
High-Grade Gliomas in Children—A Multi-Institutional Polish Study

 ,
,  , , , , ,
, , , , ,
Abstract
:Simple Summary
Abstract

1. Introduction
2. Materials and Methods
3. Results
3.1. Patients Characteristics
3.2. Primary Treatment
3.3. Recurrence of the Disease
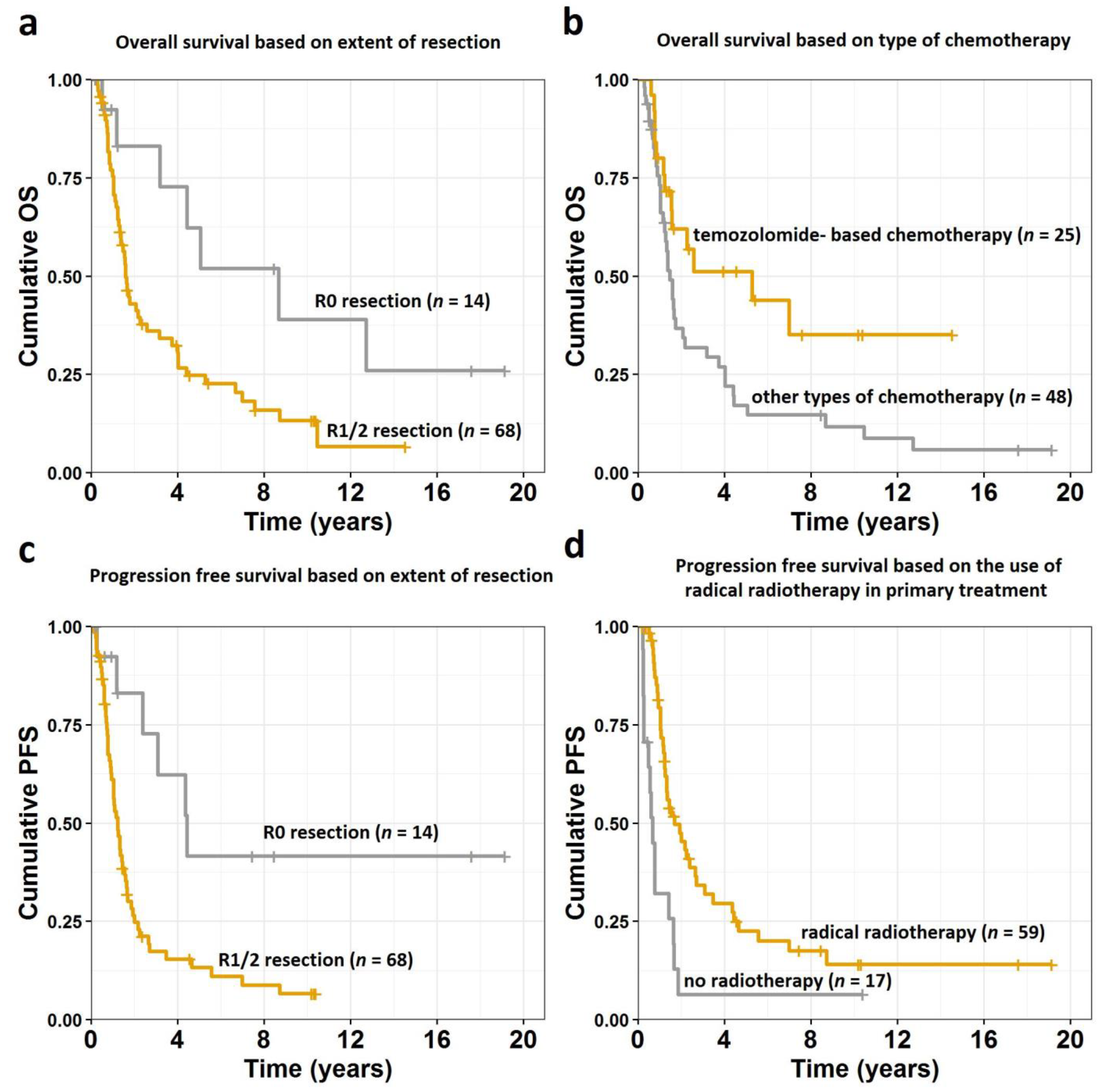
3.4. Survival Analysis
4. Discussion
4.1. Study Limitations
4.2. Clinical Presentation
4.3. Histopathological Diagnosis
4.4. Treatment—Surgery
4.5. Treatment—Chemotherapy
4.6. Treatment—Radiotherapy
4.7. Secondary Neoplasms
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yang, T.; Temkin, N.; Barber, J.; Geyer, J.R.; Leary, S.; Browd, S.; Ojemann, J.G.; Ellenbogen, R.G. Gross Total Resection Correlates with Long-Term Survival in Pediatric Patients with Glioblastoma. World Neurosurg. 2013, 79, 537–544. [Google Scholar] [CrossRef] [PubMed]
- Ostrom, Q.T.; Cioffi, G.; Gittleman, H.; Patil, N.; Waite, K.; Kruchko, C.; Barnholtz-Sloan, J.S. CBTRUS Statistical Report: Primary Brain and Other Central Nervous System Tumors Diagnosed in the United States in 2012–2016. Neuro Oncology. 2019, 21, v1–v100. [Google Scholar] [CrossRef] [PubMed]
- de Blank, P.M.; Ostrom, Q.T.; Rouse, C.; Wolinsky, Y.; Kruchko, C.; Salcido, J.; Barnholtz-Sloan, J.S. Years of life lived with disease and years of potential life lost in children who die of cancer in the United States, 2009. Cancer Med. 2015, 4, 608–619. [Google Scholar] [CrossRef]
- Vanan, M.I.; Eisenstat, D.D. Management of high-grade gliomas in the pediatric patient: Past, present, and future. Neuro Oncol. Pr. 2014, 1, 145–157. [Google Scholar] [CrossRef] [PubMed]
- Funakoshi, Y.; Hata, N.; Kuga, D.; Hatae, R.; Sangatsuda, Y.; Fujioka, Y.; Takigawa, K.; Mizoguchi, M. Pediatric Glioma: An Update of Diagnosis, Biology and Treatment. Cancers 2021, 13, 758. [Google Scholar] [CrossRef] [PubMed]
- Sposto, R.; Ertel, I.J.; Jenkin, R.D.; Boesel, C.P.; Venes, J.L.; Ortega, J.A.; Evans, A.E.; Waral, W.; Hammond, D. The effectiveness of chemotherapy for treatment of high grade astrocytoma in children: Results of a randomized trial—A report from the Childrens Cancer Study Group. J. Neuro Oncol. 1989, 7, 165–177. [Google Scholar] [CrossRef] [Green Version]
- Mallick, S.; Gandhi, A.K.; Joshi, N.P.; Kumar, A.; Puri, T.; Sharma, D.N.; Haresh, K.P.; Gupta, S.; Julka, P.K.; Rath, G.K.; et al. Outcomes of pediatric glioblastoma treated with adjuvant chemoradiation with temozolomide and correlation with prognostic factors. Indian J. Med. Paediatr. Oncol. 2015, 36, 99–104. [Google Scholar] [CrossRef] [Green Version]
