
Safety and Efficacy of Peptide-Receptor Radionuclide Therapy in Elderly Neuroendocrine Tumor Patients

 ,
,  , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
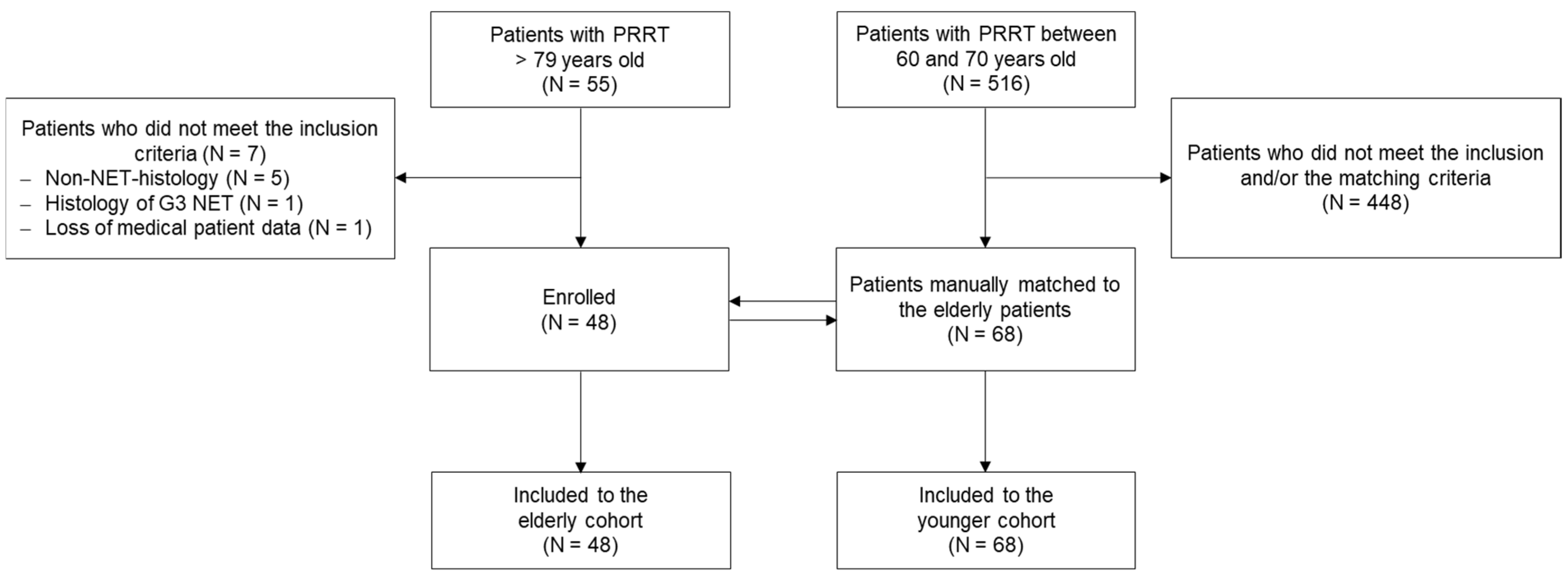
2.1. Patients
2.2. Trial Design
2.3. Treatment Protocol
2.4. Endpoints and Assessments
2.5. Statistical Analysis
3. Results
3.1. Patients and Baseline Characteristics
3.2. Safety
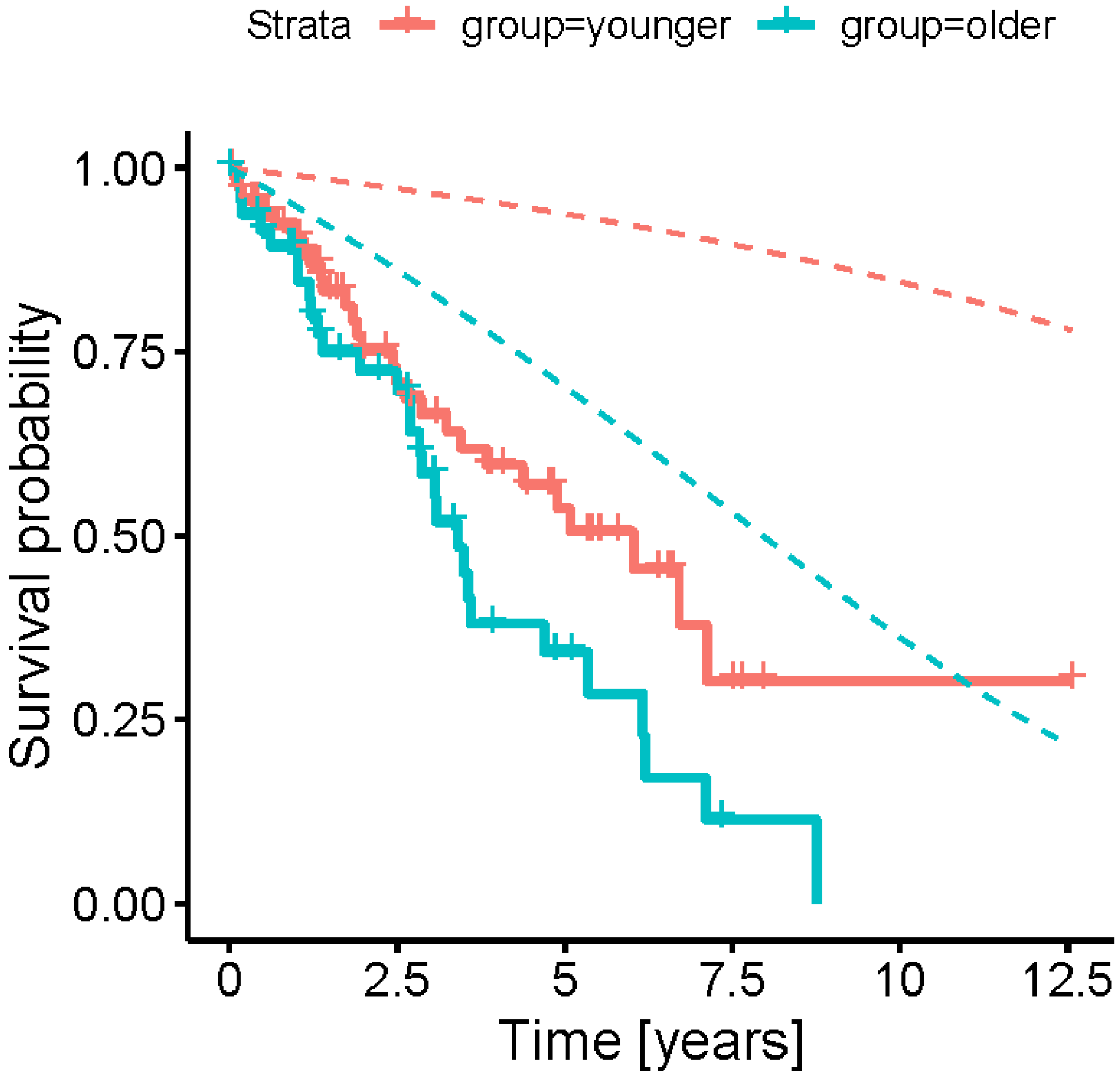
3.3. Efficacy
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Antwi, K.; Nicolas, G.; Wild, D.; Christ, E. Molecular imaging for neuroendocrine tumours. Swiss. Med. Wkly. 2019, 149, w20017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strosberg, J.; El-Haddag, G.; Wolin, E.; Hendifar, A.; Yao, J.; Chasen, B.; Mittra, E.; Kunz, P.L.; Kulke, M.H.; Jacene, H.; et al. Phase 3 Trial of (177)Lu-Dotatate for Midgut Neuroendocrine Tumors. N. Engl. J. Med. 2017, 376, 125–135. [Google Scholar] [CrossRef]
- Caplin, M.E.; Pavel, M.; Cwikla, J.B.; Phan, A.T.; Raderer, M.; Sedlackova, E.; Cadiot, G.; Wolin, E.M.; Capdevila, J.; Wall, L.; et al. Lanreotide in metastatic enteropancreatic neuroendocrine tumors. N. Engl. J. Med. 2014, 371, 224–233. [Google Scholar] [CrossRef]
- Kaderli, R.M.; Spanjol, M.; Kollar, A.; Butikoferl, L.; Gloy, V.; Dumont, R.A.; Seiler, C.A.; Christ, E.R.; Radojewski, P.; Briel, M.; et al. Therapeutic Options for Neuroendocrine Tumors: A Systematic Review and Network Meta-analysis. JAMA Oncol. 2019, 5, 480–489. [Google Scholar] [CrossRef] [PubMed]
- Nicolas, G.P.; Morgenstern, A.; Schottelius, M.; Fani, M. New Developments in Peptide Receptor Radionuclide Therapy. J. Nucl. Med. 2019, 60, 167–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rinke, A.; Muller, H.H.; Schade-Brittinger, C.; Klose, K.J.; Barth, P.; Wied, M.; Mayer, C.; Aminossadati, B.; Pape, U.F.; Blaker, M.; et al. Placebo-controlled, double-blind, prospective, randomized study on the effect of octreotide LAR in the control of tumor growth in patients with metastatic neuroendocrine midgut tumors: A report from the PROMID Study Group. J. Clin. Oncol. 2009, 27, 4656–4663. [Google Scholar] [CrossRef] [PubMed]
