
Pre-Surgery Cognitive Performance and Voxel-Based Lesion-Symptom Mapping in Patients with Left High-Grade Glioma

Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Neuropsychological Assessment
Neuropsychological Data Analyses
2.3. MRI Structural Data
2.3.1. Voxel-Based Lesion-Symptom Mapping
2.3.2. Further Exploratory Investigation: Subtraction Analysis
3. Results
3.1. Behavioral Data
3.1.1. Pre-surgical Clinical Symptoms
- We analyzed the patients’ self-reported clinical signs and symptoms gleaned from case notes and from the neuropsychological interview. Patients reported clinical signs and symptoms (see Table 2). Some patients reported a combination of cognitive and motor/proprioceptive symptoms. The most frequently reported symptoms were language-related, in particular anomia and phonological paraphasia, reading and writing difficulties.
3.1.2. Neuropsychological Data
- Considering tasks performed by 80–100% of our sample (see Table 3), naming as cognitive domain showing was most impaired. Considering tasks performed by 60–80% of our sample, reading showed to be most impaired. Considering tasks performed by 40–60% of our sample, lexical decision and writing were most impaired.
- 13/85 (15%) patients had no cognitive impairments in any domain considered.
- The patients’ mean level of accuracy ranged from 80.68% to 98.21% (see Table 3), even for the cognitive domain on which the greatest percentage of patients scored below the normal range.
3.2. Structural Data
3.2.1. Voxel-Based Lesion-Symptom Mapping (VLSM)
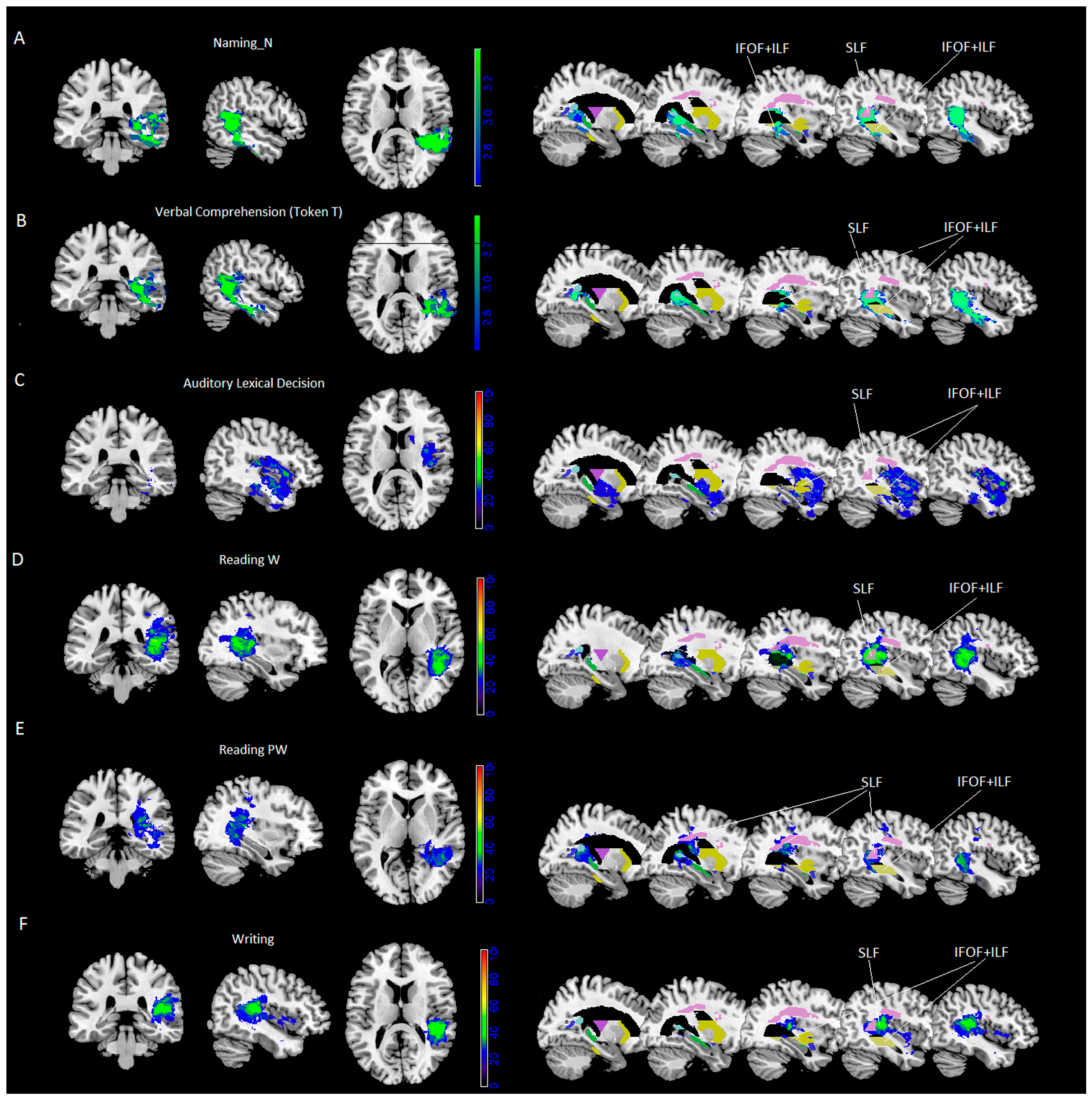
- Results of VLSM analyses were significant for noun naming and verbal comprehension (Token Test) only. VLSM performed for noun naming revealed 24% of the voxels damaged in the middle temporal cortex and, to a lesser extent (between 15% and 10%), in the inferior and superior temporal gyrus, the hippocampus/parahippocampal area and the fusiform gyrus (Figure 1A). In addition, at subcortical level we found portions of the posterior thalamic radiation and the sagittal stratum [including the inferior fronto-occipital fasciculus (IFOF) and the inferior longitudinal fasciculus (ILF)], with 40% of overlapping lesions, and to a lesser extent (% voxels damaged between 29% and 14%), the retrolenticular part of the internal capsule, the superior longitudinal fasciculus (SLF, with 50% of overlapping lesions) and pars of the tapetum (see Table 4 and Figure 1A).
