
Patterns of Sequelae in Women with a History of Localized Breast Cancer: Results from the French VICAN Survey

 ,
,  , , , ,
, , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
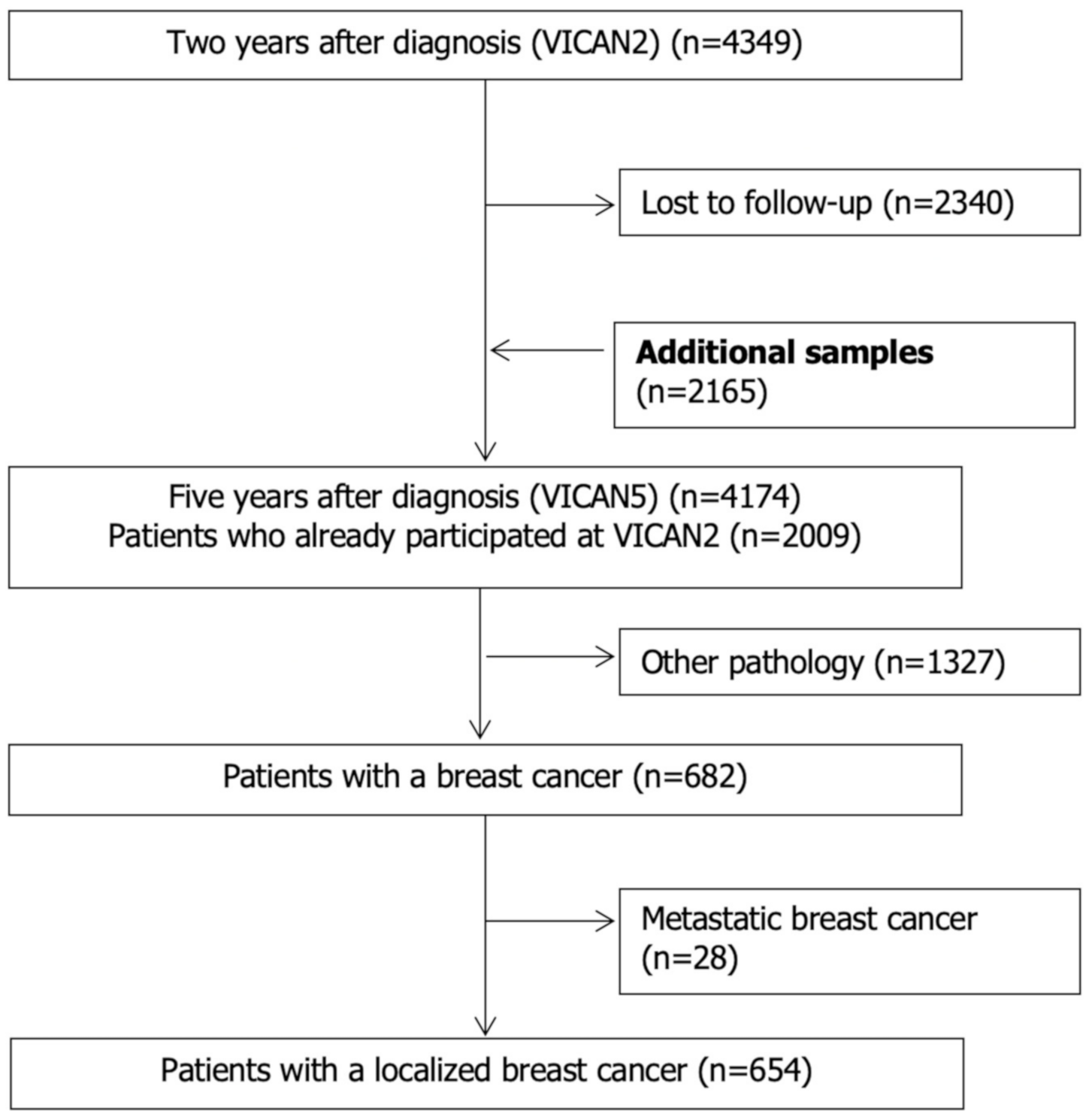
2.1. Study Population
2.2. Data Collection
2.2.1. Data on Spontaneous Sequelae
2.2.2. Socio-Demographic
2.2.3. Medical Characteristics
2.2.4. Self-Rated Global Health
2.2.5. Comorbidity
2.2.6. Neuropathic Pain
2.2.7. Fatigue
2.2.8. Tobacco use and Alcohol Consumption
2.2.9. Anthropometrics
2.2.10. Physical Activity
2.3. Statistical Analyses
3. Results
3.1. Participants’ Characteristics
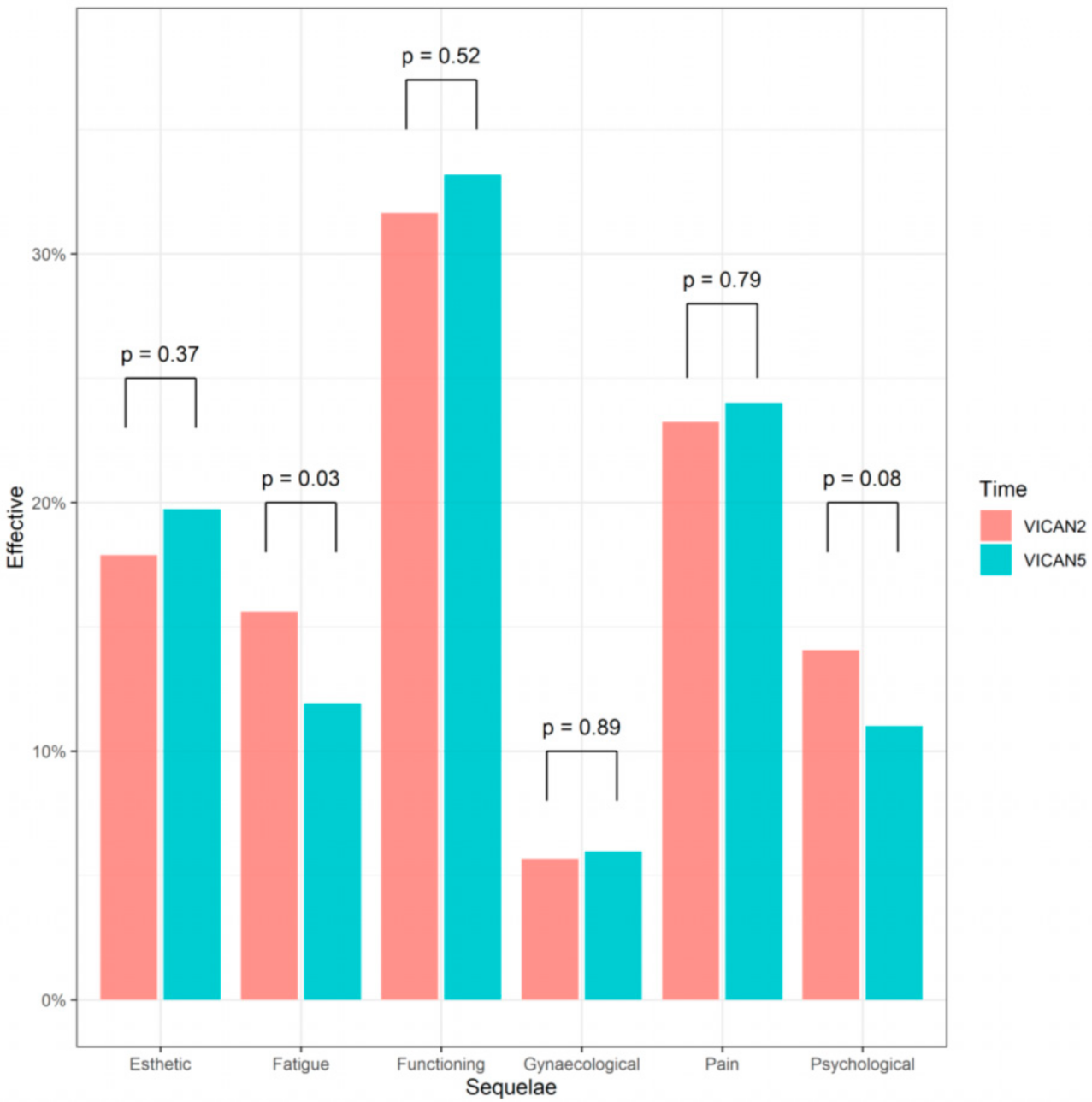
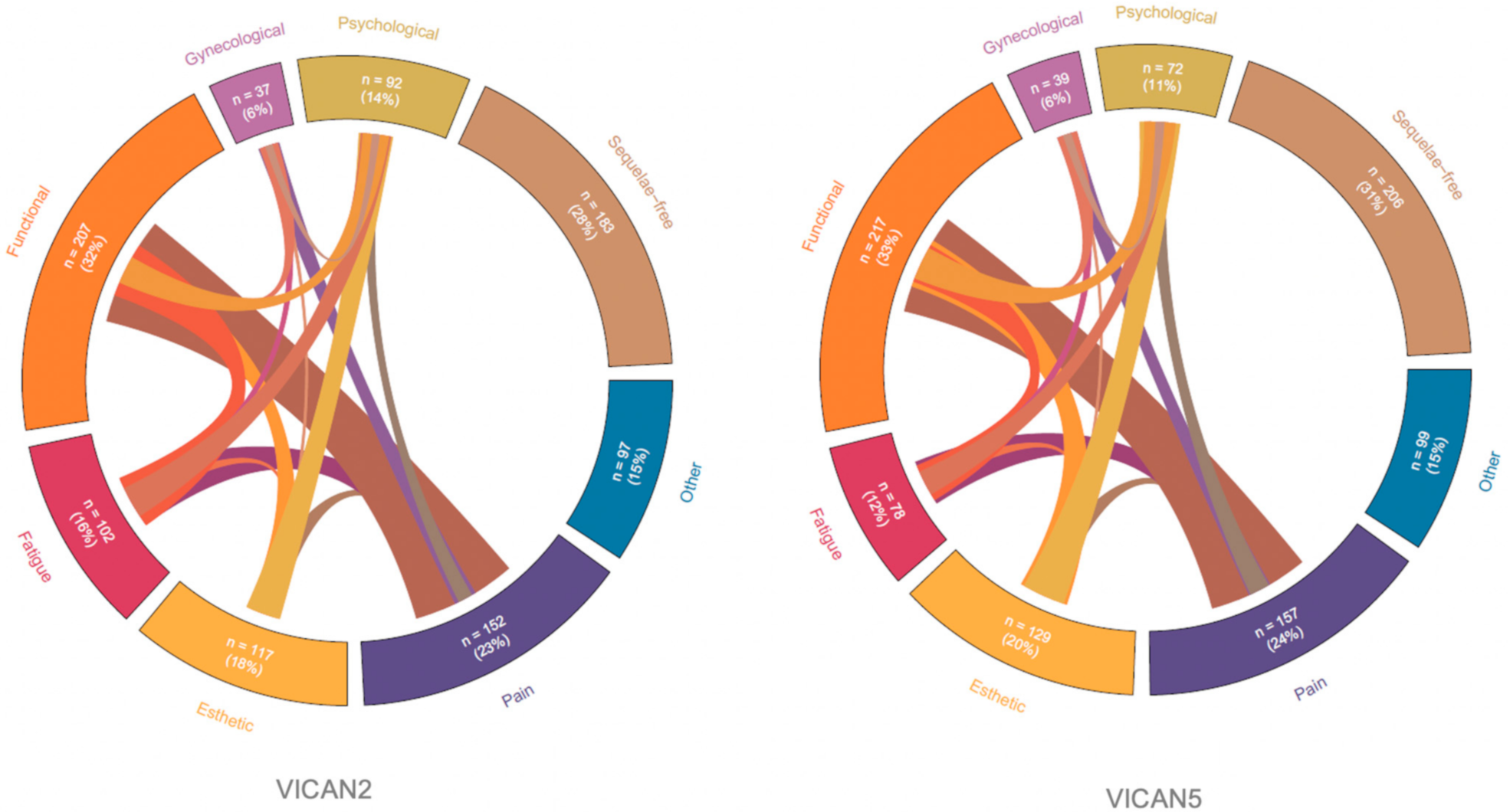
3.2. Main Sequelae of BC and Changer over Time
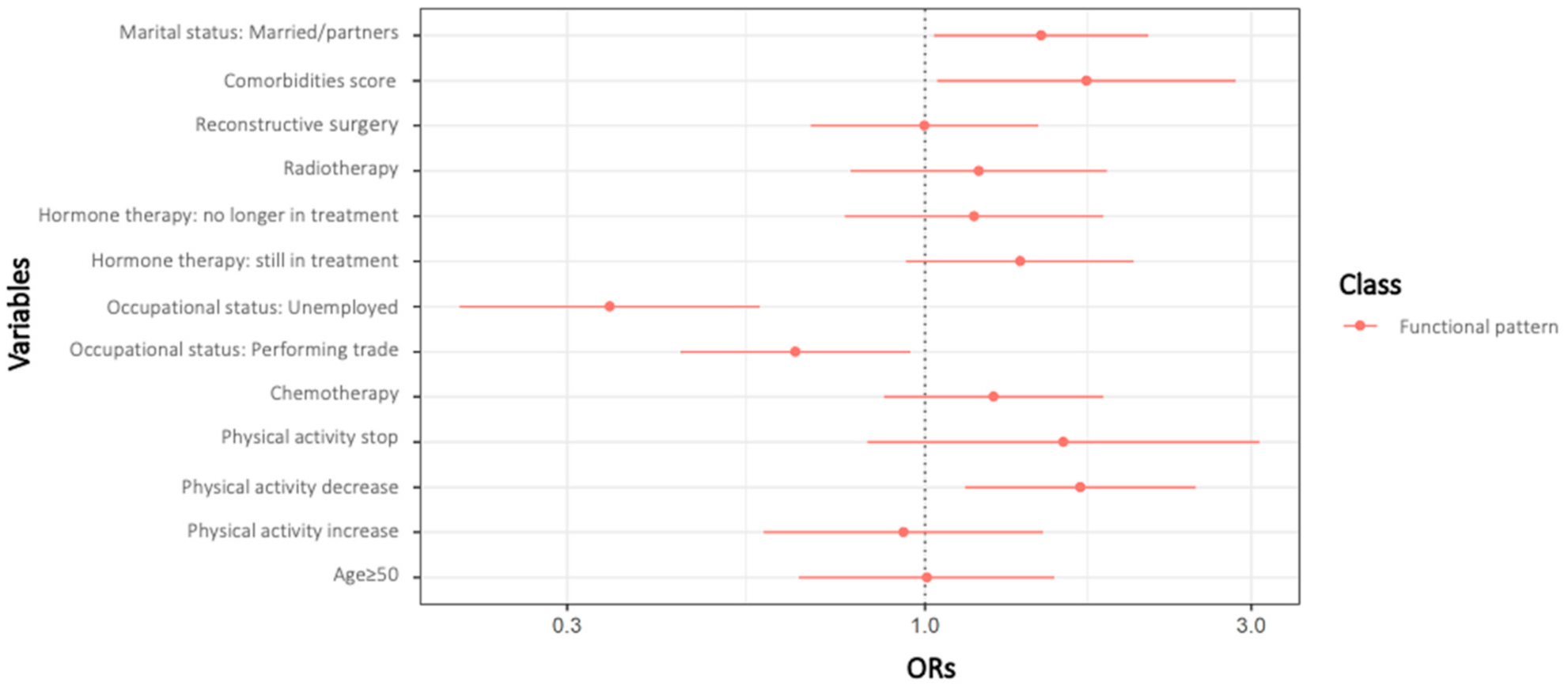
3.3. Latent-Class Analysis of Sequelae Patterns
4. Discussion
4.1. Principal Findings
4.2. BC Sequelae
4.3. Supportive Care for Patients with Cancer
4.4. Benefits of Physical Activity
4.5. Individualized Care for Patients with Cancer
4.6. Strengths and Weaknesses
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA A Cancer J. Clin. 2021, caac.21660. [Google Scholar] [CrossRef] [PubMed]
- Institut National du Cancer Les Cancers En France: L’essentiel Des Faits et Chiffres/Edition 2019. Available online: https://www.e-cancer.fr/ressources/cancers_en_france (accessed on 12 January 2021).
- Bower, J.E. Cancer-Related Fatigue-Mechanisms, Risk Factors, and Treatments. Nat. Rev. Clin. Oncol. 2014, 11, 597–609. [Google Scholar] [CrossRef] [PubMed]
- Bruera, E.; Yennurajalingam, S. Challenge of Managing Cancer-Related Fatigue. J. Clin. Oncol. 2010, 28, 3671–3672. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.S.; Zhao, F.; Fisch, M.J.; O’Mara, A.M.; Cella, D.; Mendoza, T.R.; Cleeland, C.S. Prevalence and Characteristics of Moderate to Severe Fatigue: A Multicenter Study in Cancer Patients and Survivors: Moderate to Severe Patient-Reported Fatigue. Cancer 2014, 120, 425–432. [Google Scholar] [CrossRef]
