
Biomarkers Associated with Regorafenib First-Line Treatment Benefits in Metastatic Colorectal Cancer Patients: REFRAME Molecular Study

 ,
,  ,
,  , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Results
2.1. Identification and Selection of Serum miRNAs Differentially Expressed in mCRC Patients Associated with Regorafenib Response
- Six pre-treatment serum samples from the favorable group: complete response (CR) + partial response (PR) + stable disease (SD)
- Six pre-treatment serum samples from the non-favorable group: progression of disease (PD)
2.2. Serum miRNAs as Biomarkers of Treatment Response to Regorafenib
2.3. Serum miRNAs as Biomarkers of Risk of Toxicity Associated with Regorafenib
2.4. Tissue miRNAs as Biomarkers of Response and Toxicity Risk in Primary Tumor Diagnostic Biopsies
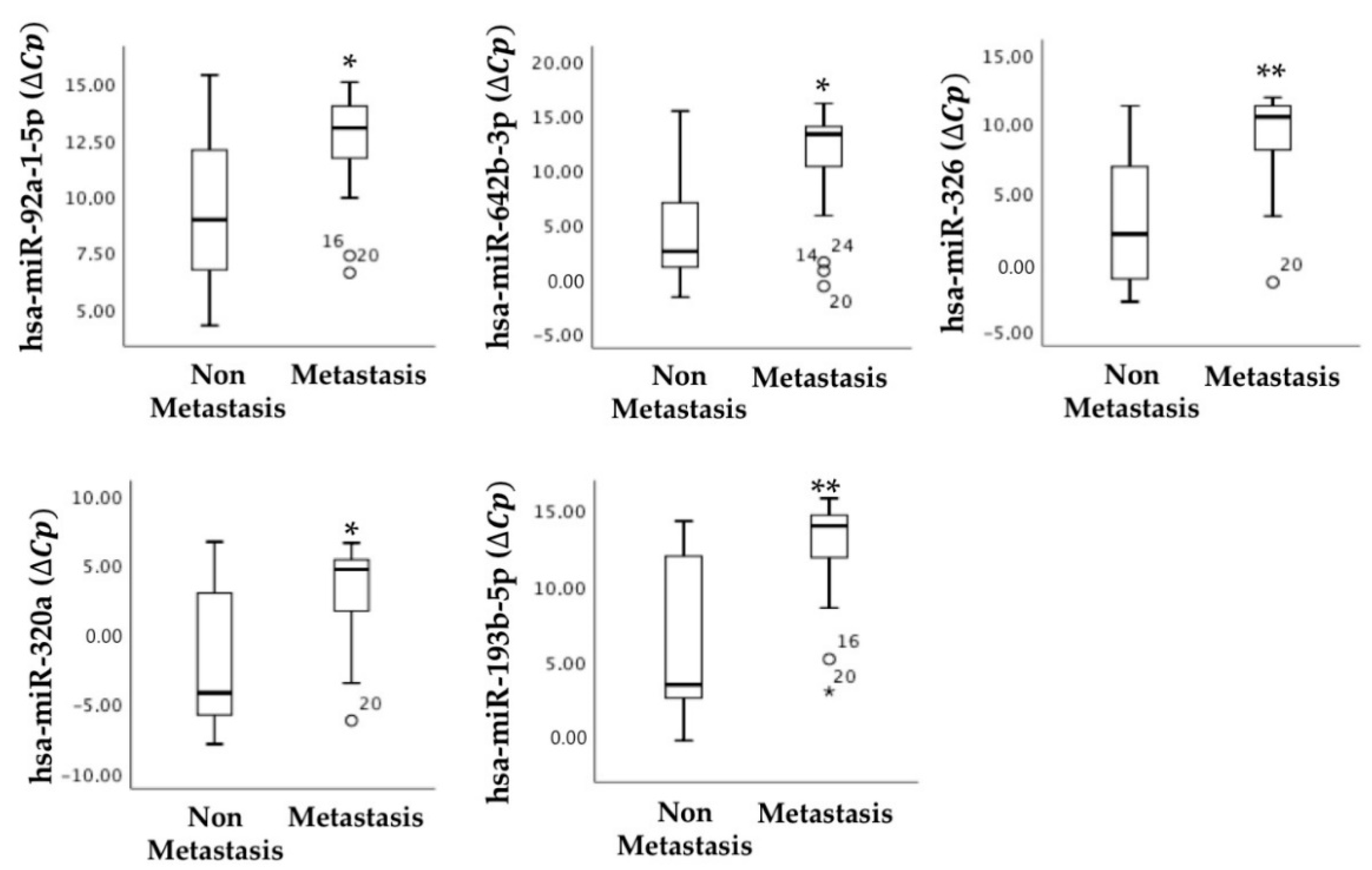
2.5. Primary Tumor miRNAs Associated with Tumor Staging
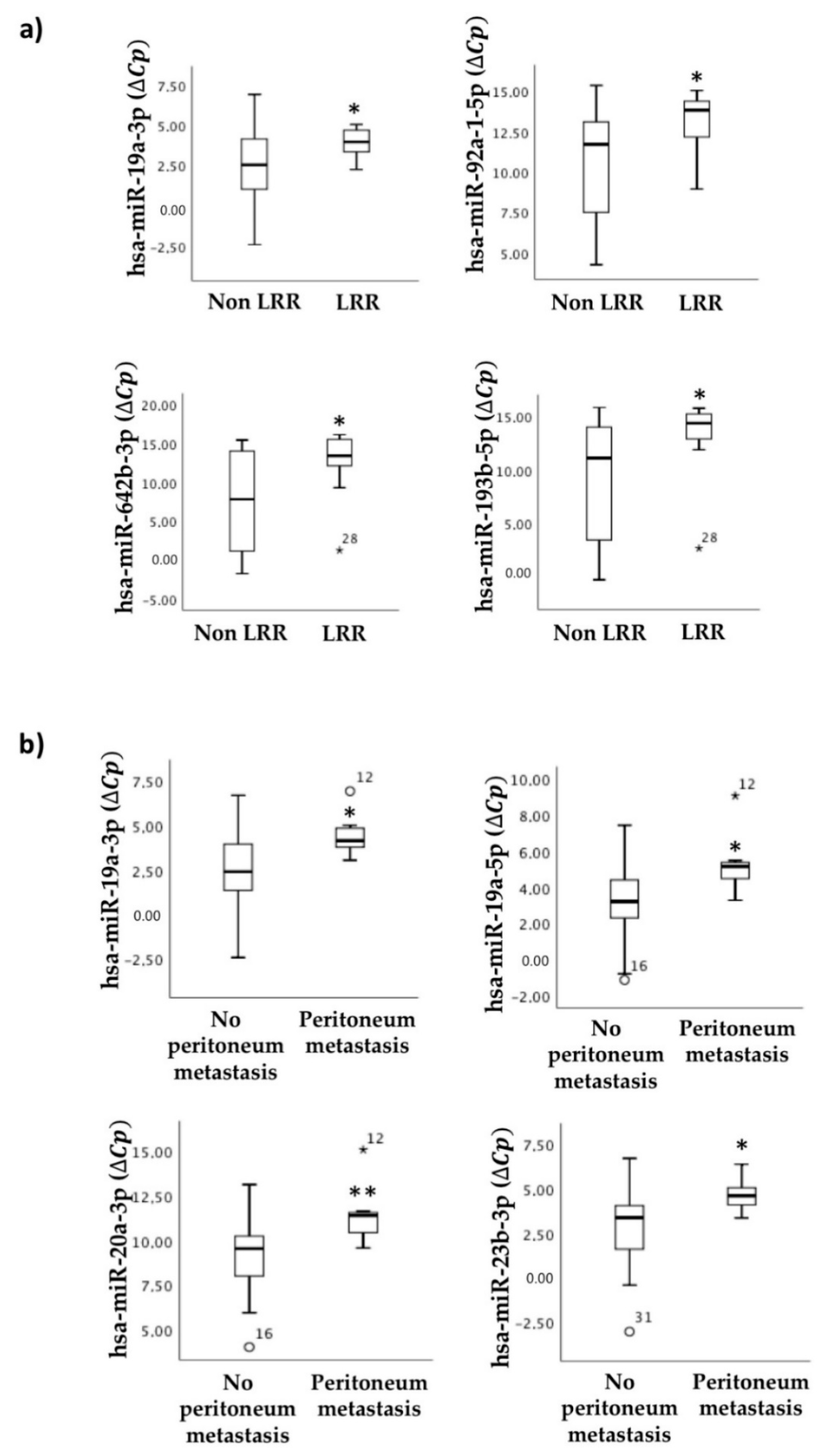
2.6. miRNAs as Indicators of CRC Progression during Regorafenib Treatment: Association with Locoregional Recurrence and Peritoneal Metastasis
2.7. Pharmacogenetic Markers in Blood: Analysis of the Association of SNP Variants with Prognosis and Response to CRC Treatment with Regorafenib
2.8. Pharmacogenetic Markers in Blood: Analysis of the Association of SNP Variants with Other Clinical and Tumor Characteristics
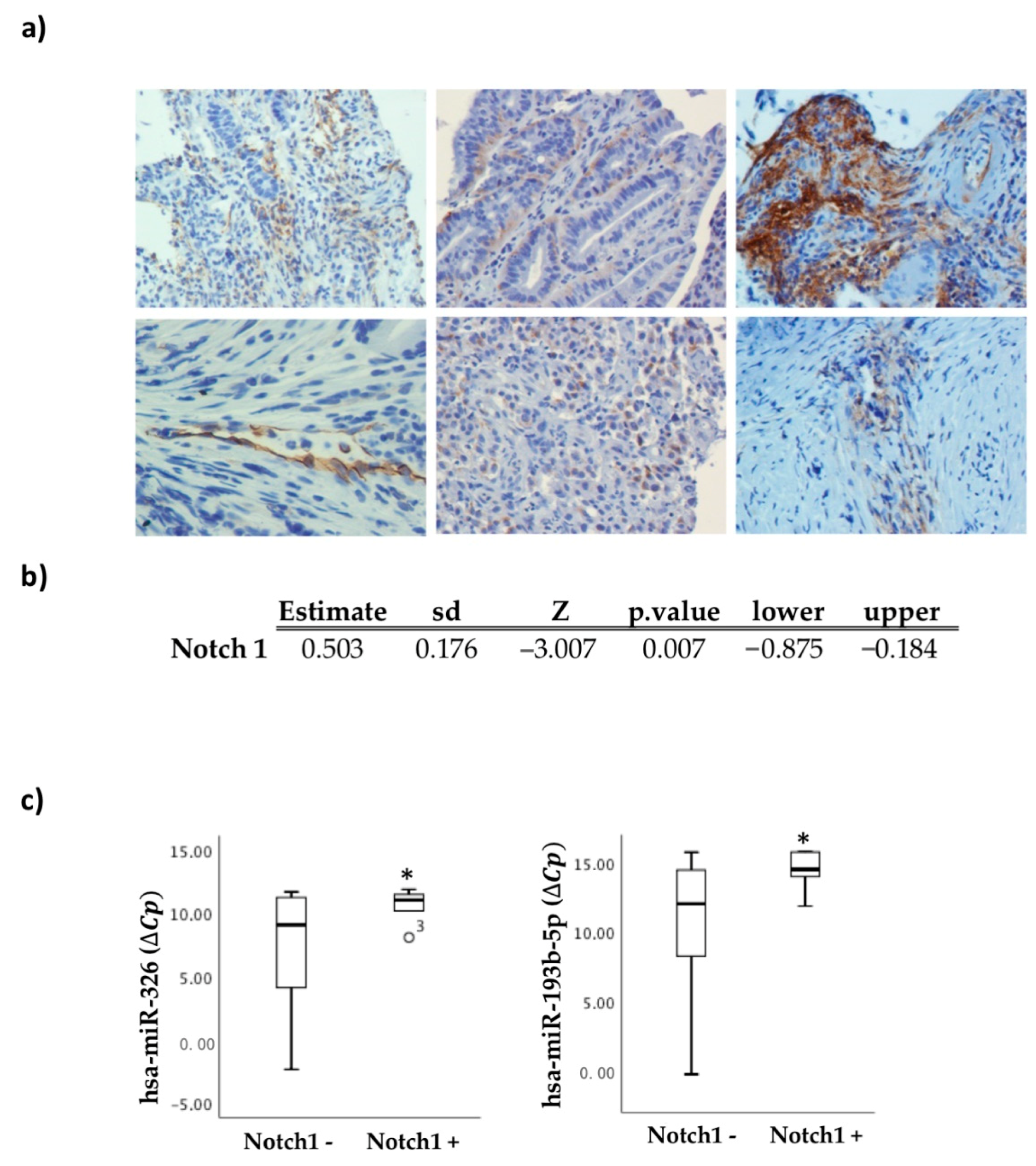
2.9. Notch 1 Expression in the Biopsy as a Useful Marker of Regorafenib Treatment Response
2.10. Association Analysis of the Studied Biomarkers with Progression-Free Survival (PFS) and Overall Survival (OS) upon Regorafenib Treatment
3. Discussion
3.1. Serum miRNAs as Biomarkers of Response and Toxicity
3.2. SNPs in the VEGF Axis as Biomarkers of Response and Toxicity
3.3. Other Biomarkers of Response to Regorafenib
3.4. Added Value of miRNAs Detected in Primary Tumor Biopsies
3.5. Study Limitations
4. Materials and Methods
4.1. Study Design
4.2. Patients and Sampling
- Favorable/non-favorable outcome groups:
- ○
- Favorable: patients with complete and a partial response (N = 3) and stable disease (N = 22)
- ○
- Non-favorable: patients with progressive disease (N = 10)
- Responder/non-responder group:
- ○
- Responders: patients with a complete and a partial response (N = 3)
- ○
- Non-responders: patients with stable disease (N = 22) and progressive disease (N = 10)
4.3. Total RNA Extraction
4.3.1. In Serum Samples
4.3.2. In Paraffin-Embedded Tumor Biopsies
4.3.3. MicroRNA Array Profiling
4.4. Validation of Selected miRNAs by RT-qPCR
4.5. Genotyping of Single-Nucleotide Polymorphisms (SNPs) in Angiogenesis-Associated Genes
4.6. Immunohistochemistry
4.7. Bioinformatics Studies