- Villard, L.; Romer, A.; Marincek, N.; Brunner, P.; Koller, M.T.; Schindler, C.; Ng, Q.K.; Macke, H.R.; Muller-Brand, J.; Rochlitz, C.; et al. Cohort study of somatostatin-based radiopeptide therapy with [(90)Y-DOTA]-TOC versus [(90)Y-DOTA]-TOC plus [(177)Lu-DOTA]-TOC in neuroendocrine cancers. J. Clin. Oncol. 2012, 30, 1100–1106. [Google Scholar] [CrossRef] [PubMed]
- Strosberg, J.; Wolin, E.; Chasen, B.; Kulke, M.; Bushnell, D.; Caplin, M.; Baum, R.P.; Kunz, P.; Hobday, T.; Hendifar, A.; et al. Health-Related Quality of Life in Patients With Progressive Midgut Neuroendocrine Tumors Treated With (177)Lu-Dotatate in the Phase III NETTER-1 Trial. J. Clin. Oncol. 2018, 36, 2578–2584. [Google Scholar] [CrossRef]
- Strosberg, J.R.; Caplin, M.E.; Kunz, P.L.; Ruszniewski, P.B.; Bodei, L.; Hendifar, A.; Mittra, E.; Wolin, E.M.; Yao, J.C.; Pavel, M.E.; et al. 177Lu-Dotatate plus long-acting octreotide versus high-dose long-acting octreotide in patients with midgut neuroendocrine tumours (NETTER-1): Final overall survival and long-term safety results from an open-label, randomised, controlled, phase 3 trial. Lancet Oncol. 2021, 22, 1752–1763. [Google Scholar] [CrossRef]
- Lemelin, A.; Maucort-Boulch, D.; Castel-Kremer, E.; Forestier, J.; Hervieu, V.; Lorcet, M.; Boutitie, F.; Theillaumas, A.; Robinson, P.; Duclos, A.; et al. Elderly Patients with Metastatic Neuroendocrine Tumors Are Undertreated and Have Shorter Survival: The LyREMeNET Study. Neuroendocrinology 2020, 110, 653–661. [Google Scholar] [CrossRef]
- Satapathy, S.; Mittal, B.R. 177-Lu-DOTATATE peptide receptor radionuclide therapy versus Everolimus in advanced pancreatic neuroendocrine tumors: A systematic review and meta-analysis. Nucl. Med. Commun. 2019, 40, 1195–1203. [Google Scholar] [CrossRef] [PubMed]
- Dasari, A.; Shen, C.; Halperin, D.; Zhao, B.; Zhou, S.; XU, Y.; Shih, T.; Yao, J.C. Trends in the Incidence, Prevalence, and Survival Outcomes in Patients with Neuroendocrine Tumors in the United States. JAMA Oncol. 2017, 3, 1335–1342. [Google Scholar] [CrossRef]
