
Clinicopathological Determinants of Recurrence Risk and Survival in Mucinous Ovarian Carcinoma

 , ,
, ,  ,
,  and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
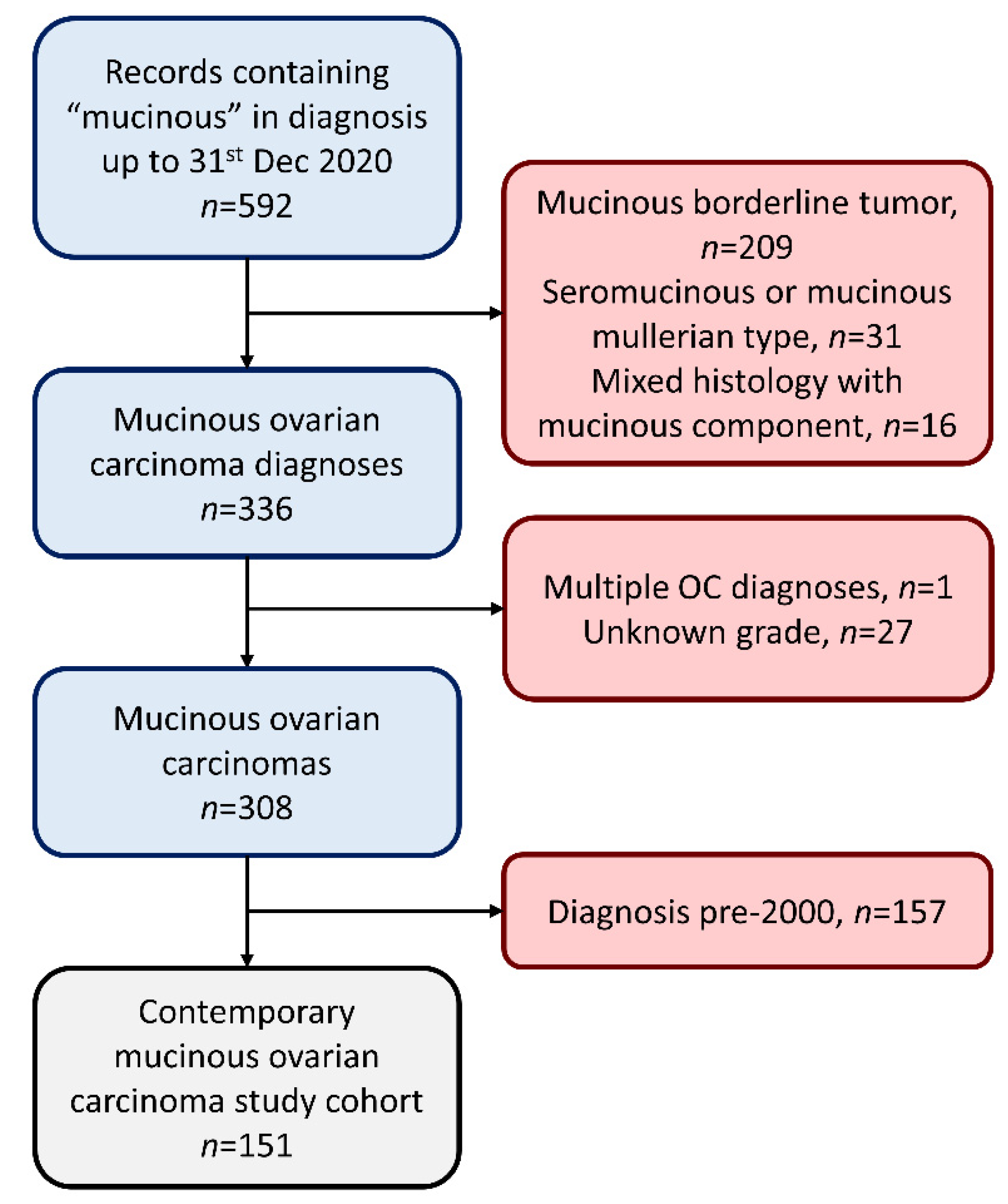
2.1. Cohort Identification
2.2. Survival Analysis
2.3. Additional Statistical Analysis
3. Results
3.1. Cohort Characteristics
3.2. First-Line Treatment
3.3. Likelihood of Relapse following 2 and 5 Year Disease-Free Milestones
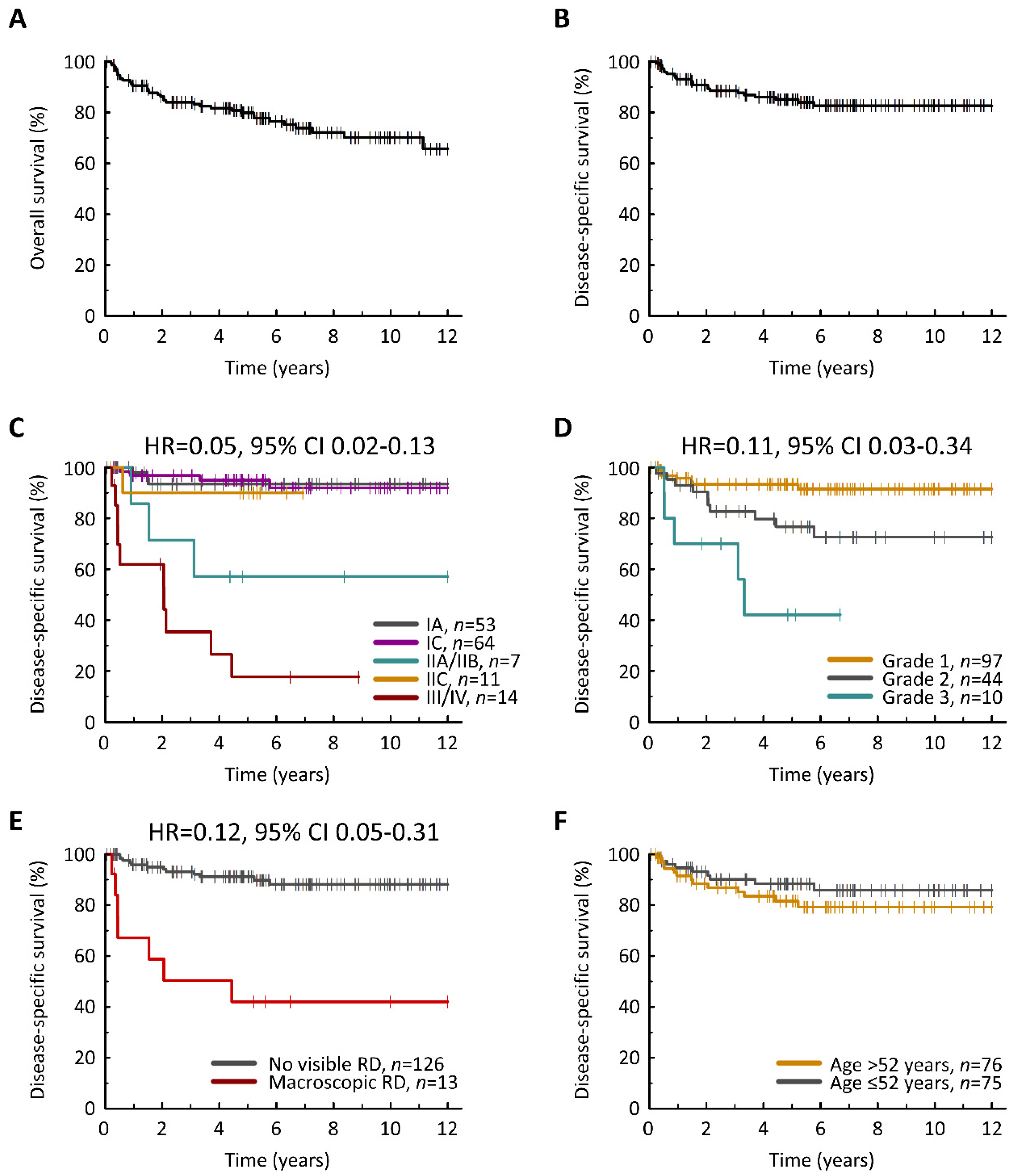
3.4. Clinical Determinants of Survival Outcome
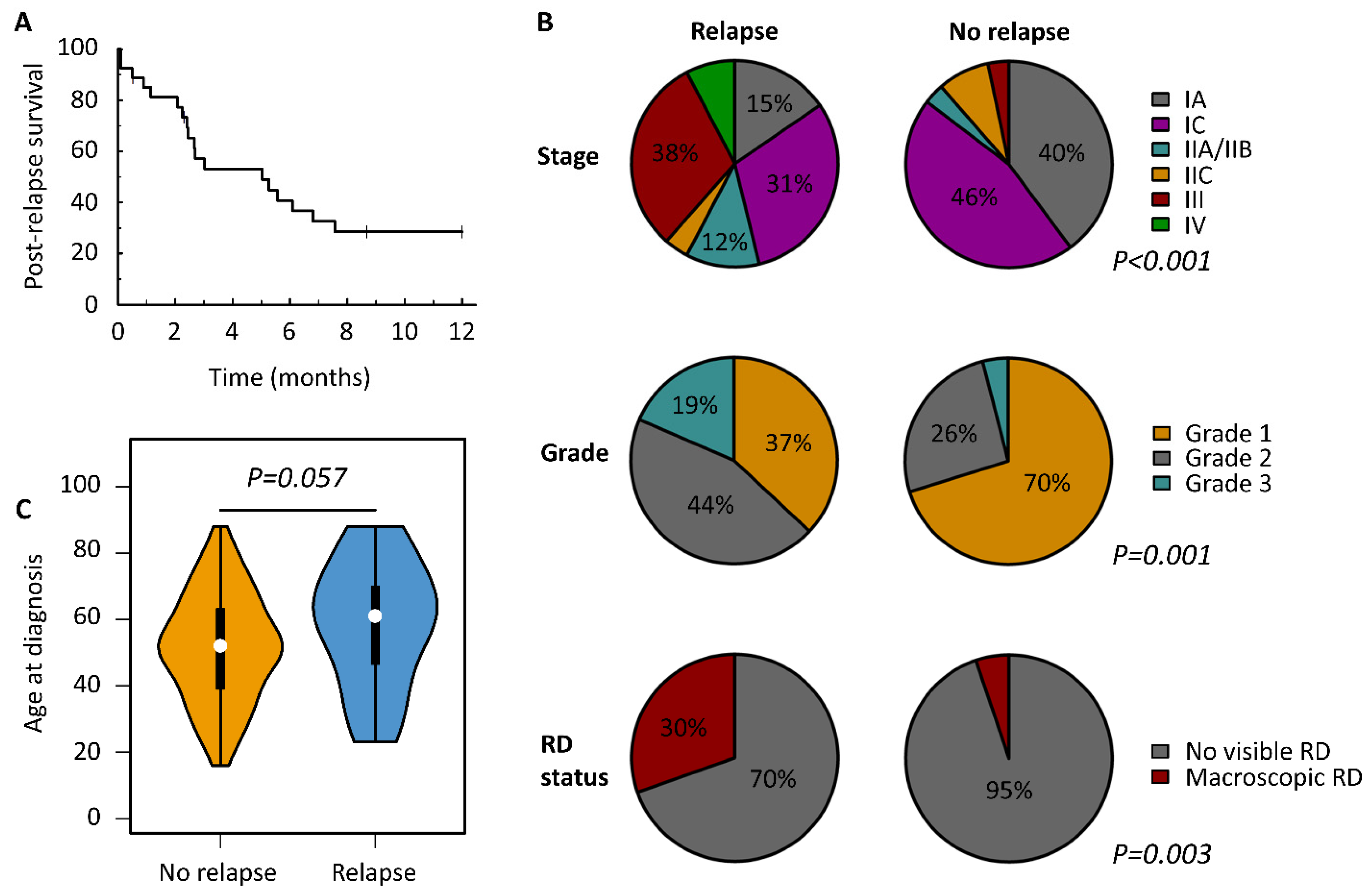
3.5. Characteristics of Relapsed MOC
3.6. Outcome in Low-Risk Mucinous Ovarian Carcinoma
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Cheasley, D.; Wakefield, M.J.; Ryland, G.L.; Allan, P.E.; Alsop, K.; Amarasinghe, K.C.; Ananda, S.; Anglesio, M.S.; Au-Yeung, G.; Böhm, M.; et al. The molecular origin and taxonomy of mucinous ovarian carcinoma. Nat. Commun. 2019, 10, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Peres, L.C.; Cushing-Haugen, K.L.; Köbel, M.; Harris, H.R.; Berchuck, A.; Rossing, M.A.; Schildkraut, J.M.; Doherty, J.A. Invasive Epithelial Ovarian Cancer Survival by Histotype and Disease Stage. J. Natl. Cancer Inst. 2018, 111, 60–68. [Google Scholar] [CrossRef]