- VLSM analyses performed for the Token Test revealed 26% of the voxels damaged in the middle temporal cortex and, to a lesser extent (between 15% and 10% of the voxel damaged), in the inferior and superior temporal gyrus, and the hippocampus (Figure 1B). At subcortical level we found parts of the sagittal stratum (including IFOF and ILF, with 43% of overlapping lesions), posterior corona radiate and posterior thalamic radiation and the retrolenticular part of the internal capsule, pars of the tapetum and, to a lesser extent (% voxels damaged between 26% and 5%), the superior longitudinal fasciculus (SLF, with 49% of overlapping lesions) and pars of the splenium (see Table 4 and Figure 1B).
- All other tasks did not survive correction for multiple comparisons. Therefore, further exploratory investigations were performed by using a subtraction approach.
3.2.2. Further Exploratory Investigation: Subtraction Analysis Performed on the Whole Sample
- Only tasks for which the maximum lesion overlap in the output image (lesion overlay of pathological patients—lesion overlay of spared patients) was at least >20% are reported (for a complete list of coordinates, see Supplementary Table S1). Local maxima (See Figure 2 and Table 5) were localized as follows:
- for verb naming: in the superior and middle temporal gyrus (25% and 24%);
- for phonological fluency: in the hippocampus (22%) and, at subcortical level, in the retrolenticular part of the internal capsule (26%);
- for short-term memory: in the superior temporal gyrus (30%), and, at subcortical level, in the retrolenticular part of the internal capsule (overlap: 26%) and sagittal stratum (including IFOF and ILF, 26%).
3.2.3. Further Exploratory Investigation: Subtraction Analysis Performed on Part of the Whole Sample
- for word reading, performed by 55/85 patients: in the superior temporal gyrus (57%) and, at subcortical level, in the superior longitudinal fasciculus (57%), the posterior thalamic radiation and the retrolenticular part of the internal capsule (47% and 44%) and the sagittal stratum (including IFOF and ILF, 36%);
- for pseudo-word reading, performed by 55/85 patients: in the calcarine cortex and the middle and inferior temporal gyrus (37%) and, at subcortical level, in the posterior thalamic radiation (39%), in the SLF (37%) and the retrolenticular part of the internal capsule and the tapetum (37%);
- for auditory lexical decision, performed by 41/85 patients: in the superior temporal gyrus (40%) and, at subcortical level, in the sagittal stratum (including IFOF and ILF, 36%);
- for writing, performed by 46/85 patients: in the superior temporal gyrus (58%) and, at subcortical level, in the SLF (45%).
