
Oral Contraceptive Use and Breast Cancer Risk Assessment: A Systematic Review and Meta-Analysis of Case-Control Studies, 2009–2020

 ,
,  ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
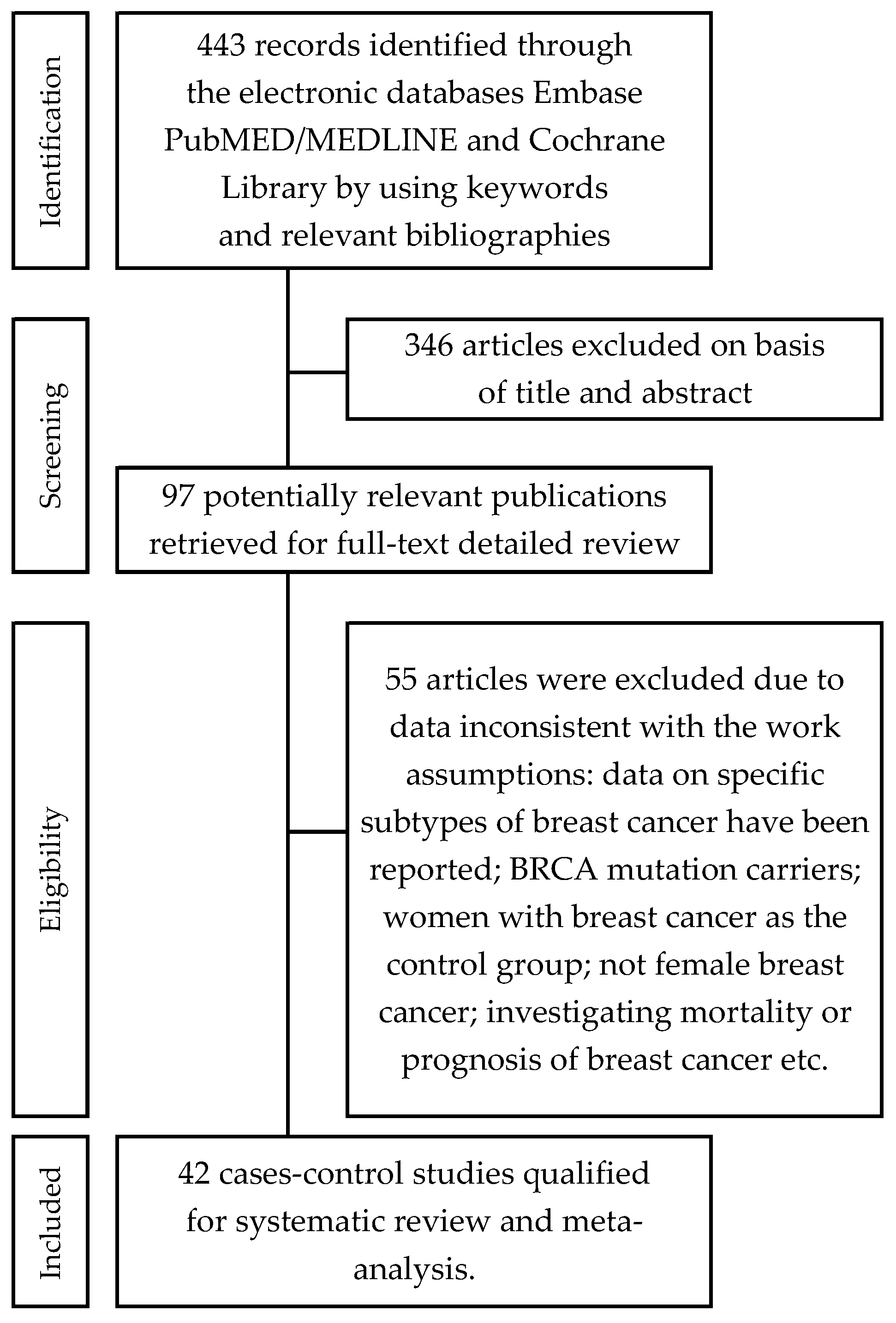
2.1. Search Strategy and Selection Criteria
2.2. Data Extraction
2.3. Assessment of Study Quality
2.4. Statistical Analysis
2.5. Subgroup Analysis
3. Results
- seven (7) case-control studies were conducted in the Americas,
- six (6) in Africa,
- sixteen (16) in the Middle East,
- eleven (11) in Asia,
- one (1) in Europe,
- one (1) was an international, multicenter research study.
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- The Cancer Atlas: Breast Cancer Accounts for Almost a Quarter of New Cancer Cases among Women. Available online: https://canceratlas.cancer.org/wp-content/uploads/2019/09/CA3_BreastCancer.pdf (accessed on 12 March 2021).
