
Comparison of Different Systemic Therapeutic Regimes in Resectable Soft-Tissue Sarcoma—Results of a Network Meta-Analysis


 ,
,  , , , and
, , , and
Abstract
:Simple Summary
Abstract
1. Background
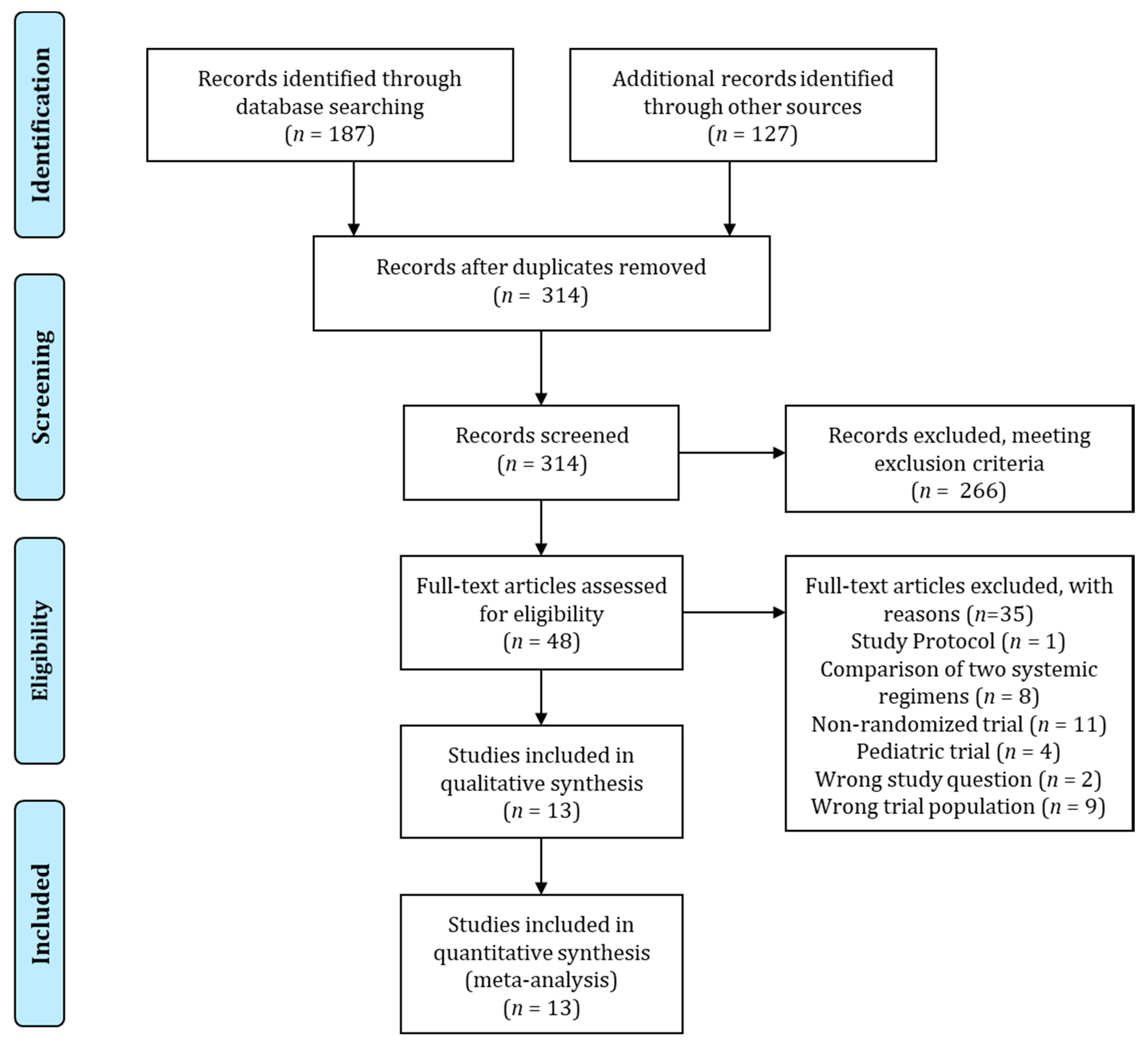
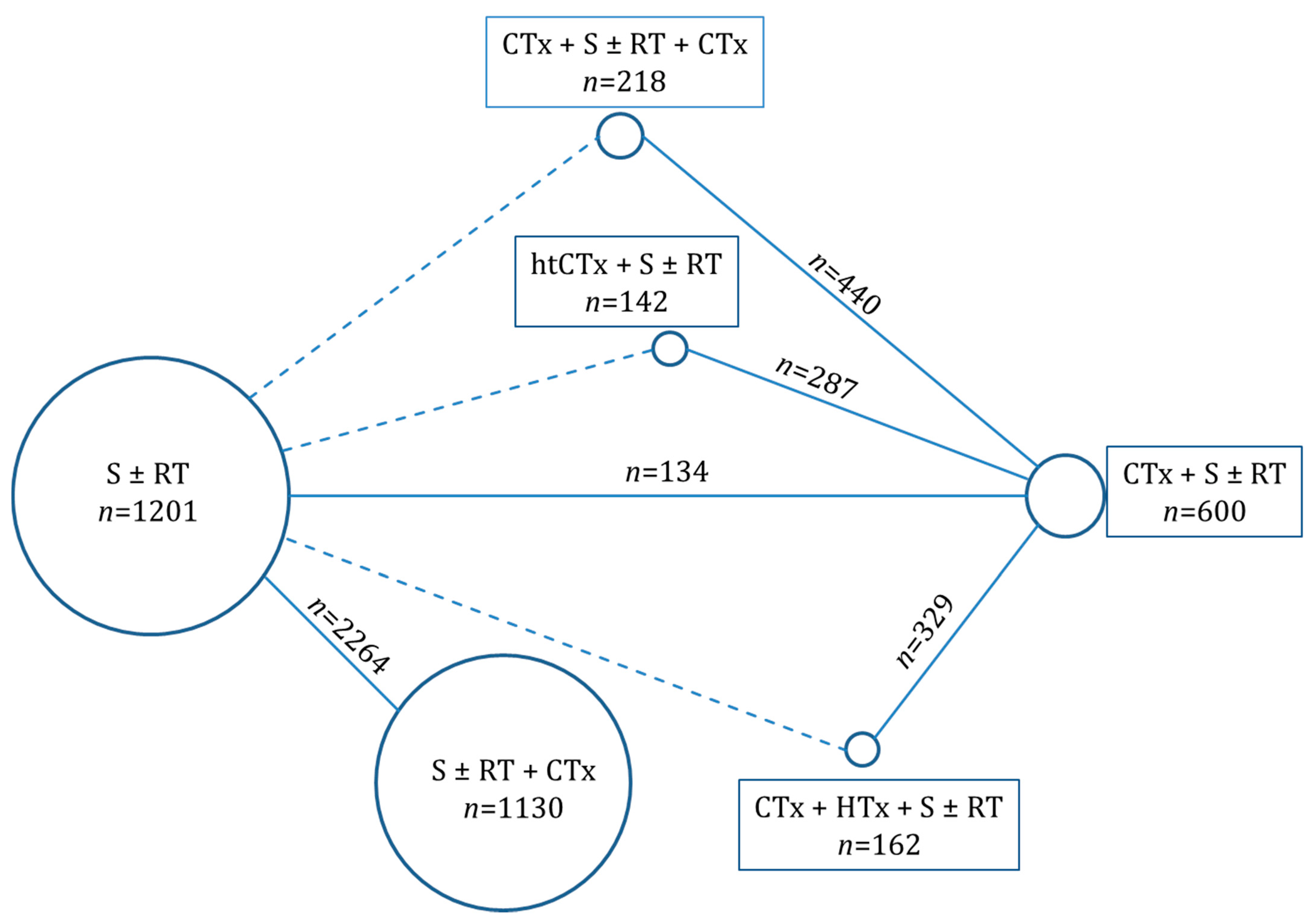
2. Methods
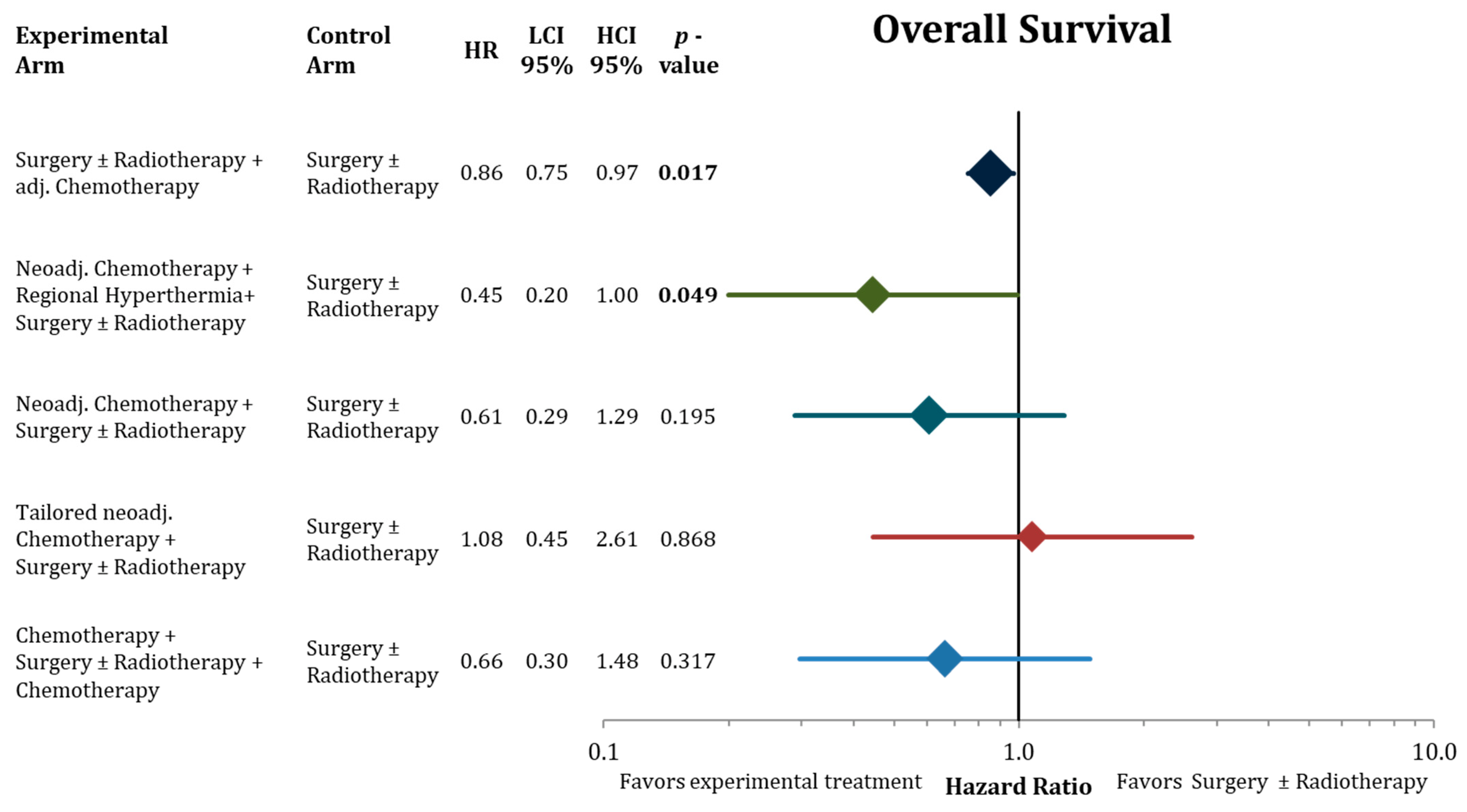
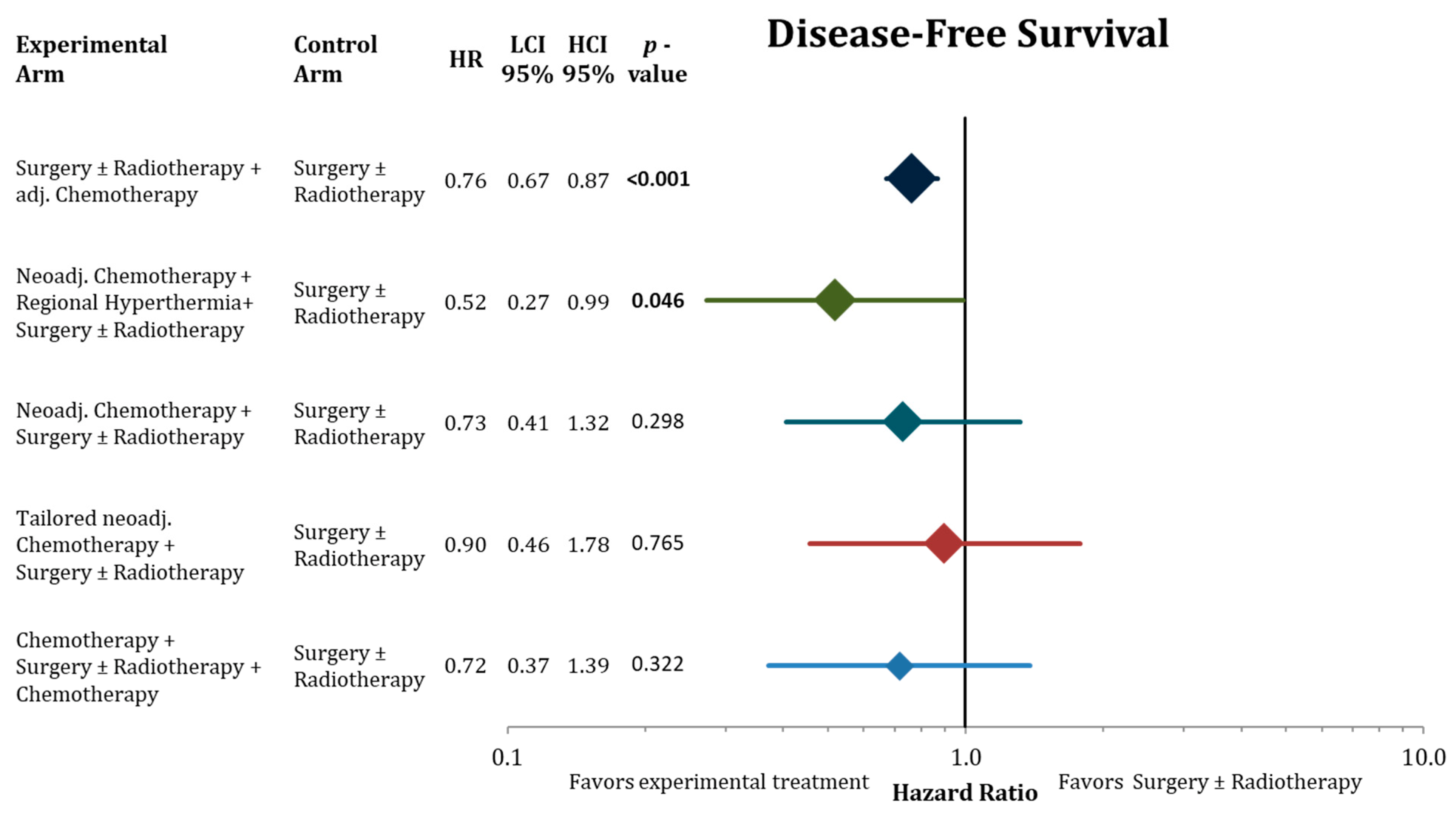
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| Abd | abdominal |
| ACTD | dactinomycin |
| adCTx | adjuvant chemotherapy |
| Amp | amputation |
| B | breast |
| C | cyclophosphamide |
| CDDP | cisplatin |
| CI | confidence interval |
| CTx | chemotherapy |
| D | doxorubicin |
| DFS | disease-free survival |
| DRFI | distant recurrence-free interval |
| DTIC | dacarbazine |
| EORTC | European Organization for Research and Treatment of Cancer |
| EPI | epirubicin |
| FU | follow-up |
| G | grade |
| GEM | gemcitabine |
| GIST | gastrointestinal stromal tumors |
| Gy | gray |
| HCI | high limit of 95% confidence interval |
| HE | hysterectomy |
| HN | head and neck |
| HTx | hyperthermia |
| HtCTx | histology tailored chemotherapy |
| IFO | ifosfamide |
| ivhet | inverse-variance heterogeneity |
| LCI | low limit of 95% confidence interval |
| LRFI | local recurrence-free interval |
| MTX | methotrexate |
| n.a. | not available |
| NCDB | National Cancer Database |
| n.r. | not reported |
| NaCTx + HTx | neoadjuvant chemotherapy and hyperthermia |
| NaCTx | neoadjuvant chemotherapy |
| OR | odds ratio |
| OS | overall survival |
| periCTx | perioperative chemotherapy |
| R | resection rate |
| RP | retroperitoneal |
| RT | radiotherapy |
| S | surgery |
| T | trunk |
| Tx | thorax |
| TXT | docetaxel |
| U | uterus |
| V | vincristine |
| WE | wide excision |
| Y | year |
References
- Davis, A.M.; O’Sullivan, B.; Turcotte, R.; Bell, R.; Catton, C.; Chabot, P.; Wunder, J.; Hammond, A.; Benk, V.; Kandel, R.; et al. Late radiation morbidity following randomization to preoperative versus postoperative radiotherapy in extremity soft tissue sarcoma. Radiother. Oncol. 2005, 75, 48–53. [Google Scholar] [CrossRef] [PubMed]
- O’Sullivan, B.; Davis, A.M.; Turcotte, R.; Bell, R.; Catton, C.; Chabot, P.; Wunder, J.; Kandel, R.; Goddard, K.; Sadura, A.; et al. Preoperative versus postoperative radiotherapy in soft-tissue sarcoma of the limbs: A randomised trial. Lancet 2002, 359, 2235–2241. [Google Scholar] [CrossRef]
- Rosenberg, S.A.; Tepper, J.; Glatstein, E.; Costa, J.; Baker, A.; Brennan, M.; DeMoss, E.V.; Seipp, C.; Sindelar, W.F.; Sugarbaker, P.; et al. The treatment of soft-tissue sarcomas of the extremities: Prospective randomized evaluations of (1) limb-sparing surgery plus radiation therapy compared with amputation and (2) the role of adjuvant chemotherapy. Ann. Surg. 1982, 196, 305–315. [Google Scholar] [CrossRef] [PubMed]
- Bonvalot, S.; Gronchi, A.; Le Péchoux, C.; Swallow, C.J.; Strauss, D.; Meeus, P.; van Coevorden, F.; Stoldt, S.; Stoeckle, E.; Rutkowski, P.; et al. Preoperative radiotherapy plus surgery versus surgery alone for patients with primary retroperitoneal sarcoma (EORTC-62092: STRASS): A multicentre, open-label, randomised, phase 3 trial. Lancet Oncol. 2020, 21, 1366–1377. [Google Scholar] [CrossRef]
