Tumori 2012, 98, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Duggan, C.; Tapsoba, J.D.D.; Stanczyk, F.; Wang, C.-Y.; Schubert, K.F.; McTiernan, A. Long-term weight loss maintenance, sex steroid hormones, and sex hormone-binding globulin. Menopause 2019, 26, 417–422. [Google Scholar] [CrossRef] [PubMed]
- Pasanisi, P.; Bruno, E.; Venturelli, E.; Morelli, D.; Oliverio, A.; Baldassari, I.; Rovera, F.; Iula, G.; Taborelli, M.; Peissel, B.; et al. A Dietary Intervention to Lower Serum Levels of IGF-I in BRCA Mutation Carriers. Cancers 2018, 10, 309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aydin, M.; Kose, E.; Odabas, I.; Meric Bingul, B.; Demirci, D.; Aydin, Z. The Effect of Exercise on Life Quality and Depression Levels of Breast Cancer Patients. Asian Pac. J. Cancer Prev. 2021, 22, 725–732. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Assessments | Instrument | Visits | |||
|---|---|---|---|---|---|
| Baseline | 3-Month | 6-Month | 12-Month | ||
| Body composition/ Anthropometrics | Body mass, BMI, waist, hip and limbs circumferences, skinfold thickness | ✓ | ✓ | ✓ | ✓ |
| Blood sample collection | Lipid profile (total cholesterol and triglycerides), insulin, glycemia, testosterone | ✓ | ✓ | ✓ | |
| Physical activity level and health-related parameters | IPAQ-SF and 6MWT | ✓ | ✓ | ✓ | |
| Dietary habits | FFQ | ✓ | ✓ | ✓ | |
| Psychological status | HADS | ✓ | ✓ | ✓ | |
| Functional status | SF-36 | ✓ | ✓ | ✓ | |
| Patients Characteristics | Tumor Characteristics | Treatments Characteristics | Clinical Data | Assessments | |||||
|---|---|---|---|---|---|---|---|---|---|
| Median (%) | Median (%) | Median (%) | Median (%) | Median (%) | |||||
| Age (years) | Histological type | Adjuvant radiotherapy | Testosterone * (ng/mL) | Physical pain (SF-36) | |||||
| ≤65 | 74 (75.5) | Ductal | 83 (84.7) | No | 14 (14.3) | ≤1.19 | 61 (82.4) | No/mild | 66 (67.3) |
| ≥65 | 24 (24.5) | Lobular | 9 (9.2) | Yes | 84 (84.7) | ≥1.2 | 13 (17.6) | Moderate/strong/very strong | 32 (32.7) |
| Mixed | 5 (5.1) | ||||||||
| Other types | 1 (1.0) | ||||||||
| Menopausal status | Grading | Neo-adjuvant chemotherapy | Insulin * (microU/mL) | Total HADS Score ** | |||||
| Pre/Peri-menopause | 27 (27.6) | G1 | 18 (18.3) | No | 96 (98.0) | 0 | 2 (2.7) | <10 | 36 (53.7) |
| Post-menopause | 71 (72.4) | G2 | 37 (37.8) | Yes | 2 (2.0) | 1–26 | 58 (78.4) | ≥10 | 31 (46.3) |
| G3 | 43 (43.9) | >27 | 14 (18.9) | ||||||
| Type of surgery | Tumor phenotype | Adjuvant chemotherapy | Glycemia (mg/dL) | Anxiety HADS score ** | |||||
| Quadrantectomy | 78 (79.6) | Luminal A-like | 31 (31.6) | No | 37 (37.8) | <110 | 75 (76.5) | <10 | 50 (74.6) |
| Mastectomy | 20 (20.4) | Luminal B HER2 negative-like | 40 (40.8) | Yes | 61 (62.2) | ≥110 | 23 (23.5) | ≥10 | 17 (25.4) |
| Luminal B HER2 positive-like | 13 (13.3) | ||||||||
| HER2 enriched-like | 5 (5.1) | ||||||||
| Triple negative | 9 (9.2) | ||||||||
| BMI (kg/m2) | Staging (Ajcc/UICC 2010) (n) | Adjuvant trastuzumab | Triglycerides (mg/dL) | Depression HADS score ** | |||||
| <25 | 5 (5.1) | I | 47 (48.0) | No | 80 (81.7) | <170 | 85 (86.7) | <10 | 59 (88.1) |
| ≥25 | 93 (94.9) | II | 36 (36.7) | Yes | 18 (18.3) | ≥170 | 13 (13.3) | ≥10 | 8 (11.9) |
| III | 15 (15.3) | ||||||||
| Waist circumference (cm) | Adjuvant endocrine therapy | Total cholesterol (mg/dL) | Practice of regular physical activity | ||||||
| <80 | 10 (10.2) | Tamoxifen | 11 (13.2) | <200 | 52 (53.1) | No | 64 (65.3) | ||
| ≥80 | 88 (89.8) | AI | 54 (66.3) | ≥200 | 46 (46.9) | Yes | 34 (34.7) | ||
| AI + LH + RHa | 5 (6.0) | ||||||||
| Tamoxifen + LH-RHa | 12 (14.5) | ||||||||
| Metabolic syndrome | Relapse | Usual diet (Kcal/day) | |||||||
| No | 77 (78.6) | No | 96 (97.6) | <1600 | 19 (19.4) | ||||