3.2.4. Further Investigations: Intersection Area
4. Discussion
4.1. Neuropsychological Results
4.2. Neuroanatomical Results
4.3. Further Exploratory Neuroanatomical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Louis, D.N.; Perry, A.; Reifenberger, G.; von Deimling, A.; Figarella-Branger, D.; Cavenee, W.K.; Wiestler, O.D.; Kleihues, P.; Ellison, D.W. The 2016 World Health Organization classification of tumors of the central nervous system: A summary. Acta Neuropathol. 2016, 131, 803–820. [Google Scholar] [CrossRef] [Green Version]
- Grech, N.; Dalli, T.; Mizzi, S.; Meilak, L.; Calleja, N.; Zrinzo, A. Rising incidence of glioblastoma multiforme in a well-defined population. Cureus 2020, 12, e8195. [Google Scholar] [CrossRef] [PubMed]
- Habets, E.J.J.; Kloet, A.; Walchenbach, R.; Vecht, C.J.; Klein, M.; Taphoorn, M.J.B. Tumour and surgery effects on cognitive functioning in high-grade glioma patients. Acta Neurochir. 2014, 156, 1451–1459. [Google Scholar] [CrossRef] [PubMed]
- Serventi, J.; Behr, J. Surgery and Evidence-based Treatments in Patients with Newly Diagnosed High-grade Glioma. Semin. Oncol. Nurs. 2018, 34, 443–453. [Google Scholar] [CrossRef] [PubMed]
- Bergo, E.; Lombardi, G.; Guglieri, I.; Capovilla, E.; Pambuku, A.; Zagone, V. Neurocognitive functions and health-related quality of life in glioblastoma patients: A concise review of the literature. Eur. J. Cancer Care 2019, 28, e12410. [Google Scholar] [CrossRef]
- Bosma, I.; Vos, M.J.; Heimans, J.J.; Taphoorn, M.J.; Aaronson, N.K.; Postma, T.J.; van der Ploeg, H.M.; Muller, M.; Vandertop, W.P.; Slotman, B.J.; et al. The course of neurocognitive functioning in high-grade glioma patients. Neuro-Oncology 2007, 9, 53–62. [Google Scholar] [CrossRef]
- Tucha, O.; Smely, C.; Preier, M.; Lange, K.W. Cognitive deficits before treatment among patients with brain tumors. Neurosurgery 2000, 47, 324–334. [Google Scholar] [CrossRef]
- Miotto, E.C.; Junior, A.S.; Silva, C.C.; Cabrera, H.N.; Machado, M.A.; Benute, G.R.; Lucia, M.C.S.; Scaff, M.; Jacobsen, M. Teixeira Cognitive impairments in patients with low grade gliomas and high grade gliomas. Arq. Neuropsiquiatr. 2011, 69, 596–601. [Google Scholar] [CrossRef] [Green Version]
- Hoffermann, M.; Bruckmann, L.; Ali, K.M.; Zaar, K.; Avian, A.; von Campe, G. Pre-and postoperative neurocognitive deficits in brain tumor patients assessed by a computer based screening test. J. Clin. Neurosci. 2017, 36, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Oldfield, R.C. The assessment and analysis of handedness: The Edinburgh Inventory. Neuropsychologia 1971, 9, 97–113. [Google Scholar] [CrossRef]
- Basso, A.; Capitani, E.; Laiacona, M. Raven’s coloured progressive matrices: Normative values on 305 adult normal controls. Funct. Neurol. 1987, 2, 189–194. [Google Scholar] [PubMed]
- Monaco, M.; Costa, A.; Caltagirone, C.; Carlesimo, G.A. Erratum to: Forward and backward span for verbal and visuo-spatial data: Standardization and normative data from an Italian adult population. Neurol. Sci. 2015, 36, 345–347. [Google Scholar] [CrossRef] [Green Version]
- De Renzi, E.; Motti, F.; Nichelli, P. Imitating gestures. A quantitative approach to ideomotor apraxia. Arch. Neurol. 1980, 37, 6–10. [Google Scholar] [CrossRef] [PubMed]
- De Renzi, E.; Piezcuro, A.; Vignolo, L.A. Oral Apraxia and Aphasia. Cortex 1966, 2, 50–73. [Google Scholar] [CrossRef]