- Azizi, A.A.; Paur, S.; Kaider, A.; Dieckmann, K.; Peyrl, A.; Chocholous, M.; Czech, T.; Slavc, I. Does the interval from tumour surgery to radiotherapy influence survival in paediatric high grade glioma? Strahlenther. Onkol. 2018, 194, 552–559. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, S.; Mallick, S.; Benson, R.; Haresh, K.P.; Julka, P.K.; Rath, G.K. Extent of surgical resection and adjuvant temozolomide improves survival in pediatric GBM: A single center experience. Childs Nerv. Syst. 2017, 33, 951–956. [Google Scholar] [CrossRef]
- Yazici, G.; Zorlu, F.; Cengiz, M.; Ozyigit, G.; Eren, G.; Yüce, D.; Varan, A.; Akyuz, C.; Akalan, N.; Gurkaynak, M. High-grade glioma in children and adolescents: A single-center experience. Childs Nerv. Syst. 2016, 32, 291–297. [Google Scholar] [CrossRef]
- Walston, S.; Hamstra, D.A.; Oh, K.; Woods, G.; Guiou, M.; Olshefski, R.S.; Chakravarti, A.; Williams, T.A. A Multi-Institutional Experience in Pediatric High-Grade Glioma. Front. Oncol. 2015, 5, 28. [Google Scholar] [CrossRef]
- Jalali, R.; Rishi, A.; Goda, J.S.; Sridhar, E.; Gurav, M.; Sharma, P.; Moiyadi, A.; Shetty, P.; Gupta, T. Clinical outcome and molecular characterization of pediatric glioblastoma treated with postoperative radiotherapy with concurrent and adjuvant temozolomide: A single institutional study of 66 children. Neuro Oncol. Pr. 2016, 3, 39–47. [Google Scholar] [CrossRef]
- Perkins, S.M.; Rubin, J.B.; Leonard, J.R.; Smyth, M.D.; El Naqa, I.; Michalski, J.M.; Simpson, J.R.; Limbrick, D.L.; Park, T.S.; Mansur, D.B. Glioblastoma in Children: A Single-Institution Experience. Int. J. Radiat. Oncol. Biol. Phys. 2011, 80, 1117–1121. [Google Scholar] [CrossRef]
- Bilginer, B.; Hanalioglu, S.; Turk, C.C.; Narin, F.; Oguz, K.K.; Soylemezoglu, F.; Akalan, N. Is the knowledge pertaining to adult glioblastomas enough for pediatric cases? Prognostic factors in childhood. Turk. Neurosurg. 2017, 27, 279–288. [Google Scholar] [CrossRef] [Green Version]
- Wolff, J.E.; Molenkamp, G.; Westphal, S.; Pietsch, T.; Gnekow, A.; Kortmann, R.D.; Kuehl, J. Oral trosfosfamide and etoposide in pediatric patients with glioblastoma multiforme. Cancer 2000, 89, 2131–2137. [Google Scholar] [CrossRef]
- Wolff, J.E.; Wagner, S.; Reinert, C.; Gnekow, A.; Kortmann, R.D.; Kühl, J.; Van Gool, S.W. Maintenance treatment with interferon-gamma and low-dose cyclophosphamide for pediatric high-grade gliomas. J. Neuro Oncol. 2006, 79, 315–321. [Google Scholar] [CrossRef]