- Cormie, P.; Zopf, E.M.; Zhang, X.; Schmitz, K.H. The Impact of Exercise on Cancer Mortality, Recurrence, and Treatment-Related Adverse Effects. Epidemiol. Rev. 2017, 39, 71–92. [Google Scholar] [CrossRef] [PubMed]
- Hamer, J.; McDonald, R.; Zhang, L.; Verma, S.; Leahey, A.; Ecclestone, C.; Bedard, G.; Pulenzas, N.; Bhatia, A.; Chow, R.; et al. Quality of Life (QOL) and Symptom Burden (SB) in Patients with Breast Cancer. Support. Care Cancer 2017, 25, 409–419. [Google Scholar] [CrossRef]
- Attal, N.; Lanteri-Minet, M.; Laurent, B.; Fermanian, J.; Bouhassira, D. The Specific Disease Burden of Neuropathic Pain: Results of a French Nationwide Survey. Pain 2011, 152, 2836–2843. [Google Scholar] [CrossRef] [PubMed]
- Glare, P.A.; Davies, P.S.; Finlay, E.; Gulati, A.; Lemanne, D.; Moryl, N.; Oeffinger, K.C.; Paice, J.A.; Stubblefield, M.D.; Syrjala, K.L. Pain in Cancer Survivors. J. Clin. Oncol. 2014, 32, 1739–1747. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jean-Pierre, P.; McDonald, B.C. Neuroepidemiology of cancer and treatment-related neurocognitive dysfunction in adult-onset cancer patients and survivors. In Handbook of Clinical Neurology; Elsevier: Amsterdam, The Netherlands, 2016; Volume 138, pp. 297–309. ISBN 978-0-12-802973-2. [Google Scholar]
- Underwood, E.A.; Rochon, P.A.; Moineddin, R.; Lee, P.E.; Wu, W.; Pritchard, K.I.; Tierney, M.C. Cognitive Sequelae of Endocrine Therapy in Women Treated for Breast Cancer: A Meta-Analysis. Breast Cancer Res. Treat. 2018, 168, 299–310. [Google Scholar] [CrossRef] [PubMed]
- Foucaut, A.-M.; Berthouze, S.E.; Touillaud, M.; Morelle, M.; Bourne-Branchu, V.; Kempf-Lépine, A.-S.; Carretier, J.; Pérol, D.; Trédan, O.; Bachmann, P.; et al. Deterioration of Physical Activity Level and Metabolic Risk Factors After Early-Stage Breast Cancer Diagnosis. Cancer Nurs. 2015, 38, E1–E9. [Google Scholar] [CrossRef] [PubMed]