- Harvey, J.; Murff, H.J.; David, R.; Spigel, D.R.; Syngal, S. Does this patient have a family history of cancer? An evidence-based analysis of the accuracy of family cancer history. JAMA 2004, 292, 1480–1489. [Google Scholar] [CrossRef]
- Palma, M.; Ristori, E.; Ricevuto, E.; Giannini, G.; Gulino, A. BRCA1 and BRCA2: The genetic testing and the current management options for mutation carriers. Crit. Rev. Oncol. Hematol. 2006, 57, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Hall, J.M.; Friedman, L.; Guenther, C.; Lee, M.K.; Weber, J.; Black, D.M.; King, M.C. Closing in on a breast cancer gene on chromosome 17q. Am. J. Hum. Genet. 1992, 50, 1235–1242. [Google Scholar]
- Wooster, R.; Neuhausen, S.L.; Mangion, J.; Quirk, Y.; Ford, D.; Collins, N.; Nguyen, K.; Seal, S.; Tran, T.; Averill, D. Localization of a breast cancer susceptibility gene, BRCA2, to chromosome 13q12–13. Science 1994, 265, 2088–2090. [Google Scholar] [CrossRef]
- Blows, F.M.; Driver, K.E.; Schmidt, M.K.; Broeks, A.; van Leeuwen, F.E.; Wesseling, J.; Cheang, M.C.; Gelmon, K.; Nielsen, T.O.; Blomqvist, C.; et al. Subtyping of breast cancer by immunohistochemistry to investigate a relationship between subtype and short and long term survival: A collaborative analysis of data for 10,159 cases from 12 studies. PLoS Med. 2010, 75, e1000279. [Google Scholar] [CrossRef]
- Kurebayashi, J.; Moriya, T.; Ishida, T.; Hirakawa, H.; Kurosumi, M.; Akiyama, F.; Kinoshita, T.; Takei, H.; Takahashi, K.; Ikeda, M.; et al. The prevalence of intrinsic subtypes and prognosis in breast cancer patients of different races. Breast 2007, 16 (Suppl. S2), 72–77. [Google Scholar] [CrossRef]
- Yang, X.R.; Chang-Claude, J.; Goode, E.L.; Yang, X.R.; Chang-Claude, J.; Goode, E.L.; Couch, F.J.; Nevanlinna, H.; Milne, R.L.; Gaudet, M.; et al. Associations of breast cancer risk factors with tumor subtypes: A pooled analysis from the Breast Cancer Association Consortium studies. J. Natl. Cancer Inst. 2011, 103, 250–263. [Google Scholar] [CrossRef]
- Collaborative Group on Hormonal Factors in Breast Cancer. Menarche, menopause, and breast cancer risk: Individual participant meta-analysis, including 118,964 women with breast cancer from 117 epidemiological studies. Lancet Oncol. 2012, 13, 1141–1151. [Google Scholar] [CrossRef]
- Mikkelsen, A.P.; Egerup, P.; Ebert, J.F.M.; Kolte, A.M.; Nielsen, H.S.; Lidegaard, Ø. Pregnancy loss and cancer risk: A nationwide observational study. Clin. Med. 2019, 15, 80–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuzhan, A.; Adli, M. The effect of socio-economic-cultural factors on breast cancer. J. Breast Health 2015, 11, 17–21. [Google Scholar] [CrossRef]
- Lee, K.; Kruper, L.; Dieli-Conwright, C.M.; Mortimer, J.E. The impact of obesity on breast cancer diagnosis and treatment. Curr. Oncol. Rep. 2019, 1, 41. [Google Scholar] [CrossRef] [Green Version]
- Dydjow-Bendek, D.; Zagozdzon, P. Selected dietary factors and breast cancer risk. Przeg Epidemiol. 2019, 73, 361–368. [Google Scholar] [CrossRef] [PubMed]
- McDonald, J.A.; Abhishek Goyal, A.; Terry, M.B. Alcohol intake and breast cancer risk: Weighing the overall evidence. Curr. Breast Cancer Rep. 2013, 5, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Preston, D.L.; Kitahara, C.M.; Freedman, D.M.; Sigurdson, A.J.; Simon, S.L.; Little, M.P.; Cahoon, E.K.; Rajaraman, P.; Miller, J.S.; Alexander, B.H.; et al. Breast cancer risk and protracted low-to-moderate dose occupational radiation exposure in the US Radiologic Technologists Cohort, 1983–2008. Br. J. Cancer 2016, 115, 1105–1112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanadys, W.; Barańska, A.; Malm, M.; Błaszczuk, A.; Polz-Dacewicz, M.; Janiszewska, J.; Jędrych, M. Use of Oral Contraceptives as a Potential Risk Factor for Breast Cancer: A Systematic Review and Meta-Analysis of Case-Control Studies Up to 2010. Int. J. Environ. Res. Public Health 2021, 18, 4638. [Google Scholar] [CrossRef]
- Charlton, B.M.; Rich-Edwards, J.W.; Colditz, G.A.; Missmer, S.A.; Rosner, B.A.; Hankinson, S.E.; Speizer, F.E.; Michels, K.B. Oral contraceptive use and mortality after 36 years of follow-up in the Nurse’ Health Study: Prospective cohort study. BMJ 2014, 349, g6356. [Google Scholar] [CrossRef] [Green Version]
- Vessey, M.; Yeates, D. Oral contraceptive use and cancer: Final report from the Oxford-Family Planning Association contraceptive study. Contraception 2013, 88, 678–683. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions; Version 6.0; John Wiley & Sons: Hoboken, NJ, USA, 2019. [Google Scholar]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Non Randomised Studies in Meta-Analyses. Available online: www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 12 March 2021).
