
Lifestyle and Hepatocellular Carcinoma What Is the Evidence and Prevention Recommendations


Abstract
:Simple Summary
Abstract
1. Introduction
2. Role of Diet and Lifestyle in General in the Prevention of Hepatocellular Carcinoma
3. The Role of Obesity in HCC
4. The Role of Dietary Composition beyond BMI
4.1. Types of Dietary Fat, Meat, and Fish
4.2. Added (Free) Sugars
5. Role of Micronutrients, Fruits, and Vegetables in HCC
6. Coffee and Tea
7. Dietary Patterns
8. Role of Physical Activity in HCC
8.1. Physical Activity and General Cancer Risk
8.2. Physical Activity and HCC in Animal and Cellular Models
8.3. Physical Activity and HCC Incidence and Prevention in Humans
8.4. Physical Activity Following HCC Treatment in Humans
9. Role of Alcohol in HCC
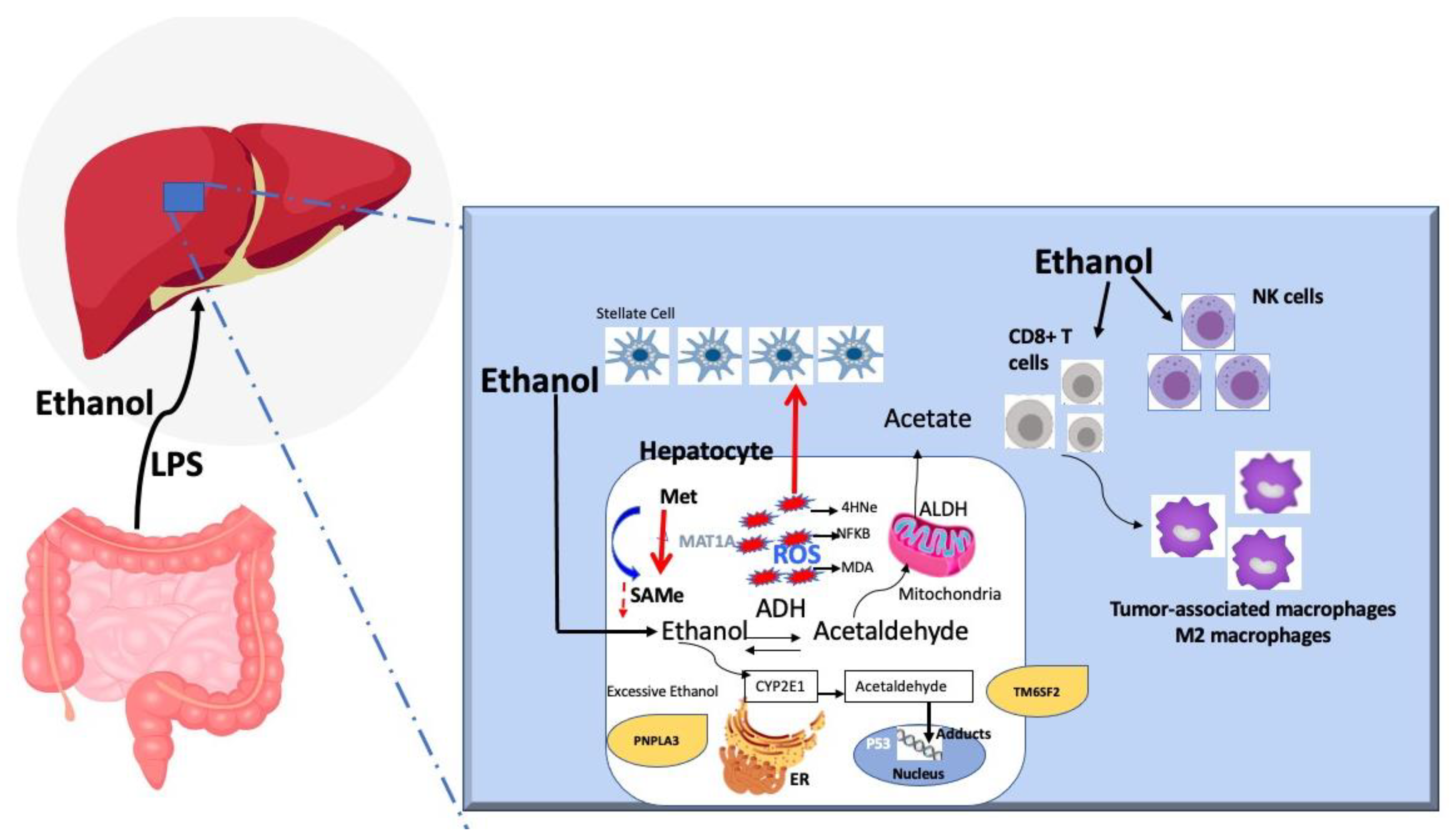
9.1. Alcohol as a Carcinogen
9.2. The Amount of Alcohol as a Risk Factor
9.3. Gender, Obesity, and Type 2 Diabetes as Additional Synergistic Risk Factors with Alcohol
9.4. Viral Hepatitis and Alcohol-Associated HCC
9.5. Change of HCC Risk after Alcohol Cessation
10. Role of Smoking in HCC
11. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
References
- Llovet, J.M.; Kelley, R.K.; Villanueva, A.; Singal, A.G.; Pikarsky, E.; Roayaie, S.; Lencioni, R.; Koike, K.; Zucman-Rossi, J.; Finn, R.S. Hepatocellular carcinoma. Nat. Rev. Dis. Primers 2021, 7, 6. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, A.; Dadduzio, V.; Ricci, A.D.; Massari, F.; Di Federico, A.; Gadaleta-Caldarola, G.; Brandi, G. Lenvatinib plus pembrolizumab: The next frontier for the treatment of hepatocellular carcinoma? Expert Opin. Investig. Drugs 2021, 1–8. [Google Scholar] [CrossRef]
- Luu, H.N.; Behari, J.; Goh, G.B.; Wang, R.; Jin, A.; Thomas, C.E.; Clemente, J.C.; Odegaard, A.O.; Koh, W.P.; Yuan, J.M. Composite Score of Healthy Lifestyle Factors and Risk of Hepatocellular Carcinoma: Findings from a Prospective Cohort Study. Cancer Epidemiol. Biomarkers Prev. 2021, 30, 380–387. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.B.; Pan, X.F.; Chen, J.; Cao, A.; Zhang, Y.G.; Xia, L.; Wang, J.; Li, H.; Liu, G.; Pan, A. Combined lifestyle factors, incident cancer, and cancer mortality: A systematic review and meta-analysis of prospective cohort studies. Br. J. Cancer 2020, 122, 1085–1093. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Yang, W.; VoPham, T.; Ma, Y.; Simon, T.G.; Gao, X.; Chan, A.T.; Meyerhardt, J.A.; Giovannucci, E.L.; Zhang, X. Plant-Based and Animal-Based Low-Carbohydrate Diets and Risk of Hepatocellular Carcinoma Among US Men and Women. Hepatology 2021, 73, 175–185. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.C.; Zhu, X.; Dai, Q.; Peek, R.M.; Shrubsole, M.J. Magnesium intake is associated with a reduced risk of incident liver cancer, based on an analysis of the NIH-American Association of Retired Persons (NIH-AARP) Diet and Health Study prospective cohort. Am. J. Clin. Nutr. 2021, 113, 630–638. [Google Scholar] [CrossRef] [PubMed]
- Luu, H.N.; Neelakantan, N.; Geng, T.T.; Wang, R.; Goh, G.B.; Clemente, J.C.; Jin, A.; van Dam, R.M.; Jia, W.; Behari, J.; et al. Quality diet indexes and risk of hepatocellular carcinoma: Findings from the Singapore Chinese Health Study. Int. J. Cancer 2021, 148, 2102–2114. [Google Scholar] [CrossRef] [PubMed]
- Yang, W.; Sui, J.; Zhao, L.; Ma, Y.; Tabung, F.K.; Simon, T.G.; Lee, D.H.; Zeng, X.; Nguyen, L.H.; Meyerhardt, J.A.; et al. Association of Inflammatory and Insulinemic Potential of Diet and Lifestyle with Risk of Hepatocellular Carcinoma. Cancer Epidemiol. Biomarkers Prev. 2021, 30, 789–796. [Google Scholar] [CrossRef] [PubMed]
- Ji, X.W.; Wang, J.; Shen, Q.M.; Li, Z.Y.; Jiang, Y.F.; Liu, D.K.; Tan, Y.T.; Li, H.L.; Xiang, Y.B. Dietary fat intake and liver cancer incidence: A population-based cohort study in Chinese men. Int. J. Cancer 2021, 148, 2982–2996. [Google Scholar] [CrossRef]
- Luo, Y.; Zhang, Y.J.; Zhang, D.M.; Yishake, D.; Liu, Z.Y.; Chen, M.S.; Wang, F.; Zhou, Z.G.; Long, J.A.; Zhong, R.H.; et al. Association between dietary patterns and prognosis of hepatocellular carcinoma in the Guangdong liver cancer cohort study. Hepatol. Res. 2020, 50, 1164–1175. [Google Scholar] [CrossRef]
- Zhong, G.C.; Wang, K.; Peng, Y.; Shivappa, N.; Hebert, J.R.; Wu, Y.Q.; Gong, J.P. Dietary inflammatory index and incidence of and death from primary liver cancer: A prospective study of 103,902 American adults. Int. J. Cancer 2020, 147, 1050–1058. [Google Scholar] [CrossRef]
- Jayedi, A.; Shab-Bidar, S. Fish Consumption and the Risk of Chronic Disease: An Umbrella Review of Meta-Analyses of Prospective Cohort Studies. Adv. Nutr. 2020, 11, 1123–1133. [Google Scholar] [CrossRef] [PubMed]
- Zhong, G.C.; Peng, Y.; Wang, K.; Wan, L.; Wu, Y.Q.; Hao, F.B.; Hu, J.J.; Gu, H.T. Magnesium intake and primary liver cancer incidence and mortality in the Prostate, Lung, Colorectal and Ovarian Cancer Screening Trial. Int. J. Cancer 2020, 147, 1577–1586. [Google Scholar] [CrossRef] [PubMed]
- Yang, W.; Sui, J.; Ma, Y.; Simon, T.G.; Petrick, J.L.; Lai, M.; McGlynn, K.A.; Campbell, P.T.; Giovannucci, E.L.; Chan, A.T.; et al. High Dietary Intake of Vegetable or Polyunsaturated Fats Is Associated With Reduced Risk of Hepatocellular Carcinoma. Clin. Gastroenterol. Hepatol. 2020, 18, 2775–2783.e2711. [Google Scholar] [CrossRef]
- Yang, W.; Sui, J.; Ma, Y.; Simon, T.G.; Chong, D.; Meyerhardt, J.A.; Willett, W.C.; Giovannucci, E.L.; Chan, A.T.; Zhang, X. A prospective study of dairy product intake and the risk of hepatocellular carcinoma in U.S. men and women. Int. J. Cancer 2020, 146, 1241–1249. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.L.; Jeong, G.H.; Yang, J.W.; Lee, K.H.; Kronbichler, A.; van der Vliet, H.J.; Grosso, G.; Galvano, F.; Aune, D.; Kim, J.Y.; et al. Tea Consumption and Risk of Cancer: An Umbrella Review and Meta-Analysis of Observational Studies. Adv. Nutr. 2020, 11, 1437–1452. [Google Scholar] [CrossRef]