- Morice, P.; Gouy, S.; Leary, A. Mucinous Ovarian Carcinoma. N. Engl. J. Med. 2019, 380, 1256–1266. [Google Scholar] [CrossRef] [PubMed]
- McGuire, V.; Jesser, C.A.; Whittemore, A.S. Survival among U.S. Women with Invasive Epithelial Ovarian Cancer. Gynecol. Oncol. 2002, 84, 399–403. [Google Scholar] [CrossRef] [PubMed]
- Zaino, R.J.; Brady, M.F.; Lele, S.M.; Michael, H.; Greer, B.; Bookman, M.A. Advanced stage mucinous adenocarcinoma of the ovary is both rare and highly lethal: A Gynecologic Oncology Group study. Cancer 2011, 117, 554–562. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seidman, J.D.; Kurman, R.J.; Ronnett, B.M. Primary and metastatic mucinous adenocarcinomas in the ovaries: Incidence in routine practice with a new approach to improve intraoperative diagnosis. Am. J. Surg. Pathol. 2003, 27, 985–993. [Google Scholar] [CrossRef]
- Perren, T.J. Mucinous epithelial ovarian carcinoma. Ann. Oncol. 2016, 27 (Suppl. S1), i53–i57. [Google Scholar] [CrossRef] [PubMed]
- Irodi, A.; Rye, T.; Herbert, K.; Churchman, M.; Bartos, C.; Mackean, M.; Nussey, F.; Herrington, C.S.; Gourley, C.; Hollis, R.L. Patterns of clinicopathological features and out-come in epithelial ovarian cancer patients: 35 years of prospectively collected data. BJOG Int. J. Obstet. Gynaecol. 2020, 127, 1409–1420. [Google Scholar] [CrossRef] [Green Version]