- Wolff, J.E.; Driever, P.H.; Erdlenbruch, B.; Kortmann, R.D.; Rutkowski, S.; Pietsch, T.; Parker, C.; Metz, M.W.; Gnekow, A.; Kramm, C.M. Intensive chemotherapy improves survival in pediatric high-grade glioma after gross total resection: Results of the HIT-GBM-C protocol. Cancer 2010, 116, 705–712. [Google Scholar] [CrossRef]
- Wolff, J.E.; Kortmann, R.D.; Wolff, B.; Pietsch, T.; Peters, O.; Schmid, H.-J.; Rutkowski, S.; Warmuth-Metz, M.; Kramm, C. High dose methotrexate for pediatric high grade glioma: Results of the HIT-GBM-D pilot study. J. Neuro Oncol. 2011, 102, 433–442. [Google Scholar] [CrossRef] [PubMed]
- Wolff, J.E.; Gnekow, A.K.; Kortmann, R.D.; Pietsch, T.; Urban, C.; Graf, N.; Kühl, J. Preradiation chemotherapy for pediatric patients with high-grade glioma. Cancer 2002, 94, 264–271. [Google Scholar] [CrossRef] [PubMed]
- Chastagner, P.; Kalifa, C.; Doz, F.; Bouffet, E.; Gentet, J.C.; Ruchoux, M.M.; Bracard, S.; Desandes, E.; Frappaz, D. Outcome of children treated with preradiation chemotherapy for a high-grade glioma: Results of a French Society of Pediatric Oncology (SFOP) pilot study. Pediatr. Blood Cancer 2007, 49, 803–880. [Google Scholar] [CrossRef] [PubMed]
- McDonald, T.J.; Arenson, E.B.; Ater, J.; Sposto, R.; Bevan, H.H.; Bruner, J.; Deutsch, M.; Kurczynski, E.; Luerssen, T.; McGuire-Cullen, P.; et al. Phase II study of high dose chemotherapy before radiation in children with newly diagnosed high-grade astrocytomas: Final analysis of Children’s Cancer Group Study 9933. Cancer 2005, 104, 2862–2871. [Google Scholar] [CrossRef]
- Finlay, J.L.; Boyett, J.M.; Yates, A.J.; Wisoff, J.H.; Milstein, J.M.; Geyer, J.R.; Bertolone, S.J.; McGuire, P.; Cherlow, J.M.; Tefft, M. Randomized phase III trial in childhood high-grade astrocytoma comparing vincristine, lomustine, and prednisone with the eight-drugs-in-1-day regimen. Childrens Cancer Group. J. Clin. Oncol. 1995, 13, 112–123. [Google Scholar] [CrossRef]
- López-Aguilar, E.; Sepúlveda-Vildósola, A.C.; Rivera-Márquez, H.; Cerecedo-Díaz, F.; Valdés-Sánchez, M.; Delgado-Huerta, S.; Wanzke-del Angel, V.; Ramón-García, G.; Rodríguez-Jiménez, H.; Hernández-Contreras, I.; et al. Preirradiation ifosfamide, carboplatin and etoposide (ICE) for the treatment of high-grade astrocytomas in children. Childs Nerv. Syst. 2003, 19, 818–823. [Google Scholar] [CrossRef]
- Espinoza, J.C.; Haley, K.; Patel, N.; Dhall, G.; Gardner, S.; Allen, J.; Torkildson, J.; Cornelius, A.; Rassekh, R.; Bedros, A.; et al. Outcome of young children with high-grade glioma treated with irradiation-avoiding intensive chemotherapy regimens: Final report of the Head Start II and III trials. Pediatr. Blood Cancer 2016, 63, 1806–1813. [Google Scholar] [CrossRef] [Green Version]
