
The Clinical Utility of the Geriatric Nutritional Risk Index in Predicting Postoperative Complications and Long-Term Survival in Elderly Patients with Colorectal Cancer after Curative Surgery

 , , , ,
, , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
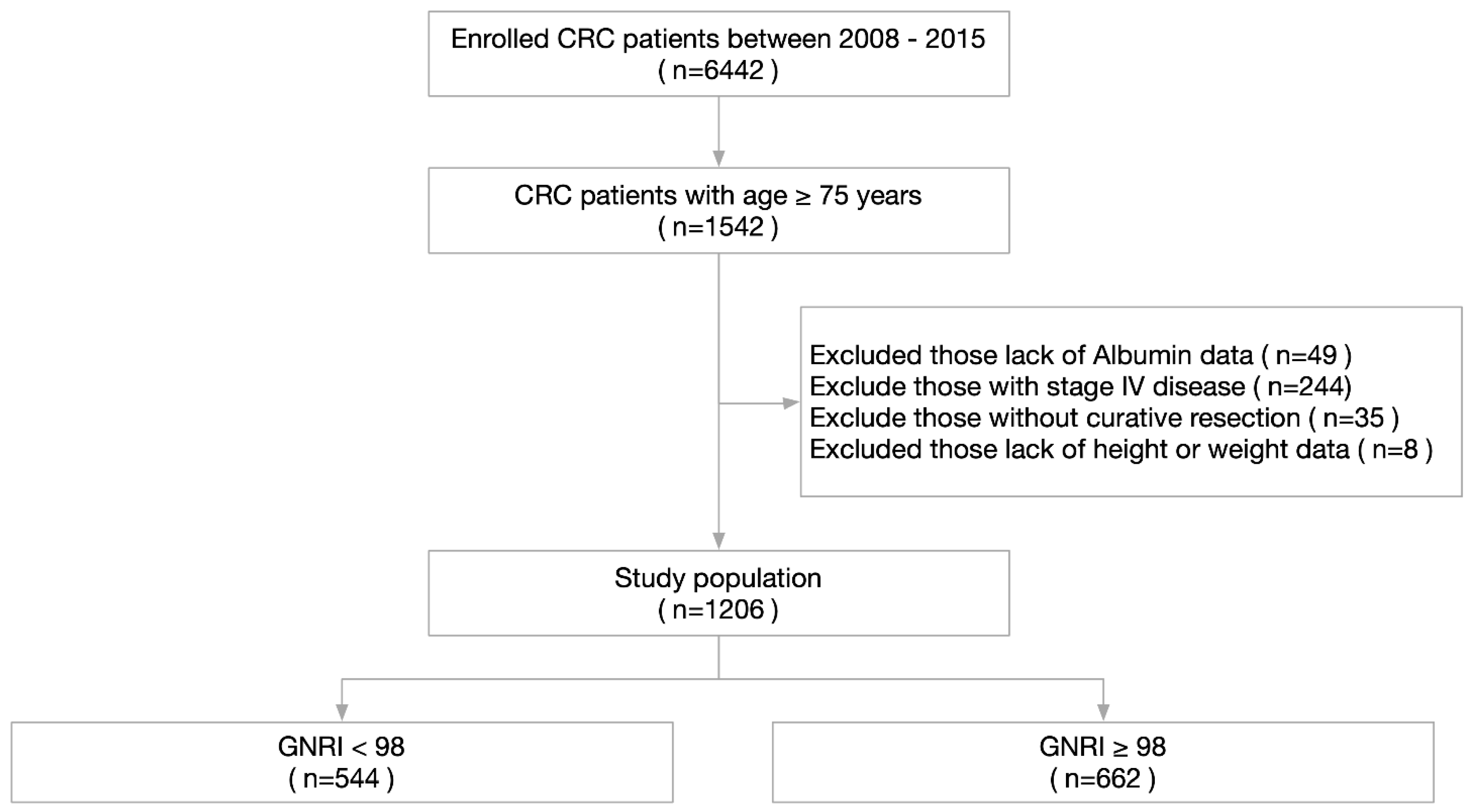
2.1. Patient Selection
2.2. Data Collection
2.3. Nutritional Assessment by GNRI and Other Parameters
2.4. Follow-Up
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. The Association of GNRI and Clinicopathological Factors
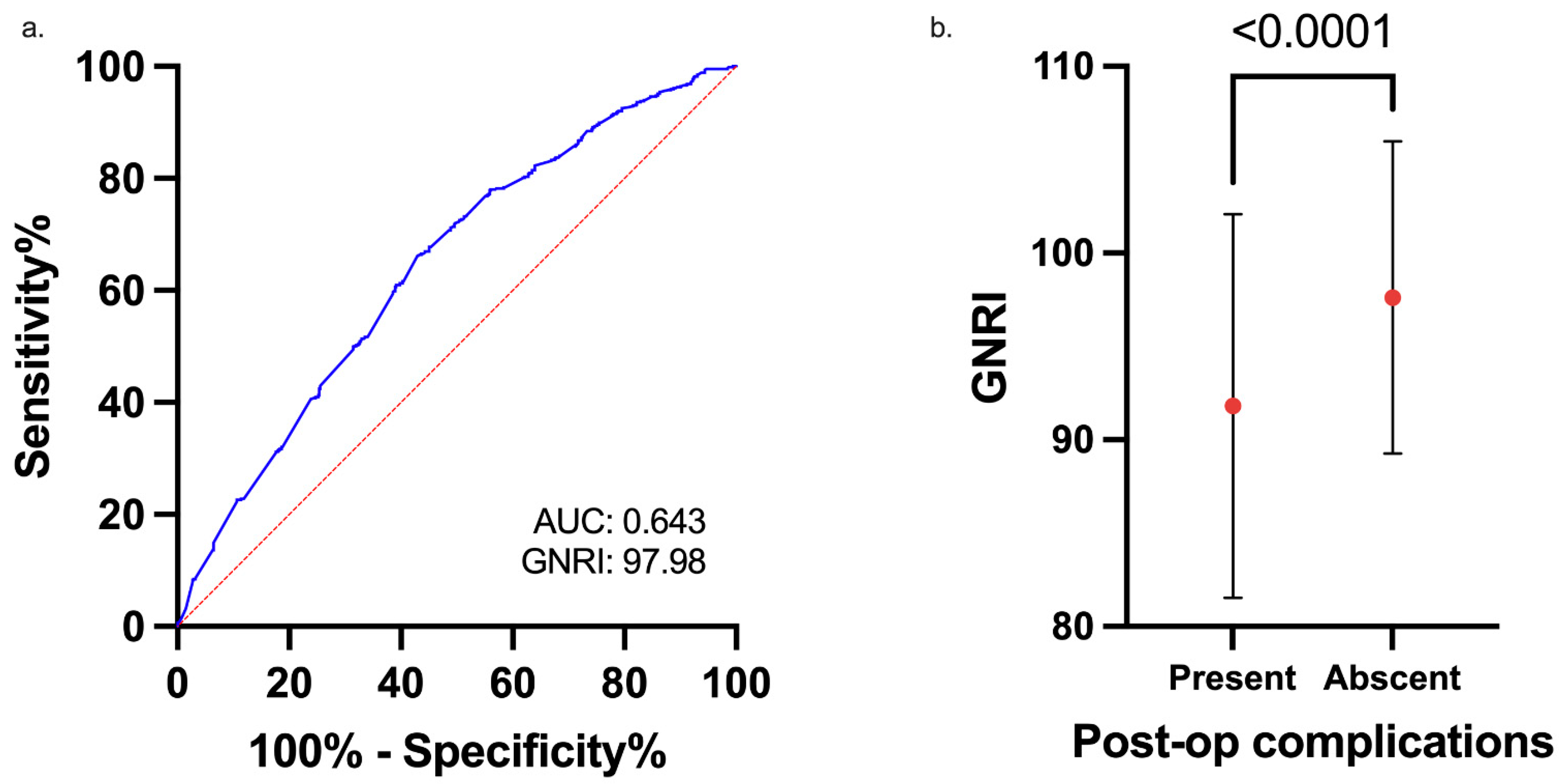
3.3. The Association of GNRI and Postoperative Complications
3.4. Risk Factors for CD Grade ≥ 2 Complications
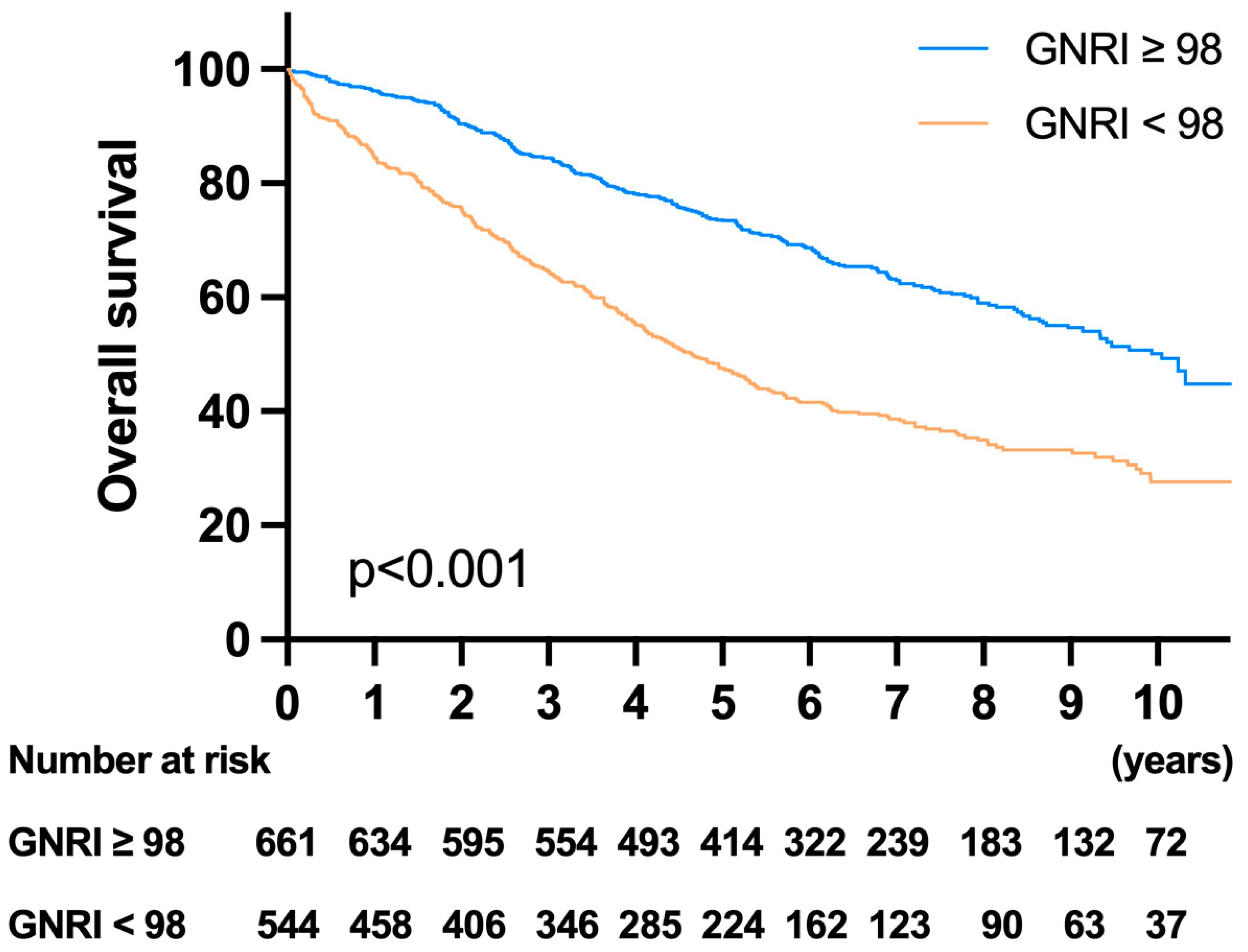
3.5. Survival Analysis and Prognostic Factors for OS
3.6. Survival Analysis and Prognostic Factors for DFS
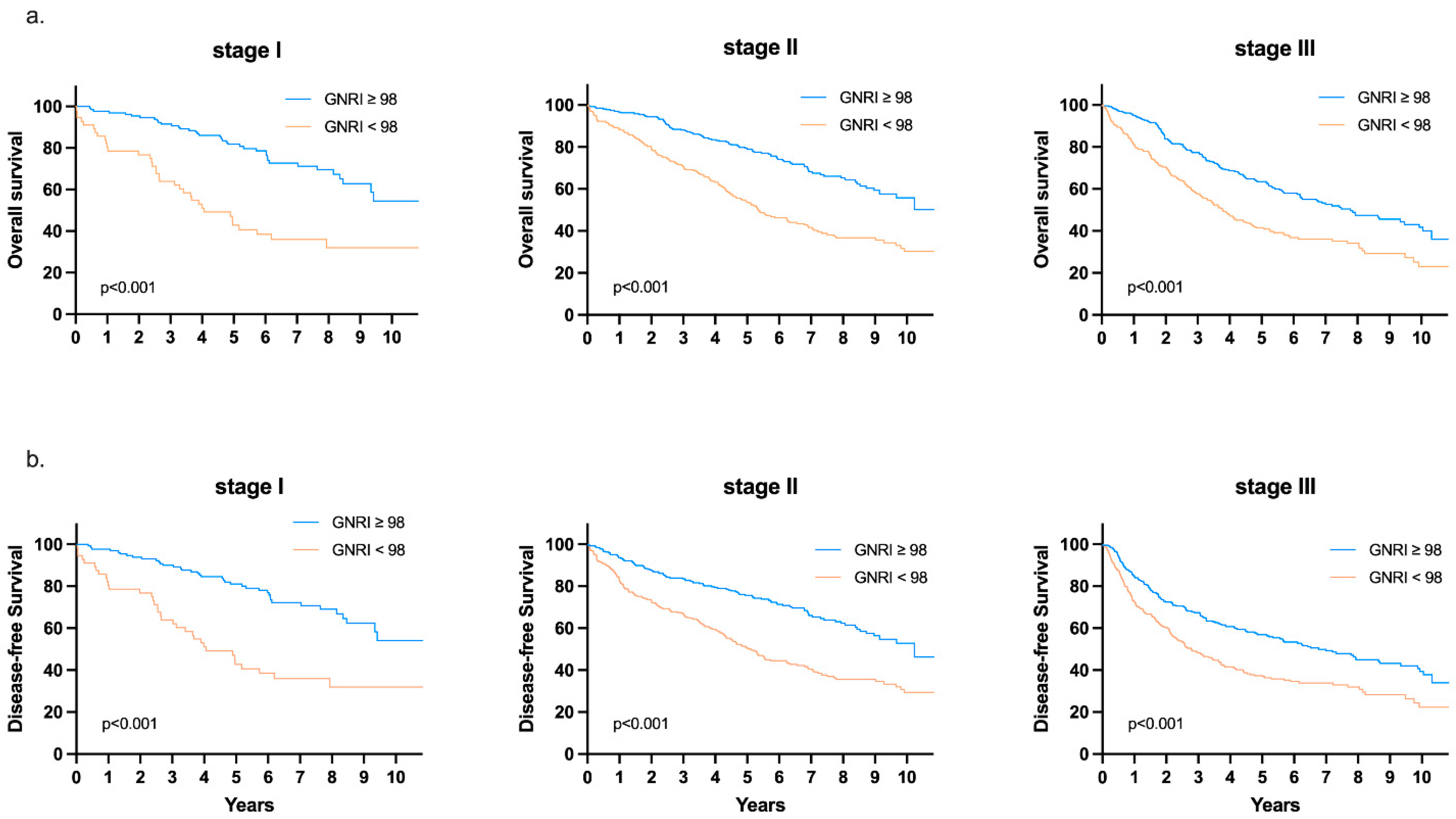
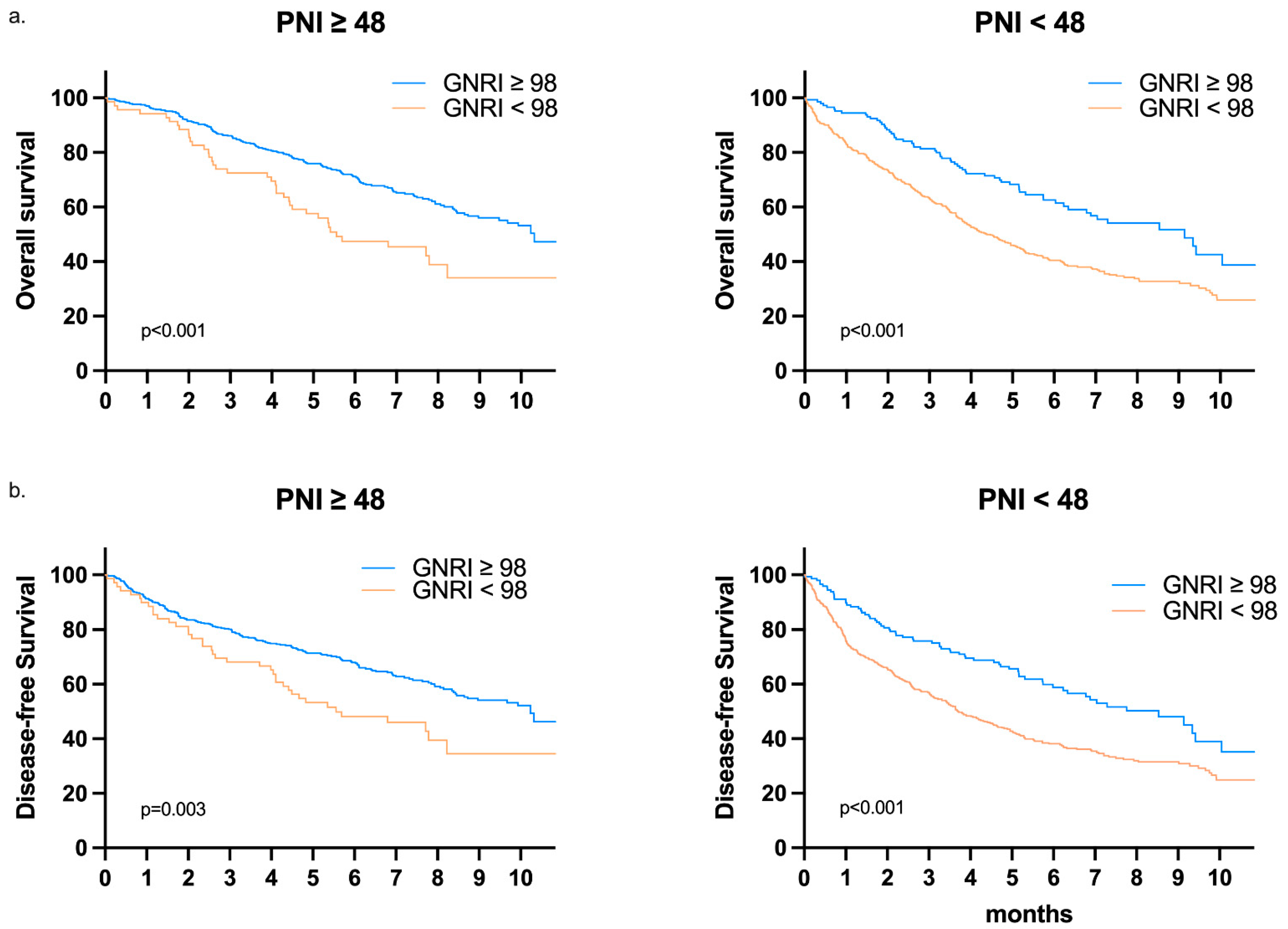
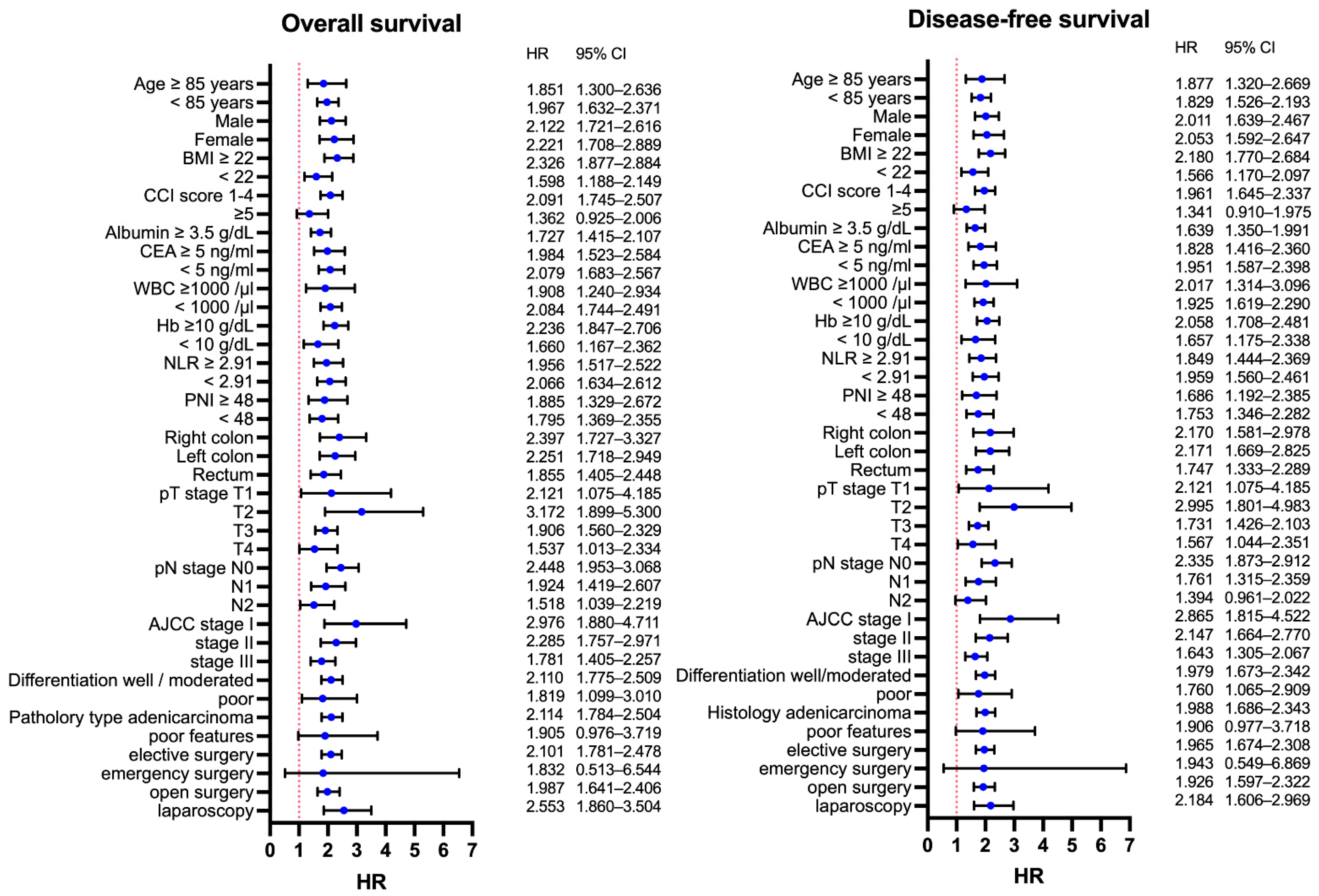
3.7. Subgroup Analysis and the Utility of GNRI on Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Goding Sauer, A.; Fedewa, S.A.; Butterly, L.F.; Anderson, J.C.; Cercek, A.; Smith, R.A.; Jemal, A. Colorectal cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 145–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, G.R.; Mackenzie, A.; Magnuson, A.; Olin, R.; Chapman, A.; Mohile, S.; Allore, H.; Somerfield, M.R.; Targia, V.; Extermann, M.; et al. Comorbidity in older adults with cancer. J. Geriatr. Oncol. 2016, 7, 249–257. [Google Scholar] [CrossRef] [Green Version]
- Von Meyenfeldt, M. Cancer-associated malnutrition: An introduction. Eur. J. Oncol. Nurs. 2005, 9 (Suppl. 2), S35–S38. [Google Scholar] [CrossRef] [PubMed]
- De Pinho, N.B.; Martucci, R.B.; Rodrigues, V.D.; D’Almeida, C.A.; Thuler, L.C.S.; Saunders, C.; Jager-Wittenaar, H.; Peres, W.A.F. High prevalence of malnutrition and nutrition impact symptoms in older patients with cancer: Results of a Brazilian multicenter study. Cancer 2020, 126, 156–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, X.; Edwards, B.J. Malnutrition in older adults with cancer. Curr. Oncol. Rep. 2019, 21, 80. [Google Scholar] [CrossRef]
- Bozzetti, F.; Gianotti, L.; Braga, M.; Di Carlo, V.; Mariani, L. Postoperative complications in gastrointestinal cancer patients: The joint role of the nutritional status and the nutritional support. Clin. Nutr. 2007, 26, 698–709. [Google Scholar] [CrossRef]
- Zhang, X.; Tang, T.; Pang, L.; Sharma, S.V.; Li, R.; Nyitray, A.G.; Edwards, B.J. Malnutrition and overall survival in older adults with cancer: A systematic review and meta-analysis. J. Geriatr. Oncol. 2019, 10, 874–883. [Google Scholar] [CrossRef]