- Nasioudis, D.; Haggerty, A.F.; Giuntoli, R.L., 2nd; Burger, R.A.; Morgan, M.A.; Ko, E.M.; Latif, N.A. Adjuvant chemotherapy is not associated with a survival benefit for patients with early stage mucinous ovarian carcinoma. Gynecol. Oncol. 2019, 154, 302–307. [Google Scholar] [CrossRef]
- Ledermann, J.A.; Luvero, D.; Shafer, A.; O’Connor, D.; Mangili, G.; Friedlander, M.; Pfisterer, J.; Mirza, M.R.; Kim, J.-W.; Alexandre, J.; et al. Gynecologic Cancer InterGroup (GCIG) consensus review for mucinous ovarian carcinoma. Int. J. Gynecol. Cancer 2014, 24, S14–S19. [Google Scholar] [CrossRef] [PubMed]
- Bamias, A.; Psaltopoulou, T.; Sotiropoulou, M.; Haidopoulos, D.; Lianos, E.; Bournakis, E.; Papadimitriou, C.; Rodolakis, A.; Vlahos, G.; Dimopoulos, M.A. Mucinous but not clear cell histology is associated with inferior survival in patients with advanced stage ovarian carcinoma treated with plati-num-paclitaxel chemotherapy. Cancer 2010, 116, 1462–1468. [Google Scholar] [CrossRef] [PubMed]
- Hess, V.; A’hern, R.; Nasiri, N.; King, D.M.; Blake, P.R.; Barton, D.P.; Shepherd, J.H.; Ind, R.; Bridges, J.; Harrington, K.; et al. Mucinous epithelial ovarian cancer: A separate entity requiring specific treatment. J. Clin. Oncol. 2004, 22, 1040–1044. [Google Scholar] [CrossRef] [PubMed]