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Begg, C.B.; Mazumdar, M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994, 50, 1088–1101. [Google Scholar] [CrossRef]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [Green Version]
- Engbang, N.J.P.; Essome, H.; Mve, K.V.; Sukam, N.D.S.; Mboudou, T.E. Risk factors for breast cancer in the city of Douala: A case control study. Adv. Breast Cancer Res. 2020, 9, 66–77. [Google Scholar] [CrossRef]
- Hamdi-Cherif, M.; Serraino, D.; Bouad, S.; Dib, A.; Boudaoud, K.; Atoui, S.; Mergherm, I.; Toffolutti, F.; Bidoli, E.; Kara, L.; et al. Sociodemographic and reproductive risk factors for breast cancer: A case-control study in the Setif Province, Northern Algeria. Asian Pac. J. Cancer Prev. 2020, 21, 457–464. [Google Scholar] [CrossRef] [PubMed]
- Alipour, S.; Omranipour, R.; Malekzadeh, R.; Poustchi, H.; Pourshams, A.; Khoshnia, M.; Gharavi, A.; Roshandel, G.; Eslami, B. A Case-control study of breast cancer in Northeast of Iran: The Golestan Cohort Study. Arch. Iran. Med. 2019, 22, 355–360. [Google Scholar]
- Alsolami, F.J.; Azzeh, F.S.; Ghafouri, K.J.; Ghaith, M.M.; Almaimani, R.A.; Almasmoum, H.A.; Abdulal, R.H.; Abdulaal, W.H.; Jazar, A.S.; Tashtoush, S.H. Determinants of breast cancer in Saudi women from Makkah region: A case-control study (breast cancer risk factors among Saudi women). BMC Public Health 2019, 19, 1554. [Google Scholar] [CrossRef] [PubMed]
- Andarieh, M.G.; Delavar, M.A.; Moslemi, D.; Ahmadi, M.H.; Zabihi, E.; Esmaeilzadeh, S. Infertility as a risk factor for breast cancer: Results from a hospital-based case-control study. J. Cancer Res. Ther. 2019, 15, 976–980. [Google Scholar] [CrossRef]
- Yuan, X.; Yi, F.; Hou, C.; Lee, H.; Zhong, X.; Tao, P.; Li, H.; Xu, Z.; Li, J. Induced abortion, birth control methods, and breast cancer risk: A case-control study in China. J. Epidemiol. 2019, 29, 173–179. [Google Scholar] [CrossRef] [Green Version]
- Bashamakha, G.; Sumait, H.B.; Bashamakha, M.; Al Serouri, A.; Khader, Y. Risk factors of breast cancer in Hadramout Valley and Desert, Yemen. Int. J. Prev. Med. 2019, 10, 161. [Google Scholar] [CrossRef] [PubMed]
- Wahidin, M.; Djuwita, R.; Adisasmita, A. Oral contraceptive and breast cancer risks: A case control study in six referral hospitals in Indonesia. Asian Pac. J. Cancer Prev. 2018, 19, 2199–2203. [Google Scholar] [CrossRef]
- Khalis, M.; Charbotel, B.; Chajès, V.; Rinaldi, S.; Moskal, A.; Biessy, C.; Dossus, L.; Huybrechts, I.; Fort, E.; Mellas, N.; et al. Menstrual and reproductive factors and risk of breast cancer: A case-control study in the Fez Region, Morocco. PLoS ONE 2018, 13, e0191333. [Google Scholar] [CrossRef]
- Sofi, N.Y.; Jain, M.; Kapil, U.; Seenu, V.R.L.; Yadav, C.P.; Pandey, R.M.; Sareen, N. Reproductive factors, nutritional status and serum 25(OH)D levels in women with breast cancer: A case control study. J. Steroid Biochem. Mol. Biol. 2018, 175, 200–204. [Google Scholar] [CrossRef]
- Tan, M.M.; Ho, W.K.; Yoon, S.Y.; Mariapun, S.; Hasan, S.N.; Lee, D.S.C.; Hassan, T.; Lee, S.Y.; Phuah, S.Y.; Sivanandan, K.; et al. A case-control study of breast cancer risk factors in 7663 women in Malaysia. PLoS ONE 2018, 13, e0203469. [Google Scholar] [CrossRef]
- Ellingjord-Dale, M.; Vos, L.; Tretli, S.; Hofvind, S.; Dos-Santos-Silva, I.; Ursin, G. Parity, hormones and breast cancer subtypes—Results from a large nested case-control study in a national screening program. Breast Cancer Res. 2017, 19, 10. [Google Scholar] [CrossRef] [Green Version]