- Kawamoto, T.; Hara, H.; Morishita, M.; Fukase, N.; Kawakami, Y.; Takemori, T.; Fujiwara, S.; Kitayama, K.; Yahiro, S.; Miyamoto, T.; et al. Prognostic influence of the treatment approach for pulmonary metastasis in patients with soft tissue sarcoma. Clin. Exp. Metastasis 2020, 37, 509–517. [Google Scholar] [CrossRef] [PubMed]
- Adjuvant chemotherapy for localised resectable soft-tissue sarcoma of adults: Meta-analysis of individual data. Sarcoma Meta-analysis Collaboration. Lancet 1997, 350, 1647–1654. [CrossRef]
- Pervaiz, N.; Colterjohn, N.; Farrokhyar, F.; Tozer, R.; Figueredo, A.; Ghert, M. A systematic meta-analysis of randomized controlled trials of adjuvant chemotherapy for localized resectable soft-tissue sarcoma. Cancer 2008, 113, 573–581. [Google Scholar] [CrossRef] [PubMed]
- Woll, P.J.; Reichardt, P.; Le Cesne, A.; Bonvalot, S.; Azzarelli, A.; Hoekstra, H.J.; Leahy, M.; Van Coevorden, F.; Verweij, J.; Hogendoorn, P.C.; et al. Adjuvant chemotherapy with doxorubicin, ifosfamide, and lenograstim for resected soft-tissue sarcoma (EORTC 62931): A multicentre randomised controlled trial. Lancet Oncol. 2012, 13, 1045–1054. [Google Scholar] [CrossRef]
- Corradini, S.; Krug, D.; Meattini, I.; Matuschek, C.; Bolke, E.; Francolini, G.; Baumann, R.; Figlia, V.; Pazos, M.; Tonetto, F.; et al. Preoperative radiotherapy: A paradigm shift in the treatment of breast cancer? A review of literature. Crit. Rev. Oncol. Hematol. 2019, 141, 102–111. [Google Scholar] [CrossRef] [PubMed]
- Sun, R.; Wei, L.J. Regional Hyperthermia With Neoadjuvant Chemotherapy for Treatment of Soft Tissue Sarcoma. JAMA Oncol. 2019, 5, 112–113. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [Green Version]
- Hutton, B.; Salanti, G.; Caldwell, D.M.; Chaimani, A.; Schmid, C.H.; Cameron, C.; Ioannidis, J.P.; Straus, S.; Thorlund, K.; Jansen, J.P.; et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: Checklist and explanations. Ann. Intern. Med. 2015, 162, 777–784. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parmar, M.K.; Torri, V.; Stewart, L. Extracting summary statistics to perform meta-analyses of the published literature for survival endpoints. Stat. Med. 1998, 17, 2815–2834. [Google Scholar] [CrossRef]
- Tierney, J.F.; Stewart, L.A.; Ghersi, D.; Burdett, S.; Sydes, M.R. Practical methods for incorporating summary time-to-event data into meta-analysis. Trials 2007, 8, 16. [Google Scholar] [CrossRef] [Green Version]
- Doi, S.A.; Barendregt, J.J.; Khan, S.; Thalib, L.; Williams, G.M. Advances in the meta-analysis of heterogeneous clinical trials I: The inverse variance heterogeneity model. Contemp. Clin. Trials 2015, 45, 130–138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bramwell, V.; Rouesse, J.; Steward, W.; Santoro, A.; Schraffordt-Koops, H.; Buesa, J.; Ruka, W.; Priario, J.; Wagener, T.; Burgers, M.; et al. Adjuvant CYVADIC chemotherapy for adult soft tissue sarcoma--reduced local recurrence but no improvement in survival: A study of the European Organization for Research and Treatment of Cancer Soft Tissue and Bone Sarcoma Group. J. Clin. Oncol. 1994, 12, 1137–1149. [Google Scholar] [CrossRef] [PubMed]