- Miceli, G.; Laudanna, A.; Burani, C.; Capasso, R. Batteria Per L’analisi Dei Deficit Afasici: BADA BADA: A Battery for the Assessment of Aphasic Disorders; CEPSAG: Roma, Italy, 1994. [Google Scholar]
- De Renzi, E.; Faglioni, P. Normative data and screening power of a shortened version of the Token Test. Cortex 1978, 14, 41–49. [Google Scholar] [CrossRef]
- Novelli, G.; Papagno, C.; Capitani, E.; Laiacona, M.; Vallar, G.; Cappa, S.F. Tre test clinici di ricerca e produzione lessicale.Taratura su soggetti normali. Arch. Psicol. Neurol. Psichiatr. 1996, 47, 477–505. [Google Scholar]
- Karnath, H.-O.; Berger, M.F.; Zopf, R.; Küker, W. Using SPM normalization for lesion analysis in spatial neglect. Brain 2004, 127, e10. [Google Scholar] [CrossRef] [Green Version]
- Karnath, H.-O.; Berger, M.F.; Küker, W.; Rorden, C. The anatomy of spatial neglect based on voxelwise statistical analysis: A study of 140 patients. Cereb. Cortex 2004, 14, 1164–1172. [Google Scholar] [CrossRef] [PubMed]
- Tzourio-Mazoyer, N.; Landeau, B.; Papathanassiou, D.; Crivello, F.; Etard, O.; Delcroix, N.; Mazoyerc, B.; Joliot, M. Automated anatomical labeling of activations in SPM using a macroscopic anatomical parcellation of the MNI MRI single-subject brain. Neuroimage 2002, 15, 273–289. [Google Scholar] [CrossRef] [PubMed]
- Hua, K.; Zhang, J.; Wakana, S.; Jiang, H.; Li, X.; Reich, D.S.; Calabresi, P.A.; Pekar, J.J.; van Zijl, P.C.M.; Mori, S. Tract probability maps in stereotaxic spaces: Analyses of white matter anatomy and tract-specific quantification. Neuroimage 2008, 39, 336–347. [Google Scholar] [CrossRef] [Green Version]
- Friederici, A.D.; Gierhan, S.M. The language network. Curr. Opin. Neurobiol. 2013, 23, 250–254. [Google Scholar] [CrossRef]
- Hickok, G. The functional neuroanatomy of language. Phys. Life Rev. 2009, 6, 121–143. [Google Scholar] [CrossRef] [Green Version]
- Hickok, G.; Poeppel, D. Towards a functional neuroanatomy of speech perception. Trends Cogn. Sci 2000, 4, 131–138. [Google Scholar] [CrossRef]
- Hickok, G.; Poeppel, D. The cortical organization of speech processing. Nat. Rev. Neurosci. 2007, 8, 393–402. [Google Scholar] [CrossRef]
- Chang, E.F.; Raygor, K.P.; Berger, M.S. Contemporary model of language organization: An overview for neurosurgeons. J. Neurosurg. 2015, 122, 250–261. [Google Scholar] [CrossRef] [PubMed]
- Ries, S.K.; Piai, V.; Perry, D.; Griffin, S.; Jordan, K.; Henry, R.; Knight, R.T.; Berger, M.S. Roles of ventral versus dorsal pathways in language production: An awake language mapping study. Brain Lang. 2019, 191, 17–27. [Google Scholar] [CrossRef]
- Tomasino, B.; Marin, D.; Maieron, M.; Ius, T.; Budai, R.; Fabbro, F.; Skrap, M. Foreign accent syndrome: A multimodal mapping study. Cortex 2013, 49, 18–39. [Google Scholar] [CrossRef] [PubMed]
- Tomasino, B.; Marin, D.; Maieron, M.; D’Agostini, S.; Medeossi, I.; Fabbro, F.; Skrap, M.; Luzzatti, C. A multimodal mapping study of conduction aphasia with impaired repetition and spared reading aloud. Neuropsychologia 2015, 70, 214–226. [Google Scholar] [CrossRef]
- Zheng, G.; Chen, X.; Xu, B.; Zhang, J.; Lv, X.; Li, J.; Li, F.; Hu, S.; Zhang, T.; Li, Y. Plasticity of language pathways in patients with low-grade glioma: A diffusion tensor imaging study. Neural Regen Res. 2013, 8, 647–654. [Google Scholar] [PubMed]
- Tomasino, B.; Tronchin, G.; Marin, D.; Maieron, M.; Fabbro, F.; Cubelli, R.; Skrap, M.; Luzzatti, C. Noun–verb naming dissociation in neurosurgical patients. Aphasiology 2018. [Google Scholar] [CrossRef]
