Radiomics Features of 18F-Fluorodeoxyglucose Positron-Emission Tomography as a Novel Prognostic Signature in Colorectal Cancer

 , , , , ,
, , , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. PET/CT Protocol
2.3. Feature Extraction for Radiomics Analysis
2.4. Feature Selection, Building of Rad_Score, and Validation
2.5. Development and Validation of the Radiomics Nomogram
2.6. Statistical Analysis
3. Results
3.1. Patient Characteristics
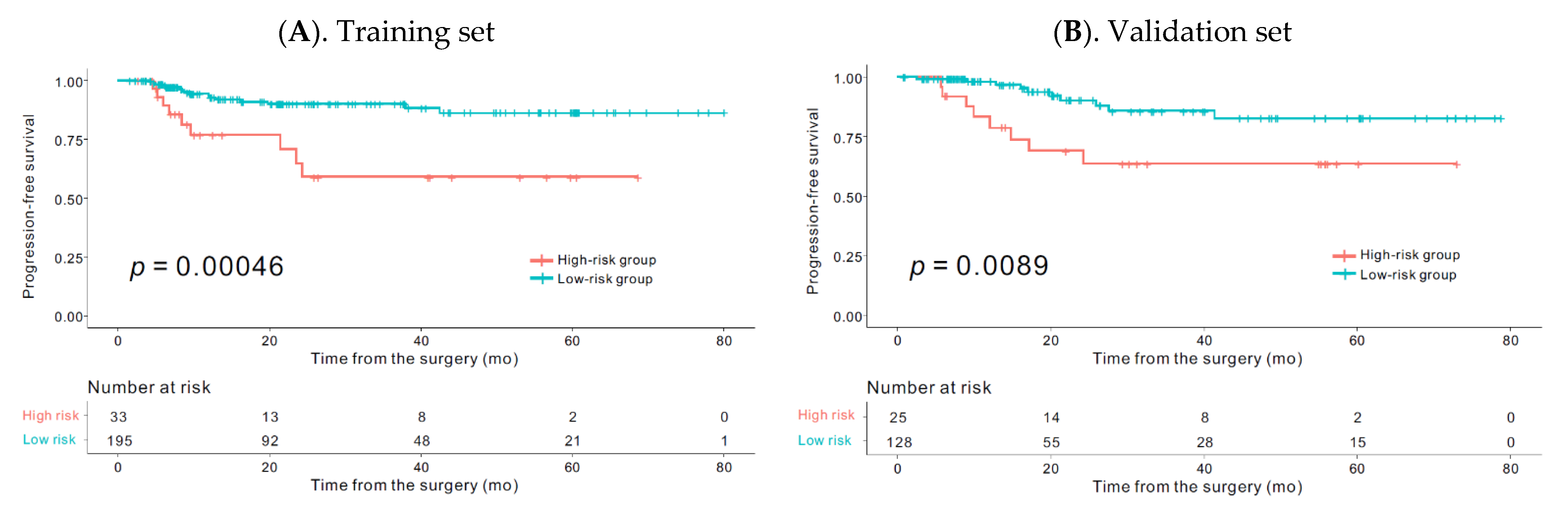
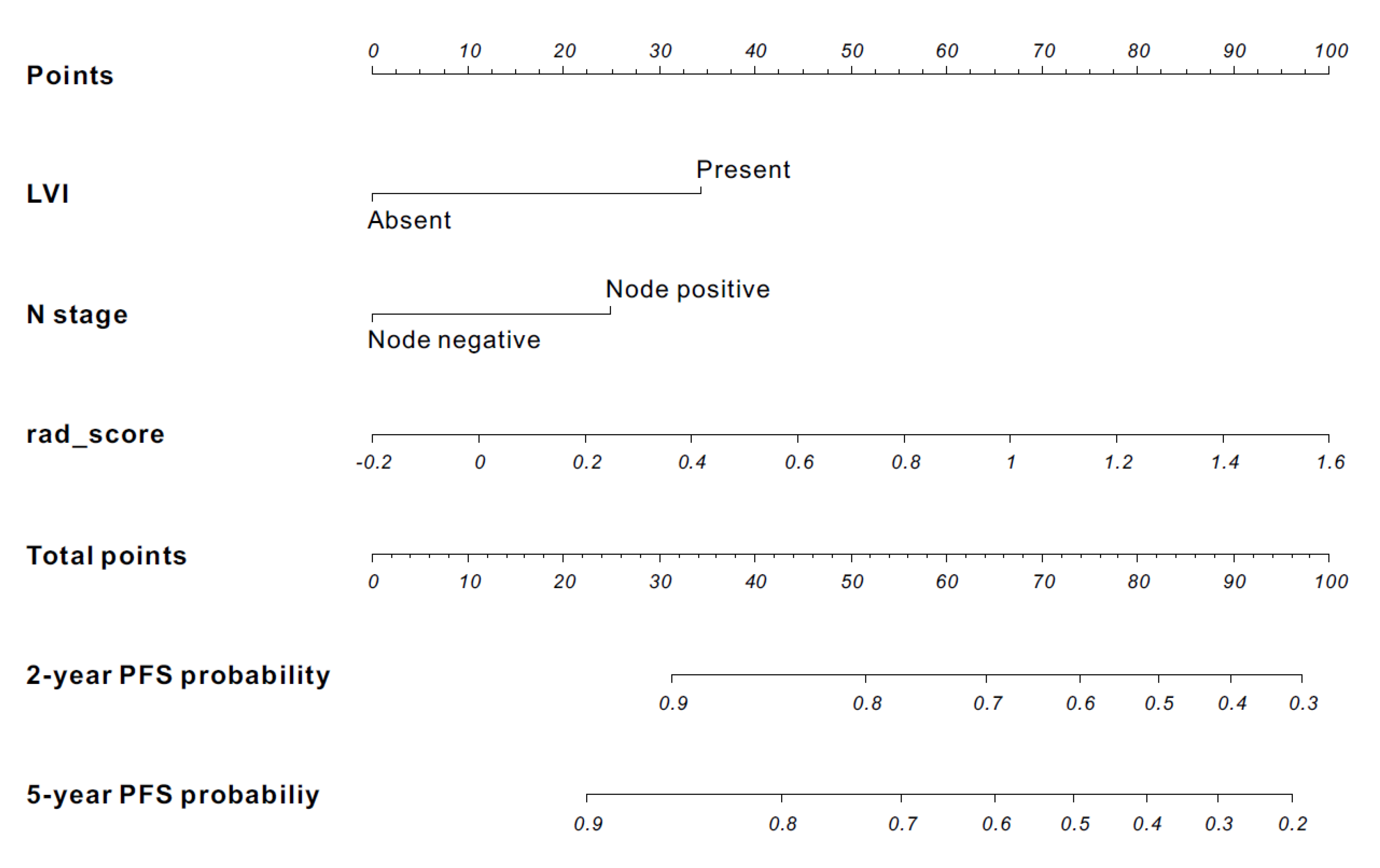
3.2. Radiomics Signature-Based Prediction Model
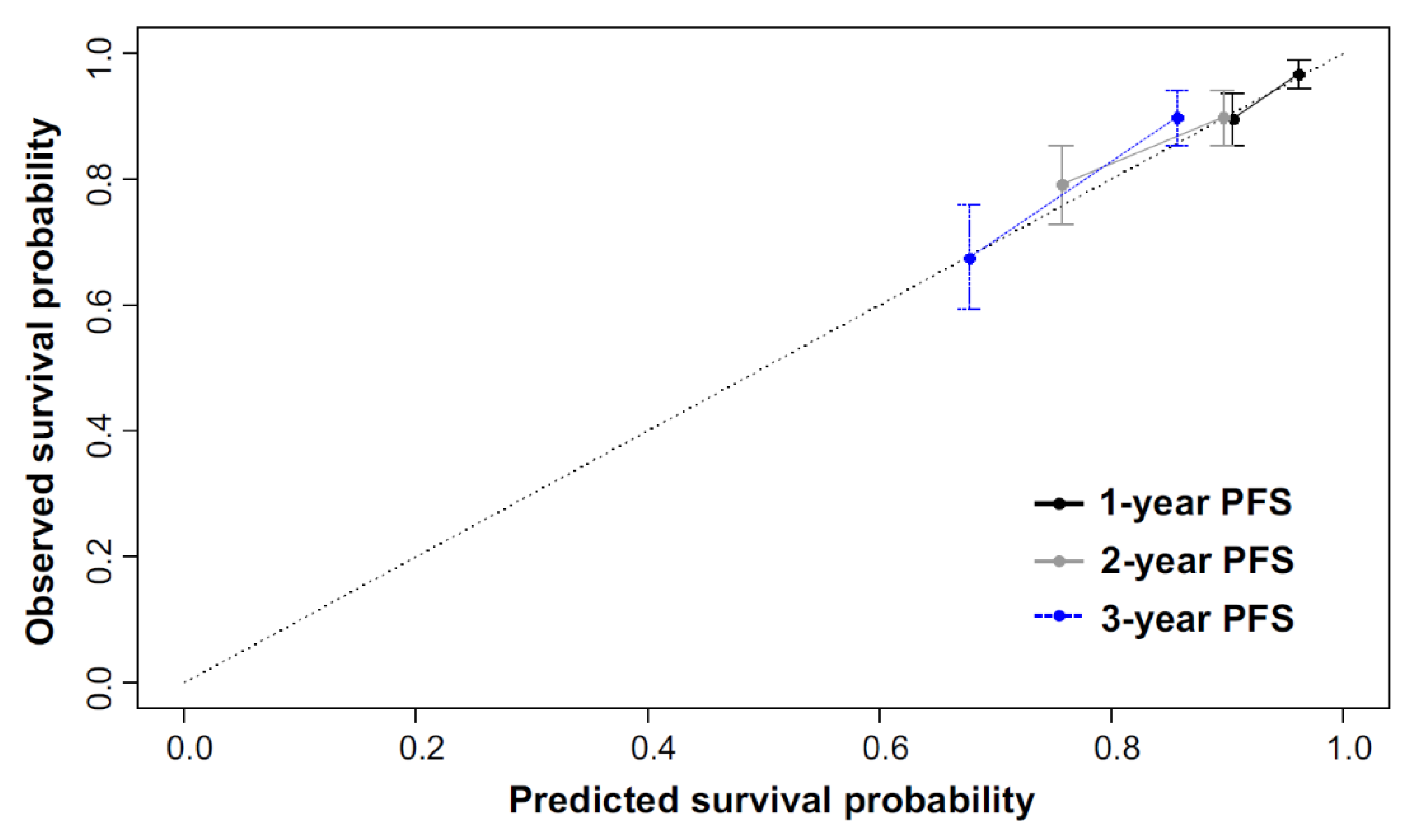
3.3. Calibration and Discriminative Performance Measurement of the Radiomics Nomogram
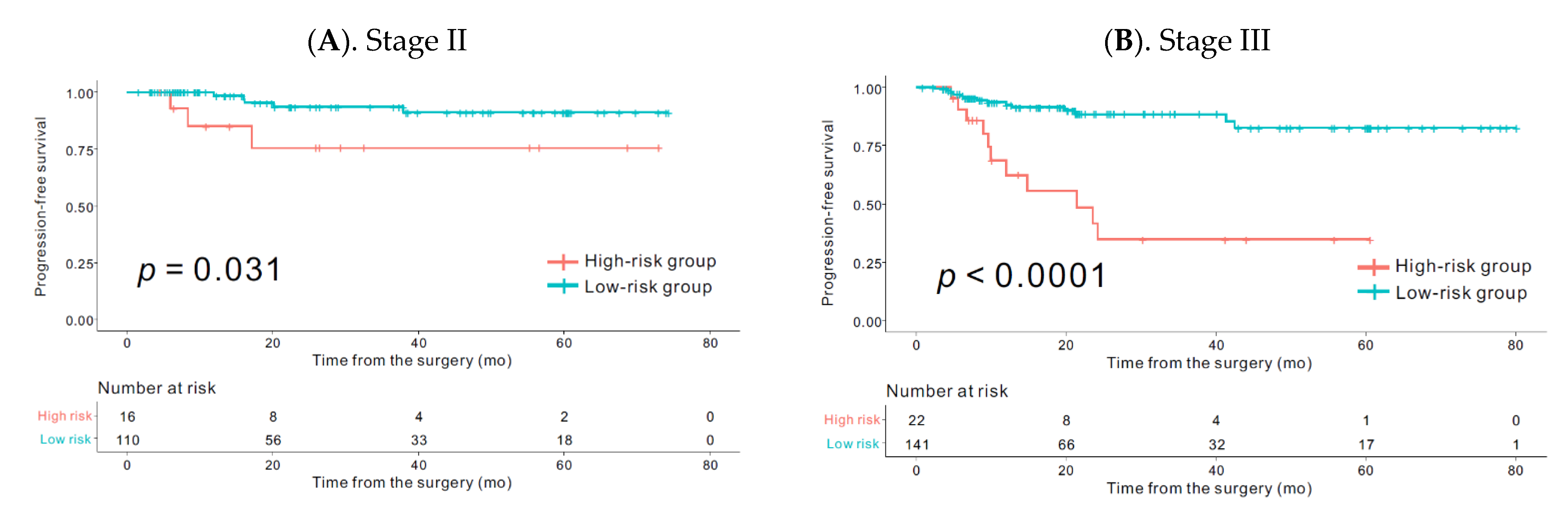
3.4. Comparison of Survival within the Same Stages According to the Rad_Score
3.5. Correlation between Rad_Score and PET Derived Conventional Parameters such as SUVmax, TLG, and MTV