- Balekouzou, A.; Yin, P.; Pamatika, C.M.; Bekolo, C.E.; Nambei, S.W.; Djeintote, M.; Kota, K.; Mossoro-Kpinde, C.D.; Shu, C.; Yin, M.; et al. Reproductive risk factors associated with breast cancer in women in Bangui: A case-control study. BMC Womens Health 2017, 17, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kariri, M.; Jalambo, M.O.; Kanou, B.; Deqes, S.; Younis, S.; Zabut, B.; Balawi, U. Risk factors for breast cancer in Gaza Strip, Palestine: A case-control study. Clin. Nutr. Res. 2017, 6, 161–171. [Google Scholar] [CrossRef] [Green Version]
- Dianatinasab, M.; Fararouei, M.; Mohammadianpanah, M.; Zare-Bandamiri, M.; Rezaianzadeh, A. Hair Coloring, Stress, and Smoking Increase the Risk of Breast Cancer: A Case-Control Study. Clin. Breast Cancer 2017, 17, 650–659. [Google Scholar] [CrossRef] [PubMed]
- Chollet-Hinton, L.; Olshan, A.F.; Nichols, H.B.; Anders, C.K.; Lund, J.L.; Allott, E.H.; Bethea, T.N.; Hong, C.C.; Cohen, S.M.; Khoury, T.; et al. Biology and Etiology of Young-Onset Breast Cancers among Premenopausal African American Women: Results from the AMBER Consortium. Cancer Epidemiol. Biomark. Prev. 2017, 26, 1722–1729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, J.; Le, Q.H.; Duong, B.H.; Sun, P.; Pham, H.T.; Ta, V.T.; Kotsopoulos, J.; Narod, S.A.; Ginsburg, O. A matched case-control study of risk factors for breast cancer risk in Vietnam. Int. J. Breast Cancer 2016, 2016, 1–7. [Google Scholar] [CrossRef]
- Wang, F.; Dai, J.; Li, M.; Chan, W.; Kwok, C.C.; Leung, S.; Wu, C.; Li, W.; Yu, W.; Tsang, K.-H.; et al. Risk assessment model for invasive breast cancer in Hong Kong women. Medicine 2016, 95, e4515. [Google Scholar] [CrossRef] [PubMed]
- Al-Amri, F.A.; Saeedi, M.Y.; Al-Tahan, F.M.; Ali, A.M.; Alomary, S.A.; Arafa, M.; Ibrahim, A.K.; Kassim, K.A. Breast cancer correlates in a cohort of breast screening program participants in Riyadh, KSA. J. Egypt Natl. Cancer Inst. 2015, 27, 77–82. [Google Scholar] [CrossRef] [Green Version]
- Ichida, M.; Kataoka, A.; Tsushima, R.; Taguchi, T. No increase in breast cancer risk in Japanese women taking oral contraceptives: A case-control study investigating reproductive, menstrual and familial risk factors for breast cancer. Asian Pac. J. Cancer Prev. 2015, 16, 3685–3690. [Google Scholar] [CrossRef]
- Karim, S.M.; Baeshen, W.; Neamatullah, S.N.; Bin, B. Oral contraceptives, abortion and breast cancer risk: A case control study in Saudi Arabia. Asian Pac. J. Cancer Prev. 2015, 16, 3957–3960. [Google Scholar] [CrossRef] [Green Version]
- Mohite, V.R.; Pratinidhi, A.K.; Mohite, R.V. Reproductive risk factors and breast cancer: A case control study from rural India. Bangladesh J. Med. Sci. 2015, 14, 258–264. [Google Scholar] [CrossRef] [Green Version]
- Laamiri, F.Z.; Bouayad, A.; Hasswane, N.; Ahid, S.; Mrabet, M.; Amina, B. Risk factors for breast cancer of different age groups: Moroccan Data? Open J. Obst. Gynecol. 2015, 5, 79–87. [Google Scholar] [CrossRef] [Green Version]
- Kawai, M.; Malone, K.E.; Tang, M.T.C.; Li, C.I. Active smoking and the risk of estrogen receptor-positive and triple-negative breast cancer among women ages 20 to 44 years. Cancer 2014, 120, 1026–1034. [Google Scholar] [CrossRef] [Green Version]
- Work, M.E.; John, E.M.; Andrulis, I.L.; Knight, J.A.; Liao, Y.; Mulligan, A.M.; Southey, M.C.; Giles, G.G.; Dite, G.S.; Apicella, C.; et al. Reproductive risk factors and oestrogen/progesterone receptor-negative breast cancer in the Breast Cancer Family Registry. Brit. J. Cancer 2014, 110, 1367–1377. [Google Scholar] [CrossRef] [Green Version]
- Beaber, E.F.; Malone, K.E.; Tang, M.T.; Barlow, W.E.; Porter, P.L.; Daling, J.R.; Li, C.I. Oral contraceptives and breast cancer risk overall and by molecular subtype among young women. Cancer Epidemiol. Biomark. Prev. 2014, 23, 755–764. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hosseinzadeh, M.; Eivazi Ziaei, J.; Mahdavi, N.; Aghajari, P.; Vahidi, M.; Fateh, A.; Asghari, E. Risk factors for breast cancer in Iranian women: A hospital-based case-control study in Tabriz. Iran. J. Breast Cancer 2014, 17, 236–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaisy, A.; Lotfinejad, S.; Zhian, F. Risk of cancer with combined oral contraceptive use among Iranian women. Asian Pac. J. Cancer Prev. 2014, 15, 5517–5522. [Google Scholar] [CrossRef] [PubMed]