- Bouillanne, O.; Morineau, G.; Dupont, C.; Coulombel, I.; Vincent, J.P.; Nicolis, I.; Benazeth, S.; Cynober, L.; Aussel, C. Geriatric nutritional risk index: A new index for evaluating at-risk elderly medical patients. Am. J. Clin. Nutr. 2005, 82, 777–783. [Google Scholar] [CrossRef] [Green Version]
- Abd-El-Gawad, W.M.; Abou-Hashem, R.M.; El Maraghy, M.O.; Amin, G.E. The validity of geriatric nutrition risk index: Simple tool for prediction of nutritional-related complication of hospitalized elderly patients. Comparison with mini nutritional assessment. Clin. Nutr. 2014, 33, 1108–1116. [Google Scholar] [CrossRef]
- Cereda, E.; Zagami, A.; Vanotti, A.; Piffer, S.; Pedrolli, C. Geriatric nutritional risk index and overall-cause mortality prediction in institutionalised elderly: A 3-year survival analysis. Clin. Nutr. 2008, 27, 717–723. [Google Scholar] [CrossRef] [PubMed]
- Cereda, E.; Klersy, C.; Pedrolli, C.; Cameletti, B.; Bonardi, C.; Quarleri, L.; Cappello, S.; Bonoldi, A.; Bonadeo, E.; Caccialanza, R. The geriatric nutritional risk index predicts hospital length of stay and in-hospital weight loss in elderly patients. Clin. Nutr. 2015, 34, 74–78. [Google Scholar] [CrossRef] [PubMed]
- Kushiyama, S.; Sakurai, K.; Kubo, N.; Tamamori, Y.; Nishii, T.; Tachimori, A.; Inoue, T.; Maeda, K. The preoperative geriatric nutritional risk index predicts postoperative complications in elderly patients with gastric cancer undergoing gastrectomy. In Vivo 2018, 32, 1667–1672. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bo, Y.; Wang, K.; Liu, Y.; You, J.; Cui, H.; Zhu, Y.; Lu, Q.; Yuan, L. The geriatric nutritional risk index predicts survival in elderly esophageal squamous cell carcinoma patients with radiotherapy. PLoS ONE 2016, 11, e0155903. [Google Scholar] [CrossRef]
- Li, L.; Wang, H.; Yang, J.; Jiang, L.; Yang, J.; Wu, H.; Wen, T.; Yan, L. Geriatric nutritional risk index predicts prognosis after hepatectomy in elderly patients with hepatitis B virus-related hepatocellular carcinoma. Sci. Rep. 2018, 8, 12561. [Google Scholar] [CrossRef]
- Hino, H.; Saito, T.; Matsui, H.; Taniguchi, Y.; Murakawa, T. Utility of geriatric nutritional risk index in patients with lung cancer undergoing surgery. Eur. J. Cardiothorac. Surg. 2020, 58, 775–782. [Google Scholar] [CrossRef]
- Sasaki, M.; Miyoshi, N.; Fujino, S.; Ogino, T.; Takahashi, H.; Uemura, M.; Matsuda, C.; Yamamoto, H.; Mizushima, T.; Mori, M.; et al. The geriatric nutritional risk index predicts postoperative complications and prognosis in elderly patients with colorectal cancer after curative surgery. Sci. Rep. 2020, 10, 10744. [Google Scholar] [CrossRef] [PubMed]