- Adjuvant chemotherapy for localised resectable soft tissue sarcoma in adults. Sarcoma Meta-analysis Collaboration (SMAC). Cochrane Database Syst. Rev. 2000, Cd001419. [CrossRef]
- Gortzak, E.; Azzarelli, A.; Buesa, J.; Bramwell, V.H.; van Coevorden, F.; van Geel, A.N.; Ezzat, A.; Santoro, A.; Oosterhuis, J.W.; van Glabbeke, M.; et al. A randomised phase II study on neo-adjuvant chemotherapy for ‘high-risk’ adult soft-tissue sarcoma. Eur. J. Cancer 2001, 37, 1096–1103. [Google Scholar] [CrossRef]
- Eilber, F.R.; Giuliano, A.E.; Huth, J.F.; Morton, D.L. A randomized prospective trial using postoperative adjuvant chemotherapy (adriamycin) in high-grade extremity soft-tissue sarcoma. Am. J. Clin. Oncol. 1988, 11, 39–45. [Google Scholar] [CrossRef]
- Gronchi, A.; Stacchiotti, S.; Verderio, P.; Ferrari, S.; Martin Broto, J.; Lopez-Pousa, A.; Llombart-Bosch, A.; Dei Tos, A.P.; Collini, P.; Jurado, J.C.; et al. Short, full-dose adjuvant chemotherapy (CT) in high-risk adult soft tissue sarcomas (STS): Long-term follow-up of a randomized clinical trial from the Italian Sarcoma Group and the Spanish Sarcoma Group. Ann. Oncol. 2016, 27, 2283–2288. [Google Scholar] [CrossRef] [PubMed]
- Issels, R.D.; Lindner, L.H.; Verweij, J.; Wessalowski, R.; Reichardt, P.; Wust, P.; Ghadjar, P.; Hohenberger, P.; Angele, M.; Salat, C.; et al. Effect of Neoadjuvant Chemotherapy Plus Regional Hyperthermia on Long-term Outcomes Among Patients With Localized High-Risk Soft Tissue Sarcoma: The EORTC 62961-ESHO 95 Randomized Clinical Trial. JAMA Oncol. 2018, 4, 483–492. [Google Scholar] [CrossRef] [PubMed]
- Issels, R.D.; Lindner, L.H.; Verweij, J.; Wust, P.; Reichardt, P.; Schem, B.C.; Abdel-Rahman, S.; Daugaard, S.; Salat, C.; Wendtner, C.M.; et al. Neo-adjuvant chemotherapy alone or with regional hyperthermia for localised high-risk soft-tissue sarcoma: A randomised phase 3 multicentre study. Lancet Oncol. 2010, 11, 561–570. [Google Scholar] [CrossRef] [Green Version]
- Gronchi, A.; Ferrari, S.; Quagliuolo, V.; Broto, J.M.; Pousa, A.L.; Grignani, G.; Basso, U.; Blay, J.Y.; Tendero, O.; Beveridge, R.D.; et al. Histotype-tailored neoadjuvant chemotherapy versus standard chemotherapy in patients with high-risk soft-tissue sarcomas (ISG-STS 1001): An international, open-label, randomised, controlled, phase 3, multicentre trial. Lancet Oncol. 2017, 18, 812–822. [Google Scholar] [CrossRef]
- Gronchi, A.; Palmerini, E.; Quagliuolo, V.; Martin Broto, J.; Lopez Pousa, A.; Grignani, G.; Brunello, A.; Blay, J.Y.; Tendero, O.; Diaz Beveridge, R.; et al. Neoadjuvant Chemotherapy in High-Risk Soft Tissue Sarcomas: Final Results of a Randomized Trial From Italian (ISG), Spanish (GEIS), French (FSG), and Polish (PSG) Sarcoma Groups. J. Clin. Oncol. 2020, 38, 2178–2186. [Google Scholar] [CrossRef]