4.8. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rawla, P.; Sunkara, T.; Gaduputi, V. Epidemiology of Pancreatic Cancer: Global Trends, Etiology and Risk Factors. World J. Oncol. 2019, 10, 10–27. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Goding Sauer, A.; Fedewa, S.A.; Butterly, L.F.; Anderson, J.C.; Cercek, A.; Smith, R.A.; Jemal, A. Colorectal cancer statistics, 2020. CA Cancer J. Clin. 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aparicio, T.; Pamoukdjian, F.; Quero, L.; Manfredi, S.; Wind, P.; Paillaud, E. Colorectal cancer care in elderly patients: Unsolved issues. Dig. Liver Dis. 2016, 48, 1112–1118. [Google Scholar] [CrossRef] [PubMed]
- Carrato, A.; Benavides, M.; Massutí, B.; Ferreiro-Monteagudo, R.; García Alfonso, P.; Falcó, E.; Reboredo, M.; Cano, T.; Gallego, J.; Viéitez, J.M.; et al. First-line single-agent regorafenib in frail patients with metastatic colorectal cancer: A pilot phase II study of the Spanish Cooperative Group for the Treatment of Digestive Tumours (TTD). BMC Cancer 2019, 19. [Google Scholar] [CrossRef]
- Ha, M.; Kim, V.N. Regulation of microRNA biogenesis. Nat. Rev. Mol. Cell Biol. 2014, 15, 509–524. [Google Scholar] [CrossRef]
- Lee, L.W.; Zhang, S.; Etheridge, A.; Ma, L.; Martin, D.; Galas, D.; Wang, K. Complexity of the microRNA repertoire revealed by next-generation sequencing. RNA 2010, 16, 2170–2180. [Google Scholar] [CrossRef] [Green Version]
- Balacescu, O.; Sur, D.; Cainap, C.; Visan, S.; Cruceriu, D.; Manzat-Saplacan, R.; Muresan, M.S.; Balacescu, L.; Lisencu, C.; Irimie, A. The impact of miRNA in colorectal cancer progression and its liver metastases. Int. J. Mol. Sci. 2018, 19, 3711. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Chen, J.; Sen, S. MicroRNA as Biomarkers and Diagnostics. J. Cell. Physiol. 2016, 231, 25–30. [Google Scholar] [CrossRef]
- Patel, N.; Sauter, E.R. Body fluid micro(mi)RNAs as biomarkers for human cancer. J. Nucleic Acids Investig. 2011, 2, 1–4. [Google Scholar] [CrossRef] [Green Version]
- Wilhelm, S.M.; Dumas, J.; Adnane, L.; Lynch, M.; Carter, C.A.; Schütz, G.; Thierauch, K.-H.; Zopf, D. Regorafenib (BAY 73-4506): A new oral multikinase inhibitor of angiogenic, stromal and oncogenic receptor tyrosine kinases with potent preclinical antitumor activity. Int. J. Cancer 2011, 129, 245–255. [Google Scholar] [CrossRef]
- Eisen, T.; Joensuu, H.; Nathan, P.D.; Harper, P.G.; Wojtukiewicz, M.Z.; Nicholson, S.; Bahl, A.; Tomczak, P.; Pyrhonen, S.; Fife, K.; et al. Regorafenib for patients with previously untreated metastatic or unresectable renal-cell carcinoma: A single-group phase 2 trial. Lancet Oncol. 2012, 13, 1055–1062. [Google Scholar] [CrossRef]