- Pimhanam, C.; Sangrajrang, S.; Ekpanyaskul, C. Tobacco smoke exposure and breast cancer risk in Thai urban females. Asian Pac. J. Cancer Prev. 2014, 15, 7407–7411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sepandi, M.; Akrami, M.; Tabatabaee, H.; Rajaeefard, A.; Tahmasebi, S.; Angali, K.A.; Rezaianzadeh, A.; Talei, A. Breast cancer risk factors in women participating in a breast screening program: A study on 11,850 Iranian females. Asian Pac. J. Cancer Prev. 2014, 15, 8499–8502. [Google Scholar] [CrossRef] [Green Version]
- Tazhibi, M.; Dehghani, M.; Babazadeh, S.; Makkarian, F.; Tabatabaeian, M.; Sadeghi, M.; Rezaei, P.; Faghihi, M. Hormonal and reproductive risk factors associated with breast cancer in Isfahan patients. J. Educ. Health Promot. 2014, 3, 69. [Google Scholar] [CrossRef]
- Amadou, A.; Fabre, A.; Torres-Mejía, G.; Ortega-Olvera, C.; Angeles-Llerenas, A.; McKenzie, F.; Biessy, C.; Hainaut, P.; Romieu, I. Hormonal therapy and risk of breast cancer in Mexican women. PLoS ONE 2013, 8, e79695. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morales, L.; Alvarez-Garriga, C.; Matta, J.; Ortiz, C.; Vergne, Y.; Vargas, W.; Acosta, H.; Ramírez, J.; Perez-Mayoral, J.; Bayona, M.; et al. Factors associated with breast cancer in Puerto Rican women. J. Epidemiol. Glob. Health 2013, 3, 205–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ehsanpour, S.; Nejad, F.S.; Rajabi, F.M.; Taleghani, F. Investigation on the association between breast cancer and consumption patterns of combined oral contraceptive pills in the women of Isfahan in Iranian. Iran. J. Nurs. Midwifery Res. 2013, 18, 186–190. [Google Scholar] [PubMed]
- Urban, M.; Banks, E.; Egger, S.; Canfell, K.; O’Connell, D.; Beral, V.; Sitas, F. Injectable and oral contraceptive use and cancers of the breast, cervix, ovary, and endometrium in black South African women: Case-control study. PLoS Med. 2012, 9, e1001182. [Google Scholar] [CrossRef]
- Ronco, A.L.; De Stefani, E.; Deneo-Pellegrini, H. Risk factors for premenopausal breast cancer: A case-control study in Uruguay. Asian Pac. J. Cancer Prev. 2012, 13, 2879–2886. [Google Scholar] [CrossRef] [Green Version]
- Matalqah, L.; Radaideh, K.; Yusoff, Z.M.; Awaisu, A. Predictors of breast cancer among women in a northern state of Malaysia: A matched case-control study. Asian Pac. J. Cancer Prev. 2011, 12, 1549–1553. [Google Scholar]
- Ghiasvand, R.; Maram, E.S.; Tahmasebi, S.; Tabatabaee, S.H.R. Risk factor for breast cancer among young women in Southern Iran. Int. J. Cancer 2011, 129, 1443–1449. [Google Scholar] [CrossRef]
- Ekpanyaskul, C.; Khuhaprema, T.; Wiangnon, S.; Sangrajrang, S. Case-control study of occupational categories and breast cancer risk in Thailand. Asian Pac. J. Cancer Prev. 2010, 11, 793–797. [Google Scholar]
- Ma, H.; Wang, Y.; Sullivan-Halley, J.; Linda Weiss, L.; Marchbanks, P.A.; Spirtas, R.; Ursin, G.; Burkman, R.T.; Simon, M.S.; Malone, K.E.; et al. Use of four biomarkers to evaluate the risk of breast cancer subtypes in the Women's Contraceptive and Reproductive Experiences Study. Cancer Res. 2010, 70, 575–587. [Google Scholar] [CrossRef] [Green Version]
- Hadjisavvas, A.; Loizidou, M.A.; Middleton, N.; Michael, T.; Papachristoforou, R.; Kakouri, E.; Daniel, M.; Papadopoulos, P.; Malas, S.; Marcou, Y.; et al. An investigation of breast cancer risk factors in Cyprus: A case control study. BMC Cancer 2010, 10, 447. [Google Scholar] [CrossRef] [Green Version]