- Omura, G.A.; Blessing, J.A.; Major, F.; Lifshitz, S.; Ehrlich, C.E.; Mangan, C.; Beecham, J.; Park, R.; Silverberg, S. A randomized clinical trial of adjuvant adriamycin in uterine sarcomas: A Gynecologic Oncology Group Study. J. Clin. Oncol. 1985, 3, 1240–1245. [Google Scholar] [CrossRef]
- Benjamin, R.S.; Terjanian, T.O.; Fenoglio, C.J.; Barkley, H.T.; Evans, H.L.; Murphy, W.K.; Martin, R.G. The importance of combination chemotherapy for adjuvant treatment of high-risk patients with soft-tissue sarcomas of the extremities. In Adjuvant Therapy of Cancer V; Salmon, S.E., Ed.; Grune and Stratton: Orlando, FL, USA, 1987; pp. 735–744. [Google Scholar]
- Edmonson, J.H.; Fleming, T.R.; Ivins, J.C.; Burgert, E.O., Jr.; Soule, E.H.; O’Connell, M.J.; Sim, F.H.; Ahmann, D.L. Randomized study of systemic chemotherapy following complete excision of nonosseous sarcomas. J. Clin. Oncol. 1984, 2, 1390–1396. [Google Scholar] [CrossRef] [PubMed]
- JH, E. Systemic chemotherapy following complete excision of nonosseous sarcomas: Mayo Clinic experience. Cancer Treat. Symp. 1985, 3, 89–97. [Google Scholar]
- Rosenberg, S.A.; Tepper, J.; Glatstein, E.; Costa, J.; Young, R.; Baker, A.; Brennan, M.F.; Demoss, E.V.; Seipp, C.; Sindelar, W.F.; et al. Prospective randomized evaluation of adjuvant chemotherapy in adults with soft tissue sarcomas of the extremities. Cancer 1983, 52, 424–434. [Google Scholar] [CrossRef]
- Chang, A.E.; Kinsella, T.; Glatstein, E.; Baker, A.R.; Sindelar, W.F.; Lotze, M.T.; Danforth, D.N., Jr.; Sugarbaker, P.H.; Lack, E.E.; Steinberg, S.M.; et al. Adjuvant chemotherapy for patients with high-grade soft-tissue sarcomas of the extremity. J. Clin. Oncol. 1988, 6, 1491–1500. [Google Scholar] [CrossRef]
- Glenn, J.; Kinsella, T.; Glatstein, E.; Tepper, J.; Baker, A.; Sugarbaker, P.; Sindelar, W.; Roth, J.; Brennan, M.; Costa, J.; et al. A randomized, prospective trial of adjuvant chemotherapy in adults with soft tissue sarcomas of the head and neck, breast, and trunk. Cancer 1985, 55, 1206–1214. [Google Scholar] [CrossRef]
- Glenn, J.; Sindelar, W.F.; Kinsella, T.; Glatstein, E.; Tepper, J.; Costa, J.; Baker, A.; Sugarbaker, P.; Brennan, M.F.; Seipp, C.; et al. Results of multimodality therapy of resectable soft-tissue sarcomas of the retroperitoneum. Surgery 1985, 97, 316–325. [Google Scholar] [PubMed]
- Antman, K.; Suit, H.; Amato, D.; Corson, J.; Wood, W.; Proppe, K.; Harmon, D.; Carey, R.; Greenberger, J.; Blum, R.; et al. Preliminary results of a randomized trial of adjuvant doxorubicin for sarcomas: Lack of apparent difference between treatment groups. J. Clin. Oncol. 1984, 2, 601–608. [Google Scholar] [CrossRef] [PubMed]
- Lerner, H.J.; Amato, D.A.; Savlov, E.D.; DeWys, W.D.; Mittleman, A.; Urtasun, R.C.; Sobel, S.; Shiraki, M. Eastern Cooperative Oncology Group: A comparison of adjuvant doxorubicin and observation for patients with localized soft tissue sarcoma. J. Clin. Oncol. 1987, 5, 613–617. [Google Scholar] [CrossRef] [PubMed]