- Tang, S.; Xie, H.; Kuang, J.; Gao, F.; Gan, J.; Ou, H. The value of geriatric nutritional risk index in evaluating postoperative complication risk and long-term prognosis in elderly colorectal cancer patients. Cancer Manag. Res. 2020, 12, 165–175. [Google Scholar] [CrossRef] [Green Version]
- Attar, A.; Malka, D.; Sabaté, J.M.; Bonnetain, F.; Lecomte, T.; Aparicio, T.; Locher, C.; Laharie, D.; Ezenfis, J.; Taieb, J. Malnutrition is high and underestimated during chemotherapy in gastrointestinal cancer: An AGEO prospective cross-sectional multicenter study. Nutr. Cancer 2012, 64, 535–542. [Google Scholar] [CrossRef]
- Shpata, V.; Prendushi, X.; Kreka, M.; Kola, I.; Kurti, F.; Ohri, I. Malnutrition at the time of surgery affects negatively the clinical outcome of critically ill patients with gastrointestinal cancer. Med. Arch. 2014, 68, 263–267. [Google Scholar] [CrossRef] [Green Version]
- Maia, F.C.P.; Silva, T.A.; Generoso, S.V.; Correia, M. Malnutrition is associated with poor health-related quality of life in surgical patients with gastrointestinal cancer. Nutrition 2020, 75–76, 110769. [Google Scholar] [CrossRef] [PubMed]
- Lai, C.C.; You, J.F.; Yeh, C.Y.; Chen, J.S.; Tang, R.; Wang, J.Y.; Chin, C.C. Low preoperative serum albumin in colon cancer: A risk factor for poor outcome. Int. J. Colorectal Dis. 2011, 26, 473–481. [Google Scholar] [CrossRef] [PubMed]
- Isik, A.; Okan, I.; Firat, D.; Yilmaz, B.; Akcakaya, A.; Sahin, M. A new prognostic strategy for gastric carcinoma: Albumin level and metastatic lymph node ratio. Minerva Chir. 2014, 69, 147–153. [Google Scholar]
- Sun, K.; Chen, S.; Xu, J.; Li, G.; He, Y. The prognostic significance of the prognostic nutritional index in cancer: A systematic review and meta-analysis. J. Cancer Res. Clin. Oncol. 2014, 140, 1537–1549. [Google Scholar] [CrossRef] [PubMed]
- Nozoe, T.; Kohno, M.; Iguchi, T.; Mori, E.; Maeda, T.; Matsukuma, A.; Ezaki, T. The prognostic nutritional index can be a prognostic indicator in colorectal carcinoma. Surg. Today 2012, 42, 532–535. [Google Scholar] [CrossRef]
- Lee, J.H.; Park, B.; Joo, J.; Kook, M.C.; Kim, Y.I.; Lee, J.Y.; Kim, C.G.; Choi, I.J.; Eom, B.W.; Yoon, H.M.; et al. Body mass index and mortality in patients with gastric cancer: A large cohort study. Gastric Cancer 2018, 21, 913–924. [Google Scholar] [CrossRef] [Green Version]
- Miyamoto, Y.; Baba, Y.; Sakamoto, Y.; Ohuchi, M.; Tokunaga, R.; Kurashige, J.; Hiyoshi, Y.; Iwagami, S.; Yoshida, N.; Yoshida, M.; et al. Sarcopenia is a negative prognostic factor after curative resection of colorectal cancer. Ann. Surg. Oncol. 2015, 22, 2663–2668. [Google Scholar] [CrossRef]
- Choi, Y.; Oh, D.Y.; Kim, T.Y.; Lee, K.H.; Han, S.W.; Im, S.A.; Kim, T.Y.; Bang, Y.J. Skeletal muscle depletion predicts the prognosis of patients with advanced pancreatic cancer undergoing palliative chemotherapy, independent of body mass index. PLoS ONE 2015, 10, e0139749. [Google Scholar] [CrossRef] [Green Version]