- Guo, X.F.; Shao, X.F.; Li, J.M.; Li, S.; Li, K.L.; Li, D. Fruit and vegetable intake and liver cancer risk: A meta-analysis of prospective cohort studies. Food Funct. 2019, 10, 4478–4485. [Google Scholar] [CrossRef]
- Ma, Y.; Yang, W.; Li, T.; Liu, Y.; Simon, T.G.; Sui, J.; Wu, K.; Giovannucci, E.L.; Chan, A.T.; Zhang, X. Meat intake and risk of hepatocellular carcinoma in two large US prospective cohorts of women and men. Int. J. Epidemiol. 2019, 48, 1863–1871. [Google Scholar] [CrossRef]
- Ma, Y.; Yang, W.; Simon, T.G.; Smith-Warner, S.A.; Fung, T.T.; Sui, J.; Chong, D.; VoPham, T.; Meyerhardt, J.A.; Wen, D.; et al. Dietary Patterns and Risk of Hepatocellular Carcinoma Among, U.S. Men and Women. Hepatology 2019, 70, 577–586. [Google Scholar] [CrossRef]
- Tran, K.T.; Coleman, H.G.; McMenamin, Ú.C.; Cardwell, C.R. Coffee consumption by type and risk of digestive cancer: A large prospective cohort study. Br. J. Cancer 2019, 120, 1059–1066. [Google Scholar] [CrossRef] [Green Version]
- Kennedy, O.J.; Roderick, P.; Buchanan, R.; Fallowfield, J.A.; Hayes, P.C.; Parkes, J. Coffee, including caffeinated and decaffeinated coffee, and the risk of hepatocellular carcinoma: A systematic review and dose-response meta-analysis. BMJ Open 2017, 7, e013739. [Google Scholar] [CrossRef]
- Gao, M.; Sun, K.; Guo, M.; Gao, H.; Liu, K.; Yang, C.; Li, S.; Liu, N. Fish consumption and n-3 polyunsaturated fatty acids, and risk of hepatocellular carcinoma: Systematic review and meta-analysis. Cancer Causes Control 2015, 26, 367–376. [Google Scholar] [CrossRef]
- Yang, Y.; Zhang, D.; Feng, N.; Chen, G.; Liu, J.; Chen, G.; Zhu, Y. Increased intake of vegetables, but not fruit, reduces risk for hepatocellular carcinoma: A meta-analysis. Gastroenterology 2014, 147, 1031–1042. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luo, J.; Yang, Y.; Liu, J.; Lu, K.; Tang, Z.; Liu, P.; Liu, L.; Zhu, Y. Systematic review with meta-analysis: Meat consumption and the risk of hepatocellular carcinoma. Aliment. Pharmacol. Ther. 2014, 39, 913–922. [Google Scholar] [CrossRef] [Green Version]
- Bravi, F.; Bosetti, C.; Tavani, A.; Gallus, S.; La Vecchia, C. Coffee reduces risk for hepatocellular carcinoma: An updated meta-analysis. Clin. Gastroenterol. Hepatol. 2013, 11, 1413–1421.e1. [Google Scholar] [CrossRef]
- Fedirko, V.; Lukanova, A.; Bamia, C.; Trichopolou, A.; Trepo, E.; Nothlings, U.; Schlesinger, S.; Aleksandrova, K.; Boffetta, P.; Tjonneland, A.; et al. Glycemic index, glycemic load, dietary carbohydrate, and dietary fiber intake and risk of liver and biliary tract cancers in Western Europeans. Ann. Oncol. 2013, 24, 543–553. [Google Scholar] [CrossRef] [PubMed]
- Sawada, N.; Inoue, M.; Iwasaki, M.; Sasazuki, S.; Shimazu, T.; Yamaji, T.; Takachi, R.; Tanaka, Y.; Mizokami, M.; Tsugane, S.; et al. Consumption of n-3 fatty acids and fish reduces risk of hepatocellular carcinoma. Gastroenterology 2012, 142, 1468–1475. [Google Scholar] [CrossRef] [PubMed]
- Freedman, N.D.; Cross, A.J.; McGlynn, K.A.; Abnet, C.C.; Park, Y.; Hollenbeck, A.R.; Schatzkin, A.; Everhart, J.E.; Sinha, R. Association of meat and fat intake with liver disease and hepatocellular carcinoma in the NIH-AARP cohort. J. Natl. Cancer Inst. 2010, 102, 1354–1365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ioannou, G.N.; Morrow, O.B.; Connole, M.L.; Lee, S.P. Association between dietary nutrient composition and the incidence of cirrhosis or liver cancer in the United States population. Hepatology 2009, 50, 175–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, C.; Lu, Y.; Xia, H.; Liu, H.; Pan, D.; Yang, X.; Sun, G. Excess Body Weight and the Risk of Liver Cancer: Systematic Review and a Meta-Analysis of Cohort Studies. Nutr. Cancer 2020, 72, 1085–1097. [Google Scholar] [CrossRef]
- Sohn, W.; Lee, H.W.; Lee, S.; Lim, J.H.; Lee, M.W.; Park, C.H.; Yoon, S.K. Obesity and the risk of primary liver cancer: A systematic review and meta-analysis. Clin. Mol. Hepatol. 2021, 27, 157. [Google Scholar] [CrossRef] [PubMed]
- Parra-Soto, S.; Cowley, E.S.; Rezende, L.F.M.; Ferreccio, C.; Mathers, J.C.; Pell, J.P.; Ho, F.K.; Celis-Morales, C. Associations of six adiposity-related markers with incidence and mortality from 24 cancers-findings from the UK Biobank prospective cohort study. BMC Med. 2021, 19, 7. [Google Scholar] [CrossRef] [PubMed]
- Rahmani, J.; Kord Varkaneh, H.; Kontogiannis, V.; Ryan, P.M.; Bawadi, H.; Fatahi, S.; Zhang, Y. Waist Circumference and Risk of Liver Cancer: A Systematic Review and Meta-Analysis of over 2 Million Cohort Study Participants. Liver Cancer 2020, 9, 6–14. [Google Scholar] [CrossRef] [PubMed]
- Zhao, L.; Deng, C.; Lin, Z.; Giovannucci, E.; Zhang, X. Dietary Fats, Serum Cholesterol and Liver Cancer Risk: A Systematic Review and Meta-Analysis of Prospective Studies. Cancers 2021, 13, 1580. [Google Scholar] [CrossRef] [PubMed]
- Baratta, F.; Pastori, D.; Polimeni, L.; Bucci, T.; Ceci, F.; Calabrese, C.; Ernesti, I.; Pannitteri, G.; Violi, F.; Angelico, F.; et al. Adherence to Mediterranean Diet and Non-Alcoholic Fatty Liver Disease: Effect on Insulin Resistance. Am. J. Gastroenterol. 2017, 112, 1832–1839. [Google Scholar] [CrossRef]
- Alferink, L.J.; Kiefte-de Jong, J.C.; Erler, N.S.; Veldt, B.J.; Schoufour, J.D.; de Knegt, R.J.; Ikram, M.A.; Metselaar, H.J.; Janssen, H.; Franco, O.H.; et al. Association of dietary macronutrient composition and non-alcoholic fatty liver disease in an ageing population: The Rotterdam Study. Gut 2019, 68, 1088–1098. [Google Scholar] [CrossRef]