- Ravaud, A. Adjuvant chemotherapy with cyvadic in high risk soft tissue sarcoma: A randomized prospective trial. In Adjuvant Therapy of Cancer VI; Salmon, S.E., Ed.; Saunders, WB: Philadelphia, PA, USA, 1990; pp. 556–566. [Google Scholar]
- Alvegard, T.A.; Sigurdsson, H.; Mouridsen, H.; Solheim, O.; Unsgaard, B.; Ringborg, U.; Dahl, O.; Nordentoft, A.M.; Blomqvist, C.; Rydholm, A.; et al. Adjuvant chemotherapy with doxorubicin in high-grade soft tissue sarcoma: A randomized trial of the Scandinavian Sarcoma Group. J. Clin. Oncol. 1989, 7, 1504–1513. [Google Scholar] [CrossRef]
- Gherlinzoni, F.; Bacci, G.; Picci, P.; Capanna, R.; Calderoni, P.; Lorenzi, E.G.; Bernini, M.; Emiliani, E.; Barbieri, E.; Normand, A.; et al. A randomized trial for the treatment of high-grade soft-tissue sarcomas of the extremities: Preliminary observations. J. Clin. Oncol. 1986, 4, 552–558. [Google Scholar] [CrossRef]
- Picci, P.; Bacci, G.; Gherlizoni, F.; Capanna, R.; Mercuri, M.; Ruggieri, P.; Baldini, N.; Avella, M.; Pignatti, G.; Manfrini, M. Results of randomized trial for the treatment of localised soft tissue tumors (STS) of the extremities in adult patients. In Recent Concepts in Sarcoma Treatment; Ryan, J.R., Baker, L.H., Eds.; Kluwer Academic Publishers: Dordrecht, The Netherlands, 1988; pp. 144–148. [Google Scholar]
- Baker, L.H. Adjuvant Therapy for Soft Tissue Sarcomas. In Recent Concepts in Sarcoma Treatment: Proceedings of the International Symposium on Sarcomas, Tarpon Springs, FL, USA, 8–10 October 1987; Ryan, J.R., Baker, L.O., Eds.; Springer: Dordrecht, The Netherlands, 1988; pp. 130–135. [Google Scholar] [CrossRef]
- Antman, K.; Ryan, L.; Borden, E.; Wood, W.C.; Lerner, H.L.; Corson, J.M.; Carey, R.; Suit, H.; Balcerak, S. Pooled results from three randomized adjuvant studies of doxoru bicin versus observation in soft tissue sarcoma: 10 year results and review of the literature. In Adjuvant Therapy of Cancer VI; Salmon, S.E., Ed.; Saunders WB: Philadelphia, PA, USA, 1990; pp. 529–543. [Google Scholar]
- Pautier, P.; Floquet, A.; Gladieff, L.; Bompas, E.; Ray-Coquard, I.; Piperno-Neumann, S.; Selle, F.; Guillemet, C.; Weber, B.; Largillier, R.; et al. A randomized clinical trial of adjuvant chemotherapy with doxorubicin, ifosfamide, and cisplatin followed by radiotherapy versus radiotherapy alone in patients with localized uterine sarcomas (SARCGYN study). A study of the French Sarcoma Group. Ann. Oncol. 2013, 24, 1099–1104. [Google Scholar] [CrossRef]
- Fakhrai, N.; Ebm, C.; Kostler, W.J.; Jantsch, M.; Abdolvahab, F.; Dominkus, M.; Pokrajac, B.; Kauer-Dorner, D.; Zielinski, C.C.; Brodowicz, T.; et al. Intensified adjuvant IFADIC chemotherapy in combination with radiotherapy versus radiotherapy alone for soft tissue sarcoma: Long-term follow-up of a prospective randomized feasibility trial. Wien. Klin. Wochenschr. 2010, 122, 614–619. [Google Scholar] [CrossRef] [PubMed]
- Frustaci, S.; Gherlinzoni, F.; De Paoli, A.; Bonetti, M.; Azzarelli, A.; Comandone, A.; Olmi, P.; Buonadonna, A.; Pignatti, G.; Barbieri, E.; et al. Adjuvant chemotherapy for adult soft tissue sarcomas of the extremities and girdles: Results of the Italian randomized cooperative trial. J. Clin. Oncol. 2001, 19, 1238–1247. [Google Scholar] [CrossRef]