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Torre, L.A.; Bray, F.; Siegel, R.L.; Ferlay, J.; Lortet-Tieulent, J.; Jemal, A. Global cancer statistics, 2012. CA Cancer J. Clin. 2015, 65, 87–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, D.; Cai, G.; Peng, J.; Li, D.; Li, X.; Xu, Y.; Cai, S. The preoperative suvmax for (18)f-fdg uptake predicts survival in patients with colorectal cancer. BMC Cancer 2015, 15, 991. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suzuki, Y.; Okabayashi, K.; Hasegawa, H.; Tsuruta, M.; Shigeta, K.; Murakami, K.; Kitagawa, Y. Metabolic tumor volume and total lesion glycolysis in pet/ct correlate with the pathological findings of colorectal cancer and allow its accurate staging. Clin. Nucl. Med. 2016, 41, 761–765. [Google Scholar] [CrossRef] [PubMed]
- Woff, E.; Hendlisz, A.; Ameye, L.; Garcia, C.; Kamoun, T.; Guiot, T.; Paesmans, M.; Flamen, P. Metabolic active tumor volume and total lesion glycolysis by (18)f-fdg pet/ct validated as prognostic imaging biomarkers in chemorefractory metastatic colorectal cancer. J. Nucl. Med. 2018. [Google Scholar] [CrossRef] [Green Version]