- Zelber-Sagi, S.; Ivancovsky-Wajcman, D.; Fliss Isakov, N.; Webb, M.; Orenstein, D.; Shibolet, O.; Kariv, R. High red and processed meat consumption is associated with non-alcoholic fatty liver disease and insulin resistance. J. Hepatol. 2018, 68, 1239–1246. [Google Scholar] [CrossRef]
- Noureddin, M.; Zelber-Sagi, S.; Wilkens, L.R.; Porcel, J.; Boushey, C.J.; Le Marchand, L.; Rosen, H.R.; Setiawan, V.W. Diet Associations With Nonalcoholic Fatty Liver Disease in an Ethnically Diverse Population: The Multiethnic Cohort. Hepatology 2020, 71, 1940–1952. [Google Scholar] [CrossRef]
- Etemadi, A.; Sinha, R.; Ward, M.H.; Graubard, B.I.; Inoue-Choi, M.; Dawsey, S.M.; Abnet, C.C. Mortality from different causes associated with meat, heme iron, nitrates, and nitrites in the NIH-AARP Diet and Health Study: Population based cohort study. BMJ 2017, 357, j1957. [Google Scholar] [CrossRef] [Green Version]
- Farvid, M.S.; Sidahmed, E.; Spence, N.D.; Mante Angua, K.; Rosner, B.A.; Barnett, J.B. Consumption of red meat and processed meat and cancer incidence: A systematic review and meta-analysis of prospective studies. Eur. J. Epidemiol. 2021, 36, 937–951. [Google Scholar] [CrossRef]
- Li, Y.; Guo, L.; He, K.; Huang, C.; Tang, S. Consumption of sugar-sweetened beverages and fruit juice and human cancer: A systematic review and dose-response meta-analysis of observational studies. J. Cancer 2021, 12, 3077–3088. [Google Scholar] [CrossRef] [PubMed]
- Rizk, M.; Guilloteau, A.; Mouillot, T.; Thiefin, G.; Bronowicki, J.P.; Richou, C.; Doffoel, M.; Diab Assaf, M.; Hillon, P.; Cottet, V. Dietary components modulate the risk of hepatocellular carcinoma in cirrhotic patients. Nutr. Res. 2019, 61, 82–94. [Google Scholar] [CrossRef] [PubMed]
- Stepien, M.; Duarte-Salles, T.; Fedirko, V.; Trichopoulou, A.; Lagiou, P.; Bamia, C.; Overvad, K.; Tjonneland, A.; Hansen, L.; Boutron-Ruault, M.C.; et al. Consumption of soft drinks and juices and risk of liver and biliary tract cancers in a European cohort. Eur. J. Nutr. 2016, 55, 7–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Setiawan, V.W.; Wilkens, L.R.; Lu, S.C.; Hernandez, B.Y.; Le Marchand, L.; Henderson, B.E. Association of coffee intake with reduced incidence of liver cancer and death from chronic liver disease in the US multiethnic cohort. Gastroenterology 2015, 148, 118–125. [Google Scholar] [CrossRef] [Green Version]
- Kennedy, O.J.; Fallowfield, J.A.; Poole, R.; Hayes, P.C.; Parkes, J.; Roderick, P.J. All coffee types decrease the risk of adverse clinical outcomes in chronic liver disease: A UK Biobank study. BMC Public Health 2021, 21, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Turati, F.; Trichopoulos, D.; Polesel, J.; Bravi, F.; Rossi, M.; Talamini, R.; Franceschi, S.; Montella, M.; Trichopoulou, A.; La Vecchia, C.; et al. Mediterranean diet and hepatocellular carcinoma. J. Hepatol. 2014, 60, 606–611. [Google Scholar] [CrossRef]
- Bogumil, D.; Park, S.Y.; Le Marchand, L.; Haiman, C.A.; Wilkens, L.R.; Boushey, C.J.; Setiawan, V.W. High-Quality Diets Are Associated With Reduced Risk of Hepatocellular Carcinoma and Chronic Liver Disease: The Multiethnic Cohort. Hepatol. Commun. 2019, 3, 437–447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shivappa, N.; Hebert, J.R.; Marcos, A.; Diaz, L.E.; Gomez, S.; Nova, E.; Michels, N.; Arouca, A.; Gonzalez-Gil, E.; Frederic, G.; et al. Association between dietary inflammatory index and inflammatory markers in the HELENA study. Mol. Nutr. Food Res. 2017, 61, 1600707. [Google Scholar] [CrossRef]
- Dyrstad, S.M.; Hansen, B.H.; Holme, I.M.; Anderssen, S.A. Comparison of self-reported versus accelerometer-measured physical activity. Med. Sci. Sports Exerc. 2014, 46, 99–106. [Google Scholar] [CrossRef]
- Saran, U.; Humar, B.; Kolly, P.; Dufour, J.-F. Hepatocellular carcinoma and lifestyles. J. Hepatol. 2016, 64, 203–214. [Google Scholar] [CrossRef]
- Lange, N.F.; Radu, P.; Dufour, J.F. Prevention of NAFLD-associated HCC: Role of lifestyle and chemoprevention. J. Hepatol. 2021, 75, 1217–1227. [Google Scholar] [CrossRef] [PubMed]
- Moore, S.C.; Lee, I.-M.; Weiderpass, E.; Campbell, P.T.; Sampson, J.N.; Kitahara, C.M.; Keadle, S.K.; Arem, H.; De Gonzalez, A.B.; Hartge, P. Association of leisure-time physical activity with risk of 26 types of cancer in 1.44 million adults. JAMA Intern. Med. 2016, 176, 816–825. [Google Scholar] [CrossRef] [PubMed]
- Kerr, J.; Anderson, C.; Lippman, S.M. Physic.cal activity, sedentary behaviour, diet, and cancer: An update and emerging new evidence. Lancet Oncol. 2017, 18, e457–e471. [Google Scholar] [CrossRef]
- Eliassen, A.H.; Hankinson, S.E.; Rosner, B.; Holmes, M.D.; Willett, W.C. Physical activity and risk of breast cancer among postmenopausal women. Arch. Intern. Med. 2010, 170, 1758–1764. [Google Scholar] [CrossRef] [Green Version]
- Aguiar e Silva, M.A.; Vechetti-Junior, I.J.; Nascimento, A.F.d.; Furtado, K.S.; Azevedo, L.; Ribeiro, D.A.; Barbisan, L.F. Effects of swim training on liver carcinogenesis in male Wistar rats fed a low-fat or high-fat diet. Appl.Physiol.Nutr. Metab. 2012, 37, 1101–1109. [Google Scholar] [CrossRef] [Green Version]
- Monda, M.; Messina, G.; Scognamiglio, I.; Lombardi, A.; Martin, G.A.; Sperlongano, P.; Porcelli, M.; Caraglia, M.; Stiuso, P. Short-term diet and moderate exercise in young overweight men modulate cardiocyte and hepatocarcinoma survival by oxidative stress. Oxidative Med. Cell. Longev. 2014. [Google Scholar] [CrossRef]
- Piguet, A.-C.; Saran, U.; Simillion, C.; Keller, I.; Terracciano, L.; Reeves, H.L.; Dufour, J.-F. Regular exercise decreases liver tumors development in hepatocyte-specific PTEN-deficient mice independently of steatosis. J. Hepatol. 2015, 62, 1296–1303. [Google Scholar] [CrossRef] [Green Version]
