
Increased Production of B-Cell Activating Cytokines and Altered Peripheral B-Cell Subset Distribution during HIV-Related Classical Hodgkin Lymphoma

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Patients and Methods
2.1. Patient Populations
2.2. Immunological Analyses
2.3. Statistical Analyses
3. Results
3.1. Characteristics of Patients at cHL Diagnosis
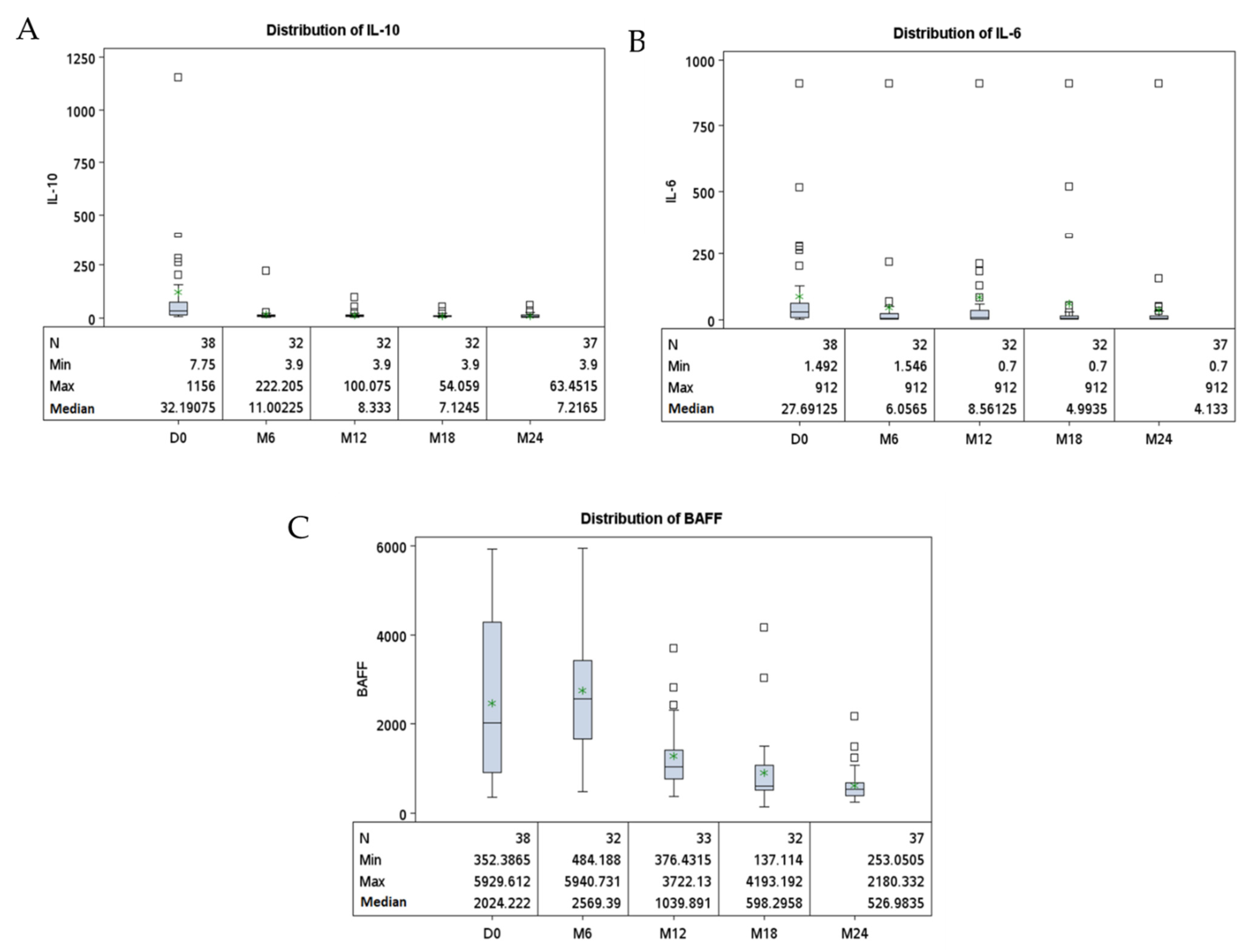
3.2. Increased Serum Levels of Cytokines Related to B-Cell Activation (IL10, IL6 and BAFF) in HIV-cHL Patients at cHL Diagnosis
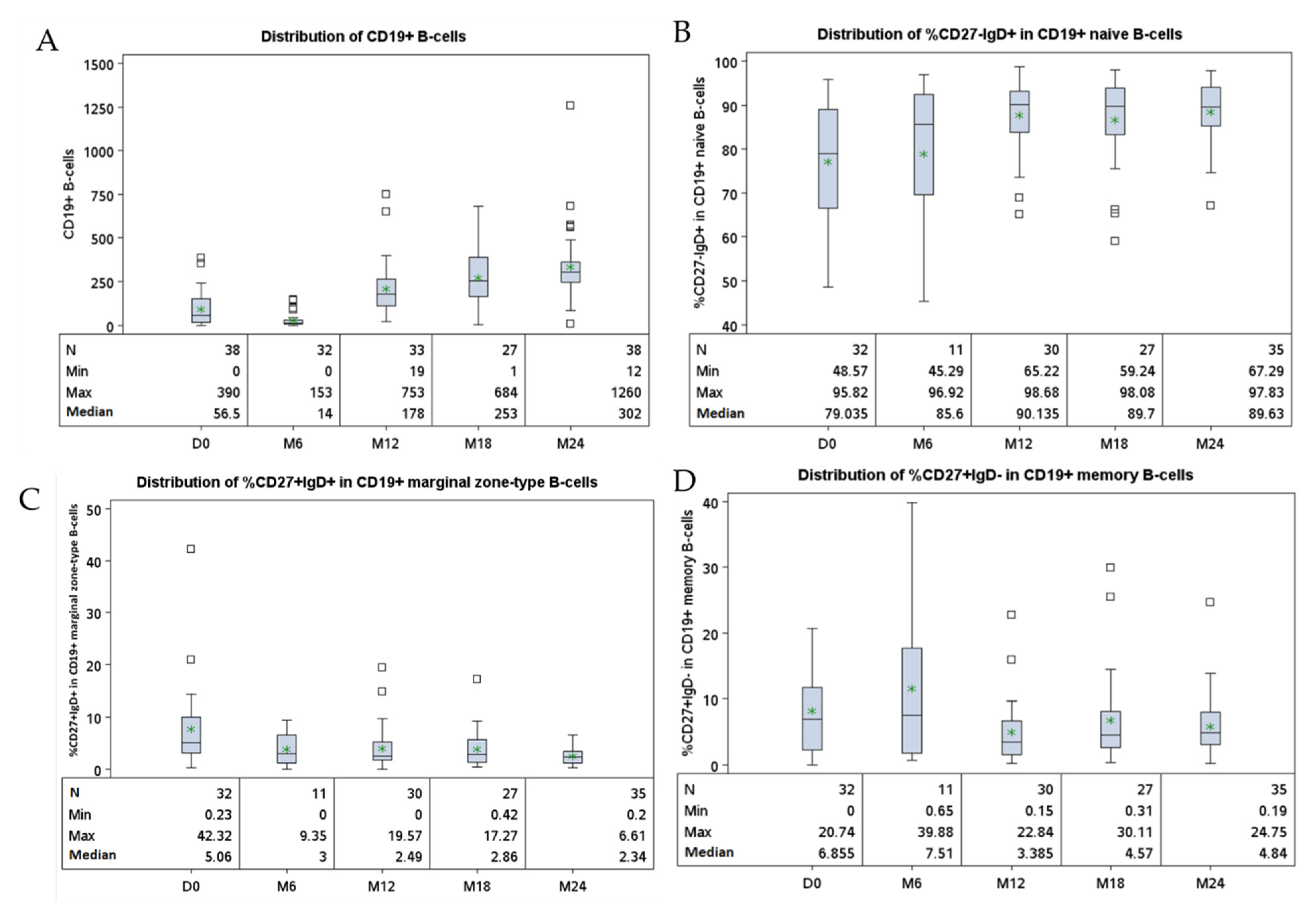
3.3. Altered Peripheral B-Cell Compartment in HIV-1 Infected-Patients Developing cHL
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Swerdlow, S.H.; Campo, E.; Harris, N.L.; Jaffe, E.S.; Pileri, S.A.; Thiele, J.; Stein, H. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues WHO Classification of Tumours, 4th ed.; International Agency for Research on Cancer: Lyon, France, 2016; Volume 2. [Google Scholar]
- Clifford, G.M.; Polesel, J.; Rickenbach, M.; Dal Maso, L.; Keiser, O.; Kofler, A.; Rapiti, E.; Levi, F.; Jundt, G.; Fisch, T.; et al. Cancer risk in the swiss HIV cohort study: Associations with immunodeficiency, smoking, and highly active antiretroviral therapy. J. Natl. Cancer Inst. 2005, 97, 425–432. [Google Scholar] [CrossRef] [Green Version]
- Frisch, M.; Biggar, R.J.; Engels, E.A.; Goedert, J.J.; AIDS-Cancer Match Registry Study Group. Association of cancer with AIDS-Related immunosuppression in adults. JAMA 2001, 285, 1736–1745. [Google Scholar] [CrossRef] [PubMed]
- Dal Maso, L.; Franceschi, S.; Polesel, J.; Braga, C.; Piselli, P.; Crocetti, E.; Falcini, F.; Guzzinati, S.; Zanetti, R.; Vercelli, M.; et al. Risk of cancer in persons with AIDS in Italy, 1985–1998. Br. J. Cancer 2003, 89, 94–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biggar, R.J.; Jaffe, E.S.; Goedert, J.J.; Chaturvedi, A.; Pfeiffer, R.; Engels, E.A. Hodgkin lymphoma and immunodeficiency in persons with HIV/AIDS. Blood 2006, 108, 3786–3791. [Google Scholar] [CrossRef]