- Bullock, A.F.; Greenley, S.L.; McKenzie, G.A.G.; Paton, L.W.; Johnson, M.J. Relationship between markers of malnutrition and clinical outcomes in older adults with cancer: Systematic review, narrative synthesis and meta-analysis. Eur. J. Clin. Nutr. 2020, 74, 1519–1535. [Google Scholar] [CrossRef]
- Reber, E.; Gomes, F.; Vasiloglou, M.F.; Schuetz, P.; Stanga, Z. Nutritional Risk Screening and Assessment. J. Clin. Med. 2019, 20, 1065. [Google Scholar] [CrossRef] [Green Version]
- Xie, H.; Tang, S.; Wei, L.; Gan, J. Geriatric nutritional risk index as a predictor of complications and long-term outcomes in patients with gastrointestinal malignancy: A systematic review and meta-analysis. Cancer Cell Int. 2020, 20, 530. [Google Scholar] [CrossRef] [PubMed]
- Liao, C.K.; Chiang, J.M.; Tsai, W.S.; You, J.F.; Hsieh, P.S.; Hung, H.Y.; Chen, H.H.; Tang, R.P.; Chen, J.S.; Yeh, C.Y. Primary tumor location in stage III colon cancer has prognostic impact on subsequent liver metastasis. J. Surg. Oncol. 2018, 118, 1301–1310. [Google Scholar] [CrossRef]
- Duraes, L.C.; Stocchi, L.; Steele, S.R.; Kalady, M.F.; Church, J.M.; Gorgun, E.; Liska, D.; Kessler, H.; Lavryk, O.A.; Delaney, C.P. The relationship between clavien-dindo morbidity classification and oncologic outcomes after colorectal cancer resection. Ann. Surg. Oncol. 2018, 25, 188–196. [Google Scholar] [CrossRef] [PubMed]
- Walsh, S.R.; Cook, E.J.; Goulder, F.; Justin, T.A.; Keeling, N.J. Neutrophil-lymphocyte ratio as a prognostic factor in colorectal cancer. J. Surg. Oncol. 2005, 91, 181–184. [Google Scholar] [CrossRef] [PubMed]
- Mohri, Y.; Inoue, Y.; Tanaka, K.; Hiro, J.; Uchida, K.; Kusunoki, M. Prognostic nutritional index predicts postoperative outcome in colorectal cancer. World J. Surg. 2013, 37, 2688–2692. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | All Patients (n = 1206) |
|---|---|
| Age | 80.45 ± 4.42 |
| Sex (male/female) | 673/573 (55.8%/44.2%) |
| BMI | 23.45 ± 3.70 |
| Charlson comorbidity index score | |
| Mild (1–2) | 423 (35.1) |
| Moderate (3–4) | 627 (52.0) |
| Severe (≥5) | 156 (12.9) |
| Albumin (g/dL) | 3.82 ± 0.52 |
| CEA (ng/mL) | 11.76 ± 57.86 |
| Operation type (elective/emergent) | 1184/22 |
| Operative method (open/laparoscopy) | 848/358 |
| Tumor location | |
| Right colon | 351 (29.1) |
| Left colon | 462 (38.2) |
| Rectum | 393 (32.5) |
| GNRI | 96.92 ± 8.82 |
| Tumor invasion | |
| T1 | 84 (7) |
| T2 | 153 (12.7) |
| T3 | 807 (66.9) |
| T4 | 161 (13.3) |
| Lymph node metastasis | |
| N0 | 713 (59.1) |
| N1 | 332 (27.5) |
| N2 | 160 (13.3) |
| Stage | |
| Stage I | 187 (15.5) |