- Arfianti, A.; Pok, S.; Barn, V.; Haigh, W.G.; Yeh, M.M.; Ioannou, G.N.; Teoh, N.C.; Farrell, G.C. Exercise retards hepatocarcinogenesis in obese mice independently of weight control. J. Hepatol. 2020, 73, 140–148. [Google Scholar] [CrossRef]
- Saran, U.; Guarino, M.; Rodríguez, S.; Simillion, C.; Montani, M.; Foti, M.; Humar, B.; St-Pierre, M.V.; Dufour, J.F. Anti-tumoral effects of exercise on hepatocellular carcinoma growth. Hepatol. Commun. 2018, 2, 607–620. [Google Scholar] [CrossRef]
- Guarino, M.; Kumar, P.; Felser, A.; Terracciano, L.M.; Guixé-Muntet, S.; Humar, B.; Foti, M.; Nuoffer, J.-M.; St-Pierre, M.V.; Dufour, J.-F. Exercise attenuates the transition from Fatty Liver to Steatohepatitis and reduces tumor formation in Mice. Cancers 2020, 12, 1407. [Google Scholar] [CrossRef]
- Zhang, X.; Cao, L.; Ji, B.; Li, L.; Qi, Z.; Ding, S. Endurance training but not high-intensity interval training reduces liver carcinogenesis in mice with hepatocellular carcinogen diethylnitrosamine. Exp. Gerontol. 2020, 133, 110853. [Google Scholar] [CrossRef] [PubMed]
- Cao, L.; Zhang, X.; Ji, B.; Ding, S.; Qi, Z. Mod.derate endurance training reduced hepatic tumourigenesis associated with lower lactate overload compared to high-intensity interval training. Clin. Exp. Pharmacol. Physiol. 2021, 48, 1239–1250. [Google Scholar] [CrossRef] [PubMed]
- Yun, Y.H.; Lim, M.K.; Won, Y.-J.; Park, S.M.; Chang, Y.J.; Oh, S.W.; Shin, S.A. Dietary preference, physical activity, and cancer risk in men: National health insurance corporation study. BMC Cancer 2008, 8, 1–17. [Google Scholar] [CrossRef] [Green Version]
- Inoue, M. Impact of lifestyle on overall cancer risk among Japanese: The Japan Public Health Center-based Prospective Study (JPHC Study). J. Epidemiol. 2010, 20, 90–96. [Google Scholar] [CrossRef] [Green Version]
- Wen, C.-P.; Lin, J.; Yang, Y.C.; Tsai, M.K.; Tsao, C.K.; Etzel, C.; Huang, M.; Hsu, C.Y.; Ye, Y.; Mishra, L. Hepatocellular carcinoma risk prediction model for the general population: The predictive power of transaminases. J. Natl. Cancer Inst. 2012, 104, 1599–1611. [Google Scholar] [CrossRef] [PubMed]
- Behrens, G.; Matthews, C.E.; Moore, S.C.; Freedman, N.D.; McGlynn, K.A.; Everhart, J.E.; Hollenbeck, A.R.; Leitzmann, M.F. The association between frequency of vigorous physical activity and hepatobiliary cancers in the NIH-AARP Diet and Health Study. Eur. J. Epidemiol. 2013, 28, 55–66. [Google Scholar] [CrossRef] [Green Version]
- Arem, H.; Loftfield, E.; Saint-Maurice, P.F.; Freedman, N.D.; Matthews, C.E. Physical activity across the lifespan and liver cancer incidence in the NIH-AARP Diet and Health Study cohort. Cancer Med. 2018, 7, 1450–1457. [Google Scholar] [CrossRef] [Green Version]
- Baumeister, S.E.; Schlesinger, S.; Aleksandrova, K.; Jochem, C.; Jenab, M.; Gunter, M.J.; Overvad, K.; Tjønneland, A.; Boutron-Ruault, M.-C.; Carbonnel, F. Association between physical activity and risk of hepatobiliary cancers: A multinational cohort study. J. Hepatol. 2019, 70, 885–892. [Google Scholar] [CrossRef]
- Simon, T.G.; Kim, M.N.; Luo, X.; Yang, W.; Ma, Y.; Chong, D.Q.; Fuchs, C.S.; Meyerhardt, J.A.; Corey, K.E.; Chung, R.T. Physical activity compared to adiposity and risk of liver-related mortality: Results from two prospective, nationwide cohorts. J. Hepatol. 2020, 72, 1062–1069. [Google Scholar] [CrossRef] [Green Version]
- Luo, X.; Yang, W.; Ma, Y.; Simon, T.G.; Meyerhardt, J.A.; Chan, A.T.; Giovannucci, E.L.; Zhang, X. Physical activity and risk of hepatocellular carcinoma among US men and women. Cancer Prev. Res. 2020, 13, 707–714. [Google Scholar] [CrossRef] [Green Version]
- Lee, J. Associations between Physical Activity and Liver Cancer Risks and Mortality: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 8943. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.T.; Wang, J.J.; Luu, M.; Tseng, H.R.; Rich, N.E.; Lu, S.C.; Nissen, N.N.; Noureddin, M.; Singal, A.G.; Yang, J.D. State-Level HCC Incidence and Association With Obesity and Physical Activity in the United States. Hepatology 2021, 74, 1384–1394. [Google Scholar] [CrossRef]
- Feng, Y.; Powell, L.; Vassallo, A.J.; Hamer, M.; Stamatakis, E. Does adequate physical activity attenuate the associations of alcohol and alcohol-related cancer mortality? A pooled study of 54 686 British adults. Int. J. Cancer 2020, 147, 2754–2763. [Google Scholar] [CrossRef] [PubMed]
- Chun, H.S.; Park, S.; Lee, M.; Cho, Y.; Kim, H.S.; Choe, A.R.; Kim, H.Y.; Yoo, K.; Kim, T.H. Association of Physical Activity with the Risk of Hepatocellular Carcinoma in Patients with Chronic Hepatitis B. Cancers 2021, 13, 3424. [Google Scholar] [CrossRef]
- Kaibori, M.; Ishizaki, M.; Matsui, K.; Nakatake, R.; Yoshiuchi, S.; Kimura, Y.; Kwon, A.-H. Perioperative exercise for chronic liver injury patients with hepatocellular carcinoma undergoing hepatectomy. Am. J. Surg. 2013, 206, 202–209. [Google Scholar] [CrossRef] [PubMed]
- Kaibori, M.; Matsui, K.; Yoshii, K.; Ishizaki, M.; Iwasaka, J.; Miyauchi, T.; Kimura, Y. Perioperative exercise capacity in chronic liver injury patients with hepatocellular carcinoma undergoing hepatectomy. PLoS ONE 2019, 14, e0221079. [Google Scholar] [CrossRef] [Green Version]
- Koya, S.; Kawaguchi, T.; Hashida, R.; Goto, E.; Matsuse, H.; Saito, H.; Hirota, K.; Taira, R.; Matsushita, Y.; Imanaga, M. Effects of in-hospital exercise on liver function, physical ability, and muscle mass during treatment of hepatoma in patients with chronic liver disease. Hepatol. Res. 2017, 47, E22–E34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koya, S.; Kawaguchi, T.; Hashida, R.; Hirota, K.; Bekki, M.; Goto, E.; Yamada, M.; Sugimoto, M.; Hayashi, S.; Goshima, N. Effects of in-hospital exercise on sarcopenia in hepatoma patients who underwent transcatheter arterial chemoembolization. J. Gastroenterol. Hepatol. 2019, 34, 580–588. [Google Scholar] [CrossRef]