- Klassen, O.; Schmidt, M.E.; Scharhag-Rosenberger, F.; Sorkin, M.; Ulrich, C.M.; Schneeweiss, A.; Potthoff, K.; Steindorf, K.; Wiskemann, J. Cardiorespiratory Fitness in Breast Cancer Patients Undergoing Adjuvant Therapy. Acta Oncol. 2014, 53, 1356–1365. [Google Scholar] [CrossRef] [PubMed]
- Toth, M.J.; Miller, M.S.; Callahan, D.M.; Sweeny, A.P.; Nunez, I.; Grunberg, S.M.; Der-Torossian, H.; Couch, M.E.; Dittus, K. Molecular Mechanisms Underlying Skeletal Muscle Weakness in Human Cancer: Reduced Myosin-Actin Cross-Bridge Formation and Kinetics. J. Appl. Physiol. 2013, 114, 858–868. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McLaughlin, S.A.; Wright, M.J.; Morris, K.T.; Giron, G.L.; Sampson, M.R.; Brockway, J.P.; Hurley, K.E.; Riedel, E.R.; Van Zee, K.J. Prevalence of Lymphedema in Women with Breast Cancer 5 Years after Sentinel Lymph Node Biopsy or Axillary Dissection: Objective Measurements. J. Clin. Oncol. 2008, 26, 5213–5219. [Google Scholar] [CrossRef] [PubMed]
- Carver, J.R.; Shapiro, C.L.; Ng, A.; Jacobs, L.; Schwartz, C.; Virgo, K.S.; Hagerty, K.L.; Somerfield, M.R.; Vaughn, D.J. American Society of Clinical Oncology Clinical Evidence Review on the Ongoing Care of Adult Cancer Survivors: Cardiac and Pulmonary Late Effects. J. Clin. Oncol. 2007, 25, 3991–4008. [Google Scholar] [CrossRef] [Green Version]
- Giza, D.E.; Iliescu, G.; Hassan, S.; Marmagkiolis, K.; Iliescu, C. Cancer as a Risk Factor for Cardiovascular Disease. Curr. Oncol. Rep. 2017, 19. [Google Scholar] [CrossRef]
- Okwuosa, T.M.; Anzevino, S.; Rao, R. Cardiovascular Disease in Cancer Survivors. Postdrad. Med. J. 2017, 93, 82–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peel, J.B.; Sui, X.; Adams, S.A.; Hébert, J.R.; Hardin, J.W.; Blair, S.N. A Prospective Study of Cardiorespiratory Fitness and Breast Cancer Mortality. Med. Sci. Sports Exerc. 2009, 41, 742–748. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Babak, S.; Brezden-Masley, C. Cardiovascular Sequelae of Breast Cancer Treatments: A Review. Curr. Probl. Cancer 2018, 42, 409–421. [Google Scholar] [CrossRef]