- Pectasides, D.; Fountzilas, G.; Aravantinos, G.; Kalofonos, H.P.; Efstathiou, E.; Salamalekis, E.; Farmakis, D.; Skarlos, D.; Briasoulis, E.; Economopoulos, T.; et al. Advanced stage mucinous epithelial ovarian cancer: The Hellenic Cooperative Oncology Group experience. Gynecol. Oncol. 2005, 97, 436–441. [Google Scholar] [CrossRef] [PubMed]
- Pisano, C.; Greggi, S.; Tambaro, R.; Losito, S.; Iodice, F.; Di Maio, M.; Ferrari, E.; Falanga, M.; Formato, R.; Iaffaioli, V.R.; et al. Activity of chemotherapy in mucinous epithelial ovarian cancer: A retrospective study. Anticancer. Res. 2005, 25, 3501–3505. [Google Scholar]
- Gore, M.; Hackshaw, A.; Brady, W.E.; Penson, R.T.; Zaino, R.; McCluggage, W.G.; Ganesan, R.; Wilkinson, N.; Perren, T.; Montes, A.; et al. An international, phase III randomized trial in patients with mucinous epithelial ovarian cancer (mEOC/GOG 0241) with long-term follow-up: And experience of conducting a clinical trial in a rare gynecological tumor. Gynecol. Oncol. 2019, 153, 541–548. [Google Scholar] [CrossRef] [Green Version]
- Therneau, T. A Package for Survival Analysis in R. R Package Version 3.2-10. 2021. Available online: https://CRAN.R-project.org/package=survival (accessed on 16 March 2021).