- Bushnell, D.L.; O’Dorisio, T.M.; O’Dorisio, M.S.; Menda, Y.; Hicks, R.J.; Van Cutsem, E.; Baulieu, J.; Borson-Chazot, F.; Anthony, L.; Benson, A.B.; et al. 90Y-edotreotide for metastatic carcinoid refractory to octreotide. J. Clin. Oncol. 2010, 28, 1652–1659. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagtegaal, I.D.; Odze, R.D.; Klimstra, D.; Paradis, V.; Rugge, M.; Schirmacher, P.; Washington, K.M.; Carneiro, F.; Cree, I.A.; WHO Classification of Tumours Editorial Board. The 2019 WHO classification of tumours of the digestive system. Histopathology 2020, 76, 182–188. [Google Scholar] [CrossRef] [Green Version]
- Bodei, L.; Mueller-Brand, J.; Baum, R.P.; Pavel, M.E.; Hörsch, D.; O’Dorisio, M.S.; O’Dorisio, T.M.; Howe, J.R.; Cremonesi, M.; Kwekkeboom, D.J.; et al. The joint IAEA, EANM, and SNMMI practical guidance on peptide receptor radionuclide therapy (PRRNT) in neuroendocrine tumours. Eur. J. Nucl. Med. Mol. Imaging 2013, 40, 800–816. [Google Scholar] [CrossRef]
- Hicks, R.J.; Kwekkeboom, D.K.; Krenning, E.; Bodei, L.; Grozinsky-Glasberg, S.; Arnold, R.; Borbath, I.; Cwikla, J.; Toumpanakis, C.; Kaltsas, G.; et al. ENETS Consensus Guidelines for the Standards of Care in Neuroendocrine Neoplasia: Peptide Receptor Radionuclide Therapy with Radiolabeled Somatostatin Analogues. Neuroendocrinology 2017, 105, 295–309. [Google Scholar] [CrossRef] [PubMed]
- Ming, K.; Rosenbaum, P.R. Substantial gains in bias reduction from matching with a variable number of controls. Biometrics 2000, 56, 118–124. [Google Scholar] [CrossRef] [PubMed]
- Imhof, A.; Brunner, P.; Marincek, N.; Briel, M.; Schindler, C.; Rasch, H.; Mäcke, H.R.; Rochlitz, C.; Müller-Brand, J.; Walter, M.A. Response, survival, and long-term toxicity after therapy with the radiolabeled somatostatin analogue [90Y-DOTA]-TOC in metastasized neuroendocrine cancers. J. Clin. Oncol. 2011, 29, 2416–2423. [Google Scholar] [CrossRef] [PubMed]