- Tabernero, J.; Lenz, H.-J.; Siena, S.; Sobrero, A.; Falcone, A.; Ychou, M.; Humblet, Y.; Bouché, O.; Mineur, L.; Barone, C.; et al. Analysis of circulating DNA and protein biomarkers to predict the clinical activity of regorafenib and assess prognosis in patients with metastatic colorectal cancer: A retrospective, exploratory analysis of the CORRECT trial. Lancet Oncol. 2015, 16, 937–948. [Google Scholar] [CrossRef]
- Schneider, B.P.; Shen, F.; Miller, K.D. Pharmacogenetic biomarkers for the prediction of response to antiangiogenic treatment. Lancet Oncol. 2012, 13, e427–e436. [Google Scholar] [CrossRef] [Green Version]
- Rogers, M.S.; D’Amato, R.J. Common polymorphisms in angiogenesis. Cold Spring Harb. Perspect. Med. 2012, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Habboubi, H.H.; Sater, M.S.; Almawi, A.W.; Al-Khateeb, G.M.; Almawi, W.Y. Contribution of VEGF polymorphisms to variation in VEGF serum levels in a healthy population. Eur. Cytokine Netw. 2011, 22, 154–158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siebel, C.; Lendahl, U. Notch signaling in development, tissue homeostasis, and disease. Physiol. Rev. 2017, 97, 1235–1294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mirone, G.; Perna, S.; Shukla, A.; Marfe, G. Involvement of Notch-1 in Resistance to Regorafenib in Colon Cancer Cells. J. Cell. Physiol. 2016, 231, 1097–1105. [Google Scholar] [CrossRef] [PubMed]
- Moreno, E.C.; Pascual, A.; Prieto-Cuadra, D.; Laza, V.F.; Molina-Cerrillo, J.; Ramos-Muñoz, M.E.; Rodríguez-Serrano, E.M.; Soto, J.L.; Carrato, A.; García-Bermejo, M.L.; et al. Novel Molecular Characterization of Colorectal Primary Tumors Based on miRNAs. Cancers 2019, 11, 346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papamichael, D.; Audisio, R.A.; Glimelius, B.; de Gramont, A.; Glynne-Jones, R.; Haller, D.; Köhne, C.H.; Rostoft, S.; Lemmens, V.; Mitry, E.; et al. Treatment of colorectal cancer in older patients: International Society of Geriatric Oncology (SIOG) consensus recommendations 2013. Ann. Oncol. 2015, 26, 463–476. [Google Scholar] [CrossRef]
- Seymour, M.T.; Thompson, L.C.; Wasan, H.S.; Middleton, G.; Brewster, A.E.; Shepherd, S.F.; O’Mahony, M.S.; Maughan, T.S.; Parmar, M.; Langley, R.E. Chemotherapy options in elderly and frail patients with metastatic colorectal cancer (MRC FOCUS2): An open-label, randomised factorial trial. Lancet 2011, 377, 1749–1759. [Google Scholar] [CrossRef] [Green Version]
- Saif, M.W. Chemotherapy options in elderly and frail patients with metastatic colorectal cancer. Ann. Gastroenterol. 2012, 25, 274–275. [Google Scholar]
- Teufel, M.; Seidel, H.; Köchert, K.; Meinhardt, G.; Finn, R.S.; Llovet, J.M.; Bruix, J. Biomarkers Associated With Response to Regorafenib in Patients With Hepatocellular Carcinoma. Gastroenterology 2019, 156, 1731–1741. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wei, F.; Wang, M.; Li, Z.; Wang, Y.; Zhou, Y. Long Non-coding RNA MIR570MG Causes Regorafenib Resistance in Colon Cancer by Repressing miR-145/SMAD3 Signaling. Front. Oncol. 2020, 10. [Google Scholar] [CrossRef] [PubMed]