- Wu, S.-G.; Wang, J.; Sun, J.-Y.; He, Z.-Y.; Zhang, W.-W.; Zhou, J. Real-World Impact of Survival by Period of Diagnosis in Epithelial Ovarian Cancer Between 1990 and 2014. Front. Oncol. 2019, 9, 639. [Google Scholar] [CrossRef] [Green Version]
- Mueller, J.J.; Lajer, H.; Mosgaard, B.J.; Bach Hamba, S.; Morice, P.; Gouy, S.; Hussein, Y.; Soslow, R.A.; Schlappe, B.A.; Zhou, Q.C.; et al. International Study of Primary Mucinous Ovarian Carcinomas Managed at Tertiary Medical Centers. Int. J. Gynecol. Cancer 2018, 28, 915–924. [Google Scholar] [CrossRef] [Green Version]
- Zhou, J.; Wu, S.G.; Wang, J.; Sun, J.Y.; He, Z.Y.; Jin, X.; Zhang, W.W. The Effect of Histological Subtypes on Outcomes of Stage IV Epitheli-al Ovarian Cancer. Front. Oncol. 2018, 8, 577. [Google Scholar] [CrossRef]
- Matsuo, K.; Huang, Y.; Zivanovic, O.; Shimada, M.; Machida, H.; Grubbs, B.H.; Roman, L.D.; Wright, J.D. Effectiveness of postoperative chemotherapy for stage IC mucinous ovarian cancer. Gynecol. Oncol. 2019, 154, 505–515. [Google Scholar] [CrossRef]
- Zacharakis, M.; Xynos, I.D.; Lazaris, A.; Smaro, T.; Kosmas, C.; Dokou, A.; Felekouras, E.; Antoniou, E.; Polyzos, A.; Sarantonis, J.; et al. Predictors of survival in stage IV metastatic colorectal cancer. Anticancer. Res. 2010, 30, 653–660. [Google Scholar]
- Ledermann, J.A.; Harter, P.; Gourley, C.; Friedlander, M.; Vergote, I.; Rustin, G.; Scott, C.; Meier, W.; Shapira-Frommer, R.; Safra, T.; et al. Overall survival in patients with platinum-sensitive recurrent serous ovarian cancer receiving olaparib maintenance monotherapy: An updated analysis from a randomised, placebo-controlled, double-blind, phase 2 trial. Lancet Oncol. 2016, 17, 1579–1589. [Google Scholar] [CrossRef]
- Pujade-Lauraine, E.; Hilpert, F.; Weber, B.; Reuss, A.; Poveda, A.; Kristensen, G.; Sorio, R.; Vergote, I.; Witteveen, P.; Bamias, A.; et al. Bevacizumab Combined with Chemotherapy for Platinum-Resistant Recurrent Ovarian Cancer: The AURELIA Open-Label Randomized Phase III Trial. J. Clin. Oncol. 2014, 32, 1302–1308. [Google Scholar] [CrossRef]
- Gershenson, D.M.; Sun, C.C.; Bodurka, D.; Coleman, R.L.; Lu, K.H.; Sood, A.K.; Deavers, M.; Malpica, A.L.; Kavanagh, J.J. Recurrent low-grade serous ovarian carcinoma is relatively chemoresistant. Gynecol. Oncol. 2009, 114, 48–52. [Google Scholar] [CrossRef] [PubMed]
- Billingham, L.; Malottki, K.; Steven, N. Research methods to change clinical practice for patients with rare cancers. Lancet Oncol. 2016, 17, e70–e80. [Google Scholar] [CrossRef]
- McCluggage, W.G. Immunohistochemistry in the distinction between primary and metastatic ovarian mucinous neo-plasms. J. Clin. Pathol. 2012, 65, 596–600. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| N | % | ||
|---|---|---|---|
| Total cases | N | 151 | |
| Age at diagnosis | Median years | 52 | range 16–88 |