- Sun, L.; Ang, E.; Ang, W.H.D.; Lopez, V. Losing the Breast: A Meta-Synthesis of the Impact in Women Breast Cancer Survivors. Psycho-Oncol. 2018, 27, 376–385. [Google Scholar] [CrossRef]
- Jabłoński, M.J.; Streb, J.; Mirucka, B.; Słowik, A.J.; Jach, R. The Relationship between Surgical Treatment (Mastectomy vs. Breast Conserving Treatment) and Body Acceptance, Manifesting Femininity and Experiencing an Intimate Relation with a Partner in Breast Cancer Patients. Psychiatr. Pol. 2018, 52, 859–872. [Google Scholar] [CrossRef] [PubMed]
- Candy, B.; Jones, L.; Vickerstaff, V.; Tookman, A.; King, M. Interventions for Sexual Dysfunction Following Treatments for Cancer in Women. Cochrane Database Syst. Rev. 2016. [Google Scholar] [CrossRef] [PubMed]
- Hewitt, M.; Rowland, J.H.; Yancik, R. Cancer Survivors in the United States: Age, Health, and Disability. J. Gerontol. A. Biol. Sci. Med. Sci. 2003, 58, M82–M91. [Google Scholar] [CrossRef]
- Elliott, J.; Fallows, A.; Staetsky, L.; Smith, P.W.F.; Foster, C.L.; Maher, E.J.; Corner, J. The Health and Well-Being of Cancer Survivors in the UK: Findings from a Population-Based Survey. Br. J. Cancer 2011, 105, S11–S20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vannorsdall, T.D. Cognitive Changes Related to Cancer Therapy. Med. Clin. N. Am. 2017, 101, 1115–1134. [Google Scholar] [CrossRef] [PubMed]
- Jégu, J.; Colonna, M.; Daubisse-Marliac, L.; Trétarre, B.; Ganry, O.; Guizard, A.-V.; Bara, S.; Troussard, X.; Bouvier, V.; Woronoff, A.-S.; et al. The Effect of Patient Characteristics on Second Primary Cancer Risk in France. BMC Cancer 2014, 14. [Google Scholar] [CrossRef] [PubMed]
- Identifier et Prévenir Les Risques de Second Cancer Primitif Chez l’adulte. 2013. Available online: https://www.e-cancer.fr/Expertises-et-publications/Catalogue-des-publications/Identifier-et-prevenir-les-risques-de-second-cancer-primitif-chez-l-adulte (accessed on 12 January 2021).