- Lim, Y.; Bang, J.I.; Han, S.W.; Paeng, J.C.; Lee, K.H.; Kim, J.H.; Kang, G.H.; Jeong, S.Y.; Park, K.J.; Kim, T.Y. Total lesion glycolysis (tlg) as an imaging biomarker in metastatic colorectal cancer patients treated with regorafenib. Eur. J. Nucl. Med. Mol. Imag. 2017, 44, 757–764. [Google Scholar] [CrossRef]
- Huang, J.; Huang, L.; Zhou, J.; Duan, Y.; Zhang, Z.; Wang, X.; Huang, P.; Tan, S.; Hu, P.; Wang, J.; et al. Elevated tumor-to-liver uptake ratio (tlr) from (18)f-fdg-pet/ct predicts poor prognosis in stage iia colorectal cancer following curative resection. Eur. J. Nucl. Med. Mol. Imag. 2017, 44, 1958–1968. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.E.; Kim, S.W.; Kim, J.S.; Choi, K.Y.; Kang, W.K.; Oh, S.T.; Yoo Ie, R.; Kim, S.H. Prognostic value of 18-fluorodeoxyglucose positron emission tomography-computed tomography in resectable colorectal cancer. World J. Gastroenterol. 2012, 18, 5072–5077. [Google Scholar] [CrossRef]
- NCCN Guidelines®. National Comprehensive Cancer Network (nccn) Guidelines for Treatment of Cancer by Site. Available online: https://www.nccn.org/professionals/physician_gls/default.aspx (accessed on 30 June 2019).