- Berlingeri, M.; Crepaldi, D.; Roberti, R.; Scialfa, G.; Luzzatti, C.; Paulesu, E. Nouns and verbs in the brain: Grammatical class and task specific effects as revealed by fMRI. Cogn. Neuropsychol. 2008, 25, 528–558. [Google Scholar] [CrossRef] [Green Version]
- Boylan, C.; Trueswell, J.C.; Thompson-Schill, S.L. Multi-voxel pattern analysis of noun and verb differences in ventral temporal cortex. Brain Lang. 2014, 137, 40–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shapiro, K.A.; Mottaghy, F.M.; Schiller, N.O.; Poeppel, T.D.; Fluss, M.O.; Muller, H.W.; Caramazza, A.; Krause, B.J. Dissociating neural correlates for nouns and verbs. Neuroimage 2005, 24, 1058–1067. [Google Scholar] [CrossRef] [Green Version]
- Shapiro, K.A.; Moo, L.R.; Caramazza, A. Cortical signatures of noun and verb production. Proc. Natl. Acad. Sci. USA 2006, 103, 1644–1649. [Google Scholar] [CrossRef] [Green Version]
- Binder, J.R.; Desai, R.H.; Graves, W.W.; Conant, L.L. Where Is the Semantic System? A Critical Review and Meta-Analysis of 120 Functional Neuroimaging Studies. Cereb. Cortex 2009, 19, 2767–2796. [Google Scholar] [CrossRef]
- Crepaldi, D.; Berlingheri, M.; Cattinelli, I.; Borghese, N.A.; Luzzatti, C.; Paulesu, E. Clustering the Lexicon in the Brain: A Meta-Analysis of the Neurofunctional Evidence on Noun and Verb Processing. Front. Hum. Neurosci. 2013, 7, 303. [Google Scholar] [CrossRef] [Green Version]
- Kümmerer, D.; Hartwigsen, G.; Kellmeyer, P.; Glauche, V.; Mader, I.; Klöppel, S.; Suchan, J.; Karnath, H.-O.; Weiller, C.; Saur, D. Damage to ventral and dorsal language pathways in acute aphasia. Brain A J. Neurol. 2013, 136, 619–629. [Google Scholar] [CrossRef] [Green Version]
- Pisoni, A.; Mattavelli, G.; Casarotti, A.; Comi, A.; Riva, M.; Bello, L.; Papagno, C. The neural correlates of auditory-verbal short-term memory: A voxel-based lesion-symptom mapping study on 103 patients after glioma removal. Brain Struct. Funct. 2019, 224, 2199–2211. [Google Scholar] [CrossRef] [PubMed]
- Xiao, Z.; Zhang, J.X.; Wang, X.; Wu, R.; Hu, X.; Weng, X.; Tan, L.H. Differential activity in left inferior frontal gyrus for pseudowords and real words: An event-related fMRI study on auditory lexical decision. Hum. Brain Mapp. 2005, 25, 212–221. [Google Scholar] [CrossRef]
- Specht, K.; Holtel, C.; Zahn, R.; Herzog, H.; Krause, B.J.; Mottaghy, F.M.; Radermacher, I.; Schmidt, D.; Tellmann, L.; Weis, S.; et al. Lexical decision of nonwords and pseudowords in humans: A positron emission tomography study. Neurosci. Lett. 2003, 345, 177–181. [Google Scholar] [CrossRef]
- Cohen, L.; Dehaene, S.; Naccache, L.; Lehericy, S.; Dehaene-Lambertz, G.; Henaff, M.A.; Michel, F. The visual word form area: Spatial and temporal characterization of an initial stage of reading in normal subjects and posterior split-brain patients. Brain 2000, 123, 291–307. [Google Scholar] [CrossRef] [Green Version]
- Simos, P.G.; Breier, J.I.; Wheless, J.W.; Maggio, W.W.; Fletcher, J.M.; Castillo, E.M.; Papanicolaou, A.C. Brain mechanisms for reading: The role of the superior temporal gyrus in word and pseudoword naming. Neuro. Rep. 2000, 11, 2443–2446. [Google Scholar] [CrossRef] [PubMed]
- Jobard, G.; Crivello, F.; Tzourio-Mazoyer, N. Evaluation of the dual route theory of reading: A metanalysis of 35 neuroimaging studies. Neuroimage 2003, 20, 693–712. [Google Scholar] [CrossRef]
- Vandermosten, M.; Boets, B.; Wouters, J.; Ghesquiere, P. A qualitative and quantitative review of diffusion tensor imaging studies in reading and dyslexia. Neurosci. Biobehav. Rev. 2012, 36, 1532–1552. [Google Scholar] [CrossRef] [PubMed]