- Sierra, M.L.; Agazzi, A.; Bodei, L.; Pacifici, M.; Arico, D.; De Cicco, C.; Quarna, J.; Sansovini, M.; De Simone, M.; Paganelli, G. Lymphocytic toxicity in patients after peptide-receptor radionuclide therapy (PRRT) with 177Lu-DOTATATE and 90Y-DOTATOC. Cancer Biother. Radiopharm. 2009, 24, 659–665. [Google Scholar] [CrossRef] [PubMed]
- van Buuren, S.; Groothuis-Oudshoorn, K. mice: Multivariate imputation by chained equations in R. J. Stat. Softw. 2011, 45, 1–67. [Google Scholar] [CrossRef] [Green Version]
- Hurley, M.A. A reference relative time-scale as an alternative to chronological age for cohorts with long follow-up. Emerg. Themes Epidemiol. 2015, 12, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stare, J.; Henderson, R.; Perme, M. An individual measure of relative survival. J. R. Stat. Soc. Ser. C 2005, 54, 115–126. [Google Scholar] [CrossRef] [Green Version]
- Hallet, J.; Law, C.H.; Cukier, M.; Saskin, R.; Liu, N.; Singh, S. Exploring the rising incidence of neuroendocrine tumors: A population-based analysis of epidemiology, metastatic presentation, and outcomes. Cancer 2015, 121, 589–597. [Google Scholar] [CrossRef] [PubMed]
- Plante, A.; Baudin, E.; Do Cao, C.; Hentic, O.; Dubreuil, O.; Terrebonne, E.; Granger, V.; Smith, D.; Lombard-Bohas, C.; Walter, T. Patient-reported tolerance in treatments approved in neuroendocrine tumors: A national survey from the French Group of Endocrine Tumors. Clin. Res. Hepatol. Gastroenterol. 2018, 42, 153–159. [Google Scholar] [CrossRef] [PubMed]
- Kwekkeboom, D.K.; de Herder, W.W.; Kam, B.L.; van Eijck, C.H.; van Essen, M.; Kooij, P.P.; Feelders, R.A.; van Aken, M.O.; Krenning, E.P. Treatment With the Radiolabeled Somatostatin Analog [177Lu-DOTA0,Tyr3]Octreotate: Toxicity, Efficacy, and Survival. J. Clin. Oncol. 2008, 26, 2124–2130. [Google Scholar] [CrossRef] [Green Version]
- Ambrosini, V.; Kunikowska, J.; Baudin, E.; Bodei, L.; Bouvier, C.; Capdevila, J.; Cremonesi, M.; de Herder, W.W.; Dromain, C.; Falconi, M.; et al. Consensus on molecular imaging and theranostics in neuroendocrine neoplasms. Eur. J. Cancer 2021, 146, 56–73. [Google Scholar] [CrossRef] [PubMed]