- Huang, Y.Q.; Liang, C.H.; He, L.; Tian, J.; Liang, C.S.; Chen, X.; Ma, Z.L.; Liu, Z.Y. Development and validation of a radiomics nomogram for preoperative prediction of lymph node metastasis in colorectal cancer. J. Clin. Oncol. 2016, 34, 2157–2164. [Google Scholar] [CrossRef]
- Wu, S.; Zheng, J.; Li, Y.; Yu, H.; Shi, S.; Xie, W.; Liu, H.; Su, Y.; Huang, J.; Lin, T. A radiomics nomogram for the preoperative prediction of lymph node metastasis in bladder cancer. Clin. Cancer Res. 2017, 23, 6904–6911. [Google Scholar] [CrossRef] [Green Version]
- Antunovic, L.; De Sanctis, R.; Cozzi, L.; Kirienko, M.; Sagona, A.; Torrisi, R.; Tinterri, C.; Santoro, A.; Chiti, A.; Zelic, R.; et al. Pet/ct radiomics in breast cancer: Promising tool for prediction of pathological response to neoadjuvant chemotherapy. Eur. J. Nucl. Med. Mol. Imag. 2019, 46, 1468–1477. [Google Scholar] [CrossRef]
- Beukinga, R.J.; Hulshoff, J.B.; Mul, V.E.M.; Noordzij, W.; Kats-Ugurlu, G.; Slart, R.; Plukker, J.T.M. Prediction of response to neoadjuvant chemotherapy and radiation therapy with baseline and restaging (18)f-fdg pet imaging biomarkers in patients with esophageal cancer. Radiology 2018, 287, 983–992. [Google Scholar] [CrossRef] [Green Version]
- Andor, N.; Graham, T.A.; Jansen, M.; Xia, L.C.; Aktipis, C.A.; Petritsch, C.; Ji, H.P.; Maley, C.C. Pan-cancer analysis of the extent and consequences of intratumor heterogeneity. Nat. Med. 2016, 22, 105–113. [Google Scholar] [CrossRef]
- Sagaert, X.; Vanstapel, A.; Verbeek, S. Tumor heterogeneity in colorectal cancer: What do we know so far? Pathobiology 2018, 85, 72–84. [Google Scholar] [CrossRef] [PubMed]
- Nelson, A.C.; Boone, J.; Cartwright, D.; Thyagarajan, B.; Kincaid, R.; Lambert, A.P.; Karnuth, K.; Henzler, C.; Yohe, S. Optimal detection of clinically relevant mutations in colorectal carcinoma: Sample pooling overcomes intra-tumoral heterogeneity. Mod. Pathol. 2018, 31, 343–349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davnall, F.; Yip, C.S.; Ljungqvist, G.; Selmi, M.; Ng, F.; Sanghera, B.; Ganeshan, B.; Miles, K.A.; Cook, G.J.; Goh, V. Assessment of tumor heterogeneity: An emerging imaging tool for clinical practice? Insights Imag. 2012, 3, 573–589. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bundschuh, R.A.; Dinges, J.; Neumann, L.; Seyfried, M.; Zsoter, N.; Papp, L.; Rosenberg, R.; Becker, K.; Astner, S.T.; Henninger, M.; et al. Textural parameters of tumor heterogeneity in (1)(8)f-fdg pet/ct for therapy response assessment and prognosis in patients with locally advanced rectal cancer. J. Nucl. Med. 2014, 55, 891–897. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bang, J.I.; Ha, S.; Kang, S.B.; Lee, K.W.; Lee, H.S.; Kim, J.S.; Oh, H.K.; Lee, H.Y.; Kim, S.E. Prediction of neoadjuvant radiation chemotherapy response and survival using pretreatment [(18)f]fdg pet/ct scans in locally advanced rectal cancer. Eur. J. Nucl. Med. Mol. Imag. 2016, 43, 422–431. [Google Scholar] [CrossRef] [PubMed]
- Lovinfosse, P.; Polus, M.; Van Daele, D.; Martinive, P.; Daenen, F.; Hatt, M.; Visvikis, D.; Koopmansch, B.; Lambert, F.; Coimbra, C.; et al. Fdg pet/ct radiomics for predicting the outcome of locally advanced rectal cancer. Eur. J. Nucl. Med. Mol. Imag. 2018, 45, 365–375. [Google Scholar] [CrossRef]
- Giannini, V.; Mazzetti, S.; Bertotto, I.; Chiarenza, C.; Cauda, S.; Delmastro, E.; Bracco, C.; Di Dia, A.; Leone, F.; Medico, E.; et al. Predicting locally advanced rectal cancer response to neoadjuvant therapy with (18)f-fdg pet and mri radiomics features. Eur. J. Nucl. Med. Mol. Imag. 2019, 46, 878–888. [Google Scholar] [CrossRef]
- Soret, M.; Bacharach, S.L.; Buvat, I. Partial-volume effect in pet tumor imaging. J. Nucl. Med. 2007, 48, 932–945. [Google Scholar] [CrossRef] [Green Version]