- Cai, M.-H.; Xu, X.-G.; Yan, S.-L.; Sun, Z.; Ying, Y.; Wang, B.-K.; Tu, Y.-X. Regorafenib suppresses colon tumorigenesis and the generation of drug resistant cancer stem-like cells via modulation of miR-34a associated signaling. J. Exp. Clin. Cancer Res. 2018, 37, 151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shrestha, S.; Shrestha, S.; Khanal, S. Polypharmacy in elderly cancer patients: Challenges and the way clinical pharmacists can contribute in resource-limited settings. Aging Med. 2019, 2, 42–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Extermann, M.; Boler, I.; Reich, R.R.; Lyman, G.H.; Brown, R.H.; Defelice, J.; Levine, R.M.; Lubiner, E.T.; Reyes, P.; Schreiber, F.J.; et al. Predicting the risk of chemotherapy toxicity in older patients: The chemotherapy risk assessment scale for high-age patients (CRASH) score. Cancer 2012, 118, 3377–3386. [Google Scholar] [CrossRef]
- Hurria, A.; Togawa, K.; Mohile, S.G.; Owusu, C.; Klepin, H.D.; Gross, C.P.; Lichtman, S.M.; Gajra, A.; Bhatia, S.; Katheria, V.; et al. Predicting chemotherapy toxicity in older adults with cancer: A prospective multicenter study. J. Clin. Oncol. 2011, 29, 3457–3465. [Google Scholar] [CrossRef] [Green Version]
- Schneider, B.P.; Wang, M.; Radovich, M.; Sledge, G.W.; Badve, S.; Thor, A.; Flockhart, D.A.; Hancock, B.; Davidson, N.; Gralow, J.; et al. Association of Vascular Endothelial Growth Factor and Vascular Endothelial Growth Factor Receptor-2 Genetic Polymorphisms With Outcome in a Trial of Paclitaxel. J. Clin. Oncol. 2008, 26, 4672–4678. [Google Scholar] [CrossRef]
- Miller, K.D. E2100: A phase III trial of paclitaxel versus paclitaxel/bevacizumab for metastatic breast cancer. Clin. Breast Cancer 2003, 3, 421–422. [Google Scholar] [CrossRef]
- Miles, D.W.; De Haas, S.L.; Dirix, L.Y.; Romieu, G.; Chan, A.; Pivot, X.; Tomczak, P.; Provencher, L.; Cortés, J.; Delmar, P.R.; et al. Biomarker results from the AVADO phase 3 trial of first-line bevacizumab plus docetaxel for HER2-negative metastatic breast cancer. Br. J. Cancer 2013, 108, 1052–1060. [Google Scholar] [CrossRef]
- Kim, D.H.; Xu, W.; Kamel-Reid, S.; Liu, X.; Jung, C.W.; Kim, S.; Lipton, J.H. Clinical relevance of vascular endothelial growth factor (VEGFA) and VEGF receptor (VEGFR2) gene polymorphism on the treatment outcome following imatinib therapy. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2010, 21, 1179–1188. [Google Scholar] [CrossRef] [PubMed]