- Vandermosten, M.; Boets, B.; Poelmans, H.; Sunaert, S.; Wouters, J.; Ghesquiere, P. A tractography study in dyslexia: Neuroanatomic correlates of orthographic, phonological and speech processing. Brain 2012, 135, 935–948. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burton, M.W.; Small, S.L.; Blumstein, S.E. The role of segmentation in phonological processing: An fMRI investigation. J. Cogn. Neurosci. 2000, 12, 679–690. [Google Scholar] [CrossRef] [Green Version]
- Pugh, K.R.; Mencl, W.E.; Shaywitz, B.A.; Shaywitz, S.E.; Fulbright, R.K.; Constable, R.T.; Skudlarski, P.; Marchione, K.E.; Jenner, A.R.; Fletcher, J.M.; et al. The angular gyrus in developmental dyslexia: Task-specific differences in functional connectivity within posterior cortex. Psychol. Sci. 2000, 11, 51–56. [Google Scholar] [CrossRef]
- Rapcsak, S.Z.; Beeson, P.M.; Henry, M.L.; Leyden, A.; Kim, E.; Rising, K.; Andersen, S.; Cho, H. Phonological dyslexia and dysgraphia: Cognitive mechanisms and neural substrates. Cortex 2009, 45, 575–591. [Google Scholar] [CrossRef] [Green Version]
- Roux, F.E.; Durand, J.B.; Rehault, E.; Planton, S.; Draper, L.; Demonet, J.F. The neural basis for writing from dictation in the temporoparietal cortex. Cortex 2014, 50, 64–75. [Google Scholar] [CrossRef]
- Shinoura, N.; Midorikawa, A.; Onodera, T.; Yamada, R.; Tabei, Y.; Onda, Y.; Itoi, C.; Saito, S.; Yagi, K. The left superior longitudinal fasciculus within the primary sensory area of inferior parietal lobe plays a role in dysgraphia of kana omission within sentences. Behav. Neurol. 2012, 25, 363–368. [Google Scholar] [CrossRef]
- Crosson, B.A. Subcortical Functions in Language and Memory; Guilford Press: New York, NY, USA, 1992. [Google Scholar]
- Klostermann, F.; Krugel, L.K.; Ehlen, F. Functional roles of the thalamus for language capacities. Front. Syst. Neurosci. 2013, 7, 32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murdoch, B.E. Speech and Language Disorders Associated with Subcortical Pathology; John Wiley & Sons: Hoboken, NJ, USA, 2009. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Parameter | Value |
|---|---|
| No. of patients | n = 85 |
| Age (years) | Mean = 57.68; sd = 10.72; range 26–74 years |
| School (years) | Mean = 11.36; sd = 4.18; range 5–18 years |
| Handedness | Right = 83 patients; left = 2 patients |
| Sex | 53 males; 33 females |
| Tumor volume | Mean = 43.74, sd = 38.57; range 1.43–260.15 |
| WHO grade | III = 8 patients; IV = 77 patients |
| Edema | Present = 44 patients; absent = 41 patients |
| Signs and Symptoms | No. of Patients | Percentages Positive for Each Symptom | 95% Confidence Interval Lower | 95% Confidence Interval Upper |
|---|---|---|---|---|
| Language disorders (anomia, paraphasia, writing and reading) | 36 | 42.35 | 32 | 53 |
| Tingling (face and/or limbs) | 9 | 10.59 | 4 | 17 |
| Seizures | 13 | 15.29 | 7 | 23 |
| Emotional lability | 1 | 1.18 | −1 | 4 |
| Memory difficulty | 3 | 3.53 | 0 | 8 |
| Attention deficit | 2 | 2.35 | −1 | 6 |
| Clonia (face and/or limbs) | 7 | 8.24 | 2 | 14 |
| Vomiting | 3 | 3.53 | 0 | 8 |
| Ear disorders | 1 | 1.18 | −1 | 4 |
| Dizziness and/or head turns | 2 | 2.35 | −1 | 6 |
| Visual disturbances (hempianopsia) | 4 | 4.71 | 0 | 9 |
| Loss of balance | 1 | 1.18 | −1 | 4 |
| Strength loss | 5 | 5.88 | 0 | 11 |
| Headaches | 6 | 7.06 | 2 | 13 |
| Paresis | 2 | 2.35 | −1 | 6 |