- Narao, H.; Hirota, K.; Koya, S.; Tomita, M.; Manako, Y.; Ogawa, S.; Nakao, N.; Tsutsumi, T.; Nakano, D.; Hashida, R. Effects of In-Hospital Physical Therapy on Activities of Daily Living in Patients with Hepatocellular Carcinoma. Int. J. Environ. Res. Public Health 2020, 17, 9098. [Google Scholar] [CrossRef]
- Tsuchihashi, J.; Koya, S.; Hirota, K.; Koga, N.; Narao, H.; Tomita, M.; Kawaguchi, T.; Hashida, R.; Nakano, D.; Tsutsumi, T. Effects of In-Hospital Exercise on Frailty in Patients with Hepatocellular Carcinoma. Cancers 2021, 13, 194. [Google Scholar] [CrossRef]
- Hyun, J.; Han, J.; Lee, C.; Yoon, M.; Jung, Y. Pathophysiological Aspects of Alcohol Metabolism in the Liver. Int. J. Mol. Sci. 2021, 22, 5717. [Google Scholar] [CrossRef]
- Chang, J.S.; Hsiao, J.R.; Chen, C.H. ALDH2 polymorphism and alcohol-related cancers in Asians: A public health perspective. J. Biomed. Sci. 2017, 24, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paradis, V.; Scoazec, J.Y.; Kollinger, M.; Holstege, A.; Moreau, A.; Feldmann, G.; Bedossa, P. Cellular and subcellular localization of acetaldehyde-protein adducts in liver biopsies from alcoholic patients. J. Histochem. Cytochem. 1996, 44, 1051–1057. [Google Scholar] [CrossRef]
- Siegmund, S.V.; Dooley, S.; Brenner, D.A. Molecular mechanisms of alcohol-induced hepatic fibrosis. Dig. Dis. 2005, 23, 264–274. [Google Scholar] [CrossRef]
- Haorah, J.; Ramirez, S.H.; Floreani, N.; Gorantla, S.; Morsey, B.; Persidsky, Y. Mechanism of alcohol-induced oxidative stress and neuronal injury. Free Radic. Biol. Med. 2008, 45, 1542–1550. [Google Scholar] [CrossRef] [Green Version]
- Hu, W.; Feng, Z.; Eveleigh, J.; Iyer, G.; Pan, J.; Amin, S.; Chung, F.L.; Tang, M.S. The major lipid peroxidation product, trans-4-hydroxy-2-nonenal, preferentially forms DNA adducts at codon 249 of human p53 gene, a unique mutational hotspot in hepatocellular carcinoma. Carcinogenesis 2002, 23, 1781–1789. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Yang, J.L.; Yu, K.K.; Xu, M.; Xu, Y.Z.; Chen, L.; Lu, Y.M.; Fang, H.S.; Wang, X.Y.; Hu, Z.Q.; et al. Activation of the NF-kappaB pathway as a mechanism of alcohol enhanced progression and metastasis of human hepatocellular carcinoma. Mol. Cancer 2015, 14, 10. [Google Scholar] [CrossRef] [Green Version]
- Asare, G.A.; Mossanda, K.S.; Kew, M.C.; Paterson, A.C.; Kahler-Venter, C.P.; Siziba, K. Hepatocellular carcinoma caused by iron overload: A possible mechanism of direct hepatocarcinogenicity. Toxicology 2006, 219, 41–52. [Google Scholar] [CrossRef] [PubMed]
- Lu, S.C.; Mato, J.M. Role of methionine adenosyltransferase and S-adenosylmethionine in alcohol-associated liver cancer. Alcohol 2005, 35, 227–234. [Google Scholar] [CrossRef]
- Tahmasebi Birgani, M.; Carloni, V. Tumor Microenvironment, a Paradigm in Hepatocellular Carcinoma Progression and Therapy. Int. J. Mol. Sci. 2017, 18, 405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ambade, A.; Satishchandran, A.; Gyongyosi, B.; Lowe, P.; Szabo, G. Adult mouse model of early hepatocellular carcinoma promoted by alcoholic liver disease. World J. Gastroenterol. 2016, 22, 4091–4108. [Google Scholar] [CrossRef]
- Hoechst, B.; Voigtlaender, T.; Ormandy, L.; Gamrekelashvili, J.; Zhao, F.; Wedemeyer, H.; Lehner, F.; Manns, M.P.; Greten, T.F.; Korangy, F. Myeloid derived suppressor cells inhibit natural killer cells in patients with hepatocellular carcinoma via the NKp30 receptor. Hepatology 2009, 50, 799–807. [Google Scholar] [CrossRef] [PubMed]
- Cai, L.; Zhang, Z.; Zhou, L.; Wang, H.; Fu, J.; Zhang, S.; Shi, M.; Zhang, H.; Yang, Y.; Wu, H.; et al. Functional impairment in circulating and intrahepatic NK cells and relative mechanism in hepatocellular carcinoma patients. Clin. Immunol. 2008, 129, 428–437. [Google Scholar] [CrossRef]
- Mathurin, P.; Deng, Q.G.; Keshavarzian, A.; Choudhary, S.; Holmes, E.W.; Tsukamoto, H. Exacerbation of alcoholic liver injury by enteral endotoxin in rats. Hepatology 2000, 32, 1008–1017. [Google Scholar] [CrossRef] [PubMed]
- Machida, K.; Cheng, K.T.; Sung, V.M.; Levine, A.M.; Foung, S.; Lai, M.M. Hepatitis C virus induces toll-like receptor 4 expression, leading to enhanced production of beta interferon and interleukin-6. J. Virol. 2006, 80, 866–874. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guyot, E.; Sutton, A.; Rufat, P.; Laguillier, C.; Mansouri, A.; Moreau, R.; Ganne-Carrie, N.; Beaugrand, M.; Charnaux, N.; Trinchet, J.C.; et al. PNPLA3 rs738409, hepatocellular carcinoma occurrence and risk model prediction in patients with cirrhosis. J. Hepatol. 2013, 58, 312–318. [Google Scholar] [CrossRef]
- Falleti, E.; Cussigh, A.; Cmet, S.; Fabris, C.; Toniutto, P. PNPLA3 rs738409 and TM6SF2 rs58542926 variants increase the risk of hepatocellular carcinoma in alcoholic cirrhosis. Dig. Liver Dis. 2016, 48, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Bellentani, S.; Saccoccio, G.; Costa, G.; Tiribelli, C.; Manenti, F.; Sodde, M.; Saveria Croce, L.; Sasso, F.; Pozzato, G.; Cristianini, G.; et al. Drinking habits as cofactors of risk for alcohol induced liver damage. The Dionysos Study Group. Gut 1997, 41, 845–850. [Google Scholar] [CrossRef] [Green Version]
- Savolainen, V.T.; Liesto, K.; Mannikko, A.; Penttila, A.; Karhunen, P.J. Alcohol consumption and alcoholic liver disease: Evidence of a threshold level of effects of ethanol. Alcohol Clin. Exp. Res. 1993, 17, 1112–1117. [Google Scholar] [CrossRef]
- Corrao, G.; Bagnardi, V.; Zambon, A.; La Vecchia, C. A meta-analysis of alcohol consumption and the risk of 15 diseases. Prev. Med. 2004, 38, 613–619. [Google Scholar] [CrossRef]