- Tralongo, P.; Pescarenico, M.G.; Surbone, A.; Bordonaro, S.; Berretta, M.; DI Mari, A. Physical Needs of Long-Term Cancer Patients. Anticancer Res. 2017, 37, 4733–4746. [Google Scholar] [CrossRef] [PubMed]
- Patnaik, J.L.; Byers, T.; DiGuiseppi, C.; Dabelea, D.; Denberg, T.D. Cardiovascular Disease Competes with Breast Cancer as the Leading Cause of Death for Older Females Diagnosed with Breast Cancer: A Retrospective Cohort Study. Breast Cancer Res. 2011, 13. [Google Scholar] [CrossRef] [Green Version]
- Spyropoulou, D.; Leotsinidis, M.; Tsiamita, M.; Spiropoulos, K.; Kardamakis, D. Pulmonary Function Testing in Women with Breast Cancer Treated with Radiotherapy and Chemotherapy. In Vivo 2009, 23, 867–871. [Google Scholar]
- Melisko, M.E.; Gradishar, W.J.; Moy, B. Issues in Breast Cancer Survivorship: Optimal Care, Bone Health, and Lifestyle Modifications. Am. Soc. Clin Oncol. Educ. Book 2016, e22–e29. [Google Scholar] [CrossRef] [PubMed]
- Hamer, J.; Warner, E. Lifestyle Modifications for Patients with Breast Cancer to Improve Prognosis and Optimize Overall Health. Can. Med. Assoc. J. 2017, 189, E268–E274. [Google Scholar] [CrossRef] [Green Version]
- Bouhnik, A.-D.; Bendiane, M.-K.; Cortaredona, S.; Teyssier, L.S.; Rey, D.; Berenger, C.; Seror, V.; Peretti-Watel, P.; members of the VICAN Group. The Labour Market, Psychosocial Outcomes and Health Conditions in Cancer Survivors: Protocol for a Nationwide Longitudinal Survey 2 and 5 Years after Cancer Diagnosis (the VICAN Survey). BMJ Open 2015, 5, e005971. [Google Scholar] [CrossRef] [PubMed]
- Paci, E.; Cariddi, A.; Barchielli, A.; Bianchi, S.; Cardona, G.; Distante, V.; Giorgi, D.; Pacini, P.; Zappa, M.; Del Turco, M.R. Long-Term Sequelae of Breast Cancer Surgery. Tumori J. 1996, 82, 321–324. [Google Scholar] [CrossRef]
- Cooney, M.A.; Galvin, R.; Stokes, E.K. Do Women with Breast Cancer Report Treatment After-Effects to Healthcare Professionals, and Who Provides the Intervention? Int. J. of Rehab. Res. 2015, 38, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Cox, B.; Oyen, H.V.; Cambois, E.; Jagger, C.; le Roy, S.; Robine, J.-M.; Romieu, I. The Reliability of the Minimum European Health Module. Int. J. Public Health 2009, 54, 55–60. [Google Scholar] [CrossRef]
- Cortaredona, S.; Pambrun, E.; Verdoux, H.; Verger, P. Comparison of Pharmacy-Based and Diagnosis-Based Comorbidity Measures from Medical Administrative Data: Comorbidity Measures. Pharmacoepidemiol. Drug Saf. 2017, 26, 402–411. [Google Scholar] [CrossRef]
- Bouhassira, D.; Attal, N.; Alchaar, H.; Boureau, F.; Brochet, B.; Bruxelle, J.; Cunin, G.; Fermanian, J.; Ginies, P.; Grun-Overdyking, A.; et al. Comparison of Pain Syndromes Associated with Nervous or Somatic Lesions and Development of a New Neuropathic Pain Diagnostic Questionnaire (DN4). Pain 2005, 114, 29–36. [Google Scholar] [CrossRef]
- Osoba, D.; Zee, B.; Pater, J.; Warr, D.; Kaizer, L.; Latreille, J. Psychometric Properties and Responsiveness of the EORTC Quality of Life Questionnaire (QLQ-C30) in Patients with Breast, Ovarian and Lung Cancer. Qual. Life Res. 1994, 3, 353–364. [Google Scholar] [CrossRef]
- Aaronson, N.K.; Ahmedzai, S.; Bergman, B.; Bullinger, M.; Cull, A.; Duez, N.J.; Filiberti, A.; Flechtner, H.; Fleishman, S.B.; de Haes, J.C. The European Organization for Research and Treatment of Cancer QLQ-C30: A Quality-of-Life Instrument for Use in International Clinical Trials in Oncology. J. Natl. Cancer Inst. 1993, 85, 365–376. [Google Scholar] [CrossRef] [PubMed]
- Lazarsfeld, P.F.; Henry, N.W. Latent Structure Analysis; Houghton, Mifflin: New York, NY, USA, 1968; ISBN 978-0-395-04768-2. [Google Scholar]
- McLachlan, G.J.; Peel, D. Finite Mixture Models; Wiley series in probability and statistics. Applied probability and statistics section; Wiley: New York, NY, USA, 2000; ISBN 978-0-471-00626-8. [Google Scholar]
- Schmitz, K.H.; Speck, R.M.; Rye, S.A.; DiSipio, T.; Hayes, S.C. Prevalence of Breast Cancer Treatment Sequelae over 6 Years of Follow-up: The Pulling Through Study. Cancer 2012, 118, 2217–2225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khan, F.; Amatya, B.; Pallant, J.F.; Rajapaksa, I. Factors Associated with Long-Term Functional Outcomes and Psychological Sequelae in Women after Breast Cancer. Breast 2012, 21, 314–320. [Google Scholar] [CrossRef]