- Shebl, F.M.; Yu, K.; Landgren, O.; Goedert, J.J.; Rabkin, C.S. Increased levels of circulating cytokines with HIV-related immunosuppression. AIDS Res. Hum. Retrovir. 2012, 28, 809–815. [Google Scholar] [CrossRef]
- Kowalkowski, M.A.; Mims, M.P.; Amiran, E.S.; Lulla, P.; Chiao, E.Y. Effect of immune reconstitution on the incidence of HIV-related Hodgkin lymphoma. PLoS ONE 2013, 8, e77409. [Google Scholar] [CrossRef] [Green Version]
- Levin, L.I.; Breen, E.C.; Birmann, B.M.; Batista, J.L.; Magpantay, L.I.; Li, Y.; Ambinder, R.F.; Mueller, N.E.; Martínez-Maza, O. Elevated serum levels of SCD30 and IL6 and detectable IL10 precede classical Hodgkin lymphoma diagnosis. Cancer Epidemiol. Biomark. Prev. 2017, 26, 1114–1123. [Google Scholar] [CrossRef] [Green Version]
- Breen, E.C.; Hussain, S.K.; Magpantay, L.; Jacobson, L.P.; Detels, R.; Rabkin, C.S.; Kaslow, R.A.; Variakojis, D.; Bream, J.H.; Rinaldo, C.R.; et al. B-Cell stimulatory cytokines and markers of immune activation are elevated several years prior to the diagnosis of systemic AIDS-associated non-Hodgkin B-cell lymphoma. Cancer Epidemiol. Biomark. 2011, 20, 1303–1314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bibas, M.; Trotta, M.P.; Cozzi-Lepri, A.; Lorenzini, P.; Pinnetti, C.; Rizzardini, G.; Angarano, G.; Caramello, P.; Sighinolfi, L.; Mastroianni, C.M.; et al. Role of serum free light chains in predicting HIV-associated non-Hodgkin lymphoma and Hodgkin’s lymphoma and its correlation with antiretroviral therapy. Am. J. Hematol. 2012, 87, 749–753. [Google Scholar] [CrossRef] [PubMed]
- Tittle, V.; Rayment, M.; Keeling, E.; Gabriel, I.; Yarranton, H.; Bower, M. Serum-free light chains in HIV-associated lymphoma: No correlation with histology or prognosis. AIDS Lond. Engl. 2015, 29, 1201–1204. [Google Scholar] [CrossRef] [PubMed]