- Persson, E.C.; Schwartz, L.M.; Park, Y.; Trabert, B.; Hollenbeck, A.R.; Graubard, B.I.; Freedman, N.D.; McGlynn, K.A. Alcohol consumption, folate intake, hepatocellular carcinoma, and liver disease mortality. Cancer Epidemiol. Biomarkers Prev. 2013, 22, 415–421. [Google Scholar] [CrossRef] [Green Version]
- Grant, B.F.; Dufour, M.C.; Harford, T.C. Epidemiology of alcoholic liver disease. Semin. Liver Dis. 1988, 8, 12–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mancebo, A.; Gonzalez-Dieguez, M.L.; Cadahia, V.; Varela, M.; Perez, R.; Navascues, C.A.; Sotorrios, N.G.; Martinez, M.; Rodrigo, L.; Rodriguez, M. Annual incidence of hepatocellular carcinoma among patients with alcoholic cirrhosis and identification of risk groups. Clin. Gastroenterol. Hepatol. 2013, 11, 95–101. [Google Scholar] [CrossRef]
- Torisu, Y.; Ikeda, K.; Kobayashi, M.; Hosaka, T.; Sezaki, H.; Akuta, N.; Kawamura, Y.; Yatsuji, H.; Suzuki, F.; Suzuki, Y.; et al. Diabetes mellitus increases the risk of hepatocarcinogenesis in patients with alcoholic cirrhosis: A preliminary report. Hepatol. Res. 2007, 37, 517–523. [Google Scholar] [CrossRef]
- Kodama, K.; Tokushige, K.; Hashimoto, E.; Taniai, M.; Shiratori, K. Hepatic and extrahepatic malignancies in cirrhosis caused by nonalcoholic steatohepatitis and alcoholic liver disease. Alcohol Clin. Exp. Res. 2013, 37 (Suppl. S1), E247–E252. [Google Scholar] [CrossRef]
- N’Kontchou, G.; Paries, J.; Htar, M.T.; Ganne-Carrie, N.; Costentin, L.; Grando-Lemaire, V.; Trinchet, J.C.; Beaugrand, M. Risk factors for hepatocellular carcinoma in patients with alcoholic or viral C cirrhosis. Clin. Gastroenterol. Hepatol. 2006, 4, 1062–1068. [Google Scholar] [CrossRef]
- Ganne-Carrie, N.; Chaffaut, C.; Bourcier, V.; Archambeaud, I.; Perarnau, J.M.; Oberti, F.; Roulot, D.; Moreno, C.; Louvet, A.; Dao, T.; et al. Estimate of hepatocellular carcinoma incidence in patients with alcoholic cirrhosis. J. Hepatol. 2018, 69, 1274–1283. [Google Scholar] [CrossRef]
- Mandayam, S.; Jamal, M.M.; Morgan, T.R. Epidemiology of alcoholic liver disease. Semin. Liver Dis. 2004, 24, 217–232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donato, F.; Tagger, A.; Gelatti, U.; Parrinello, G.; Boffetta, P.; Albertini, A.; Decarli, A.; Trevisi, P.; Ribero, M.L.; Martelli, C.; et al. Alcohol and hepatocellular carcinoma: The effect of lifetime intake and hepatitis virus infections in men and women. Am. J. Epidemiol. 2002, 155, 323–331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baraona, E.; Abittan, C.S.; Dohmen, K.; Moretti, M.; Pozzato, G.; Chayes, Z.W.; Schaefer, C.; Lieber, C.S. Gender differences in pharmacokinetics of alcohol. Alcohol Clin. Exp. Res. 2001, 25, 502–507. [Google Scholar] [CrossRef] [PubMed]
- Ikejima, K.; Enomoto, N.; Iimuro, Y.; Ikejima, A.; Fang, D.; Xu, J.; Forman, D.T.; Brenner, D.A.; Thurman, R.G. Estrogen increases sensitivity of hepatic Kupffer cells to endotoxin. Am. J. Physiol. 1998, 274, G669–G676. [Google Scholar] [CrossRef]
- Wu, H.; Yao, S.; Zhang, S.; Wang, J.R.; Guo, P.D.; Li, X.M.; Gan, W.J.; Mei, L.; Gao, T.M.; Li, J.M. Elevated expression of Erbin destabilizes ERalpha protein and promotes tumorigenesis in hepatocellular carcinoma. J. Hepatol. 2017, 66, 1193–1204. [Google Scholar] [CrossRef] [PubMed]
- Naugler, W.E.; Sakurai, T.; Kim, S.; Maeda, S.; Kim, K.; Elsharkawy, A.M.; Karin, M. Gender disparity in liver cancer due to sex differences in MyD88-dependent IL-6 production. Science 2007, 317, 121–124. [Google Scholar] [CrossRef] [Green Version]
- Yuan, J.M.; Govindarajan, S.; Arakawa, K.; Yu, M.C. Synergism of alcohol, diabetes, and viral hepatitis on the risk of hepatocellular carcinoma in blacks and whites in the U.S. Cancer 2004, 101, 1009–1017. [Google Scholar] [CrossRef] [PubMed]
- Tovar, V.; Alsinet, C.; Villanueva, A.; Hoshida, Y.; Chiang, D.Y.; Sole, M.; Thung, S.; Moyano, S.; Toffanin, S.; Minguez, B.; et al. IGF activation in a molecular subclass of hepatocellular carcinoma and pre-clinical efficacy of IGF-1R blockage. J. Hepatol. 2010, 52, 550–559. [Google Scholar] [CrossRef] [Green Version]
- Loomba, R.; Yang, H.I.; Su, J.; Brenner, D.; Barrett-Connor, E.; Iloeje, U.; Chen, C.J. Synergism between obesity and alcohol in increasing the risk of hepatocellular carcinoma: A prospective cohort study. Am. J. Epidemiol. 2013, 177, 333–342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costentin, C.E.; Mourad, A.; Lahmek, P.; Causse, X.; Pariente, A.; Hagege, H.; Dobrin, A.S.; Becker, C.; Marks, B.; Bader, R.; et al. Hepatocellular carcinoma is diagnosed at a later stage in alcoholic patients: Results of a prospective, nationwide study. Cancer 2018, 124, 1964–1972. [Google Scholar] [CrossRef]
- Heckley, G.A.; Jarl, J.; Asamoah, B.O.; G-Gerdtham, U. How the risk of liver cancer changes after alcohol cessation: A review and meta-analysis of the current literature. BMC Cancer 2011, 11, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Trichopoulos, D.; Bamia, C.; Lagiou, P.; Fedirko, V.; Trepo, E.; Jenab, M.; Pischon, T.; Nothlings, U.; Overved, K.; Tjonneland, A.; et al. Hepatocellular carcinoma ris.sk factors and disease burden in a European cohort: A nested case-control study. J. Natl. Cancer Inst. 2011, 103, 1686–1695. [Google Scholar] [CrossRef]
- Lee, Y.C.; Cohet, C.; Yang, Y.C.; Stayner, L.; Hashibe, M.; Straif, K. Meta-analysis of epidemiologic studies on cigarette smoking and liver cancer. Int. J. Epidemiol. 2009, 38, 1497–1511. [Google Scholar] [CrossRef]
- Mukaiya, M.; Nishi, M.; Miyake, H.; Hirata, K. Chronic liver diseases for the risk of hepatocellular carcinoma: A case-control study in Japan. Etiologic association of alcohol consumption, cigarette smoking and the development of chronic liver diseases. Hepatogastroenterology 1998, 45, 2328–2332. [Google Scholar] [PubMed]