- Juvet, L.K.; Thune, I.; Elvsaas, I.K.Ø.; Fors, E.A.; Lundgren, S.; Bertheussen, G.; Leivseth, G.; Oldervoll, L.M. The Effect of Exercise on Fatigue and Physical Functioning in Breast Cancer Patients during and after Treatment and at 6 Months Follow-up: A Meta-Analysis. Breast 2017, 33, 166–177. [Google Scholar] [CrossRef]
- Ancoli-Israel, S.; Liu, L.; Marler, M.R.; Parker, B.A.; Jones, V.; Sadler, G.R.; Dimsdale, J.; Cohen-Zion, M.; Fiorentino, L. Fatigue, Sleep, and Circadian Rhythms Prior to Chemotherapy for Breast Cancer. Support. Care Cancer 2006, 14, 201–209. [Google Scholar] [CrossRef] [Green Version]
- Armstrong, C.W.; McGregor, N.R.; Butt, H.L.; Gooley, P.R. Metabolism in Chronic Fatigue Syndrome. Adv. Clin. Chem. 2014, 66, 121–172. [Google Scholar]
- Condorelli, R.; Vaz-Luis, I. Managing Side Effects in Adjuvant Endocrine Therapy for Breast Cancer. Expert. Rev. Anticancer Ther. 2018, 18, 1101–1112. [Google Scholar] [CrossRef]
- Early Breast Cancer Trialists’ Collaborative Group (EBCTCG) Effects of Chemotherapy and Hormonal Therapy for Early Breast Cancer on Recurrence and 15-Year Survival: An Overview of the Randomised Trials. Lancet 2005, 365, 1687–1717. [CrossRef]
- Berkowitz, M.J.; Thompson, C.K.; Zibecchi, L.T.; Lee, M.K.; Streja, E.; Berkowitz, J.S.; Wenziger, C.M.; Baker, J.L.; DiNome, M.L.; Attai, D.J. How Patients Experience Endocrine Therapy for Breast Cancer: An Online Survey of Side Effects, Adherence, and Medical Team Support. J. Cancer Surviv. 2020. [Google Scholar] [CrossRef] [PubMed]
- Bernhard, J.; Luo, W.; Ribi, K.; Colleoni, M.; Burstein, H.J.; Tondini, C.; Pinotti, G.; Spazzapan, S.; Ruhstaller, T.; Puglisi, F.; et al. Patient-Reported Outcomes with Adjuvant Exemestane versus Tamoxifen in Premenopausal Women with Early Breast Cancer Undergoing Ovarian Suppression (TEXT and SOFT): A Combined Analysis of Two Phase 3 Randomised Trials. Lancet Oncol. 2015, 16, 848–858. [Google Scholar] [CrossRef] [Green Version]
- Cavadias, I.; Rouzier, R.; Lerebours, F.; Héquet, D. Hot flushes and breast cancer with positive hormone receptors: Mechanisms and management. Bull. Cancer 2020. [Google Scholar] [CrossRef]
- Zdenkowski, N.; Tesson, S.; Lombard, J.; Lovell, M.; Hayes, S.; Francis, P.A.; Dhillon, H.M.; Boyle, F.M. Supportive Care of Women with Breast Cancer: Key Concerns and Practical Solutions. Med. J. Aust. 2016, 205, 471–475. [Google Scholar] [CrossRef] [PubMed]
- Thariat, J.; Creisson, A.; Chamignon, B.; Dejode, M.; Gastineau, M.; Hébert, C.; Boissin, F.; Topfer, C.; Gilbert, E.; Grondin, B.; et al. Éducation thérapeutique du patient, concepts et mise en œuvre. Bull. Cancer 2016, 103, 674–690. [Google Scholar] [CrossRef]
- Pérol, D.; Toutenu, P.; Lefranc, A.; Régnier, V.; Chvetzoff, G.; Saltel, P.; Chauvin, F. Therapeutic education in oncology: Involving patient in the management of cancer. Bull. Cancer 2007, 94, 267–274. [Google Scholar]
- Kuo, C.-C.; Lin, C.-C.; Tsai, F.-M. Effectiveness of Empowerment-Based Self-Management Interventions on Patients with Chronic Metabolic Diseases: A Systematic Review and Meta-Analysis. Worldviews Evid. Based Nurs. 2014, 11, 301–315. [Google Scholar] [CrossRef]
- Groen, W.G.; Kuijpers, W.; Oldenburg, H.S.; Wouters, M.W.; Aaronson, N.K.; van Harten, W.H. Empowerment of Cancer Survivors Through Information Technology: An Integrative Review. J. Med. Internet Res. 2015, 17, e270. [Google Scholar] [CrossRef] [Green Version]
- Fong, D.Y.T.; Ho, J.W.C.; Hui, B.P.H.; Lee, A.M.; Macfarlane, D.J.; Leung, S.S.K.; Cerin, E.; Chan, W.Y.Y.; Leung, I.P.F.; Lam, S.H.S.; et al. Physical Activity for Cancer Survivors: Meta-Analysis of Randomised Controlled Trials. BMJ 2012, 344, e70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Speck, R.M.; Courneya, K.S.; Mâsse, L.C.; Duval, S.; Schmitz, K.H. An Update of Controlled Physical Activity Trials in Cancer Survivors: A Systematic Review and Meta-Analysis. J. Cancer Surviv. 2010, 4, 87–100. [Google Scholar] [CrossRef]
- Boing, L.; Vieira, M.D.C.S.; Moratelli, J.; Bergmann, A.; de Azevedo Guimarães, A.C. Effects of Exercise on Physical Outcomes of Breast Cancer Survivors Receiving Hormone Therapy—A Systematic Review and Meta-Analysis. Maturitas 2020, 141, 71–81. [Google Scholar] [CrossRef]
- Sabiston, C.M.; Wrosch, C.; Fong, A.J.; Brunet, J.; Gaudreau, P.; O’Loughlin, J.; Meterissian, S. Life after Breast Cancer: Moving on, Sitting down or Standing Still? A Prospective Study of Canadian Breast Cancer Survivors. BMJ Open 2018, 8, e021770. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Halpern, M.T.; Argenbright, K.E. Evaluation of Effectiveness of Survivorship Programmes: How to Measure Success? Lancet Oncol. 2017, 18, e51–e59. [Google Scholar] [CrossRef]