- Orlhac, F.; Soussan, M.; Maisonobe, J.A.; Garcia, C.A.; Vanderlinden, B.; Buvat, I. Tumor texture analysis in 18f-fdg pet: Relationships between texture parameters, histogram indices, standardized uptake values, metabolic volumes, and total lesion glycolysis. J. Nucl. Med. 2014, 55, 414–422. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nioche, C.; Orlhac, F.; Boughdad, S.; Reuze, S.; Goya-Outi, J.; Robert, C.; Pellot-Barakat, C.; Soussan, M.; Frouin, F.; Buvat, I. Lifex: A freeware for radiomic feature calculation in multimodality imaging to accelerate advances in the characterization of tumor heterogeneity. Cancer Res. 2018, 78, 4786–4789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tibshirani, R. The lasso method for variable selection in the cox model. Statist. Med. 1997, 16, 385–395. [Google Scholar] [CrossRef] [Green Version]
- Camp, R.L.; Dolled-Filhart, M.; Rimm, D.L. X-tile: A new bio-informatics tool for biomarker assessment and outcome-based cut-point optimization. Clin. Cancer Res. 2004, 10, 7252–7259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akaike, H. Information theory and an extension of the maximum likelihood principle. In Selected Papers of Hirotugu Akaike; Springer: Berlin/Heidelberg, Germany, 1998; pp. 199–213. [Google Scholar]
- Harrell, F.E., Jr.; Lee, K.L.; Mark, D.B. Multivariable prognostic models: Issues in developing models, evaluating assumptions and adequacy, and measuring and reducing errors. Statist. Med. 1996, 15, 361–387. [Google Scholar] [CrossRef]
- Jiang, Y.; Yuan, Q.; Lv, W.; Xi, S.; Huang, W.; Sun, Z.; Chen, H.; Zhao, L.; Liu, W.; Hu, Y.; et al. Radiomic signature of (18)f fluorodeoxyglucose pet/ct for prediction of gastric cancer survival and chemotherapeutic benefits. Theranostics 2018, 8, 5915–5928. [Google Scholar] [CrossRef]
- Huang, Y.; Liu, Z.; He, L.; Chen, X.; Pan, D.; Ma, Z.; Liang, C.; Tian, J.; Liang, C. Radiomics signature: A potential biomarker for the prediction of disease-free survival in early-stage (i or ii) non-small cell lung cancer. Radiology 2016, 281, 947–957. [Google Scholar] [CrossRef]
- Park, H.; Lim, Y.; Ko, E.S.; Cho, H.H.; Lee, J.E.; Han, B.K.; Ko, E.Y.; Choi, J.S.; Park, K.W. Radiomics signature on magnetic resonance imaging: Association with disease-free survival in patients with invasive breast cancer. Clin. Cancer Res. 2018, 24, 4705–4714. [Google Scholar] [CrossRef] [Green Version]
- Huh, J.W.; Lee, W.Y.; Shin, J.K.; Park, Y.A.; Cho, Y.B.; Kim, H.C.; Yun, S.H. A novel histologic grading system based on lymphovascular invasion, perineural invasion, and tumor budding in colorectal cancer. J. Cancer Res. Clin. Oncol. 2019, 145, 471–477. [Google Scholar] [CrossRef]
- Nikberg, M.; Chabok, A.; Letocha, H.; Kindler, C.; Glimelius, B.; Smedh, K. Lymphovascular and perineural invasion in stage ii rectal cancer: A report from the swedish colorectal cancer registry. Acta Oncol. 2016, 55, 1418–1424. [Google Scholar] [CrossRef] [Green Version]
- Yuan, H.; Dong, Q.; Zheng, B.; Hu, X.; Xu, J.B.; Tu, S. Lymphovascular invasion is a high risk factor for stage i/ii colorectal cancer: A systematic review and meta-analysis. Oncotarget 2017, 8, 46565–46579. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, J.; Guo, B.C.; Sun, L.R.; Wang, J.W.; Fu, X.H.; Zhang, S.Z.; Poston, G.; Ding, K.F. Tnm staging of colorectal cancer should be reconsidered by t stage weighting. World J. Gastroenterol. 2014, 20, 5104–5112. [Google Scholar] [CrossRef]
- Pages, F.; Mlecnik, B.; Marliot, F.; Bindea, G.; Ou, F.S.; Bifulco, C.; Lugli, A.; Zlobec, I.; Rau, T.T.; Berger, M.D.; et al. International validation of the consensus immunoscore for the classification of colon cancer: A prognostic and accuracy study. Lancet 2018, 391, 2128–2139. [Google Scholar] [CrossRef]