- Petrick, J.L.; Campbell, P.T.; Koshiol, J.; Thistle, J.E.; Andreotti, G.; Beane-Freeman, L.E.; Buring, J.E.; Chan, A.T.; Chong, D.Q.; Doody, M.M.; et al. Tobacco, alcohol use and risk of hepatocellular carcinoma and intrahepatic cholangiocarcinoma: The Liver Cancer Pooling Project. Br. J. Cancer 2018, 118, 1005–1012. [Google Scholar] [CrossRef] [PubMed]
- Yu, M.W.; Yang, S.Y.; Chiu, Y.H.; Chiang, Y.C.; Liaw, Y.F.; Chen, C.J. A p53 genetic polymorphism as a modulator of hepatocellular carcinoma risk in relation to chronic liver disease, familial tendency, and cigarette smoking in hepatitis B carriers. Hepatology 1999, 29, 697–702. [Google Scholar] [CrossRef]
- Moszczynski, P.; Zabinski, Z.; Moszczynski, P., Jr.; Rutowski, J.; Slowinski, S.; Tabarowski, Z. Immunological findings in cigarette smokers. Toxicol. Lett. 2001, 118, 121–127. [Google Scholar] [CrossRef]
- Watanabe, K.; Eto, K.; Furuno, K.; Mori, T.; Kawasaki, H.; Gomita, Y. Effect of cigarette smoke on lipid peroxidation and liver function tests in rats. Acta Med. Okayama 1995, 49, 271–274. [Google Scholar] [CrossRef]
- El-Zayadi, A.R. Heavy smoking and liver. World J. Gastroenterol. 2006, 12, 6098–6101. [Google Scholar] [CrossRef]
- Wang, H.; Chen, L.; Zhou, T.; Zhang, Z.; Zeng, C. p53 Mutation at Serine 249 and Its Gain of Function Are Highly Related to Hepatocellular Carcinoma after Smoking Exposure. Public Health Genom. 2021, 24, 171–181. [Google Scholar] [CrossRef]
- Guarino, M.; Dufour, J.F. Smoking favours hepatocellular carcinoma. Ann. Transl. Med. 2019, 7, S99. [Google Scholar] [CrossRef]
- Zhang, L.; Huang, Y.; Zhu, Y.; Yu, Z.; Shao, M.; Luo, Y. Identification and Characterization of Cadmium-Related Genes in Liver Carcinoma. Biol. Trace Elem. Res. 2018, 182, 238–247. [Google Scholar] [CrossRef]
- Tabata, Y.; Omori, M.; Shidoji, Y. Age-Dependent Decrease in Hepatic Geranylgeranoic Acid Content in C3H/HeN Mice and Its Oral Supplementation Prevents Spontaneou.us Hepatoma. Metabolites 2021, 11, 634. [Google Scholar] [CrossRef]
- Tabata, Y.; Shidoji, Y. Hepatic monoamine oxidase B is involved in endogenous geranylgeranoic acid synthesis in mammalian liver cells. J. Lipid Res. 2020, 61, 778–789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sari, Y.; Khalil, A. Monoamine Oxidase Inhibitors Extracted from Tobacco Smoke as Neuroprotective Factors for Potential Treatment of Parkinson’s Disease. CNS Neurol. Disord. Drug Targets 2015, 14, 777–785. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Author, Year of Publication (Ref) | Study Design Cohort Study/Meta-Analysis of Cohort Studies | Study Population and Sample Size | Nutrient/Food Group | Adjusted HR/RR (CI) of Highest Category vs. Lowest Category | Nutrient/Food Intake Categories Which Were Compared (Highest Category vs. Reference Category) |
|---|---|---|---|---|---|
| Liu Y., 2021 [5] | Prospective cohort | Nurses’ Health Study (n = 88,770 women). The Health Professionals Follow-up Study (n = 48,197 men) | Plant based low-carbohydrate diet | 0.83 (0.70–0.98) | Per 1 standard deviation increase |
| Carbohydrates from refined grains | 1.18 (1.00–1.39) | Per 1 standard deviation increase | |||
| Plant fat | 0.78 (0.65–0.95) | Per 1 standard deviation increase | |||
| Shah SC., 2021 [6] | Prospective cohort | The NIH-American Association of Retired Persons (NIH-AARP) Diet and Health Study (n = 536,359) | Magnesium (diet + supplements) | 0.65 (0.48–0.87) | 4th vs. 1st quartile |
| Luu HN., 2021 [7] | Prospective cohort | Singapore Chinese Health Study (n = 63,2570) | Alternative Health Eating Index-2010 (AHEI-2010) | 0.69 (0.53–0.89) | 4th vs. 1st quartile |
| Alternate Mediterranean Diet (aMED) | 0.70 (0.52–0.95) | 4th vs. 1st quartile | |||
| Dietary Approaches to Stop Hypertension (DASH) | 0.67 (0.51–0.87) | 4th vs. 1st quartile | |||
| Yang W., 2021 [8] | Prospective cohort | Nurses’ Health Study (n =70,055 women). Health Professionals Follow-up Study (n = 49,261 men) | Empirical lifestyle pattern score for hyperinsulinemia (ELIH) | 1.89 (1.25–2.87) | 3rd vs. 1st tertile |
| Empirical lifestyle pattern score for insulin resistance (ELIR) | 2.05 (1.34–3.14) | 3rd vs. 1st tertile | |||
| Empirical dietary inflammatory pattern (EDIP) | 2.03 (1.31–3.16) | 3rd vs. 1st tertile | |||
| Ji XW., 2021 [9] | Prospective cohort | Chinese men (n = 59 998) | Total fat | 1.33 (1.01–1.75) | 4th vs. 1st quartile |
| Saturated fat | 1.50 (1.13–1.97) | 4th vs. 1st quartile | |||
| Monounsaturated fat | 1.26 (0.96–1.65) | 4th vs. 1st quartile | |||
| Polyunsaturated fat | 1.41 (1.07–1.86) | 4th vs. 1st quartile | |||
| Luo Y., 2020 [10] | Prospective cohort | Patients with new HCC enrolled in the Guangdong Liver Cancer Cohort (n = 887) | Chinese Healthy Eating Index (CHEI-2016) | 0.74 (0.56–0.98) Outcome: HCC specific mortality | 3rd vs. 1st tertile |
| Healthy Eating Index-2015 (HEI-2015) | 0.93 (0.71–1.21) Outcome: HCC specific mortality | 3rd vs. 1st tertile | |||
| Zhong GC., 2020 [11] | Prospective cohort | American adults from the prostate, lung, colorectal and ovarian cancer screening trial (n = 103,902) | Dietary inflammatory index (DII) from food and supplements | 2.05 (1.23–3.41) Outcome: PLC incidence | 3rd vs. 1st tertile |
| Dietary inflammatory index (DII) from food and supplements | 1.97 (1.13–3.41) Outcome: PLC mortality (n = 102) | 3rd vs. 1st tertile | |||
| Dietary inflammatory index (DII) from food only | 2.57 (1.44–4.60) Outcome: PLC incidence | 3rd vs. 1st tertile | |||
| Jayedi A., 2020 [12] | Umbrella Review of Meta-Analyses of Prospective Cohort Studies (5 Meta-analyses) | Mixed populations | Fish | 0.65 (0.48–0.87) | per 100 gr/day |
| Zhong GC., 2020 [13] | Prospective cohort | American adults from the prostate, lung, colorectal and ovarian cancer screening trial (n = 104,025) | Magnesium (diet + supplements) | 0.44 (0.24–0.80) Outcome: PLC incidence | 3rd vs. 1st tertile |