- Das, K.K.; Mehrotra, A.; Nair, A.P.; Kumar, S.; Srivastava, A.K.; Sahu, R.N.; Kumar, R. Pediatric glioblastoma: Clinico-radiological profile and factors affecting the outcome. Childs Nerv. Syst. 2012, 28, 2055–2062. [Google Scholar] [CrossRef]
- Boudaouara, O.; Charfi, S.; Bahri, M.; Daoud, J.; Boudawara, M.Z.; Gouiaa, N.; Boudawara, S.T. Pediatric high grade gliomas: Clinico-pathological profile, therapeutic approaches and factors affecting overall survival. Neurochirurgie 2019, 65, 63–68. [Google Scholar] [CrossRef] [PubMed]
- Jung, T.-Y.; Lee, J.Y.; Kim, D.-S.; Park, H.J.; Kim, C.-Y.; Ra, Y.-S.; Lee, M.-J.; Kim, S.-H.; Baek, H.-J.; Kim, I.H.; et al. Pediatric supratentorial high-grade glioma: Multicenter retrospective observational study of the Korean Society for Pediatric Neuro-Oncology. J. Neuro Oncol. 2015, 121, 413–419. [Google Scholar] [CrossRef] [PubMed]
- Lucas, J.T.; Cooper, D.A.; Hwang, S.; Tinkle, C.; Li, X.; Li, Y.; Orr, B.; Merchant, T.E.; Broniscer, A. Prognostic Relevance of Treatment Failure Patterns in Pediatric High-Grade Glioma: Is There a Role for a Revised Failure Classification System? Int. J. Radiat. Oncol. Biol. Phys. 2017, 99, 450–458. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.W.; Lim, D.H.; Sung, K.W.; Lee, H.J.; Yi, E.S.; Yoo, K.H.; Koo, H.H.; Suh, Y.L.; Shin, H.J. Tandem High-Dose Chemotherapy and Autologous Stem Cell Transplantation for High-Grade Gliomas in Children and Adolescents. J. Korean Med. Sci. 2017, 32, 195–203. [Google Scholar] [CrossRef] [Green Version]
- Cohen, K.J.; Pollack, I.F.; Zhou, T.; Buxton, A.; Holmes, E.J.; Burger, P.C.; Brat, D.J.; Rosenblum, M.K.; Hamilton, R.L.; Lavey, R.S.; et al. Temozolomide in the treatment of high-grade gliomas in children: A report from the Children’s Oncology Group. Neuro Oncol. 2011, 13, 317–323. [Google Scholar] [CrossRef]
- Cabanas, R.; Saurez, G.; Rios, M.; Alert, J.; Reyes, A.; Valdes, J.; Gonzalez, M.C.; Pedrayes, J.L.; Avila, M.; Herrera, R.; et al. Treatment of children with high grade glioma with nimotuzumab: A 5-year institutional experience. MAB 2013, 5, 202–207. [Google Scholar] [CrossRef] [Green Version]