- Norcic, G. Liquid biopsy in colorectal cancer-current status and potential clinical applications. Micromachines 2018, 9, 300. [Google Scholar] [CrossRef] [Green Version]
- Reinert, T.; Scholer, L.V.; Thomsen, R.; Tobiasen, H.; Vang, S.; Nordentoft, I.; Lamy, P.; Kannerup, A.S.; Mortensen, F.V.; Stribolt, K.; et al. Analysis of circulating tumour DNA to monitor disease burden following colorectal cancer surgery. Gut 2016, 65, 625–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.; Li, L.; Cohen, J.D.; Kinde, I.; Ptak, J.; Popoli, M.; Schaefer, J.; Silliman, N.; Dobbyn, L.; Tie, J.; et al. Prognostic potential of circulating tumor DNA measurement in postoperative surveillance of nonmetastatic colorectal cancer. JAMA Oncol. 2019. [Google Scholar] [CrossRef] [PubMed]
- Reinert, T.; Henriksen, T.V.; Christensen, E.; Sharma, S.; Salari, R.; Sethi, H.; Knudsen, M.; Nordentoft, I.; Wu, H.T.; Tin, A.S.; et al. Analysis of plasma cell-free DNA by ultradeep sequencing in patients with stages i to iii colorectal cancer. JAMA Oncol. 2019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foxtrot Collaborative, G. Feasibility of preoperative chemotherapy for locally advanced, operable colon cancer: The pilot phase of a randomised controlled trial. Lancet Oncol. 2012, 13, 1152–1160. [Google Scholar] [CrossRef] [Green Version]
- Dehal, A.; Graff-Baker, A.N.; Vuong, B.; Fischer, T.; Klempner, S.J.; Chang, S.C.; Grunkemeier, G.L.; Bilchik, A.J.; Goldfarb, M. Neoadjuvant chemotherapy improves survival in patients with clinical t4b colon cancer. J. Gastrointestin. Surg. 2018, 22, 242–249. [Google Scholar] [CrossRef]
- Sollini, M.; Antunovic, L.; Chiti, A.; Kirienko, M. Towards clinical application of image mining: A systematic review on artificial intelligence and radiomics. Eur. J. Nucl. Med. Mol. Imag. 2019. [Google Scholar] [CrossRef] [Green Version]
- Van Helden, E.J.; Vacher, Y.J.L.; van Wieringen, W.N.; van Velden, F.H.P.; Verheul, H.M.W.; Hoekstra, O.S.; Boellaard, R.; Menke-van der Houven van Oordt, C.W. Radiomics analysis of pre-treatment [(18)f]fdg pet/ct for patients with metastatic colorectal cancer undergoing palliative systemic treatment. Eur. J. Nucl. Med. Mol. Imag. 2018, 45, 2307–2317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yan, J.; Chu-Shern, J.L.; Loi, H.Y.; Khor, L.K.; Sinha, A.K.; Quek, S.T.; Tham, I.W.; Townsend, D. Impact of image reconstruction settings on texture features in 18f-fdg pet. J. Nucl. Med. 2015, 56, 1667–1673. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papp, L.; Rausch, I.; Grahovac, M.; Hacker, M.; Beyer, T. Optimized feature extraction for radiomics analysis of (18)f-fdg pet imaging. J. Nucl. Med. 2019, 60, 864–872. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shiri, I.; Rahmim, A.; Ghaffarian, P.; Geramifar, P.; Abdollahi, H.; Bitarafan-Rajabi, A. The impact of image reconstruction settings on 18f-fdg pet radiomic features: Multi-scanner phantom and patient studies. Eur. Radiol. 2017, 27, 4498–4509. [Google Scholar] [CrossRef] [PubMed]
- Sveen, A.; Kopetz, S.; Lothe, R.A. Biomarker-guided therapy for colorectal cancer: Strength in complexity. Nat. Rev. Clin. Oncol. 2019. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Subcategory | Training Set (n = 228) n (%) | Validation Set (n = 153) n (%) | p |
|---|---|---|---|---|
| Sex | Male | 132 (57.9) | 92 (60.1) | 0.743 |
| Female | 96 (42.1) | 61 (39.9) | ||
| Age (years) | <70 | 156 (68.4) | 107 (69.9) | 0.841 |
| ≥70 | 72 (31.6) | 46 (30.1) | ||
| ASA | 1 | 110 (48.2) | 72 (47.1) | 0.163 |
| 2 | 88 (38.6) | 62 (40.5) | ||
| 3 | 30 (13.2) | 19 (12.4) | ||
| BMI (kg/m2) | <25 | 161 (70.6) | 115 (75.2) | 0.391 |
| ≥25 | 67 (29.4) | 38 (24.8) | ||
| Preop CEA (ng/mL) | <5 | 147 (64.5) | 100 (65.4) | 0.946 |
| ≥5 | 81 (35.5) | 53 (34.6) | ||
| Tumor location | Colon | 165 (72.4) | 117 (76.5) | 0.438 |