- Liberini, V.; Huellner, M.W.; Grimaldis, S.; Finessi, M.; Thuillier, P.; Muni, A.; Pellerito, R.E.; Papotti, M.G.; Piovesan, A.; Arvat, E.; et al. The Challenge of Evaluating Response to Peptide Receptor Radionuclide Therapy in Gastroenteropancreatic Neuroendocrine Tumors: The Present and the Future. Diagnostics 2020, 10, 1083. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristic | Elderly Cohort (N = 48) | Younger Cohort (N = 68) |
|---|---|---|
| Age—years | 81.7 ± 1.5 | 67.6 ± 1.7 |
| Range—years | 79–86 | 60–70 |
| Sex—no. (%) | ||
| Male | 26 (54) | 38 (56) |
| Female | 22 (46) | 30 (44) |
| Median time since diagnosis—y | 4.3 ± 4.8 | 4.2 ± 6.0 |
| Primary tumour site—no. (%) | ||
| Midgut | 21 (44) | 28 (41) |
| Hindgut | 3 (6) | 3 (4) |
| Pancreas | 11 (23) | 19 (28) |
| Lungs | 6 (13) | 7 (10) |
| Unknown | 7 (15) | 11 (16) |
| Hormonal secretion—no. (%) | ||
| Functional | 11 (23) | 17 (25) |
| Non-functional | 37 (77) | 51 (75) |
| Tumor grade—no. (%) | ||
| Grade 1 | 29 (60) | 37 (54) |
| Grade 2 | 19 (40) | 31 (46) |
| Metastasis—no. (%) | 48 (100) | 68 (100) |
| Site of metastasis—no. (%) | ||
| Liver | 39 (81) | 65 (96) |
| Lymph nodes | 22 (46) | 30 (44) |
| Bone | 21 (44) | 19 (28) |
| Peritoneum | 11 (23) | 6 (9) |
| Others | 8 (17) | 8 (12) |
| PRRT cycles—no. (per patient) | 139 (2.9) | 211 (3.1) |
| 177lutetium—no. (%) | 107 (77) | 148 (70) |
| 90yttrium—no. (%) | 32 (23) | 63 (30) |
| Retreatment—no. (%) ** | 14 (29) | 17 (25) |
| Characteristic | Elderly Cohort (N = 48) | Younger Cohort (N = 68) |
|---|---|---|
| Pretreatment—no. (%) | ||
| PRRT | 14 (29) | 17 (25) |
| Surgery | 21 (44) | 28 (41) |
| Local ablative treatments | 5 (10) | 5 (7) |
| Chemotherapy | 6 (13) | 12 (18) |
| Radiotherapy | 1 (2) | 3 (4) |
| Targeted therapies | 5 (10) | 5 (7) |
| Other biotherapies | 0 (0) | 2 (3) |
| Somatostatin analogues | 16 (33) | 43 (63) |
| Comorbidities—no. (%) | ||
| Cardiovascular | 32 (67) | 31 (46) |
| Renal insufficiency ** | 15 (31) | 9 (13) |