| Yes | 21 (21.4) | Yes | 2 (2.4) | ≥1600 | 79 (80.6) | ||||
| Physical function (6MWT) | |||||||||
| Passed | 17 (17.3) | ||||||||
| Failed | 81 (82.7) | ||||||||
| Body Mass Index (T0) | ||||||
|---|---|---|---|---|---|---|
| Variables | Levene’s Test p-Value | Degree of Freedom | Sum of Squares | Mean Squares | F | ANOVA F-Test p-Value |
| Waist Circumference | 0.160 | 97 | 4.74 | 0.07 | 0.544 | 0.463 |
| Insulin | 0.661 | 73 | 3.78 | 0.06 | 0.098 | 0.907 |
| Testosterone | 0.001 | 73 | 3.78 | 0.21 | 3.118 | 0.082 |
| Hads Score | 0.364 | 66 | 2.86 | 0.05 | 0.206 | 0.652 |
| Joint Pain | 0.214 | 97 | 4.74 | 0.07 | 0.377 | 0.541 |
| Glycemia | 0.007 | 97 | 4.74 | 0.13 | 1.609 | 0.208 |
| Total Cholesterol | <0.001 | 97 | 4.74 | 0.27 | 4.794 | 0.031 |
| Triglycerides | 0.379 | 97 | 4.74 | 0.06 | 0.204 | 0.653 |
| Body Mass Index (T2) | ||||||
|---|---|---|---|---|---|---|
| Variables | Levene’s Test p-Value | Degree of Freedom | Sum of Squares | Mean Squares | F | ANOVA F-Test p-Value |
| Waist Circumference | 0.509 | 97 | 21.19 | 6.05 | 36.981 | <0.001 |
| Insulin | 0.729 | 67 | 10.51 | 0.17 | 0.080 | 0.923 |
| Testosterone | 0.193 | 73 | 13.09 | 0.33 | 0.865 | 0.355 |
| Hads Score | 0.500 | 66 | 10.48 | 0.18 | 0.119 | 0.731 |
| Joint Pain | 0.538 | 97 | 21.19 | 0.24 | 0.088 | 0.768 |
| Glycemia | 0.094 | 97 | 21.19 | 0.33 | 0.500 | 0.481 |
| Total Cholesterol | 0.004 | 97 | 21.19 | 0.66 | 2.082 | 0.152 |
| Triglycerides | <0.001 | 97 | 21.19 | 0.71 | 2.279 | 0.134 |
| Body Mass Index (T3) | ||||||
|---|---|---|---|---|---|---|
| Variables | Levene’s Test p-Value | Degree of Freedom | Sum of Squares | Mean Squares | F | ANOVA F-Test p-Value |
| Waist Circumference | 0.109 | 97 | 22.77 | 9.62 | 68.479 | <0.001 |
| Insulin | 0.021 | 67 | 12.23 | 0.31 | 0.673 | 0.514 |
| Testosterone | 0.734 | 73 | 15.04 | 0.22 | 0.037 | 0.848 |
| Hads Score | 0.261 | 66 | 11.64 | 0.24 | 0.380 | 0.540 |
| Joint Pain | 0.478 | 97 | 22.77 | 0.28 | 0.171 | 0.680 |
| Glycemia | 0.264 | 97 | 22.77 | 0.29 | 0.213 | 0.645 |
| Total Cholesterol | 0.001 | 97 | 22.77 | 0.89 | 2.870 | 0.093 |
| Triglycerides | 0.692 | 97 | 22.77 | 0.25 | 0.050 | 0.823 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pistelli, M.; Natalucci, V.; Scortichini, L.; Agostinelli, V.; Lenci, E.; Crocetti, S.; Merloni, F.; Bastianelli, L.; Taus, M.; Fumelli, D.; et al. The Impact of Lifestyle Interventions in High-Risk Early Breast Cancer Patients: A Modeling Approach from a Single Institution Experience. Cancers 2021, 13, 5539. https://doi.org/10.3390/cancers13215539
Pistelli M, Natalucci V, Scortichini L, Agostinelli V, Lenci E, Crocetti S, Merloni F, Bastianelli L, Taus M, Fumelli D, et al. The Impact of Lifestyle Interventions in High-Risk Early Breast Cancer Patients: A Modeling Approach from a Single Institution Experience. Cancers. 2021; 13(21):5539. https://doi.org/10.3390/cancers13215539
Chicago/Turabian StylePistelli, Mirco, Valentina Natalucci, Laura Scortichini, Veronica Agostinelli, Edoardo Lenci, Sonia Crocetti, Filippo Merloni, Lucia Bastianelli, Marina Taus, Daniele Fumelli, and et al. 2021. "The Impact of Lifestyle Interventions in High-Risk Early Breast Cancer Patients: A Modeling Approach from a Single Institution Experience" Cancers 13, no. 21: 5539. https://doi.org/10.3390/cancers13215539
APA StylePistelli, M., Natalucci, V., Scortichini, L., Agostinelli, V., Lenci, E., Crocetti, S., Merloni, F., Bastianelli, L., Taus, M., Fumelli, D., Giulietti, G., Cola, C., Capecci, M., Serrani, R., Ceravolo, M. G., Ricci, M., Nicolai, A., Barbieri, E., Nicolai, G., ... Berardi, R. (2021). The Impact of Lifestyle Interventions in High-Risk Early Breast Cancer Patients: A Modeling Approach from a Single Institution Experience. Cancers, 13(21), 5539. https://doi.org/10.3390/cancers13215539