| Stage II | 527 (43.7) |
| Stage III | 492 (40.8) |
| Follow up time (months) | 63.01 ± 35.79 |
| All postoperative complications | 220 (18.2) |
| CD grade ≥ 2 complications | 145 (12.0) |
| Variables | GNRI < 98 (n = 544) | GNRI ≥ 98 (n = 662) | p Value |
|---|---|---|---|
| Age | 81.58 ± 4.80 | 79.51 ± 3.84 | <0.001 |
| Sex | |||
| Male | 291 (53.5) | 382 (57.7) | 0.143 |
| Female | 253 (46.5) | 280 (42.3) | |
| BMI | 21.74 ± 3.57 | 24.85 ± 3.70 | <0.001 |
| CCI score | |||
| 1–4 | 439 (80.7) | 611 (92.3) | <0.001 |
| ≥5 | 105 (19.3) | 51 (7.7) | |
| Albumin | |||
| <3.5 g/dL | 264 (48.5) | 0 (0) | <0.001 |
| ≥3.5 g/dL | 280 (51.5) | 662 (100) | |
| CEA | |||
| <5 ng/mL | 319 (60.0) | 462 (69.9) | <0.001 |
| ≥5 ng/mL | 213 (40.0) | 199 (30.1) | |
| WBC | |||
| <1000/µL | 435 (80) | 599 (90.5) | <0.001 |
| ≥1000/µL | 109 (20) | 63 (9.5) | |
| Hb | |||
| <10 g/dL | 216 (39.7) | 94 (14.2) | <0.001 |
| ≥10 g/dL | 328 (60.3) | 568 (85.8) | |
| NLR | |||
| <2.91 | 241 (46.1) | 421 (68.8) | <0.001 |
| ≥2.91 | 282 (53.9) | 191 (31.2) | |
| PNI | |||
| <48 | 454 (86.8) | 145 (23.5) | <0.001 |
| ≥48 | 69 (13.2) | 472 (76.5) | |
| Tumor location | |||
| Right colon | 201 (36.9) | 150 (22.7) | <0.001 |
| Left colon | 200 (36.8) | 262 (39.6) | |
| Rectum | 143 (26.3) | 250 (37.8) | |
| Neoadjuvant treatment * | |||
| Yes | 26 (18.2) | 45 (18) | 0.964 |
| No | 117 (81.8) | 205 (82) | |
| Tumor invasion | |||
| T1 | 24 (4.4) | 60 (9.1) | <0.001 |
| T2 | 50 (9.2) | 103 (15.6) | |
| T3 | 362 (66.7) | 445 (67.2) | |
| T4 | 107 (19.7) | 54 (8.2) | |
| Lymph node metastasis | |||
| N0 | 315 (58.0) | 398 (60.1) | 0.575 |
| N1 | 150 (27.6) | 182 (27.5) | |
| N2 | 78 (14.4) | 81 (12.4) | |
| Stage | |||
| Stage I | 56 (10.3) | 131 (19.8) | <0.001 |
| Stage II | 260 (47.8) | 267 (40.3) | |
| Stage III | 228 (41.9) | 264 (40.8) | |
| Histological grade | |||
| Well/moderately differentiated | 473 (86.9) | 615 (92.9) | 0.001 |
| Poorly differentiated | 71 (13.1) | 47 (7.1) | |
| Histological type | |||
| Adenocarcinoma | 489 (90.7) | 638 (96.4) | <0.001 |
| Poor features ** | 50 (9.3) | 24 (3.6) | |
| Operative type | |||
| Elective | 528 (97.1) | 656 (99.1) | 0.009 |
| Emergency | 16 (2.9) | 6 (0.9) | |
| Operative method | |||
| Laparotomy | 420 (77.2) | 428 (64.7) | <0.001 |
| Laparoscopy | 124 (22.8) | 234 (35.3) |
| Variables | GNRI < 98 (n = 544) | GNRI ≥ 98 (n = 662) | p Value |
|---|---|---|---|
| All complications | 136 (25) | 84 (12.7) | <0.001 |
| Surgical site infection | 40 (7.4) | 23 (3.5) | 0.003 |
| Ileus | 29 (5.3) | 21 (3.2) | 0.061 |
| Leakage | 7 (1.3) | 12 (1.8) | 0.465 |
| Wound dehiscence | 6 (1.1) | 1 (0.2) | 0.051 * |
| IAI | 12 (2.2) | 6 (0.9) | 0.064 |
| Pneumonia | 37 (6.8) | 7 (1.1) | <0.001 |