- Frustaci, S.; De Paoli, A.; Bidoli, E.; La Mura, N.; Berretta, M.; Buonadonna, A.; Boz, G.; Gherlinzoni, F. Ifosfamide in the Adjuvant Therapy of Soft Tissue Sarcomas. Oncology 2003, 65 (Suppl. 2), 80–84. [Google Scholar] [CrossRef] [PubMed]
- Petrioli, R.; Coratti, A.; Correale, P.; D’Aniello, C.; Grimaldi, L.; Tanzini, G.; Civitelli, S.; Marsili, S.; Messinese, S.; Marzocca, G.; et al. Adjuvant epirubicin with or without Ifosfamide for adult soft-tissue sarcoma. Am. J. Clin. Oncol. 2002, 25, 468–473. [Google Scholar] [CrossRef] [PubMed]
- Hensley, M.L.; Enserro, D.; Hatcher, H.; Ottevanger, P.B.; Krarup-Hansen, A.; Blay, J.Y.; Fisher, C.; Moxley, K.M.; Lele, S.B.; Lea, J.S.; et al. Adjuvant Gemcitabine Plus Docetaxel Followed by Doxorubicin Versus Observation for High-Grade Uterine Leiomyosarcoma: A Phase III NRG Oncology/Gynecologic Oncology Group Study. J. Clin. Oncol. 2018, 36, JCO1800454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gronchi, A.; Frustaci, S.; Mercuri, M.; Martin, J.; Lopez-Pousa, A.; Verderio, P.; Mariani, L.; Valagussa, P.; Miceli, R.; Stacchiotti, S.; et al. Short, full-dose adjuvant chemotherapy in high-risk adult soft tissue sarcomas: A randomized clinical trial from the Italian Sarcoma Group and the Spanish Sarcoma Group. J. Clin. Oncol. 2012, 30, 850–856. [Google Scholar] [CrossRef] [PubMed]
- Casali, P.G.; Abecassis, N.; Aro, H.T.; Bauer, S.; Biagini, R.; Bielack, S.; Bonvalot, S.; Boukovinas, I.; Bovee, J.; Brodowicz, T.; et al. Gastrointestinal stromal tumours: ESMO-EURACAN Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2018, 29, iv267. [Google Scholar] [CrossRef] [PubMed]
- Lindner, L.H.; Blay, J.Y.; Eggermont, A.M.M.; Issels, R.D. Perioperative chemotherapy and regional hyperthermia for high-risk adult-type soft tissue sarcomas. Eur. J. Cancer 2021, 147, 164–169. [Google Scholar] [CrossRef]
- Le Cesne, A.; Ouali, M.; Leahy, M.G.; Santoro, A.; Hoekstra, H.J.; Hohenberger, P.; Van Coevorden, F.; Rutkowski, P.; Van Hoesel, R.; Verweij, J.; et al. Doxorubicin-based adjuvant chemotherapy in soft tissue sarcoma: Pooled analysis of two STBSG-EORTC phase III clinical trials. Ann. Oncol. 2014, 25, 2425–2432. [Google Scholar] [CrossRef]
- Ingram, D.R.; Dillon, L.M.; Lev, D.C.; Lazar, A.; Demicco, E.G.; Eisenberg, B.L.; Miller, T.W. Estrogen receptor alpha and androgen receptor are commonly expressed in well-differentiated liposarcoma. BMC Clin. Pathol. 2014, 14, 42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Graham, D.S.; van Dams, R.; Jackson, N.J.; Onyshchenko, M.; Eckardt, M.A.; DiPardo, B.J.; Nelson, S.D.; Chmielowski, B.; Shabason, J.E.; Singh, A.S.; et al. Chemotherapy and Survival in Patients with Primary High-Grade Extremity and Trunk Soft Tissue Sarcoma. Cancers 2020, 12, 2389. [Google Scholar] [CrossRef]