- Gajl-Peczalska, K.J.; Hansen, J.A.; Bloomfield, C.D.; Good, R.A. B Lymphocytes in untreated patients with malignant lymphoma and Hodgkin’s disease. J. Clin. Investig. 1973, 52, 3064–3073. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Sousa, M.; Tan, C.T.; Siegal, F.P.; Filippa, D.A.; Tan, R.; Good, R.A. Immunologic parameters in childhood Hodgkin’s disease II. T and B lymphocytes in the peripheral blood of normal children and in the spleen and peripheral blood of children with Hodgkin’s disease. Pediatr. Res. 1978, 12, 143–147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamdi, L.; Creidy, R.; Boudjemaa, S.; Hendel-Chavez, H.; Hugues, P.; Taoufik, Y.; Leblanc, T.; Coulomb, A.; Krzysiek, R.; Landman-Parker, J.; et al. Frequent altered distribution of peripheral B-lymphocyte subsets in pediatric and adolescent patients with classical Hodgkin lymphoma. Leuk. Lymphoma 2021, 62, 300–307. [Google Scholar] [CrossRef] [PubMed]
- Garcillán, B.; Figgett, W.A.; Infantino, S.; Lim, E.X.; Mackay, F. Molecular control of b-cell homeostasis in health and malignancy. Immunol. Cell Biol. 2018, 96, 453–462. [Google Scholar] [CrossRef]
- Besson, C.; Lancar, R.; Prevot, S.; Brice, P.; Meyohas, M.-C.; Marchou, B.; Gabarre, J.; Bonnet, F.; Goujard, C.; Lambotte, O.; et al. High risk features contrast with favorable outcomes in HIV-associated Hodgkin lymphoma in the modern CART era, ANRS CO16 LYMPHOVIR Cohort. Clin. Infect. Dis. 2015, 61, 1469–1475. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Besson, C.; Lancar, R.; Prevot, S.; Algarte-Genin, M.; Delobel, P.; Bonnet, F.; Meyohas, M.-C.; Partisani, M.; Oberic, L.; Gabarre, J.; et al. Outcomes for HIV-associated diffuse large B-cell lymphoma in the modern combined antiretroviral therapy era. AIDS Lond. Engl. 2017, 31, 2493–2501. [Google Scholar] [CrossRef] [PubMed]
- Lupo, J.; Germi, R.; Lancar, R.; Algarte-Genin, M.; Hendel-Chavez, H.; Taoufik, Y.; Mounier, N.; Partisani, M.; Bonnet, F.; Meyohas, M.-C.; et al. Epstein–Barr virus biomarkers have no prognostic value in HIV-related hodgkin lymphoma in the modern combined antiretroviral therapy era. AIDS 2019, 33, 993–1000. [Google Scholar] [CrossRef]