| Rectum | 63 (27.6) | 36 (23.5) | ||
| Complications | No | 178 (78.1) | 127 (83) | 0.293 |
| Yes | 50 (21.9) | 26 (17) | ||
| Histologic grade | G1 | 23 (10.1) | 14 (9.2) | 0.936 |
| G2 | 186 (81.6) | 127 (83) | ||
| G3 and Mucinous | 19 (8.3) | 12 (7.8) | ||
| LVI | Absent | 175 (76.8) | 98 (64.1) | 0.010 |
| Present | 53 (23.2) | 55 (35.9) | ||
| No. of Retrieved LNs | (Mean ± SD) | 26.7 ± 16.7 | 25.5 ± 16.7 | 0.495 |
| LN numbers | <12 | 25 (11) | 20 (13.1) | 0.644 |
| ≥12 | 203 (89) | 133 (86.9) | ||
| pT a | T1–T2 | 39 (17.1) | 24 (15.7) | 0.504 |
| T3 | 156 (68.4) | 100 (65.4) | ||
| T4 | 33 (14.5) | 29 (19) | ||
| pN b | Negative | 113 (49.6) | 64 (41.8) | 0.168 |
| Positive | 115 (50.4) | 89 (58.2) | ||
| AJCC Stage c | I | 30 (13.2) | 14 (9.2) | 0.626 |
| II | 77 (33.8) | 50 (32.7) | ||
| III | 93 (40.8) | 69 (45.1) | ||
| IV | 28 (12.3) | 20 (13.1) | ||
| Distant metastasis | No | 200 (87.7) | 133 (86.9) | 0.944 |
| Yes | 28 (12.3) | 20 (13.1) | ||
| MSI | MSS/MSI-Low | 138 (60.5) | 102 (66.7) | 0.371 |
| MSI-High | 15 (6.6) | 11 (7.2) | ||
| No data | 75 (32.9) | 40 (26.1) | ||
| KRAS | Wild | 72 (31.6) | 53 (34.6) | 0.794 |
| Mutant | 35 (15.4) | 21 (13.7) | ||
| No data | 121 (53.1) | 79 (51.6) | ||
| Postoperative chemotherapy | No | 84 (36.8) | 61 (39.9) | 0.625 |
| Yes | 144 (63.2) | 92 (60.1) | ||
| Radiotherapy | No | 212 (93) | 143 (93.5) | >0.99 |
| Preoperative or postoperative | 16 (7) | 10 (6.5) | ||
| rad_score | (Mean ± SD) | 0.0 ± 0.2 | 0.0 ± 0.1 | 0.867 d |
| Variables | Subcategory | Low-Risk Group (n = 195) n (%) | High-Risk Group (n = 33) n (%) | p |
|---|---|---|---|---|
| Sex | Male | 113 (57.9) | 19 (57.6) | >0.99 |
| Female | 82 (42.1) | 14 (39.9) | ||
| Age (years) | <70 | 132 (67.7) | 24 (72.7) | 0.709 |
| ≥70 | 63 (32.3) | 9 (27.3) | ||
| ASA | 1 | 91 (46.7) | 19 (57.6) | 0.482 |
| 2 | 77 (39.5) | 11 (33.3) | ||
| 3 | 27 (13.8) | 3 (9.1) | ||
| BMI (kg/m2) | <25 | 132 (67.7) | 29 (87.9) | 0.032 |
| ≥25 | 63 (32.3) | 4 (12.1) | ||
| Preop CEA (ng/mL) | <5 | 124 (63.6) | 23 (69.7) | 0.630 |
| ≥5 | 71 (36.4) | 10 (30.3) | ||
| Tumor location | Colon | 146 (74.9) | 19 (57.6) | 0.065 |
| Rectum | 49 (25.1) | 14 (42.4) | ||
| Complications | No | 155 (79.5) | 23 (69.7) | 0.303 |
| Yes | 40 (20.5) | 10 (30.3) | ||
| Histologic grade | G1 + G2 | 184 (94.4) | 25 (75.8) | 0.001 |
| G3 and Mucinous | 11 (5.6) | 8 (24.2) | ||
| LVI | Absent | 152 (77.9) | 23 (69.7) | 0.415 |
| Present | 43 (22.1) | 10 (30.3) | ||
| No. of Retrieved LNs | (Mean ± SD) | 26.8 ± 16.6 | 26.2 ± 17.3 | 0.846 |
| LN numbers | <12 | 18 (9.2) | 7 (21.2) | 0.083 |
| ≥12 | 177 (90.8) | 26 (78.8) | ||
| pT a | T1–T2 | 33 (16.9) | 6 (78.8) | 0.356 |
| T3 | 136 (69.7) | 20 (60.6) | ||
| T4 | 26 (13.3) | 7 (21.2) | ||
| pN b | Negative | 98 (50.3) | 15 (45.5) | 0.747 |
| Positive | 97 (49.7) | 18 (54.5) | ||
| AJCC Stage c | I | 26 (13.3) | 4 (12.1) | 0.386 |
| II | 68 (34.9) | 9 (27.3) | ||
| III | 80 (41) | 13 (39.4) | ||
| IV | 21 (10.8) | 7 (21.2) | ||
| Distant metastasis | No | 174 (89.2) | 26 (78.8) | 0.160 |
| Yes | 21 (10.8) | 7 (21.2) | ||
| MSI | MSS/MSI-Low | 117 (60) | 21 (63.6) | 0.669 |
| MSI-High | 14 (7.2) | 1 (3) | ||
| No data | 64 (32.8) | 11 (33.3) | ||
| KRAS | Wild | 63 (32.3) | 9 (27.3) | 0.829 |
| Mutant | 30 (15.4) | 5 (15.2) | ||
| No data | 102 (52.3) | 19 (57.6) | ||
| Postoperative chemotherapy | No | 73 (37.4) | 11 (33.3) | 0.797 |
| Yes | 122 (62.6) | 22 (66.7) | ||
| Radiotherapy | No | 187 (95.9) | 25 (75.8) | <0.001 |
| Preoperative or postoperative | 8 (4.1) | 8 (24.2) | ||
| rad_score | (Mean ± SD) | 0.0 ± 0.0 | 0.3 ± 0.3 | <0.001 d |
| Variables | Subcategory | Univariable Analysis | |
|---|---|---|---|
| HR (95% CI) | p | ||
| Sex | Female | Ref | |
| Male | 0.54 (0.24–1.2) | 0.136 | |
| Age (years) | <70 | Ref | |
| ≥70 | 0.88 (0.38–2.04) | 0.773 | |