| Urinary tract infection | 18 (3.8) | 8 (1.2) | 0.012 |
| Cardiovascular events | 7 (1.3) | 4 (0.6) | 0.238 * |
| CD grade ≥ 2 | 100 (18.4) | 45 (6.8) | <0.001 |
| Mortality | 16 (2.9) | 2 (0.3) | <0.001 |
| Postoperative nutrition intervention | |||
| Total | 19 (14) | 5 (6) | 0.178 |
| Partial | 17 (12.5) | 12 (14.3) |
| Variables | Univariate | Multivariate | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p Value | HR | 95% CI | p Value | |
| Age (≥85/<85) | 1.771 | 1.178–2.661 | 0.006 | 1.362 | 0.884–2.098 | 0.161 |
| Sex (male/female) | 1.177 | 0.827–1.675 | 0.365 | |||
| BMI (<22/≥22) | 1.345 | 0.945–1.914 | 0.1 | |||
| CCI scores | ||||||
| 1–4 | 1 | 1 | ||||
| ≥5 | 2.358 | 1.537–3.617 | <0.001 | 1.601 | 1.004–2.554 | 0.048 |
| Albumin (<3.5/≥3.5) | 2.767 | 1.930–3.988 | <0.001 | 1.43 | 0.890–2.295 | 0.139 |
| WBC count (≥1000) | 1.605 | 1.030–2.500 | 0.037 | 1.011 | 0.607–1.685 | 0.966 |
| Hb (<10) | 1.207 | 0.821–1.773 | 0.339 | |||
| CEA (≥5) | 1.047 | 0.725–1.513 | 0.805 | |||
| PNI (<48) | 2.58 | 1.746–3.811 | <0.001 | 1.184 | 0.677–2.070 | 0.554 |
| NLR (≥2.91) | 1.911 | 1.337–2.730 | <0.001 | 1.275 | 0.832–1.955 | 0.264 |
| GNRI (<98) | 3.088 | 2.128–4.481 | <0.001 | 1.774 | 1.035–3.040 | 0.037 |
| Tumor location | ||||||
| Left/right colon | 0.715 | 0.466–1.097 | 0.125 | |||
| Rectum/right colon | 0.92 | 0.602–1.408 | 0.701 | |||
| Tumor invasion | ||||||
| T1 | 1 | |||||
| T2 | 0.8 | 0.365–1.753 | 0.577 | |||
| T3 | 0.725 | 0.378–1.389 | 0.332 | |||
| T4 | 1.263 | 0.606–2.633 | 0.533 | |||
| LN metastasis | ||||||
| N0 | 1 | |||||
| N1 | 0.942 | 0.628–1.414 | 0.774 | |||
| N2 | 1.101 | 0.661–1.837 | 0.711 | |||
| Stage | ||||||
| Stage I | 1 | |||||
| Stage II | 0.848 | 0.515–1.397 | 0.518 | |||
| Stage III | 0.883 | 0.535–1.458 | 0.627 | |||
| Histological grade | ||||||
| Well/moderately differentiated | 1 | |||||
| Poorly differentiated | 1.262 | 0.731–2.179 | 0.403 | |||
| Histological type | ||||||
| Adenocarcinoma | 1 | |||||
| Poor features * | 1.606 | 0.859–3.003 | 0.138 | |||
| Operative type (emergency) | 3.537 | 1.417–8.828 | 0.007 | 2.177 | 0.821–5.773 | 0.118 |
| Operative method (open) | 1.123 | 0.763–1.655 | 0.556 | |||
| Neoadjuvant treatment (Yes/No) ** | 1.156 | 0.548–2.437 | 0.704 | |||
| Variables | Univariate | Multivariate | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p Value | HR | 95% CI | p Value | |
| Age (≥85/<85) | 2.34 | 1.940–2.822 | <0.001 | 2.046 | 1.673–2.502 | <0.001 |
| Sex (male/female) | 1.271 | 1.078–1.499 | 0.004 | 1.332 | 1.118–1.587 | 0.001 |
| BMI (<22/≥22) | 1.485 | 1.261–1.749 | <0.001 | 1.236 | 1.026–1.489 | 0.026 |
| CCI scores | ||||||
| 1–4 | 1 | 1 | ||||
| ≥5 | 2.517 | 2.055–3.084 | <0.001 | 2.081 | 1.658–2.612 | <0.001 |