| Diabetes | 10 (21) | 16 (24) |
| Neurological | 6 (13) | 0 (0) |
| Other tumors | 9 (19) | 10 (15) |
| WHO/ECOG Performance Status—no. (%) | ||
| <2 | 38 (79) | 60 (88) |
| =2 | 10 (21) | 8 (12) |
| Laboratory Parameters | Elderly Cohort (N = 48 **) | Younger Cohort (N = 68 **) | Estimated Differences | 95% CI | p |
|---|---|---|---|---|---|
| Haemoglobin [g/L] | 126 ± 15 | 133 ± 12 | −7.30 | [−12.12, −2.47] | 0.003 |
| Thrombocytes [×109/L] | 249 ± 73 | 272 ± 85 | −23.74 | [−52.50, 5.01] | 0.106 |
| Leucocytes [×109/L] | 6.73 ± 1.61 | 7.60 ± 2.23 | −0.87 | [−1.61, −0.13] | 0.022 |
| Neutrophil granulocytes [×109/L] | 4.68 ± 1.53 | 5.32 ± 1.98 | −0.64 | [−1.32, 0.05] | 0.070 |
| Lymphocytes [×109/L] | 1.31 ± 0.54 | 1.49 ± 0.54 | −0.19 | [−0.37, −0.02] | 0.032 |
| eGFR (CKD-EPI) [mL/min/1.73 m2] | 61 ± 16 | 78 ± 19 | −17.70 | [−24.43, −10.97] | <0.001 |
| CTCAE ≥ 3 | CTCAE Δ ≥ 2 | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Elderly Cohort | Younger Cohort | OR | 95% CI | Elderly Cohort | Younger Cohort | OR | 95% CI | |||||
| Total No. of Events | % per PRRT Cycle | Total No. of Events | % per PRRT Cycle | Total No. of Events | % per PRRT Cycle | Total No. of Events | % per PRRT Cycle | |||||
| Anaemia | 1 | 0.8 | 1 | 0.5 | 1.58 | [0.10, 25.42] | 1 | 0.8 | 4 | 2.0 | 0.39 | [0.04, 3.51] |
| Thrombocytopenia | 0 | 0.0 | 5 | 2.5 | 0.00 | [0.00, Inf] | 2 | 1.6 | 6 | 3.0 | 0.70 | [0.01, 90.86] |
| Leukopenia | 1 | 0.8 | 4 | 2.0 | 0.45 | [0.00, 850.63] | 11 | 8.7 | 17 | 8.6 | 1.01 | [0.32, 3.23] |
| Neutropenia | 1 | 0.9 | 2 | 1.1 | 0.82 | [0.00, 127,175.27] | 8 | 7.3 | 9 | 4.9 | 1.43 | [0.05, 39.59] |
| Lymphopenia | 27 | 25.0 | 36 | 19.9 | 1.46 | [0.59, 3.64] | 32 | 29.6 | 52 | 28.7 | 1.05 | [0.60, 1.84] |
| Kidney disease | 6 | 4.9 | 2 | 1.0 | 7.05 | [0.02, 3213.47] | ||||||
| CTCAE ≥ 3 | CTCAE Δ ≥ 2 | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Elderly Cohort | Younger Cohort | OR | 95% CI | Elderly Cohort | Younger Cohort | OR | 95% CI | |||||