| ASA | 1 & 2 | Ref | |
| 3 | 1.51 (0.44–5.07) | 0.505 | |
| BMI (kg/m2) | <25 | Ref | |
| ≥25 | 0.52 (0.19–1.39) | 0.193 | |
| Preop CEA (ng/mL) | <5 | Ref | |
| ≥5 | 1.3 (0.58–2.89) | 0.52 | |
| Tumor location | Colon | Ref | |
| Rectum | 1.87 (0.84–4.12) | 0.12 | |
| Complications | No | Ref | |
| Yes | 2.22 (0.98–5.04) | 0.055 | |
| Histologic grade | G1 and G2 | Ref | |
| G3 and Mucinous | 2.6 (0.89–7.61) | 0.08 | |
| LVI | Absent | Ref | |
| Present | 3.96 (1.80–8.71) | <0.001 | |
| LN numbers | <12 | Ref | |
| ≥12 | 0.68 (0.25–1.84) | 0.46 | |
| pT a | T1–T3 | Ref | |
| T4 | 2.37 (0.98–5.67) | 0.052 | |
| pN b | Negative | Ref | |
| Positive | 2.95 (1.23–7.09) | 0.015 | |
| AJCC Stage c | I & II | Ref | |
| III & IV | 3.22 (1.28–8.1) | 0.012 | |
| Distant metastasis | No | Ref | |
| Yes | 1.16 (0.34–3.89) | 0.808 | |
| MSI | MSS/MSI-Low | Ref | |
| MSI-High | 4.042 × 10−8 (0–Inf) | 0.997 | |
| No data | 1.25 (0.57–2.77) | 0.571 | |
| KRAS | Wild | Ref | |
| Mutant | 1.84 (0.41–8.25) | 0.424 | |
| No data | 1.57 (0.52–4.75) | 0.419 | |
| Postoperative chemotherapy | No | Ref | |
| Yes | 0.84 (0.36–1.97) | 0.7 | |
| rad_score d | Continuous | 4.91 (1.73–13.92) | 0.002 |
| Variables | Subcategory | Training Set | Validation Set | Overall Set | |||
|---|---|---|---|---|---|---|---|
| HR (95% CI) | p | HR (95% CI) | p | HR (95% CI) | p | ||
| LVI | Absent | Ref | Ref | ||||
| Present | 3.73 (1.64–8.47) | 0.001 | 2.37 (1.22–4.59) | 0.010 | |||
| pT a | T1–T3 | Ref | Ref | ||||
| T4 | 4.33 (1.66–11.29) | 0.002 | 2.22 (1.16–4.25) | 0.016 | |||
| pN b | negative | Ref | Ref | Ref | |||
| positive | 2.52 (1.01–6.26) | 0.046 | 3.38 (0.96–11.85) | 0.056 | 2.24 (1.05–4.80) | 0.037 | |
| rad_score c | 7.82 (2.36–25.85) | <0.001 | 12.18 (2.21–66.90) | 0.004 | 8.47 (3.21–22.34) | <0.001 | |
| Parameters | Training Set (n = 228) | Validation Set (n = 153) | Overall Set (n = 381) | |||
|---|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 3 | Model 4 | Model 5 | Model 6 | |
| Included variables | AJCC stage | LVI, pN, rad_score | AJCC stage | LVI, pN, rad_score | AJCC stage | LVI, pN, rad_score |
| C-index (95% CI) (bootstrapped), p | 0.64 (0.55–0.718) | 0.737 (0.63–0.844) | 0.62 (0.516–0.705) | 0.715 (0.561–0.874) | 0.628 (0.563–0.689) | 0.705 (0.619–0.788) |
| p = 0.033 | p = 0.101 | p = 0.014 | ||||
| AIC | 241.763 | 230.996 | 156.861 | 154.19 | 455.156 | 439.26 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kang, J.; Lee, J.-H.; Lee, H.S.; Cho, E.-S.; Park, E.J.; Baik, S.H.; Lee, K.Y.; Park, C.; Yeu, Y.; Clemenceau, J.R.; et al. Radiomics Features of 18F-Fluorodeoxyglucose Positron-Emission Tomography as a Novel Prognostic Signature in Colorectal Cancer. Cancers 2021, 13, 392. https://doi.org/10.3390/cancers13030392
Kang J, Lee J-H, Lee HS, Cho E-S, Park EJ, Baik SH, Lee KY, Park C, Yeu Y, Clemenceau JR, et al. Radiomics Features of 18F-Fluorodeoxyglucose Positron-Emission Tomography as a Novel Prognostic Signature in Colorectal Cancer. Cancers. 2021; 13(3):392. https://doi.org/10.3390/cancers13030392
Chicago/Turabian StyleKang, Jeonghyun, Jae-Hoon Lee, Hye Sun Lee, Eun-Suk Cho, Eun Jung Park, Seung Hyuk Baik, Kang Young Lee, Chihyun Park, Yunku Yeu, Jean R. Clemenceau, and et al. 2021. "Radiomics Features of 18F-Fluorodeoxyglucose Positron-Emission Tomography as a Novel Prognostic Signature in Colorectal Cancer" Cancers 13, no. 3: 392. https://doi.org/10.3390/cancers13030392
APA StyleKang, J., Lee, J. -H., Lee, H. S., Cho, E. -S., Park, E. J., Baik, S. H., Lee, K. Y., Park, C., Yeu, Y., Clemenceau, J. R., Park, S., Xu, H., Hong, C., & Hwang, T. H. (2021). Radiomics Features of 18F-Fluorodeoxyglucose Positron-Emission Tomography as a Novel Prognostic Signature in Colorectal Cancer. Cancers, 13(3), 392. https://doi.org/10.3390/cancers13030392