- Mathew, R.K.; O’Kane, R.; Parslow, R.; Stiller, C.; Kenny, T.; Picton, S.; Chumas, P.D. Comparison of survival between the UK and US after surgery for most common pediatric CNS tumors. Neuro Oncol. 2014, 16, 1137–1145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lam, S.; Lin, Y.; Zinn, P.; Su, J.; Pan, I.-W. Patient and treatment factors associated with survival among pediatric glioblastoma patients: A Surveillance, Epidemiology, and End Results study. J. Clin. Neurosci. 2018, 47, 285–293. [Google Scholar] [CrossRef]
- Adams, H.; Adams, H.H.H.; Jackson, C.; Rincon-Torroella, J.; Jallo, G.I.; Quiñones-Hinojosa, A. Evaluating extent of resection in pediatric glioblastoma: A multiple propensity score-adjusted population-based analysis. Childs Nerv. Syst. 2016, 32, 493–503. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Thakkar, J.P.; Garcia, C.R.; Dolecek, T.A.; Wagner, L.M.; Dressler, E.V.M.; Villano, J.L. National cancer database analysis of outcomes in pediatric glioblastoma. Cancer Med. 2018, 7, 1151–1159. [Google Scholar] [CrossRef] [PubMed]
- Reulecke, B.C.; Erker, C.G.; Fiedler, B.J.; Niederstadt, T.-U.; Kurlemann, G. Brain Tumors in Children: Initial Symptoms and Their Influence on the Time Span Between Symptom Onset and Diagnosis. J. Child Neurol. 2008, 23, 178–183. [Google Scholar] [CrossRef] [PubMed]
- Mehta, V.; Chapman, A.; McNeely, P.D.; Walling, S.; Howes, W.J. Latency between Symptom Onset and Diagnosis of Pediatric Brain Tumors: An Eastern Canadian Geographic Study. Neurosurgery 2002, 51, 365–372. [Google Scholar] [CrossRef]
- Louis, D.N.; Ohgaki, H.; Wiestler, O.D.; Cavenee, W.K.; Burger, P.C.; Jouvet, A.; Scheithauer, B.W.; Kleihues, P. The 2007 WHO Classification of Tumours of the Central Nervous System. Acta Neuropathol. 2007, 114, 97–109. [Google Scholar] [CrossRef] [Green Version]
- Braunstein, S.; Raleigh, D.; Bindra, R.; Mueller, S.; Daphne Haas-Kogan, D. High-grade glioma: Current molecular landscape and therapeutic approaches. J. Neuro Oncol. 2017, 134, 541–549. [Google Scholar] [CrossRef]
- Pettorini, B.L.; Park, Y.-S.; Caldarelli, M.; Massimi, L.; Tamburrini, G.; Di Rocco, C. Radiation-induced brain tumours after central nervous system irradiation in childhood: A review. Childs Nerv. Syst. 2008, 24, 793–805. [Google Scholar] [CrossRef]
- Carret, A.-S.; Tabori, U.; Crooks, B.; Hukin, J.; Odame, I.; Johnston, D.L.; Keene, D.L.; Freeman, C.; Bouffet, E. Outcome of secondary high-grade glioma in children previously treated for a malignant condition: A study of the Canadian Pediatric Brain Tumour Consortium. Radiother. Oncol. 2006, 81, 33–38. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Characteristic | Value | |
|---|---|---|
| Age at diagnosis | Mean (range) | 12 (1–18) |