| Agitation | 1 | 1.18 | −1 | 4 |
| Praxis deficit | 3 | 3.53 | 0 | 8 |
| Confusion | 9 | 10.59 | 4 | 1.7 |
| Cacosmia or perception of perfumes | 2 | 2.35 | −1 | 6 |
| Test | No. of Patients Performing the Task | % Pathological | Accuracy Mean % or Mean Performance | SD | Min | Max | 95% Confidence Interval Lower | 95% Confidence Interval Upper |
|---|---|---|---|---|---|---|---|---|
| Verb naming | 85 | 61.45 | 82.27 | 17.97 | 17.86 | 100.00 | 78.34 | 86.19 |
| Object naming | 85 | 42.17 | 85.50 | 20.05 | 3.33 | 100.00 | 81.12 | 89.88 |
| Ideomotor apraxia | 85 | 10.98 | 92.08 | 15.97 | 8.33 | 100.00 | 88.54 | 95.6 |
| Oral Praxis | 85 | 2.44 | 97.20 | 8.43 | 40.00 | 100.00 | 95.34 | 99.04 |
| Token Test | 85 | 23.75 | 80.68 | 18.97 | 9.72 | 100.00 | 76.45 | 84.89 |
| Digit span forward | 79 | 36.71 | 4.81 | 1.05 | 2.77 | 7.23 | 4.56 | 5.03 |
| Raven Matrices | 85 | 0.00 | 83.76 | 10.26 | 62.5 | 100.00 | 81.44 | 86.07 |
| Phonological Fluency | 76 | 36.84 | 24.1 | 13 | 1 | 52 | 20.75 | 26.79 |
| Working Memory | 75 | 37.33 | 3.07 | 0.93 | 1.5 | 5.64 | 2.85 | 3.28 |
| Pseudoword repetition | 57 | 21.05 | 94.35 | 16.22 | 0.10 | 100.00 | 90.04 | 98.65 |
| Words repetition | 57 | 14.04 | 96.90 | 13.87 | 0.10 | 100.00 | 93.22 | 100.58 |
| Word reading | 55 | 36.36 | 93.17 | 16.35 | 0.10 | 100.00 | 88.75 | 97.59 |
| Pseudoword reading | 55 | 34.55 | 87.11 | 23.97 | 0.10 | 100.00 | 80.63 | 93.59 |
| Word and pseudoword writing | 46 | 41.30 | 89.33 | 14.28 | 24.00 | 100.00 | 85.08 | 93.56 |
| Auditory comprehension: verb | 43 | 9.30 | 97.20 | 5.61 | 85.00 | 100.00 | 96.92 | 99.35 |
| Auditory comprehension: object | 42 | 14.29 | 98.14 | 3.94 | 72.50 | 100.00 | 95.45 | 98.95 |
| Phonological Discrimination | 42 | 2.38 | 97.74 | 13.36 | 13.33 | 100.00 | 93.57 | 101.9 |
| Auditory lexical decision | 41 | 48.78 | 91.33 | 19.52 | 1.57 | 100.00 | 84.99 | 97.65 |
| Area 1 | No. of Voxels | % of tot | Max Z-Score | x | y | z |
|---|---|---|---|---|---|---|
| Naming | ||||||
| Superior Temporal Gyrus | 2716 | 10.75 | 7.15 | 43 | −38 | 12 |
| Middle Temporal Gyrus | 8509 | 23.97 | 3.89 | 49 | −35 | −13 |
| Inferior Temporal Gyrus | 3671 | 12.89 | 3.89 | 53 | −13 | −32 |
| Fusiform gyrus | 2684 | 13.26 | 3.89 | 44 | −31 | −17 |
| Hippocampus | 1160 | 15.25 | 3.89 | 31 | −36 | −4 |
| Parahippocampal area | 996 | 11.03 | 3.89 | 33 | −40 | −7 |
| Precuneus | 274 | 1.05 | 3.71 | 27 | −49 | 5 |
| Calcarine cortex | 454 | 3.05 | 3.71 | 26 | −48 | 6 |
| Supramarginal gyrus | 126 | 0.79 | 3.61 | 57 | −25 | 19 |
| Lingual gyrus | 121 | 0.65 | 3.61 | 27 | −45 | −3 |
| Middle frontal gyrus | 83 | 0.2 | 2.84 | 33 | 12 | 37 |
| Posterior thalamic radiation | 1912 | 48 | 3.89 | 34 | −47 | −3 |
| Sagittal stratum (IFOF+ILF) | 1041 | 46 | 3.89 | 41 | −34 | −14 |
| Superior longitudinal fasciculus | 950 | 14 | 6.12 | 40 | −41 | 14 |
| Retrolenticular part of the internal capsule | 725 | 29 | 3.89 | 35 | −38 | −3 |
| Fornix | 257 | 22 | 3.89 | 29 | −29 | −4 |
| Tapetum | 257 | 42 | 3.89 | 30 | −44 | 8 |
| Token Test | ||||||
| Superior temporal gyrus | 2577 | 10.21 | 3.89 | 43 | −41 | 5 |
| Middle temporal gyrus | 9295 | 26.19 | 3.89 | 49 | −35 | −13 |
| Inferior temporal gyrus | 4503 | 15.81 | 4.83 | 45 | −21 | −20 |
| Fusiform gyrus | 1606 | 7.93 | 5.11 | 44 | −24 | −16 |
| Hippocampus | 1038 | 13.64 | 4.31 | 37 | −31 | −6 |
| Parahippocampal area | 306 | 3.38 | 3.61 | 35 | −41 | −4 |
| Calcarine cortex | 829 | 5.56 | 3.89 | 27 | −50 | 5 |