- Ozmen, V.; Ozcinar, B.; Karanlik, H.; Cabioglu, N.; Tukenmez, M.; Disci, R.; Ozmen, T.; Igci, A.; Muslumanoglu, M.; Kecer, M.; et al. Breast cancer risk factors in Turkish women—A University Hospital based nested case control study. World J. Surg. Oncol. 2009, 7, 37. [Google Scholar] [CrossRef] [Green Version]
- Busund, M.; Bugge, N.S.; Braaten, T.; Waaseth, M.; Rylander, C.; Lund, E. Progestin-only and combined oral contraceptives and receptor-defined premenopausal breast cancer risk: The Norwegian Women and Cancer Study. Int. J. Cancer 2018, 142, 2293–2302. [Google Scholar] [CrossRef] [PubMed]
- Mørch, L.S.; Skovlund, C.W.; Hannaford, P.C.; Iversen, L.; Fielding, S.; Lidegaard, Ø. Contemporary hormonal contraception and the risk of breast cancer. N. Engl. J. Med. 2017, 377, 2228–2239. [Google Scholar] [CrossRef]
- Iversen, L.; Sivasubramaniam, S.; Lee, A.J.; Fielding, S.; Hannafordet, P.C. Lifetime cancer risk and combined oral contraceptives: The Royal College of General Practitioners’ Oral Contraception Study. Am. J. Obstet. Gynecol. 2017, 216, 580. [Google Scholar] [CrossRef] [PubMed]
- Gierisch, J.M.; Coeytaux, R.R.; Urrutia, R.P.; Havrilesky, L.J.; Moorman, P.G.; Lowery, W.J.; Dinan, M.; McBroom, A.J.; Hasselblad, V.; Sanders, G.D.; et al. Oral contraceptive use and risk of breast, cervical, colorectal, and endometrial cancers: A systematic review. Cancer Epidemiol. Biomark. Prev. 2013, 22, 1931–1943. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, H.; Lei, X.; Feng, J.; Wang, Y. Oral contraceptive use and risk of breast cancer: A meta-analysis of prospective cohort studies. Eur. J. Contracept. Reprod. Health Care 2012, 17, 402–414. [Google Scholar] [CrossRef] [PubMed]
- Del Pup, L.; Codacci-Pisanelli, G.; Peccatori, F. Breast cancer risk of hormonal contraception: Counselling considering new evidence. Crit. Rev. Oncol. Hematol. 2019, 137, 123–130. [Google Scholar] [CrossRef] [PubMed]
- Tamimi, R.M.; Spiegelman, D.; Smith-Warner, S.A.; Wang, M.; Pazaris, M.; Willett, W.C.; Eliassen, A.H.; Hunter, D.J. Population Attributable Risk of Modifiable and Nonmodifiable Breast Cancer Risk Factors in Postmenopausal Breast Cancer. Am. J. Epidemiol. 2016, 184, 884–893. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, B.; Venet, D.; Lambertini, M.; Desmedt, C.; Salgado, R.; Horlings, H.M.; Rothé, F.; Sotiriou, C. Imprint of parity and age at first pregnancy on the genomic landscape of subsequent breast cancer. Breast Cancer Res. 2019, 21, 25. [Google Scholar] [CrossRef] [Green Version]
- Unar-Munguía, M.; Torres-Mejía, G.; Arantxa Colchero, M.; González de Cosío, T. Breastfeeding mode and risk of breast cancer: A dose-response meta-analysis. J. Hum. Lact. 2017, 33, 422–434. [Google Scholar] [CrossRef] [PubMed]
- Amadou, A.; Hainaut, P.; Romieu, I. Role of obesity in the risk of breast cancer: Lessons from anthropometry. J. Oncol. 2013, 2013, 906495. [Google Scholar] [CrossRef] [PubMed]
- Duan, W.; Li, S.; Meng, X.; Sun, Y.; Jia, C. Smoking and survival of breast cancer patients: A meta-analysis of cohort studies. Breast 2017, 33, 117–124. [Google Scholar] [CrossRef]
- Grabrick, D.M.; Hartmann, L.C.; Cerhan, J.R.; Vierkant, R.A.; Therneau, T.M.; Vachon, C.M.; Olson, F.J.; Couch, F.J.; Anderson, K.E.; Pankratz, V.S.; et al. Risk of breast cancer with oral contraceptive use in women with a family history of breast cancer. JAMA 2000, 284, 1791–1798. [Google Scholar] [CrossRef] [Green Version]
- Petitti, D. Meta-Analysis, Decision, Analysis, and Cost-Effectiveness Analysis; Oxford University Press: New York, NY, USA, 2000. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| First Autor Pub Year (References) | Region | Recruitment (Year) | Number of Case Subjects (%) | Age (Mean ± SD or Range) | Number of Controls Subjects (%) | Source of Subjects | NOS Score |