- Hohaus, S.; Giachelia, M.; Massini, G.; Vannata, B.; Criscuolo, M.; Martini, M.; D’Alo’, F.; Voso, M.T.; Larocca, L.M.; Leone, G. Clinical significance of interleukin-10 gene polymorphisms and plasma levels in Hodgkin lymphoma. Leuk. Res. 2009, 33, 1352–1356. [Google Scholar] [CrossRef] [PubMed]
- Planès, R.; Serrero, M.; Leghmari, K.; BenMohamed, L.; Bahraoui, E. HIV-1 envelope glycoproteins induce the production of TNF-α and il-10 in human monocytes by activating calcium pathway. Sci. Rep. 2018, 8, 17215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ji, J.; Sahu, G.K.; Braciale, V.L.; Cloyd, M.W. HIV-1 Induces IL-10 production in human monocytes via a CD4-independent pathway. Int. Immunol. 2005, 17, 729–736. [Google Scholar] [CrossRef] [Green Version]
- Jiang, Y.; Yang, M.; Sun, X.; Chen, X.; Ma, M.; Yin, X.; Qian, S.; Zhang, Z.; Fu, Y.; Liu, J.; et al. IL-10+ NK and TGF-Β+ NK cells play negative regulatory roles in HIV infection. BMC Infect. Dis. 2018, 18, 80. [Google Scholar] [CrossRef] [Green Version]
- Schett, G.; Elewaut, D.; McInnes, I.B.; Dayer, J.-M.; Neurath, M.F. How cytokine networks fuel inflammation: Toward a cytokine-based disease taxonomy. Nat. Med. 2013, 19, 822–824. [Google Scholar] [CrossRef] [PubMed]
- Yasukawa, K.; Hirano, T.; Watanabe, Y.; Muratani, K.; Matsuda, T.; Nakai, S.; Kishimoto, T. Structure and expression of human b cell stimulatory factor-2 (BSF-2/IL-6) Gene. EMBO J. 1987, 6, 2939–2945. [Google Scholar] [CrossRef]
- Bethin, K.E.; Vogt, S.K.; Muglia, L.J. Interleukin-6 is an essential, corticotropin-releasing hormone-independent stimulator of the adrenal axis during immune system activation. Proc. Natl. Acad. Sci. USA 2000, 97, 9317–9322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diehl, S.; Rincón, M. The two faces of IL-6 on Th1/Th2 differentiation. Mol. Immunol. 2002, 39, 531–536. [Google Scholar] [CrossRef]