- Mayer, D.K.; Nasso, S.F.; Earp, J.A. Defining Cancer Survivors, Their Needs, and Perspectives on Survivorship Health Care in the USA. Lancet Oncol. 2017, 18, e11–e18. [Google Scholar] [CrossRef]
- Perez, E.A.; Rodeheffer, R. Clinical Cardiac Tolerability of Trastuzumab. J. Clin. Oncol. 2004, 22, 322–329. [Google Scholar] [CrossRef] [PubMed]
- Harris, E.E.R.; Correa, C.; Hwang, W.-T.; Liao, J.; Litt, H.I.; Ferrari, V.A.; Solin, L.J. Late Cardiac Mortality and Morbidity in Early-Stage Breast Cancer Patients after Breast-Conservation Treatment. J. Clin. Oncol. 2006, 24, 4100–4106. [Google Scholar] [CrossRef] [PubMed]
- De Iuliis, F.; Taglieri, L.; Salerno, G.; Lanza, R.; Scarpa, S. Taxane Induced Neuropathy in Patients Affected by Breast Cancer: Literature Review. Crit. Rev. Oncol. Hematol. 2015, 96, 34–45. [Google Scholar] [CrossRef] [PubMed]
- Song, S.J.; Min, J.; Suh, S.Y.; Jung, S.H.; Hahn, H.J.; Im, S.-A.; Lee, J.-Y. Incidence of Taxane-Induced Peripheral Neuropathy Receiving Treatment and Prescription Patterns in Patients with Breast Cancer. Support. Care Cancer 2017, 25, 2241–2248. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Mean (SD) | n (%) |
|---|---|---|
| Age at diagnosis (years) | 49.8 (10.5) | |
| Age at diagnosis (years) | ||
| <50 | 438 (67) | |
| >50 | 216 (33) | |
| Marital status a | ||
| Married/Partners | 458 (70) | |
| Single/Divorced/Separated | 195 (30) | |
| Education | ||
| <High school | 286 (44) | |
| ≥High school | 368 (56) | |
| Occupational status | ||
| Employed | ||
| Performing trades (farmers, craftsmen, laborers, employees) | 271 (42) | |
| Managerial occupations (executives and senior managers, heads of companies, intermediate professions) | 198 (30) | |
| Unemployed | 185 (28) | |
| Employment status | ||
| In employment (or short-term sick leave / leave) | 469 (72) | |
| Other situations | 185 (28) |
| Characteristics | Two Years (VICAN2) | Five Years (VICAN5) | ||
|---|---|---|---|---|
| Mean (SD) | n (%) | Mean (SD) | n (%) | |
| LIFESTYLE | ||||
| Anthropometry | ||||
| BMI (kg/m2) | 24.6 (5.6) | - | ||
| Underweight (<18.5 kg/m2) | 26 (4) | - | ||
| Normal weight (<25 kg/m2) | 382 (58) | - | ||
| Overweight (25–30 kg/m2) | 170 (26) | - | ||
| Obese (>30 kg/m2) | 76 (12) | - | ||
| Physical activity evolution since diagnosisa | ||||
| Stop | 48 (7) | 38 (6) | ||
| Decrease | 275 (42) | 295 (46) | ||
| Stable | 203 (31) | 204 (32) | ||
| Increase | 125 (19) | 109 (17) | ||
| Smoking (yes) | 128 (20) | 135 (21) | ||
| Alcohol consumption (yes) | 492 (75) | 506 (77) | ||
| Treatment | ||||
| Chemotherapy since diagnosis | 382 (58) | 387 (59) | ||
| Radiotherapy since diagnosis | 532 (81) | 532 (81) | ||
| Hormonotherapy since diagnosis | ||||
| Yes, and I’m still taking this treatment | 442 (68) | 275 (42) | ||
| Yes, and I’m no longer taking this treatment | 26 (4) | 163(25) | ||
| No | 186 (28) | 215 (33) | ||
| Reconstructive surgery | NA | 164 (25) | ||
| Pain score (DN4) b | 2.4 (1.8) c | 2.2 (1.8) c | ||
| Fatigue score (EORTC) | 50.3 (27.6) | 48.6 (26.9) | ||
| Comorbidity score | 0.5 (0.4) | 0.6 (0.4) | ||
| Self-rated global healthc | ||||
| Very good | 127 (19) | 34 (5) | ||
| Good | 252 (39) | 80 (12) | ||
| Quite good | 236 (36) | 422 (65) | ||
| Bad | 37 (6) | 86 (13) | ||
| Very bad | 0 | 25 (4) | ||
| Presence of sequelae | 471 (72) | 448 (69) | ||
| Number of sequelae (mean, SD) | 1.6 (1.4) | 1.6 (1.5) | ||
| Presence and magnitude of sequelae following the management of your diseasec | ||||
| Intense | 53 (8) | 34 (5) | ||
| Important | 146 (23) | 117 (18) | ||
| Moderate | 182 (28) | 204 (31) | ||
| Very moderate | 92 (14) | 100 (15) | ||
| No sequelae | 174 (27) | 195 (30) | ||
| Specific treatment for sequelaed | ||||
| Yes | - | 448 (69) | ||
| No | - | 1.6 (1.5) | ||
| Class 1 (%) | Class 2 (%) | |
|---|---|---|
| Patterns: | Esthetic Pattern | Functional Pattern |
| N | 340 | 314 |
| Sequelae | ||
| Functioning | 6.8 | 61.8 |
| Pain | 0 | 50.0 |
| Esthetic | 31.2 | 7.3 |
| Fatigue | 0 | 24.8 |
| Psychological | 10.9 | 11.1 |
| Gynaecological | 0 | 12.4 |
| SOCIODEMOGRAPHIC AT INCLUSION | ||
| Age at diagnosis (years) mean (SD) | 51.2 (11.3) | 48.4 (9.5) |
| <50 | 63.0 | 71.3 |
| ≥50 | 37.0 | 28.7 |
| Education | ||
| <High school | 47.6 | 39.5 |
| ≥High school | 52.4 | 60.5 |