|---|---|---|---|---|---|---|---|
| Engbang 2020 [26] | Duala; Cameroon | 2012–2018 | 297 (50.5) | 53.3 ± 12.7 | 1158 (36.7) | Hospital | 8 |
| Hamdi-Cherif 2020 [27] | Setif; Algeria | 2012–2017 | 547 (63.1) | 28–77 | 543 (59.1) | Hospital | 4 |
| Alipour 2019 [28] | Golestan; Iran | 2004–2008 | 99 (34.3) | 40–75 | 400 (33.2) | Population | 8 |
| Alsolami 2019 [29] | Mahhah; Saudi Arabia | 2014–2016 | 214 (43.9) | 57.0 ± 7.3 | 218 (25.2) | Population | 5 |
| Andarieh 2019 [30] | Babolsar; Iran | 2014–2016 | 1177 (58.5) | 48.8 ± 8.5 | 1204 (27.3) | Hospital | 7 |
| Yuan 2019 [31] | Chengdu; China | 2014–2015 | 448 (19.2) | 43.7 ± 6.1 | 463 (10.6) | Clinic | 5 |
| Bashamakha 2019 [32] | Seiyun; Yemen | 2011–2015 | 105 (49.5) | N/A | 210 (55.2) | Population | 6 |
| Wahidin 2018 [33] | Jakarta; Indonesia | 2018 | 381 (35.4) | 40–49 | 381 (20.2) | Hospital | 4 |
| Khalis 2018 [34] | Fez; Morocco | 2014–2015 | 237 (62.2) | 45–54 | 237 (61.2) | Hospital | 6 |
| Sofi 2018 [35] | New Delhi; India | 2015–2017 | 195 (12.3) | 45.0 ± 10.0 | 191 (25.1) | Hospital | 7 |
| Tan 2018 [36] | Malaysia | 2002–2016 | 3387 (27.6) | 58.0 | 3951 (29.0) | Hospital | 4 |
| Ellingjord-Dale 2017 [37] | Norway | 2006–2014 | 5050 (51.6) | 50–69 | 24,343 (50.7) | Population | 8 |
| Balekouzou 2017 [38] | Central African Republic | 2003–2015 | 174 (28.9) | 45.8 ± 13.6 | 348 (41.1) | Population | 6 |
| Kariri 2017 [39] | Gaza Strip; Palestine | 2014–2015 | 96 (28.1) | 18–60 | 197 (28.9) | Hospital | 7 |
| Dianatinasab 2017 [40] | Shiraz; Iran | 2014–2016 | 526 (46.8) | <40–60> | 562 (40.7) | Hospital | 7 |
| Chollet-Hinton 2017 [41] | USA | 2005 | 1589 (80.7) | 22–75 | 5137 (86.1) | Community | 7 |
| Nguyen 2016 [42] | Hanoi; Wietnam | 2007–2013 | 291 (8.6) | 24–65 | 291 (4.5) | Hospital | 7 |
| Wang 2016 [43] | Hong Kong SAR | 2011–2015 | 923 (32.6) | 56.0 ± 11.8 | 918 (36.3) | Hospital | 6 |
| Al-Amri 2015 [44] | Riyadh; Saudi Arabia | 2013–2014 | 58 (62.1) | 30–69 | 290 (73.8) | Hospital | 6 |
| Ichida 2015 [45] | Tokyo; Japan | 2007–2013 | 155 (23.2) | 20–69 | 12,223 (26.8 | Clinic | 6 |
| Karim 2015 [46] | Jeddah; Saudi Arabia | 2001–2013 | 92 (58.7) | 30–65 | 100 (67.0) | Clinic | 4 |
| Mohite 2015 [47] | Satara district, India | 2009–2011 | 217 (31.8) | 40–49 | 217 (22.1) | Hospital | 4 |
| Laamiri 2015 [48] | Rabat; Morocco | 2008–2010 | 400 (74.5) | 45.8 ± 11.1 | 400 (76.0) | Hospital | 5 |
| Kawai 2014 [49] | USA | 2004–2010 | 960 (88.9) | 20–44 | 938 (89.1) | Population | 6 |
| Work 2014 [50] | USA, Canada, Australia | 1995–2004 | 4011 (72.9) | 18–69 | 2997 (77.8) | Community | 6 |
| Beaber 2014 [51] | USA | 2004–2010 | 985 (87.9) | 20–44 | 882 (88.3) | Population | 7 |
| Hosseinzadeh 2014 [52] | Tabriz; Iran | 2012–2013 | 140 (69.3) | 47.6 ± 10.7 | 280 (38.6) | Clinic | 4 |
| Vaisy 2014 [53] | Urmia; Iran | 2013–2014 | 228 (72.4) | 47.63 | 216 (57.4) | Clinic | 5 |
| Pimhanam 2014 [54] | Bangkok; Thailand | 2007–2011 | 444 (45.9) | 45.8 ± 10.1 | 444 (38.7) | Hospital | 4 |
| Sepandi 2014 [55] | Shiraz; Iran | 2001–2012 | 197 (57.9) | 26–68 | 11,653 (55.8) | Hospital | 4 |
| Tazhibi 2014 [56] | Isfahan; Iran | 1999–2010 | 216 (63.9) | 20–75 | 41 (75.6) | Hospital | 5 |
| Amadou 2014 [57] | Mexico | 2004–2007 | 263 (17.9) | 35–64 | 314 (19.4) | Hospital | 6 |
| Morales 2013 [58] | Puerto Rico | 2005–2009 | 462 (48.5) | 56.4 ± 12.6 | 649 (55.0) | Hospital | 6 |
| Ehsanpour 2013 [59] | Isfahan; Iran | 2011 | 175 (43.4) | <41–60+ | 350 (25.4) | Clinic | 5 |
| Urban 2012 [60] | South Africa | 1995–2006 | 1112 (23.0) | 49.0 | 1102 (14.2) | Hospital | 4 |
| Ronco 2012 [61] | Montevideo; Uruguay | 2004–2010 | 251 (69.7) | <30–50≥ | 497 (65.2) | Hospital | 8 |