| Total No. of Events | % per Patient | Total No. of Events | % per Patient | Total No. of Events | % per Patient | Total No. of Events | % per Patient | |||||
| Anaemia | 0 | 0.0 | 0 | 0.0 | 1.00 | [0.00, Inf] | 5 | 14.3 | 5 | 11.6 | 1.27 | [0.34, 4.78] |
| Thrombocytopenia | 2 | 5.7 | 0 | 0.0 | Inf | [0.00, Inf] | 2 | 5.7 | 1 | 2.3 | 2.55 | [0.22, 29.30] |
| Leukopenia | 0 | 0.0 | 1 | 2.3 | 0.00 | [0.00, Inf] | 0 | 0.0 | 1 | 2.3 | 0.00 | [0.00, Inf] |
| Neutropenia | 0 | 0.0 | 1 | 2.5 | 0.00 | [0.00, Inf] | 0 | 0.0 | 1 | 2.5 | 0.00 | [0.00, Inf] |
| Lymphopenia | 6 | 18.2 | 3 | 7.5 | 2.74 | [0.63, 11.94] | 11 | 33.3 | 9 | 22.5 | 1.65 | [0.58, 4.73] |
| Kidney disease | 7 | 20.0 | 2 | 4.5 | 5.25 | [1.02, 27.14] | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Theiler, D.; Cattaneo, M.; Dierickx, L.O.; Igaz, P.; Grozinsky-Glasberg, S.; Bournaud, C.; O’Dorisio, T.; O’Dorisio, M.S.; Wild, D.; Christ, E.; et al. Safety and Efficacy of Peptide-Receptor Radionuclide Therapy in Elderly Neuroendocrine Tumor Patients. Cancers 2021, 13, 6290. https://doi.org/10.3390/cancers13246290
Theiler D, Cattaneo M, Dierickx LO, Igaz P, Grozinsky-Glasberg S, Bournaud C, O’Dorisio T, O’Dorisio MS, Wild D, Christ E, et al. Safety and Efficacy of Peptide-Receptor Radionuclide Therapy in Elderly Neuroendocrine Tumor Patients. Cancers. 2021; 13(24):6290. https://doi.org/10.3390/cancers13246290
Chicago/Turabian StyleTheiler, Deborah, Marco Cattaneo, Lawrence O. Dierickx, Peter Igaz, Simona Grozinsky-Glasberg, Claire Bournaud, Thomas O’Dorisio, M. Sue O’Dorisio, Damian Wild, Emanuel Christ, and et al. 2021. "Safety and Efficacy of Peptide-Receptor Radionuclide Therapy in Elderly Neuroendocrine Tumor Patients" Cancers 13, no. 24: 6290. https://doi.org/10.3390/cancers13246290
APA StyleTheiler, D., Cattaneo, M., Dierickx, L. O., Igaz, P., Grozinsky-Glasberg, S., Bournaud, C., O’Dorisio, T., O’Dorisio, M. S., Wild, D., Christ, E., & Nicolas, G. P. (2021). Safety and Efficacy of Peptide-Receptor Radionuclide Therapy in Elderly Neuroendocrine Tumor Patients. Cancers, 13(24), 6290. https://doi.org/10.3390/cancers13246290