- Sandler, A.; Gray, R.; Perry, M.C.; Brahmer, J.; Schiller, J.H.; Dowlati, A.; Lilenbaum, R.; Johnson, D.H. Paclitaxel-carboplatin alone or with bevacizumab for non-small-cell lung cancer. N. Engl. J. Med. 2006, 355, 2542–2550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giampieri, R.; Salvatore, L.; Del Prete, M.; Prochilo, T.; Danzeo, M.; Loretelli, C.; Loupakis, F.; Aprile, G.; MacCaroni, E.; Andrikou, K.; et al. Angiogenesis genotyping and clinical outcome during regorafenib treatment in metastatic colorectal cancer patients. Sci. Rep. 2016, 6. [Google Scholar] [CrossRef] [Green Version]
- Hansen, T.F.; Sørensen, F.B.; Spindler, K.L.G.; Olsen, D.A.; Andersen, R.F.; Lindebjerg, J.; Brandslund, I.; Jakobsen, A. Microvessel density and the association with single nucleotide polymorphisms of the vascular endothelial growth factor receptor 2 in patients with colorectal cancer. Virchows Arch. 2010, 456, 251–260. [Google Scholar] [CrossRef]
- Lambrechts, D.; Lenz, H.-J.; de Haas, S.; Carmeliet, P.; Scherer, S.J. Markers of Response for the Antiangiogenic Agent Bevacizumab. J. Clin. Oncol. 2013, 31, 1219–1230. [Google Scholar] [CrossRef] [PubMed]
- Lambrechts, D.; Claes, B.; Delmar, P.; Reumers, J.; Mazzone, M.; Yesilyurt, B.T.; Devlieger, R.; Verslype, C.; Tejpar, S.; Wildiers, H.; et al. VEGF pathway genetic variants as biomarkers of treatment outcome with bevacizumab: An analysis of data from the AViTA and AVOREN randomised trials. Lancet Oncol. 2012, 13, 724–733. [Google Scholar] [CrossRef]
- Schultheis, A.M.; Lurje, G.; Rhodes, K.E.; Zhang, W.; Yang, D.; Garcia, A.A.; Morgan, R.; Gandara, D.; Scudder, S.; Oza, A.; et al. Polymorphisms and clinical outcome in recurrent ovarian cancer treated with cyclophosphamide and bevacizumab. Clin. Cancer Res. 2008, 14, 7554–7563. [Google Scholar] [CrossRef] [Green Version]
- Gerger, A.; El-Khoueiry, A.; Zhang, W.; Yang, D.; Singh, H.; Bohanes, P.; Ning, Y.; Winder, T.; LaBonte, M.J.; Wilson, P.M.; et al. Pharmacogenetic angiogenesis profiling for first-line bevacizumab plus oxaliplatin-based chemotherapy in patients with metastatic colorectal cancer. Clin. Cancer Res. 2011, 17, 5783–5792. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meng, R.D.; Shelton, C.C.; Li, Y.M.; Qin, L.X.; Notterman, D.; Paty, P.B.; Schwartz, G.K. γ-secretase inhibitors abrogate oxaliplatin-induced activation of the Notch-1 signaling pathway in colon cancer cells resulting in enhanced chemosensitivity. Cancer Res. 2009, 69, 573–582. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Z.P.; Sun, Y.L.; Fu, L.; Gu, F.; Zhang, L.; Hao, X.S. Correlation of Notch1 expression and activation to cisplatin-sensitivity of head and neck squamous cell carcinoma. Chin. J. Cancer 2009, 28, 100–103. [Google Scholar]