- Pasquali, S.; Colombo, C.; Pizzamiglio, S.; Verderio, P.; Callegaro, D.; Stacchiotti, S.; Martin Broto, J.; Lopez-Pousa, A.; Ferrari, S.; Poveda, A.; et al. High-risk soft tissue sarcomas treated with perioperative chemotherapy: Improving prognostic classification in a randomised clinical trial. Eur. J. Cancer 2018, 93, 28–36. [Google Scholar] [CrossRef]
- Callegaro, D.; Miceli, R.; Bonvalot, S.; Ferguson, P.; Strauss, D.C.; Levy, A.; Griffin, A.; Hayes, A.J.; Stacchiotti, S.; Pechoux, C.L.; et al. Development and external validation of two nomograms to predict overall survival and occurrence of distant metastases in adults after surgical resection of localised soft-tissue sarcomas of the extremities: A retrospective analysis. Lancet Oncol. 2016, 17, 671–680. [Google Scholar] [CrossRef]
- Chibon, F.; Lagarde, P.; Salas, S.; Perot, G.; Brouste, V.; Tirode, F.; Lucchesi, C.; de Reynies, A.; Kauffmann, A.; Bui, B.; et al. Validated prediction of clinical outcome in sarcomas and multiple types of cancer on the basis of a gene expression signature related to genome complexity. Nat. Med. 2010, 16, 781–787. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Trial | Year | N Total | Med. AGE | Female | FU (y) | Site | G3+ | Exp. Arm | n | Contr. Arm | n | Surgery | RT | CTx |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| GOG (Omura) [25] | 1997 | 225 | n.a. | 100% | 9.4 * | U | 67% * | adCTx | 113 | S ± RT | 112 | HE | n.a. | D |
| MDA (Benjamin) [6,26] | 1997 | 54 | n.a. | 54% * | 9.4 * | Extr.,T | 67% * | adCTx | 26 | S ± RT | 28 | n.a. | n.a. | D + C + ACTD + V |
| Mayo (Edmonson) [27,28] | 1997 | 57 | n.a. | 54% * | 9.4 * | Extr., T | 67% * | adCTx | 28 | S ± RT | 29 | n.a | n.a. | D + V + ACTD + DTIC |
| NCI4 (Rosenberg/Chang) [29,30] | 1997 | 25 | n.a. | 54% * | 9.4 * | Extr. | 67% * | adCTx | 17 | S ± RT | 8 | Amp or WE | 45–70 Gy | D + C + MTX |
| NCI5 (Glenn) [31,32] | 1997 | 79 | n.a. | 54% * | 9.4 * | T, HN, RP, B | 67% * | adCTx | 38 | S ± RT | 41 | WE | 60–63 Gy | D + C + MTX |
| NCI6 (Rosenberg/Chang) [29,30] | 1997 | 41 | n.a. | 54% * | 9.4 * | Extr. | 67% * | adCTx | 21 | S ± RT | 20 | n.a. | n.a. | D + C + MTX |
| EORTC (Bramwell) [16] | 1997 | 467 | n.a. | 54% * | 9.4 * | Extr., T, HN | 67% * | adCTx | 234 | S ± RT | 233 | n.a. | 40–50 Gy | D + C + V + DTIC |
| DFCI/MGH (Antman) [33] | 1997 | 46 | n.a. | 54% * | 9.4 * | Extr. T, HN, RP | 67% * | adCTx | 21 | S ± RT | 25 | Amp or WE | 62.5–67.5 Gy | D |
| ECOG (Lerner) [34] | 1997 | 47 | n.a. | 54% * | 9.4 * | Extr., T, HN, RP | 67% * | adCTx | 24 | S ± RT | 23 | Amp or WE | 50–64 Gy | D |
| Bergonie (Ravaud) [35] | 1997 | 65 | n.a. | 54% * | 9.4 * | Extr., T, HN, RP | 67% * | adCTx | 33 | S ± RT | 32 | n.a. | n.a. | D + C + V + DTIC |
| SSG (Alvegard) [36] | 1997 | 240 | 57 | 49% | 9.4 * | Extr., T, HN, B, Tx, Abd. | 100% | adCTx | 121 | S ± RT | 119 | WE | 42–51 Gy | D |
| Rizzoli (Gherlinzoni/Picci) [37,38] | 1997 | 77 | n.a. | 54% * | 9.4 * | Extr. | 67% * | adCTx | 34 | S ± RT | 43 | WE | 45 Gy | D |
| IGSC (Baker/Antman) [39,40] | 1997 | 92 | n.a. | 54% * | 9.4 * | Extr., T, HN, RP | 67% * | adCTx | 43 | S ± RT | 49 | n.a. | n.a. | D |