| Albumin (<3.5/≥3.5) | 2.237 | 1.875–2.668 | <0.001 | 1.275 | 1.009–1.611 | 0.042 |
| WBC count (≥1000) | 1.495 | 1.208–1.849 | <0.001 | 1.005 | 0.784–1.287 | 0.971 |
| Hb (<10) | 1.331 | 1.113–1.593 | 0.002 | 0.887 | 0.724–1.086 | 0.246 |
| CEA (≥5) | 1.461 | 1.237–1.724 | <0.001 | 1.162 | 0.969–1.395 | 0.105 |
| PNI (<48) | 1.938 | 1.631–2.302 | <0.001 | 1.145 | 0.889–1.474 | 0.295 |
| NLR (≥2.91) | 1.688 | 1.429–1.995 | <0.001 | 1.208 | 0.989–1.476 | 0.064 |
| GNRI (<98) | 2.115 | 1.796–2.490 | <0.001 | 1.329 | 1.026–1.722 | 0.031 |
| Tumor location | ||||||
| Left colon/right colon | 0.804 | 0.707–1.055 | 0.152 | |||
| Rectum/right colon | 0.971 | 0.792–1.189 | 0.773 | |||
| Tumor invasion | ||||||
| T1 | 1 | 1 | ||||
| T2 | 0.929 | 0.612–1.412 | 0.73 | 0.924 | 0.598–1.428 | 0.723 |
| T3 | 1.221 | 0.864–1.726 | 0.258 | 0.904 | 0.621–1.316 | 0.904 |
| T4 | 2.453 | 1.675–3.592 | <0.001 | 1.473 | 0.959–2.263 | 0.077 |
| Lymph node metastasis | ||||||
| N0 | 1 | 1 | ||||
| N1 | 1.264 | 1.048–1.524 | 0.014 | 1.27 | 1.036–1.556 | 0.021 |
| N2 | 2.053 | 1.649–2.557 | <0.001 | 2.061 | 1.623–2.618 | <0.001 |
| Stage | ||||||
| Stage I | 1 | |||||
| Stage II | 1.178 | 0.908–1.529 | 0.218 | |||
| Stage III | 1.685 | 1.303–2.177 | <0.001 | |||
| Histological grade | ||||||
| Well/moderately differentiated | 1 | 1 | ||||
| Poorly differentiated | 1.503 | 1.171–1.929 | 0.001 | 1.127 | 0.812–1.564 | 0.475 |
| Histological type | ||||||
| Adenocarcinoma | 1 | 1 | ||||
| Poor features * | 1.537 | 1.137–2.077 | 0.005 | 1.127 | 0.766–1.656 | 0.544 |
| Operative type (emergency) | 1.951 | 1.168–3.259 | 0.011 | 1.003 | 0.539–1.868 | 0.991 |
| Operative method (open) | 1.093 | 0.909–1.315 | 0.344 | |||
| Variables | Univariate | Multivariate | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p Value | HR | 95% CI | p Value | |
| Age (≥85/<85) | 2.145 | 1.783–2.579 | <0.001 | 1.9 | 1.560–2.316 | <0.001 |
| Sex (male/female) | 1.279 | 1.090–1.502 | 0.003 | 1.341 | 1.130–1.591 | 0.001 |
| BMI (<22/≥22) | 1.394 | 1.188–1.636 | <0.001 | 1.186 | 0.988–1.423 | 0.067 |
| CCI scores | ||||||
| 1–4 | 1 | 1 | ||||
| ≥5 | 2.262 | 1.849–2.768 | <0.001 | 1.938 | 1.547–2.429 | <0.001 |
| Albumin (<3.5/≥3.5) | 2.091 | 1.759–2.486 | <0.001 | 1.201 | 0.954–1.512 | 0.118 |
| WBC count (≥1000) | 1.427 | 1.157–1.759 | 0.001 | 0.937 | 0.734–1.195 | 0.599 |
| Hb (<10) | 1.309 | 1.099–1.559 | 0.002 | 0.88 | 0.722–1.073 | 0.207 |
| CEA (≥5) | 1.554 | 1.323–1.827 | <0.001 | 1.259 | 1.054–1.503 | 0.011 |
| PNI (<48) | 1.866 | 1.578–2.207 | <0.001 | 1.162 | 0.911–1.484 | 0.227 |
| NLR (≥2.91) | 1.633 | 1.387–1.922 | <0.001 | 1.194 | 0.982–1.452 | 0.075 |
| GNRI (<98) | 1.985 | 1.694–2.327 | <0.001 | 1.312 | 1.021–1.685 | 0.034 |