| Number of patients (%) | ||
| Sex | Female | 35 (42.7) |
| Male | 47 (57.3) | |
| Pathological subtype | Glioblastoma multiforme G IV | 51 (62.2) |
| Anaplastic astrocytoma G III | 19 (23.2) | |
| Anaplastic oligodendroglioma G III | 12 (14.6) | |
| ECOG performance status | 0 | 19 (23.2) |
| 1 | 48 (58.5) | |
| 2 | 11 (13.4) | |
| 3 | 3 (3.7) | |
| 4 | 1 (1.2) | |
| Primary site | Supratentorial | 68 (82.9) |
| Infratentorial | 12 (14.6) | |
| No data | 2 (2.5) | |
| Symptoms | Seizures | 17 (20.7) |
| Paresis | 18 (21.9) | |
| Headaches | 39 (47.7) | |
| Vomiting/nausea | 34 (41.5) | |
| Visual deficits | 9 (11.0) | |
| Balance disorders | 10 (12.2) | |
| Disturbances of consciousness | 16 (19.5) | |
| Speech problems Hearing deficits | 5 (6.1) 4 (4.9) | |
| Weakness | 17 (20.7) | |
| Other * | 29 (35.4) | |
| Underwent surgery | Yes | 82 (100) |
| R0 | 14 (17.1) | |
| R1 | 16 (19.5) | |
| R2/biopsy | 52 (63.4) | |
| Underwent radiotherapy in primary treatment | Yes | 65 (79.3) |
| Radical | 59 | |
| Palliative | 6 | |
| No | 17 (20.7) | |
| Underwent chemotherapy in primary treatment | Yes | 76 (92.7) |
| No | 6 (7.3) |
| Variable | HR | 95% CI | p-Value | |
|---|---|---|---|---|
| Age (years) | 1 | 0.96–1.05 | 0.906 | |
| Sex | male | ref. | ||
| female | 0.95 | 0.57–1.60 | 0.855 | |
| Tumor grade | G III | ref. | ||
| G IV | 2.32 | 1.31–4.11 | 0.004 | |
| ECOG performance status | 0 | ref. | ||
| 1 | 1.36 | 0.73–2.56 | 0.332 | |
| 2 or more | 1.76 | 0.83–3.73 | 0.138 | |
| Tumor location | infratentorial | ref. | ||
| supratentorial | 0.87 | 0.44–1.72 | 0.679 | |
| Extent of resection | R1/2 | ref. | ||
| R0 | 0.41 | 0.18–0.92 | 0.030 | |
| Radiotherapy | no radiotherapy | ref. | ||
| radical radiotherapy | 0.52 | 0.29–0.96 | 0.036 | |
| palliative radiotherapy | 1.12 | 0.41–3.11 | 0.821 | |
| Total dose over 54 Gy | no | ref. | ||
| yes | 0.92 | 0.50–1.70 | 0.790 | |
| Chemotherapy | other than temozolomide | ref. | ||
| temozolomide-based | 0.49 | 0.26–0.91 | 0.023 | |
| no chemotherapy | 0.46 | 0.16–1.30 | 0.144 |
| Variable | HR | 95% CI | p-Value | |
|---|---|---|---|---|
| Age (years) | 0.99 | 0.95–1.04 | 0.706 | |
| Sex | male | ref. | ||
| female | 1.06 | 0.64–1.75 | 0.822 | |
| Tumor grade | G III | ref. | ||
| G IV | 1.80 | 1.05–3.12 | 0.032 | |
| ECOG performance status | 0 | ref. | ||
| 1 | 1.72 | 0.92–3.23 | 0.091 | |
| 2 or more | 2.24 | 1.05–4.79 | 0.037 | |
| Tumor location | infratentorial | ref. | ||
| supratentorial | 1.11 | 0.55–2.26 | 0.773 | |