- Taga, T.; Kishimoto, T. Role of a Two-Chain IL-6 receptor system in immune and hematopoietic cell regulation. Crit. Rev. Immunol. 1992, 11, 265–280. [Google Scholar]
- Cheung, W.-C.; Van Ness, B. Distinct IL-6 signal transduction leads to growth arrest and death cin B cells or growth promotion and cell survival in myeloma cells. Leukemia 2002, 16, 1182–1188. [Google Scholar] [CrossRef] [Green Version]
- Gilbert, L.A.; Hemann, M.T. Context-specific roles for paracrine IL-6 in lymphomagenesis. Genes Dev. 2012, 26, 1758–1768. [Google Scholar] [CrossRef] [Green Version]
- Mackay, F.; Schneider, P. Cracking the BAFF code. Nat. Rev. Immunol. 2009, 9, 491–502. [Google Scholar] [CrossRef] [Green Version]
- Yehudai, D.; Snir, A.; Peri, R.; Halasz, K.; Haj, T.; Odeh, M.; Kessel, A. B Cell-activating factor enhances interleukin-6 and Interleukin-10 production by ODN-activated human B cells. Scand. J. Immunol. 2012, 76, 371–377. [Google Scholar] [CrossRef] [Green Version]
- Fontaine, J.; Chagnon-Choquet, J.; Valcke, H.S.; Poudrier, J.; Roger, M. Montreal primary HIV infection and long-term non-progressor study groups high expression levels of B lymphocyte stimulator (BLyS) by dendritic cells correlate with HIV-Related B-Cell disease progression in humans. Blood 2011, 117, 145–155. [Google Scholar] [CrossRef]
- Borhis, G.; Burelout, C.; Chaoul, N.; Smith, N.; Goujard, C.; Meyer, L.; Paul, S.; Saoudin, H.; Hosmalin, A.; Gilbert, C.; et al. Plasmacytoid dendritic cells and myeloid cells differently contribute to b-cell-activating factor belonging to the tumor necrosis factor superfamily overexpression during primary HIV infection. AIDS Lond. Engl. 2016, 30, 365–376. [Google Scholar] [CrossRef]
- Borhis, G.; Trovato, M.; Chaoul, N.; Ibrahim, H.M.; Richard, Y. B-Cell-Activating factor and the B-Cell compartment in HIV/SIV infection. Front. Immunol. 2017, 8, 1338. [Google Scholar] [CrossRef] [Green Version]
- Tangye, S.G.; Bryant, V.L.; Cuss, A.K.; Good, K.L. BAFF, APRIL and human B Cell disorders. Semin. Immunol. 2006, 18, 305–317. [Google Scholar] [CrossRef] [PubMed]