- Aleksic, T.; Feller, S.M. Gamma-secretase inhibition combined with platinum compounds enhances cell death in a large subset of colorectal cancer cells. Cell Commun. Signal. 2008, 6, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yao, J.; Qian, C. Inhibition of Notch3 enhances sensitivity to gemcitabine in pancreatic cancer through an inactivation of PI3K/Akt-dependent pathway. Med. Oncol. 2010, 27, 1017–1022. [Google Scholar] [CrossRef] [PubMed]
- Heublein, S.; Albertsmeier, M.; Pfeifer, D.; Loehrs, L.; Bazhin, A.V.; Kirchner, T.; Werner, J.; Neumann, J.; Angele, M.K. Association of differential miRNA expression with hepatic vs. peritoneal metastatic spread in colorectal cancer. BMC Cancer 2018, 18. [Google Scholar] [CrossRef] [Green Version]
- Ohzawa, H.; Kumagai, Y.; Yamaguchi, H.; Miyato, H.; Sakuma, Y.; Horie, H.; Hosoya, Y.; Kawarai Lefor, A.; Sata, N.; Kitayama, J. Exosomal microRNA in peritoneal fluid as a biomarker of peritoneal metastases from gastric cancer. Ann. Gastroenterol. Surg. 2020, 4, 84–93. [Google Scholar] [CrossRef]
- Vo, D.T.; Karanam, N.K.; Ding, L.; Saha, D.; Yordy, J.S.; Giri, U.; Heymach, J.V.; Story, M.D. miR-125a-5p Functions as Tumor Suppressor microRNA And Is a Marker of Locoregional Recurrence And Poor prognosis in Head And Neck Cancer. Neoplasia 2019, 21, 849–862. [Google Scholar] [CrossRef] [PubMed]
- Gao, J.; Li, N.; Dong, Y.; Li, S.; Xu, L.; Li, X.; Li, Y.; Li, Z.; Ng, S.S.; Sung, J.J.; et al. MiR-34a-5p suppresses colorectal cancer metastasis and predicts recurrence in patients with stage II/III colorectal cancer. Oncogene 2015, 34, 4142–4152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hongliang, C.; Shaojun, H.; Aihua, L.; Hua, J. Correlation between expression of miR-155 in colon cancer and serum carcinoembryonic antigen level and its contribution to recurrence and metastasis forecast. Saudi Med. J. 2014, 35, 547–553. [Google Scholar]
- Jacob, H.; Stanisavljevic, L.; Storli, K.E.; Hestetun, K.E.; Dahl, O.; Myklebust, M.P. Identification of a sixteen-microRNA signature as prognostic biomarker for stage II and III colon cancer. Oncotarget 2017, 8, 87837–87847. [Google Scholar] [CrossRef] [Green Version]
- Eslamizadeh, S.; Heidari, M.; Agah, S.; Faghihloo, E.; Ghazi, H.; Mirzaei, A.; Akbari, A. The role of MicroRNA signature as diagnostic biomarkers in different clinical stages of colorectal cancer. Cell J. 2018, 20, 220–230. [Google Scholar] [CrossRef]
- Fukuoka, S.; Hara, H.; Takahashi, N.; Kojima, T.; Kawazoe, A.; Asayama, M.; Yoshii, T.; Kotani, D.; Tamura, H.; Mikamoto, Y.; et al. Regorafenib Plus Nivolumab in Patients With Advanced Gastric or Colorectal Cancer: An Open-Label, Dose-Escalation, and Dose-Expansion Phase Ib Trial (REGONIVO, EPOC1603). J. Clin. Oncol. 2020, 38. [Google Scholar] [CrossRef]