| Extent of resection | R1/2 | ref. | ||
| R0 | 0.31 | 0.13–0.72 | 0.006 | |
| Radiotherapy | no radiotherapy | ref. | ||
| radical radiotherapy | 0.36 | 0.20–0.66 | <0.001 | |
| palliative radiotherapy | 1.75 | 0.67– 4.57 | 0.253 | |
| Total dose over 54 Gy | no | ref. | ||
| yes | 0.84 | 0.46–1.52 | 0.558 | |
| Chemotherapy | other than temozolomide | ref. | ||
| temozolomide-based | 0.72 | 0.41–1.26 | 0.247 | |
| no chemotherapy | 0.51 | 0.18–1.45 | 0.210 |
| Author (Year of Publication) [Reference Number] | Number of Patients | Treatment Schema | OS | Prognostic Factors for OS |
|---|---|---|---|---|
| Sposto R. et al. (1989) [6] | 58 pts 18 G III 40 G IV | S + RT + CTH or RT alone | 1,2,5-y OS G III 65%, 60%, 60% 1,2,5-y OS G IV 65%, 35%, 15% | AA histology, lack of necrosis, location outside basal ganglia, EOR, CTH |
| Finlay J.L. et al. (1995) [22] | 172 pts 82 G III 57 G IV 33 other | S + RT + CTH or CTH-RT-CTH | 1,2,5-y OS 80%, 50%, 40% | White race, older age, EOR, AA histology, female sex |
| Wolf J.E. et al. (2002) [19] | 52 pts 25 G III 27 G IV | S + RT + CTH or CTH + RT + CTH (sandwich) | 1,2,5-y OS G III 100%, 100%, 100% 1,2,5-y OS G IV 100%, 45%, 40% | EOR, male sex, AA histology, residual tumor > 2 cm, RT ≥ 54 Gy, sandwich CTH |
| López-Aguilar E. et al. (2003) [23] | 25 pts 20 G III 5 G IV | S + CTH + hyperRT + CTH | 1,2,5-y OS 67%, 67%, 67% | AA histology, supratentorial location |
| Wolf J.E. et al. (2010) [17] | 97 pts 30 G III 41 G IV 26 no data | S + RT + CTH | 1,2,5-y OS 56%, 30%, 19% | EOR |
| Perkins M. et al. (2011) [13] | 24 pts G IV | S + RT +/− CTH | 1-2-5-y OS 57%, 32%, 10% | EOR |
| Cohen K.J. et al. (2011) [30] | 90 pts 31 G III 55 G IV 4 other | S + RCTH +CTH | 1,2,5-y OS 70%, 35%, 15% | EOR |
| Das K.K. et al. (2012) [25] | 65 pts G IV | S + RT + CTH | 1,2,5-y OS 55%, 30%, 15% | EOR |
| Yang T et al. (2013) [1] | 37 pts G IV | S + RT + CTH | 1,2,5-y OS 64%, 45%, 18% | EOR |
| Cabanas R. et al. (2013) [31] | 23 pts 19 G III 4 G IV | S + RT + CTH + nimotuzumab | 1,2,5-y OS 64%, 54%, not reported | Not reported |
| Walston S. et al. (2015) [11] | 51 pts, 23 G III 28 G IV | S +/- RT/RCTH +/− CTH | 1,2,5-y OS 87%, 59%, 37% 1,2,5-y OS GIII 90%, 75%, 50% 1,2,5-y OS GIV 90%, 30%, 20% | EOR, CTH after RT/RCTH |
| Jung T.-J. et al. (2015) [27] | 62 pts 28 G III 34 G IV | S + RCTH or RT+CTH or RT | 1,2,5-y OS 76%, 35%, not reported | EOR, cerebrospinal fluid dissemination |
| Mallick S. et al. (2015) [7] | 23 pts G IV | S + RCTH +CTH | 1,2,5-y OS 70%, 61%, 40% | CTH-TMX |