| Marital status | ||
| Married/partners | 66.7 | 73.9 |
| Single/Divorced/Separated | 33.3 | 26.1 |
| Occupational status | ||
| Performing trades (farmers, craftsmen, labourers, employees) | 39.7 | 43.3 |
| Managerial occupations (executives and senior managers, heads of companies, intermediate professions) | 24.7 | 36.3 |
| Not in employment at the time of diagnosis | 35.6 | 20.4 |
| LIFESTYLE AT VICAN2 | ||
| BMI (kg/m2) mean (SD) | 24.5 (6.2) | 24.6 (4.9) |
| BMI (kg/m2) | ||
| Underweight (<18.5 kg/m2) | 2.9 | 5.1 |
| Normal weight (<25 kg/m2) | 61.2 | 55.4 |
| Overweight (25–30 kg/m2) | 25.0 | 27.1 |
| Obese (>30 kg/m2) | 10.9 | 12.4 |
| Physical activity evolution since diagnosis | ||
| Stop | 6.5 | 8.3 |
| Decrease | 37.0 | 48.0 |
| Stable | 35.8 | 26.2 |
| Increase | 20.7 | 17.5 |
| Smoking (yes) | 17.9 | 21.3 |
| Alcohol consumption (yes) | 76.8 | 73.6 |
| TREATMENTS AT VICAN5 | ||
| Radiotherapy | ||
| Yes | 79.4 | 83.4 |
| No | 20.6 | 16.6 |
| Chemotherapy | ||
| Yes | 53.5 | 65.3 |
| No | 46.5 | 34.7 |
| Hormonotherapy since diagnosis | ||
| Yes, and I’m still taking this treatment | 37.5 | 47.1 |
| Yes, and I’m no longer taking this treatment | 26.5 | 23.2 |
| No | 36.0 | 29.7 |
| Reconstructive surgery | ||
| Yes | 76.1 | 73.6 |
| No | 23.9 | 26.4 |
| Fatigue score (mean, SD) | 43.0 (27.8) | 58.2 (25.2) |
| Comorbidities score (mean, SD) | 0.7 (0.4) | 0.7 (0.3) |
| Latent Class | ||
|---|---|---|
| Variable | Class 1 | Class 2 |
| Patterns | Esthetic pattern | Functional pattern |
| SOCIODEMOGRAPHIC AT INCLUSION | ||
| Age (ref <50) | 0.98 [0.96–0.99] | |
| ≥50 | 1 | 0.68 [0.49–0.95] |
| Education (ref ≥ High school) | ||
| <High school | 1 | 0.72 [0.53–0.98] |
| Marital status (ref = Single) | ||
| Married/partners | 1 | 1.42 [1.01–1.98] |
| Occupational status (ref = managerial occupations) | ||
| Performing trades (farmers, craftsmen, labourers, employees) | 1 | 0.74 [0.51–1.07] |
| Unemployment at the time of diagnosis | 1 | 0.39 [0.26–1.59] |
| LIFESTYLE AT VICAN2 | ||
| BMI (kg/m2) (ref = normal) | 1.01 [0.98-1.03] | |
| Underweight (<18.5 kg/m2) | 1 | 1.91 [0.85-4.32] |
| Overweight (25–30 kg/m2) | 1 | 1.20 [0.83–1.72] |
| Obese (>30 kg/m2) | 1 | 1.26 [0.77–2.06] |
| Physical activity (ref = stable) | ||
| Stop | 1 | 1.74 [0.93–3.28] |
| Decrease | 1 | 1.77 [1.23–2.56] |
| Increase | 1 | 1.15 [0.74–1.82] |
| Smoking (Ref: No) | 1 | 1.24 [0.84–1.83] |
| Alcohol consumption (Ref: No) | 1 | 0.84 [0.59–1.20] |
| TREATMENTS AT VICAN5 | ||
| Chemotherapy | ||
| Yes | 1 | 1.63 [1.19–2.24] |
| Radiotherapy | ||
| Yes | 1 | 1.31 [0.88–1.94] |
| Hormone therapy (ref = no) | ||
| Yes, and I’m still taking this treatment | 1 | 1.53 [1.07–2.19] |
| Yes, and I’m no longer taking this treatment | 1 | 1.06 [0.71–1.60] |
| Reconstructive surgery | ||
| Yes | 1 | 1.14 [0.80–1.63] |
| Pain score (mean) | 1 | 1.14 [1.04–1.26] |
| Fatigue score (mean) | 1 | 1.02 [1.01–1.03] |
| Comorbidities score (mean) | 1 | 1.57 [0.99–2.47] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Delrieu, L.; Bouaoun, L.; Fatouhi, D.E.; Dumas, E.; Bouhnik, A.-D.; Noelle, H.; Jacquet, E.; Hamy, A.-S.; Coussy, F.; Reyal, F.; et al. Patterns of Sequelae in Women with a History of Localized Breast Cancer: Results from the French VICAN Survey. Cancers 2021, 13, 1161. https://doi.org/10.3390/cancers13051161
Delrieu L, Bouaoun L, Fatouhi DE, Dumas E, Bouhnik A-D, Noelle H, Jacquet E, Hamy A-S, Coussy F, Reyal F, et al. Patterns of Sequelae in Women with a History of Localized Breast Cancer: Results from the French VICAN Survey. Cancers. 2021; 13(5):1161. https://doi.org/10.3390/cancers13051161
Chicago/Turabian StyleDelrieu, Lidia, Liacine Bouaoun, Douae El Fatouhi, Elise Dumas, Anne-Deborah Bouhnik, Hugo Noelle, Emmanuelle Jacquet, Anne-Sophie Hamy, Florence Coussy, Fabien Reyal, and et al. 2021. "Patterns of Sequelae in Women with a History of Localized Breast Cancer: Results from the French VICAN Survey" Cancers 13, no. 5: 1161. https://doi.org/10.3390/cancers13051161
APA StyleDelrieu, L., Bouaoun, L., Fatouhi, D. E., Dumas, E., Bouhnik, A. -D., Noelle, H., Jacquet, E., Hamy, A. -S., Coussy, F., Reyal, F., Heudel, P. -E., Bendiane, M. -K., Fournier, B., Michallet, M., Fervers, B., Fagherazzi, G., & Pérol, O. (2021). Patterns of Sequelae in Women with a History of Localized Breast Cancer: Results from the French VICAN Survey. Cancers, 13(5), 1161. https://doi.org/10.3390/cancers13051161