- Conde, E.; Alegre, L.; Blanco-Sánchez, I.; Sáenz-Morales, D.; Aguado-Fraile, E.; Ponte, B.; Ramos, E.; Sáiz, A.; Jiménez, C.; Ordoñez, A.; et al. Hypoxia Inducible Factor 1-Alpha (HIF-1 Alpha) Is Induced during Reperfusion after Renal Ischemia and Is Critical for Proximal Tubule Cell Survival. PLoS ONE 2012, 7, e33258. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N | % | Mean | Median | SD | Min. | Max. | ||
|---|---|---|---|---|---|---|---|---|
| Age | 47 | 79.8 | 80.8 | 6.1 | 63.2 | 89.2 | ||
| Weight | 47 | 72.2 | 71.5 | 12.8 | 43 | 105.9 | ||
| Size | 47 | 159.6 | 159 | 8.3 | 142 | 180 | ||
| Gender | Male | 26 | 55.3 | |||||
| Female | 21 | 44.7 | ||||||
| ECOG PS | 0 | 5 | 10.6 | |||||
| 1 | 25 | 53.2 | ||||||
| 2 | 17 | 36.2 |
| N | % | ||
|---|---|---|---|
| Primary tumor location | Rectum | 14 | 29.8 |
| Colon | 32 | 68.1 | |
| Colon and rectum | 1 | 2.1 | |
| Grade | Unknown | 10 | 21.3 |
| G1 | 19 | 40.4 | |
| G2 | 12 | 25.5 | |
| G3 | 3 | 6.4 | |
| G4 | 3 | 6.4 | |
| Initial T status | T1 | 1 | 2.1 |
| T2 | 5 | 10.6 | |
| T3 | 23 | 48.9 | |
| T4a | 9 | 19.1 | |
| T4b | 1 | 2.1 | |
| TX | 7 | 14.9 | |
| ND | 1 | 2.1 | |
| Initial N | N0 | 13 | 27.7 |
| N1 | 7 | 14.9 | |
| N1b | 2 | 4.3 | |
| N1c | 1 | 2.1 | |
| N2 | 9 | 19.1 | |
| N2a | 3 | 6.4 | |
| NX | 12 | 25.5 | |
| Initial M | M0 | 17 | 36.2 |
| M1 | 26 | 55.3 | |
| M1a | 1 | 2.1 | |
| M1b | 3 | 6.4 | |
| Locoregional recurrence | No | 29 | 61.7 |
| Yes | 18 | 38.3 | |
| Metastasis location | Liver | 31 | 66 |
| Lung | 29 | 61.7 | |
| Peritoneum | 11 | 23.4 |
| N | % | |
|---|---|---|
| Overall response rate | 6.4 | |
| Complete response | 1 | 2.1 |
| Partial response | 2 | 4.3 |
| Stable disease | 21 | 45.0 |
| Progression disease | 13 | 28.0 |
| Disease control rate | 24 | 51.0 |
| Non-evaluable | 10 | 21.0 |
| Median (months) | 95% CI | |
| Progression-free survival | 5.6 | 2.7–8.4 |
| Overall survival | 16 | 7.8–24 |
| Time to treatment failure | 2.1 | 1.3–2.9 |
| Time to progression | 5.6 | 1.9–9.3 |
| N | % | ||
|---|---|---|---|
| Toxicity | No | 18 | 43.9 |
| Yes | 23 | 56.1 | |
| Asthenia | No | 30 | 73.2 |
| Yes | 11 | 26.8 | |
| Hypertension | No | 28 | 68.3 |
| Yes | 13 | 31.7 | |
| Diarrhea | No | 37 | 90.2 |
| Yes | 4 | 9.8 |
| Clinical Outcome | Sample Source | Biomarker |
|---|---|---|
| Favorable response | Serum | ↑ miR-185-5p |
| Treatment response | Serum | ↑ miR-126-3p; ↑ miR-126-5p; ↑ miR-139-5p; ↑ miR-185-5p; ↑ miR-152-3p; ↓ miR-551a; ↓ miR-582-5p |
| Treatment response | Buffy coat pellets | WT allele of rs7993418 and rs9582036 |
| Treatment response | Paraffin-embedded tumor biopsies (IHC) | ↓ Notch 1 expression |
| Overall survival | Serum | ↑ miR-139-5p; ↓ miR-140-3p correlated with longer OS |