| Yazici G. et al. (2016) [10] | 63 pts, 26 G III 37 G IV | S + RT +/− CTH | 1,2,5-y OS G III 79%, 63%, 35% 1,2,5-y OS G IV 48%, 30%, 22% | AA histology, better PS, EOR, CTH-TMX |
| Espinoza J.C. et al. (2016) [24] | 32 pts 19 G III 11 G IV 2 other | S + CTH + AuHPCR +/− RT (50%) | 1,2,5-y OS 70%, 50%, 36% | Male sex |
| Jalali R. et al. (2016) [12] | 66 pts G IV | S + RCTH +CTH | 1,2,5-y OS 62%, 30%, 20% | EOR, thalamic location |
| Gupta S. et al. (2017) [9] | 51 pts G IV | S + RCTH +CTH | 1,2,5-y OS 60%, 40%, 20% | EOR, CTH-TMX |
| Bilginer B. et al. (2017) [14] | 42 pts G IV | S + RT + CTH | 1,2,5-y OS 50%, 19%, 10% | EOR, lack of seeding metastases |
| Lucas J.T. et al. (2017) [28] | 56 pts 29 G III 27 G IV | S + RT + erlotynib | 1,2,5-y OS 45%, 25%, 20% | AA histology, lack of brainstem/cerebellar involvement |
| Lee J.W. et al. (2017) [29] | 30 pts 7 G III 16 G IV 7 other | S + RT or CTH +/− HDCT/auto-SCT | 3-y OS 32% | EOR |
| Azizi AA. et al. (2018) [8] | 38 pts 17 G III 21 G IV | S + RCTH +CTH | 1,2,5-y OS 68%, 29%, 21% | EOR, lower grade, CTH-TMX |
| Boudaouara O. et al. (2019) [26] | 30 pts 3 G III 27 G IV | S + RT +/− CTH | Median OS 13 months; 1,2,5-y OS described only in subgroups | Postoperative RT, complete response |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Napieralska, A.; Krzywon, A.; Mizia-Malarz, A.; Sosna-Zielińska, J.; Pawłowska, E.; Krawczyk, M.A.; Konat-Bąska, K.; Kaczorowska, A.; Dąbrowska, A.; Harat, M. High-Grade Gliomas in Children—A Multi-Institutional Polish Study. Cancers 2021, 13, 2062. https://doi.org/10.3390/cancers13092062
Napieralska A, Krzywon A, Mizia-Malarz A, Sosna-Zielińska J, Pawłowska E, Krawczyk MA, Konat-Bąska K, Kaczorowska A, Dąbrowska A, Harat M. High-Grade Gliomas in Children—A Multi-Institutional Polish Study. Cancers. 2021; 13(9):2062. https://doi.org/10.3390/cancers13092062
Chicago/Turabian StyleNapieralska, Aleksandra, Aleksandra Krzywon, Agnieszka Mizia-Malarz, Joanna Sosna-Zielińska, Ewa Pawłowska, Małgorzata A. Krawczyk, Katarzyna Konat-Bąska, Aneta Kaczorowska, Anna Dąbrowska, and Maciej Harat. 2021. "High-Grade Gliomas in Children—A Multi-Institutional Polish Study" Cancers 13, no. 9: 2062. https://doi.org/10.3390/cancers13092062
APA StyleNapieralska, A., Krzywon, A., Mizia-Malarz, A., Sosna-Zielińska, J., Pawłowska, E., Krawczyk, M. A., Konat-Bąska, K., Kaczorowska, A., Dąbrowska, A., & Harat, M. (2021). High-Grade Gliomas in Children—A Multi-Institutional Polish Study. Cancers, 13(9), 2062. https://doi.org/10.3390/cancers13092062