| Year of diagnosis | 2000–2004 | 33 | 21.9 |
| 2005–2009 | 39 | 25.8 | |
| 2010–2014 | 45 | 29.8 | |
| 2015 onwards | 34 | 22.5 | |
| Pathological grade a | Grade 1 | 97 b | 64.2 |
| Grade 2 | 44 | 29.1 | |
| Grade 3 | 10 c | 6.6 | |
| FIGO stage at diagnosis d | IA | 53 | 35.6 |
| IC | 64 e | 43 | |
| IIA | 1 | 0.7 | |
| IIB | 6 | 4 | |
| IIC | 11 | 7.4 | |
| III | 12 f | 8.1 | |
| IV | 2 | 1.3 | |
| NA | 2 | - | |
| RD following first-line debulking | No visible RD | 126 | 90.6 |
| Macroscopic RD | 13 g | 9.4 | |
| NA | 12 | - | |
| First-line treatment regime | PDS only | 90 | 59.6 |
| PDS + carboplatin | 27 | 17.9 | |
| PDS + carboplatin-paclitaxel | 27 | 17.9 | |
| PDS + other platinum-containing combination | 4 h | 2.6 | |
| PDS + capecitabine | 1 | 0.7 | |
| Neoadjuvant carboplatin-paclitaxel | 1 i | 0.7 | |
| None | 1 j | 0.7 | |
| Status at last follow-up | No known active disease | 124 | 82.1 |
| Relapsed/progressed | 27 | 17.9 | |
| Vital status at last follow-up | Alive | 115 | 76.2 |
| Deceased—died of OC | 22 | 14.6 | |
| Deceased—other causes | 14 | 9.3 | |
| Median follow-up time | Years | 5.73 k | 95% CI 5.21–6.78 |
| Disease-Specific Survival | Progression-Free Survival | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Univariable Analysis | Multivariable Analysis | Univariable Analysis | Multivariable Analysis | ||||||||||
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | HR | 95% CI | p-Value | HR | 95% CI | p-Value | ||
| FIGO stage at diagnosis | IA | 0.05 | 0.01–0.18 | <0.0001 | 0.02 | 0.00–0.18 | <0.001 | 0.06 | 0.02–0.19 | <0.0001 | 0.04 | 0.01–0.23 | <0.001 |
| IC | 0.05 | 0.02–0.15 | <0.0001 | 0.07 | 0.02–0.30 | <0.001 | 0.09 | 0.04–0.23 | <0.0001 | 0.14 | 0.04–0.48 | 0.002 | |
| IIA/B | 0.37 | 0.10–1.35 | 0.132 | 0.33 | 0.07–1.50 | 0.150 | 0.36 | 0.10–1.31 | 0.121 | 0.37 | 0.09–1.62 | 0.187 | |
| IIC | 0.08 | 0.01–0.60 | 0.014 | 0.24 | 0.03–2.19 | 0.205 | 0.08 | 0.01–0.64 | 0.017 | 0.23 | 0.03–1.99 | 0.181 | |
| III/IV | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | |
| Pathological grade | Grade 1 | 0.11 | 0.03–0.34 | <0.001 | 0.05 | 0.01–0.22 | <0.001 | 0.14 | 0.05–0.41 | <0.001 | 0.08 | 0.02–0.31 | <0.001 |
| Grade 2 | 0.35 | 0.12–1.02 | 0.055 | 0.15 | 0.04–0.65 | 0.011 | 0.39 | 0.14–1.11 | 0.078 | 0.26 | 0.08–0.92 | 0.037 | |
| Grade 3 | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | |
| RD following first-line debulking | No visible RD | 0.12 | 0.05–0.31 | <0.0001 | 0.41 | 0.10–1.76 | 0.232 | 0.16 | 0.06–0.38 | <0.0001 | 0.60 | 0.17–2.09 | 0.418 |
| Macroscopic RD | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | ref | |
| Age at diagnosis | Years | 1.03 | 1.00–1.06 | 0.037 | 1.00 | 0.96–1.04 | 0.899 | 1.03 | 1.00–1.05 | 0.033 | 1.02 | 0.99–1.05 | 0.217 |
| Relapsed/Progressed | Recurrence Free at Last Follow-Up | |||||
|---|---|---|---|---|---|---|