| Tumor location | ||||||
| Left colon/right colon | 0.885 | 0.728–1.076 | 0.222 | |||
| Rectum/right colon | 0.998 | 0.819–1.217 | 0.987 | |||
| Tumor invasion | ||||||
| T1 | 1 | 1 | ||||
| T2 | 0.951 | 0.627–1.443 | 0.814 | 0.94 | 0.609–1.450 | 0.78 |
| T3 | 1.364 | 0.966–1.927 | 0.078 | 1.01 | 0.695–1.469 | 0.957 |
| T4 | 2.734 | 1.871–3.994 | <0.001 | 1.675 | 1.096–2.560 | 0.017 |
| Lymph node metastasis | ||||||
| N0 | 1 | 1 | ||||
| N1 | 1.337 | 1.115–1.603 | 0.002 | 1.345 | 1.106–1.637 | 0.003 |
| N2 | 2.222 | 1.792–2.756 | <0.001 | 2.212 | 1.748–2.799 | <0.001 |
| Stage | ||||||
| Stage I | 1 | |||||
| Stage II | 1.264 | 0.977–1.636 | 0.075 | |||
| Stage III | 1.883 | 1.461–2.426 | <0.001 | |||
| Histological grade | ||||||
| Well/moderately differentiated | 1 | |||||
| Poorly differentiated | 1.414 | 1.105–1.811 | 0.006 | 1.018 | 0.739–1.402 | 0.913 |
| Histological type | ||||||
| Adenocarcinoma | 1 | |||||
| Poor features * | 1.407 | 1.042–1.901 | 0.026 | 1.057 | 0.725–1.541 | 0.773 |
| Operative type (emergency) | 2.074 | 1.262–3.408 | 0.004 | 1.035 | 0.572–1.874 | 0.909 |
| Operative method (open) | 1.1 | 0.919–1.315 | 0.298 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liao, C.-K.; Chern, Y.-J.; Hsu, Y.-J.; Lin, Y.-C.; Yu, Y.-L.; Chiang, J.-M.; Yeh, C.-Y.; You, J.-F. The Clinical Utility of the Geriatric Nutritional Risk Index in Predicting Postoperative Complications and Long-Term Survival in Elderly Patients with Colorectal Cancer after Curative Surgery. Cancers 2021, 13, 5852. https://doi.org/10.3390/cancers13225852
Liao C-K, Chern Y-J, Hsu Y-J, Lin Y-C, Yu Y-L, Chiang J-M, Yeh C-Y, You J-F. The Clinical Utility of the Geriatric Nutritional Risk Index in Predicting Postoperative Complications and Long-Term Survival in Elderly Patients with Colorectal Cancer after Curative Surgery. Cancers. 2021; 13(22):5852. https://doi.org/10.3390/cancers13225852
Chicago/Turabian StyleLiao, Chun-Kai, Yih-Jong Chern, Yu-Jen Hsu, Yueh-Chen Lin, Yen-Lin Yu, Jy-Ming Chiang, Chien-Yuh Yeh, and Jeng-Fu You. 2021. "The Clinical Utility of the Geriatric Nutritional Risk Index in Predicting Postoperative Complications and Long-Term Survival in Elderly Patients with Colorectal Cancer after Curative Surgery" Cancers 13, no. 22: 5852. https://doi.org/10.3390/cancers13225852
APA StyleLiao, C. -K., Chern, Y. -J., Hsu, Y. -J., Lin, Y. -C., Yu, Y. -L., Chiang, J. -M., Yeh, C. -Y., & You, J. -F. (2021). The Clinical Utility of the Geriatric Nutritional Risk Index in Predicting Postoperative Complications and Long-Term Survival in Elderly Patients with Colorectal Cancer after Curative Surgery. Cancers, 13(22), 5852. https://doi.org/10.3390/cancers13225852