| Progression-free survival | Buffy coat pellets | Variant rs699947 correlated with a longer PFS; variants rs9582306 and rs7993418 correlated with a shorter PFS |
| Progression-free survival | Paraffin-embedded tumor biopsies (IHC) | ↓ Notch 1 expression correlated with a longer PFS |
| Toxicity | Serum | ↑ miR-126-3p; ↑ miR-152-3p |
| Toxicity | Paraffin-embedded tumor biopsies (qPCR) | ↑ miR-92a-1-5p |
| Asthenia | Serum | ↑ miR-362-3p |
| Metastatic disease | Paraffin-embedded tumor biopsies (qPCR) | ↓ miR-92a-5p; ↓ miR-642b-3p; ↓ miR-326; ↓ miR-320a; ↓ miR-193b-5p |
| Metastatic disease | Buffy coat pellets | Variant rs2230054 more frequent in metastatic disease |
| Locoregional recurrence | Paraffin-embedded tumor biopsies (qPCR) | ↓ miR-92a-5p; ↓ miR-19a-3p; ↓ miR-642b-3p; ↓ miR-193b-5p |
| Locoregional recurrence | Buffy coat pellets | Variant rs699947 correlated with LRR |
| Peritoneal metastasis | Paraffin-embedded tumor biopsies (qPCR) | ↓ miR-19a-3p; ↓ miR-19a-5p; ↓ miR-20a-5p; ↓ miR-23b-3p |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Conde, E.; Earl, J.; Crespo-Toro, L.; Blanco-Agudo, C.; Ramos-Muñoz, E.; Rodríguez-Serrano, E.M.; Martínez Ávila, J.C.; Salinas-Muñoz, L.; Serrano-Huertas, S.; Ferreiro, R.; et al. Biomarkers Associated with Regorafenib First-Line Treatment Benefits in Metastatic Colorectal Cancer Patients: REFRAME Molecular Study. Cancers 2021, 13, 1710. https://doi.org/10.3390/cancers13071710
Conde E, Earl J, Crespo-Toro L, Blanco-Agudo C, Ramos-Muñoz E, Rodríguez-Serrano EM, Martínez Ávila JC, Salinas-Muñoz L, Serrano-Huertas S, Ferreiro R, et al. Biomarkers Associated with Regorafenib First-Line Treatment Benefits in Metastatic Colorectal Cancer Patients: REFRAME Molecular Study. Cancers. 2021; 13(7):1710. https://doi.org/10.3390/cancers13071710
Chicago/Turabian StyleConde, Elisa, Julie Earl, Lorena Crespo-Toro, Carolina Blanco-Agudo, Edurne Ramos-Muñoz, E. Macarena Rodríguez-Serrano, Jose Carlos Martínez Ávila, Laura Salinas-Muñoz, Silvia Serrano-Huertas, Reyes Ferreiro, and et al. 2021. "Biomarkers Associated with Regorafenib First-Line Treatment Benefits in Metastatic Colorectal Cancer Patients: REFRAME Molecular Study" Cancers 13, no. 7: 1710. https://doi.org/10.3390/cancers13071710
APA StyleConde, E., Earl, J., Crespo-Toro, L., Blanco-Agudo, C., Ramos-Muñoz, E., Rodríguez-Serrano, E. M., Martínez Ávila, J. C., Salinas-Muñoz, L., Serrano-Huertas, S., Ferreiro, R., Rodriguez-Garrote, M., Sainz, B., Jr., Massuti, B., Alfonso, P. G., Benavides, M., Aranda, E., García-Bermejo, M. L., & Carrato, A. (2021). Biomarkers Associated with Regorafenib First-Line Treatment Benefits in Metastatic Colorectal Cancer Patients: REFRAME Molecular Study. Cancers, 13(7), 1710. https://doi.org/10.3390/cancers13071710