| Magnesium (diet + supplements) | 0.83 (0.67–1.01) Outcome: PLC incidence | Per 100 mg/d | |||
| Dietary magnesium | 0.41 (0.22–0.76) Outcome: PLC incidence | 3rd vs. 1st tertile | |||
| Dietary magnesium | 0.65 (0.51–0.82) Outcome: PLC incidence | Per 100 mg/d | |||
| Magnesium (diet + supplements) | 0.37 (0.19–0.71) Outcome: PLC mortality | 3rd vs. 1st tertile | |||
| Yang W., 2020 [14] | Prospective cohort | Nurses’ Health Study (n =88,657 women). Health Professionals Follow-up Study (n = 49,826 men) | Vegetable fats | 0.61 (0.39–0.96) | 17.7 vs. 8.7 (% energy) |
| n-3 PUFA | 0.63 (0.41–0.96) | 0.8 vs. 0.5 (% energy) | |||
| n-6 PUFA | 0.54 (0.34–0.86) | 6.5 vs. 3.7 (% energy) | |||
| Yang W., 2020 [15] | Prospective cohort | Nurses’ Health Study (n = 93,427 women). Health Professionals Follow-up Study (n = 51,418 men) | High-fat dairy | 1.81 (1.19–2.76) | 2.0 vs. 0.4 serving/day |
| Low-fat dairy | 1.18 (0.78, 1.78) | 1.9 vs. 0.2 serving/day | |||
| Butter | 1.58 (1.06–2.36) | 0.7 vs. 0 serving/day | |||
| Yogurt | 0.72 (0.49–1.05) | 0.2 vs. 0 serving/day | |||
| Kim TL., 2020 [16] | Umbrella Review of Meta-analyses of observational studies (2) | Mixed populations | Green tea | 0.87 (0.78–0.98) | High vs. low |
| Guo XF., 2019 [17] | Meta-analysis (9 cohorts) | 1,326,176 participants | Vegetable | 0.96 (0.95–0.97) | Per 100 gr/d |
| Ma Y., 2019 [18] | Prospective cohort | Nurses’ Health Study (n = 92,389 women). Health Professionals Follow-up Study (n = 50,468 men). | Processed red meat | 1.84 (1.16–2.92) | 3rd vs. 1st tertile |
| Total white meat | 0.61 (0.40–0.91) | 3rd vs. 1st tertile | |||
| Unprocessed red meat | 1.06 (0.68–1.63) | 3rd vs. 1st tertile | |||
| Poultry | 0.60 (0.40–0.90) | 3rd vs. 1st tertile | |||
| Fish | 0.70 (0.47–1.05) | 3rd vs. 1st tertile | |||
| Ma Y., 2019 [19] | Prospective cohort | Nurses’ Health Study (n = 121,700 women). Health Professionals Follow-up Study (n = 51,529 men) | Alternative Healthy Eating Index-2010 (AHEI-2010) | 0.61 (0.39–0.95) | 3rd vs. 1st tertile |
| Tran KT., (2019) [20] | Prospective cohort | UK Biobank population (n = 471,779) | Coffee | 0.50 (0.29–0.87) | Any consumption vs. none |
| Instant coffee | 0.51 (0.28–0.93) | Any consumption vs. none | |||
| Ground coffee | 0.47 (0.20–1.08) | Any consumption vs. none | |||
| Kennedy OJ., 2017 [21] | Meta-analysis (18 cohorts) | Mixed populations, 2,272,642 participants | Coffee | 0.71 (0.65–0.77) | An extra two cups per day |
| 2 cohorts | Approximately 850,000 participants | Caffeinated coffee | 0.73 (0.63–0.85) | An extra two cups per day | |
| 3 cohorts | Approximately 750,000 participants | Decaffeinated coffee | 0.86 (0.74–1.00) | An extra two cups per day | |
| Gao M., 2015 [22] | Meta-analysis (3 cohorts) | Mixed populations, 693,274 participants | Fish | 0.73 (0.56–0.90) | Highest vs. lowest consumption |
| Yang Y., 2014 [23] | Meta-analysis (9 cohorts) | Mixed populations, 1,474,309 participants | Vegetables | 0.66 (0.51–0.86) | Highest vs. lowest consumption |
| Luo J., 2014 [24] | Meta-analysis (7 cohorts) | Mixed populations, 2,677,514 participants | Red meat | 1.43 (1.08–1.90) | Highest vs. lowest consumption |
| White meat | 0.70 (0.57–0.86) | Highest vs. lowest consumption | |||
| Fish | 0.74 (0.61–0.91) | Highest vs. lowest consumption | |||
| Bravi F., 2013, [25] | Meta-analysis (8 cohorts) | Mixed populations, 378,392 participants | Coffee | 0.64 (0.52–0.7) | No consumption vs. any consumption |
| Fedirko V., 2013 [26] | Cohort | European Prospective Investigation into Cancer and Nutrition cohort (n = 477,206) | Total sugar | 1.43 (1.17–1.74) | Per 50 gr/day |
| Total dietary fiber | 0.70 (0.52–0.93) | Per 10 gr/day | |||
| Sawada N., 2012 [27] | Prospective cohort | Population-based prospective cohort of Japanese subjects (n = 90,296) | Fish (rich in n-3 PUFA) | 0.64 (0.42–0.96) | 70.6 vs. 9.6 gr/day |
| EPA | 0.56 (0.36–0.85) | 0.74 vs. 0.14 g/day | |||
| DHA | 0.56 (0.35–0.87) | 1.19 vs. 0.28 g/day | |||
| Freedman ND., 2010 [28] | Cohort | Men and women of the National Institutes of Health–AARP Diet and Health Study (n = 495,006) | White meat | 0.52 (0.36–0.77) | 65.8 vs. 9.7 g/1000 kcal |
| Red meat | 1.74 (1.16–2.61) | 64.8 vs. 10 g/1000 kcal | |||
| Ioannou GN., 2009 [29] | Cohort | General US population from the first National Health and Nutrition Examination Survey (n = 9221) | Cholesterol | 2.45 (1.3–4.7) | ≥511 vs. <156 mg/d |
| Study | Number | Location | Length of Follow Up (Year) | HCC Cases (#) | Incidence |
|---|---|---|---|---|---|
| Torisu et al. [104] | 47 | Japan | 6.8 | 9 | 2.1 |
| Kodama et al. [105] | 85 | Japan | 3.0 | 6 | 2.5 |
| Mancebo et al. [103] | 450 | Spain | 3.5 | 62 | 2.6 |
| N’kontchou et al. [106] | 478 | France | 4.2 | 108 | 5.6 |
| Ganne-Carrie et al. [107] | 652 | France/Belgium | 2.4 | 43 | 2.9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zelber-Sagi, S.; Noureddin, M.; Shibolet, O. Lifestyle and Hepatocellular Carcinoma What Is the Evidence and Prevention Recommendations. Cancers 2022, 14, 103. https://doi.org/10.3390/cancers14010103
Zelber-Sagi S, Noureddin M, Shibolet O. Lifestyle and Hepatocellular Carcinoma What Is the Evidence and Prevention Recommendations. Cancers. 2022; 14(1):103. https://doi.org/10.3390/cancers14010103
Chicago/Turabian StyleZelber-Sagi, Shira, Mazen Noureddin, and Oren Shibolet. 2022. "Lifestyle and Hepatocellular Carcinoma What Is the Evidence and Prevention Recommendations" Cancers 14, no. 1: 103. https://doi.org/10.3390/cancers14010103
APA StyleZelber-Sagi, S., Noureddin, M., & Shibolet, O. (2022). Lifestyle and Hepatocellular Carcinoma What Is the Evidence and Prevention Recommendations. Cancers, 14(1), 103. https://doi.org/10.3390/cancers14010103