| Supramarginal gyrus | 32 | 0.21 | 2.86 | 45 | −34 | 24 |
| Lingual gyrus | 86 | 0.46 | 3.71 | 23 | −51 | 4 |
| Precuneus | 221 | 0.84 | 3.89 | 27 | −47 | 5 |
| Superior temporal pole | 134 | 1.25 | 3.01 | 61 | 4 | −8 |
| Heschl’s gyrus | 43 | 2.22 | 3.41 | 39 | −26 | 9 |
| Rolandic operculum | 21 | 0.19 | 2.91 | 45 | −29 | 20 |
| Posterior thalamic radiation | 2070 | 52 | 3.89 | 37 | −42 | −3 |
| Sagittal stratum (IFOF+ILF) | 1416 | 63 | 4.31 | 37 | −31 | −6 |
| Retrolenticular part of the internal capsule | 1074 | 43 | 5.15 | 38 | −31 | −1 |
| Superior longitudinal fasciculus | 840 | 12 | 3.89 | 41 | −48 | 2 |
| Tapetum | 285 | 47 | 3.89 | 28 | −48 | 7 |
| Fornix | 59 | 5 | 3.35 | 29 | −32 | −1 |
| Splenium of the corpus callosum | 34 | 26 | 3.13 | 21 | −54 | 8 |
| Posterior corona radiata | 18 | 48 | 3.19 | 29 | −40 | 19 |
| Area | % Overlap | x | y | z |
|---|---|---|---|---|
| Reading pseudowords | ||||
| Calcarine gyrus | 37 | 27 | −52 | 11 |
| Middle temporal gyrus | 37 | 45 | −48 | −3 |
| Inferior temporal gyrus | 37 | 47 | −45 | −4 |
| Posterior thalamic radiation | 39 | 34 | −46 | 10 |
| Retrolenticular part of the internal capsule | 37 | 30 | −37 | 13 |
| Posterior corona radiata | 37 | 27 | −42 | 19 |
| Superior longitudinal fasciculus | 37 | 37 | −52 | 14 |
| Tapetum | 37 | 27 | −52 | 11 |
| Reading words | ||||
| Calcarine gyrus | 37 | 27 | −52 | 11 |
| Middle temporal gyrus | 37 | 45 | −48 | −3 |
| Inferior temporal gyrus | 37 | 47 | −45 | −4 |
| Posterior thalamic radiation | 39 | 34 | −46 | 10 |
| Retrolenticular part of the internal capsule | 37 | 30 | −37 | 13 |
| Posterior corona radiata | 37 | 27 | −42 | 19 |
| Auditory lexical decision | ||||
| Calcarine gyrus | 37 | 27 | −52 | 11 |
| Middle temporal gyrus | 37 | 45 | −48 | −3 |
| Inferior temporal gyrus | 37 | 47 | −45 | −4 |
| Posterior thalamic radiation | 39 | 34 | −46 | 10 |
| Writing | ||||
| Calcarine gyrus | 37 | 27 | −52 | 11 |
| Middle temporal gyrus | 37 | 45 | −48 | −3 |
| Short-term memory | ||||
| Calcarine gyrus | 37 | 27 | −52 | 11 |
| Middle temporal gyrus | 37 | 45 | −48 | −3 |
| Inferior temporal gyrus | 37 | 47 | −45 | −4 |
| Verb naming | ||||
| Calcarine gyrus | 37 | 27 | −52 | 11 |
| Middle temporal gyrus | 37 | 45 | −48 | −3 |
| Phonological fluency | ||||
| Calcarine gyrus | 37 | 27 | −52 | 11 |
| Middle temporal gyrus | 37 | 45 | −48 | −3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guarracino, I.; Ius, T.; Baiano, C.; D’Agostini, S.; Skrap, M.; Tomasino, B. Pre-Surgery Cognitive Performance and Voxel-Based Lesion-Symptom Mapping in Patients with Left High-Grade Glioma. Cancers 2021, 13, 1467. https://doi.org/10.3390/cancers13061467
Guarracino I, Ius T, Baiano C, D’Agostini S, Skrap M, Tomasino B. Pre-Surgery Cognitive Performance and Voxel-Based Lesion-Symptom Mapping in Patients with Left High-Grade Glioma. Cancers. 2021; 13(6):1467. https://doi.org/10.3390/cancers13061467
Chicago/Turabian StyleGuarracino, Ilaria, Tamara Ius, Cinzia Baiano, Serena D’Agostini, Miran Skrap, and Barbara Tomasino. 2021. "Pre-Surgery Cognitive Performance and Voxel-Based Lesion-Symptom Mapping in Patients with Left High-Grade Glioma" Cancers 13, no. 6: 1467. https://doi.org/10.3390/cancers13061467
APA StyleGuarracino, I., Ius, T., Baiano, C., D’Agostini, S., Skrap, M., & Tomasino, B. (2021). Pre-Surgery Cognitive Performance and Voxel-Based Lesion-Symptom Mapping in Patients with Left High-Grade Glioma. Cancers, 13(6), 1467. https://doi.org/10.3390/cancers13061467