| SAKK [6] | 1997 | 29 | n.a. | 54% * | 9.4 * | Extr., T | 67% * | adCTx | 14 | S ± RT | 15 | n.a. | n.a. | D + IFO |
| Pautier [41] | 2013 | 81 | 55 | 100% | 4.3 | U | n.a. | adCTx | 39 | S + RT | 42 | n.a. | 45/1.8 Gy | D + IFO + CDDP |
| Woll [8] | 2012 | 351 | 49 | 45% | 8 | Extr., T, HN | 46% | adCTx | 175 | S ± RT | 176 | n.a. | 50–66 Gy | D + IFO |
| Fakrai [42] | 2010 | 58 | 52 | 46% | 8.1 | Extr., T, RP | 73% | adCTx | 31 | S + RT | 27 | “adequate” | 51/1.7 Gy | D + IFO + DTIC |
| Frustaci [43,44] | 2001/2003 | 104 | n.a. | 41% | 4.9 | Extr., T | 100% | adCTx | 53 | S ± RT | 51 | HE | 44.8–66 Gy | EPI + IFO |
| Petrioli [45] | 2002 | 88 | 53 | 49% | 7.8 | Extr., T, Abd., RP | 41% | adCTx | 45 | S ± RT | 43 | WE | 54–60 Gy | EPI + IFO |
| Hensley [46] | 2018 | 38 | n.a. | 100% | 4.3 | U | 100% | adCTx | 20 | S | 18 | HE | n.a. | TXT + GEM + D |
| Issels [21,22] | 2018 | 341 | 52 | 44% | 11.3 | Extr., T, HN | 53% | NaCTx+HTx | 162 | NaCTx | 167 | n.a | 50–66 Gy | D + IFO |
| Gronchi [23,24] | 2017/-20 | 286 | 40 | 38% | 4.3 | Extr., T, Abd. | 100% | HtCTx | 142 | NaCTx | 144 | n.a | 44–66 Gy | EPI + IFO |
| Gortzak [18] | 2001 | 134 | 53 | 40% | 7.3 | Extr., T, HN | n.a. | NacCTx | 67 | S ± RT | 67 | Amp or WE | 60–80 Gy | D + IFO |
| Gronchi [20,47] | 2016 | 321 | 49 | n.a. | 9.75 | Extr., T | n.a. | NaCTx | 161 | periCTx | 160 | n.a | 44–66 Gy | EPI + IFO |
| Eilber [19] | 1988 | 119 | 59 | 45% | 2.3 | Extr. | 100% | periCTx | 57 | RT + S | 62 | Amp or WE | 17.5/3.5 Gy | D |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haussmann, J.; Matuschek, C.; Bölke, E.; Tamaskovics, B.; Corradini, S.; Wessalowski, R.; Maas, K.; Schmidt, L.; Orth, K.; Peiper, M.; et al. Comparison of Different Systemic Therapeutic Regimes in Resectable Soft-Tissue Sarcoma—Results of a Network Meta-Analysis. Cancers 2021, 13, 5631. https://doi.org/10.3390/cancers13225631
Haussmann J, Matuschek C, Bölke E, Tamaskovics B, Corradini S, Wessalowski R, Maas K, Schmidt L, Orth K, Peiper M, et al. Comparison of Different Systemic Therapeutic Regimes in Resectable Soft-Tissue Sarcoma—Results of a Network Meta-Analysis. Cancers. 2021; 13(22):5631. https://doi.org/10.3390/cancers13225631
Chicago/Turabian StyleHaussmann, Jan, Christiane Matuschek, Edwin Bölke, Balint Tamaskovics, Stefanie Corradini, Rüdiger Wessalowski, Kitti Maas, Livia Schmidt, Klaus Orth, Matthias Peiper, and et al. 2021. "Comparison of Different Systemic Therapeutic Regimes in Resectable Soft-Tissue Sarcoma—Results of a Network Meta-Analysis" Cancers 13, no. 22: 5631. https://doi.org/10.3390/cancers13225631
APA StyleHaussmann, J., Matuschek, C., Bölke, E., Tamaskovics, B., Corradini, S., Wessalowski, R., Maas, K., Schmidt, L., Orth, K., Peiper, M., Keitel, V., Feldt, T., Jensen, B. -E. O., Luedde, T., Fischer, J., Knoefel, W. T., Ashmawy, H., Pedotoa, A., Kammers, K., & Budach, W. (2021). Comparison of Different Systemic Therapeutic Regimes in Resectable Soft-Tissue Sarcoma—Results of a Network Meta-Analysis. Cancers, 13(22), 5631. https://doi.org/10.3390/cancers13225631