| Matalqah 2011 [62] | Penang, Malaysia | 2009–2010 | 150 (26.7) | 52.8 ± 1.1 | 150 (18.0) | Population | 7 |
| Ghiasvand 2011 [63] | Shiraz; Iran | 2005–2008 | 442 (66.3) | 41.2 ± 5.7 | 463 (62.9) | Hospital | 5 |
| Ekpanyaskul 2010 [64] | Khon Kaen, Thailand | 2002–2004 | 516 (42.0) | 46.9 ± 10.6 | 516 (34.9) | Hospital | 6 |
| Ma 2010 [65] | USA | 1994–1998 | 1197 (78.8) | 36–64 | 2015 (79.6) | Community | 8 |
| Hahjisavvas 2010 [66] | Cyprus | 1999–2005 | 1103 (25.4) | 50–59 | 1173 (25.1) | Hospital | 7 |
| Ozmen 2009 [67] | Istanbul, Turkey | 2000–2006 | 1492 (18.4) | 18–70 | 2167 (27.8) | Hospital | 7 |
| Variables | Studies, N (Ref.) | OR (95% CI) | p | I2 (%) |
|---|---|---|---|---|
| Taking OC | ||||
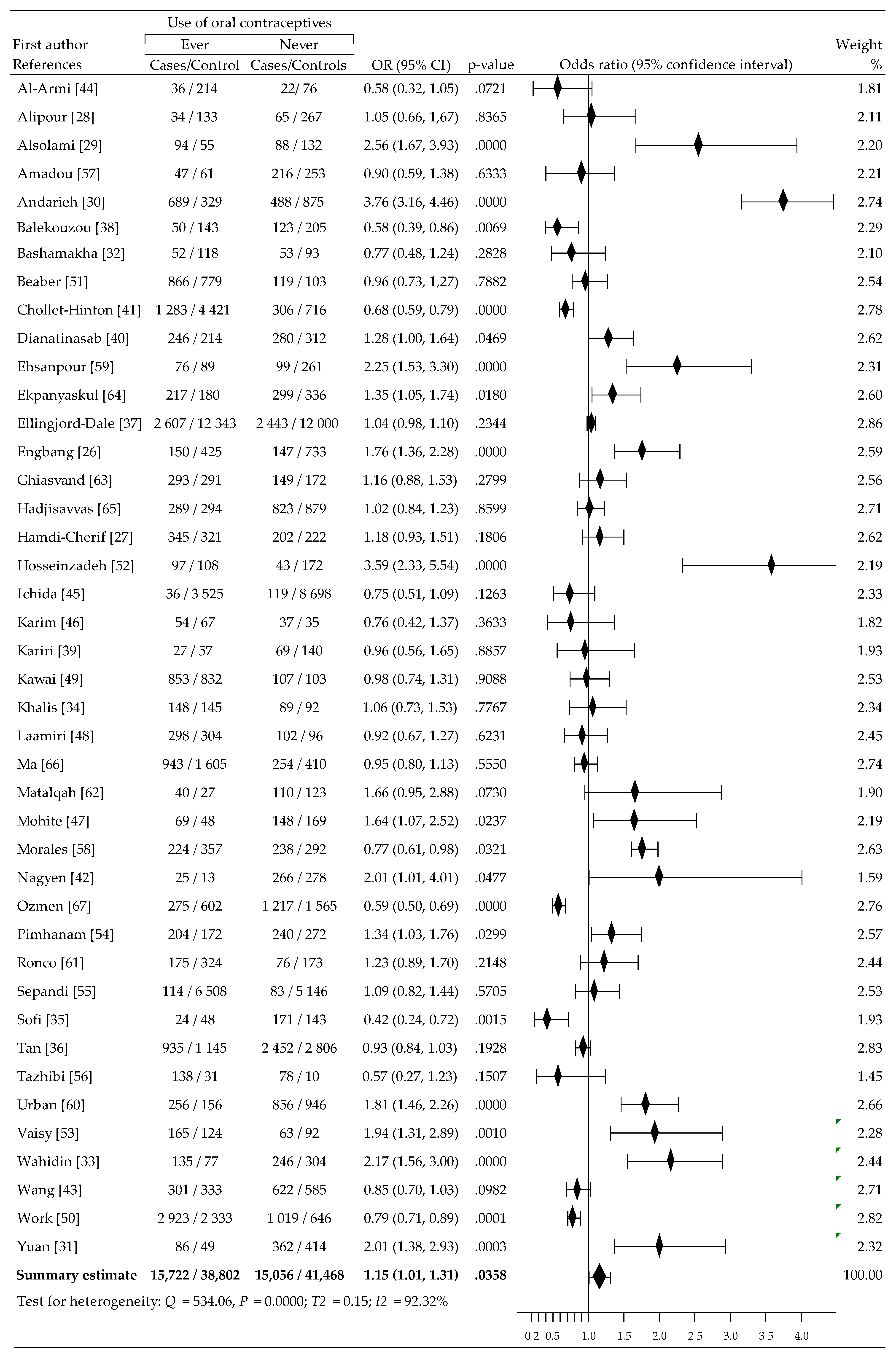
| ever vs. never | 42 [26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67] | 1.15 (1.01, 1.31) | 0.0358 | 92.32 |
| The period of OC using | ||||
| ≤5 years | 13 [28,33,37,38,41,48,49,50,51,53,59,62,66] | 0.92 (0.77, 1.10) | 0.3674 | 85.86 |
| >5 years | 1.05 (0.88, 1.25) | 0.5787 | 82.95 | |
| Age of menarche | ||||
| ≤12 years vs. >12 years | 29 [26,27,30,32,33,34,35,36,37,38,39,41,43,44,47,48,49,50,51,52,54,55,56,57,58,61,62,64,66] | 1.18 (1.07, 1.31) | 0.0016 | 80.71 |
| Parity | ||||
| Nulliparous vs. Parous | 30 [26,27,30,34,35,36,37,38,39,41,42,43,45,47,48,49,50,51,52,54,55,56,57,58,61,62,63,65,66,67] | 1.22 (1.04, 1.43) | 0.0146 | 89.88 |
| Age at first pregnancy | ||||
| ≥25 years vs. <25 years | 14 [27,35,36,37,39,41,43,49,51,55,62,63,66,67] | 1.09 (0.94, 1.25) | 0.2599 | 86.64 |
| ≥30 years vs. <30 years | 6 [26,48,52,58,64,65] | 3.08 (1.10, 8.60) | 0.0322 | 97.49 |
| Breastfeeding | ||||
| No vs. Yes | 27 [26,29,30,32,33,36,37,38,39,41,43,44,45,46,47,48,50,51,52,54,58,61,62,64,65,66,67] | 1.36 (1.13, 1.63) | 0.0010 | 91.81 |
| Menopausal status | ||||
| Post- vs. Pre- | 22 [26,32,34,35,36,37,39,42,43,44,45,46,47,48,50,52,54,55,58,62,63,64] | 1.36 (1.14, 1.63) | 0.0007 | 92.86 |
| Family history of BrCa | ||||
| Yes vs. No | 29 [27,28,29,30,32,33,34,35,37,39,41,43,44,45,46,48,49,50,51,52,54,55,57,58,61,63,64,66,67] | 1.72 (1.32, 2.24) | 0.0001 | 93.07 |
| Body mass index (kg/m2) | ||||
| ≥30 (obesitas) vs. <30 | 16 [26,27,28,29,32,34,39,41,44,49,51,54,55,57,63,66] | 1.19 (0.95, 1.5) | 0.1289 | 90.46 |
| Tobacco smoking | ||||
| Yes vs. No | 14 [26,28,29,30,36,42,49,52,54,58,62,64,66,67] | 1.52 (1.26, 1.83) | 0.0000 | 72.32 |
| Diabetes | ||||
| Yes vs. No | 4 [26,29,32,39] | 1.99 (0.60, 6.62) | 0.2605 | 93.49 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barańska, A.; Błaszczuk, A.; Kanadys, W.; Malm, M.; Drop, K.; Polz-Dacewicz, M. Oral Contraceptive Use and Breast Cancer Risk Assessment: A Systematic Review and Meta-Analysis of Case-Control Studies, 2009–2020. Cancers 2021, 13, 5654. https://doi.org/10.3390/cancers13225654
Barańska A, Błaszczuk A, Kanadys W, Malm M, Drop K, Polz-Dacewicz M. Oral Contraceptive Use and Breast Cancer Risk Assessment: A Systematic Review and Meta-Analysis of Case-Control Studies, 2009–2020. Cancers. 2021; 13(22):5654. https://doi.org/10.3390/cancers13225654
Chicago/Turabian StyleBarańska, Agnieszka, Agata Błaszczuk, Wiesław Kanadys, Maria Malm, Katarzyna Drop, and Małgorzata Polz-Dacewicz. 2021. "Oral Contraceptive Use and Breast Cancer Risk Assessment: A Systematic Review and Meta-Analysis of Case-Control Studies, 2009–2020" Cancers 13, no. 22: 5654. https://doi.org/10.3390/cancers13225654
APA StyleBarańska, A., Błaszczuk, A., Kanadys, W., Malm, M., Drop, K., & Polz-Dacewicz, M. (2021). Oral Contraceptive Use and Breast Cancer Risk Assessment: A Systematic Review and Meta-Analysis of Case-Control Studies, 2009–2020. Cancers, 13(22), 5654. https://doi.org/10.3390/cancers13225654