| N | % | N | % | p-Value | ||
| Cases | N | 27 | - | 124 | - | - |
| Age at diagnosis | Median years | 61 | range 23–88 | 52 | range 16–88 | p = 0.057 + |
| Year of diagnosis | 2000–2004 | 4 | 14.8 | 29 | 23.4 | p = 0.777 ^ |
| 2005–2009 | 8 | 29.6 | 31 | 25 | ||
| 2010–2014 | 8 | 29.6 | 37 | 29.8 | ||
| 2015 onwards | 7 | 25.9 | 27 | 21.8 | ||
| Pathological grade | Grade 1 | 10 | 37 | 87 | 70.2 | p = 0.001 ^ |
| Grade 2 | 12 | 44.4 | 32 | 25.8 | ||
| Grade 3 | 5 | 18.5 | 5 | 4 | ||
| FIGO stage at diagnosis | IA | 4 | 15.4 | 49 | 39.8 | p < 0.001 # |
| IC | 8 | 30.8 | 56 | 45.5 | ||
| IIA | 0 | 0 | 1 | 0.8 | ||
| IIB | 3 | 11.5 | 3 | 2.4 | ||
| IIC | 1 | 3.8 | 10 | 8.1 | ||
| III | 8 | 30.8 | 4 | 3.3 | ||
| IV | 2 | 7.7 | 0 | 0 | ||
| NA | 1 | - | 1 | - | ||
| RD following surgical debulking | No visible RD | 16 | 69.6 | 110 | 94.8 | p = 0.003 ~ |
| Macroscopic RD | 7 | 30.4 | 6 | 5.2 | ||
| NA | 4 | - | 8 | - | ||
| Treatment at relapse | Surgery | 5 a | 18.5 | - | - | - |
| Surgery + platinum-containing regime | 2 b | 7.4 | - | - | ||
| Single-agent platinum | 2 | 7.4 | - | - | ||
| Platinum-taxane | 2 | 7.4 | - | - | ||
| Other cytotoxic regime | 4 c | 14.8 | - | - | ||
| Radiotherapy | 1 | 3.7 | - | - | ||
| Letrozole | 1 | 3.7 | - | - | ||
| Awaiting decision at last follow-up | 1 | 3.7 | - | - | ||
| No active therapy—palliation only | 9 | 33.3 | - | - | ||
| Time to relapse | Median months | 12.4 | 95% CI 7.9–21.4 | - | - | - |
| Post-relapse survival | Median months | 5.0 | 95% CI 2.4–16.3 | - | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hollis, R.L.; Stillie, L.J.; Hopkins, S.; Bartos, C.; Churchman, M.; Rye, T.; Nussey, F.; Fegan, S.; Nirsimloo, R.; Inman, G.J.; et al. Clinicopathological Determinants of Recurrence Risk and Survival in Mucinous Ovarian Carcinoma. Cancers 2021, 13, 5839. https://doi.org/10.3390/cancers13225839
Hollis RL, Stillie LJ, Hopkins S, Bartos C, Churchman M, Rye T, Nussey F, Fegan S, Nirsimloo R, Inman GJ, et al. Clinicopathological Determinants of Recurrence Risk and Survival in Mucinous Ovarian Carcinoma. Cancers. 2021; 13(22):5839. https://doi.org/10.3390/cancers13225839
Chicago/Turabian StyleHollis, Robert L., Lorna J. Stillie, Samantha Hopkins, Clare Bartos, Michael Churchman, Tzyvia Rye, Fiona Nussey, Scott Fegan, Rachel Nirsimloo, Gareth J. Inman, and et al. 2021. "Clinicopathological Determinants of Recurrence Risk and Survival in Mucinous Ovarian Carcinoma" Cancers 13, no. 22: 5839. https://doi.org/10.3390/cancers13225839
APA StyleHollis, R. L., Stillie, L. J., Hopkins, S., Bartos, C., Churchman, M., Rye, T., Nussey, F., Fegan, S., Nirsimloo, R., Inman, G. J., Herrington, C. S., & Gourley, C. (2021). Clinicopathological Determinants of Recurrence Risk and Survival in Mucinous Ovarian Carcinoma. Cancers, 13(22), 5839. https://doi.org/10.3390/cancers13225839