- Poudrier, J.; Soulas, C.; Chagnon-Choquet, J.; Burdo, T.; Autissier, P.; Oskar, K.; Williams, K.C.; Roger, M. High expression levels of BLyS/BAFF by blood dendritic cells and granulocytes are associated with B-Cell dysregulation in SIV-infected rhesus macaques. PLoS ONE 2015, 10, e0131513. [Google Scholar] [CrossRef] [PubMed]
- Novak, A.J.; Bram, R.J.; Kay, N.E.; Jelinek, D.F. Aberrant Expression of B-lymphocyte stimulator by b chronic lymphocytic leukemia cells: A mechanism for survival. Blood 2002, 100, 2973–2979. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fu, L.; Lin-Lee, Y.-C.; Pham, L.V.; Tamayo, A.; Yoshimura, L.; Ford, R.J. Constitutive NF-ΚB and NFAT activation leads to stimulation of the BLYS survival pathway in aggressive B-cell lymphomas. Blood 2006, 107, 4540–4548. [Google Scholar] [CrossRef] [Green Version]
- Novak, A.J.; Darce, J.R.; Arendt, B.K.; Harder, B.; Henderson, K.; Kindsvogel, W.; Gross, J.A.; Greipp, P.R.; Jelinek, D.F. Expression of BCMA, TACI, and BAFF-R in multiple myeloma: A mechanism for growth and survival. Blood 2004, 103, 689–694. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elsawa, S.F.; Novak, A.J.; Grote, D.M.; Ziesmer, S.C.; Witzig, T.E.; Kyle, R.A.; Dillon, S.R.; Harder, B.; Gross, J.A.; Ansell, S.M. B-Lymphocyte Stimulator (BLyS) stimulates immunoglobulin production and malignant b-cell growth in waldenström macroglobulinemia. Blood 2006, 107, 2882–2888. [Google Scholar] [CrossRef] [Green Version]
- Chiu, A.; Xu, W.; He, B.; Dillon, S.R.; Gross, J.A.; Sievers, E.; Qiao, X.; Santini, P.; Hyjek, E.; Lee, J.; et al. Hodgkin lymphoma cells express TACI and BCMA receptors and generate survival and proliferation signals in response to BAFF and APRIL. Blood 2006, 109, 729–739. [Google Scholar] [CrossRef] [PubMed]
- Epeldegui, M.; Lee, J.Y.; Martínez, A.C.; Widney, D.P.; Magpantay, L.I.; Regidor, D.; Mitsuyasu, R.; Sparano, J.A.; Ambinder, R.F.; Martínez-Maza, O. Predictive value of cytokines and immune activation biomarkers in AIDS-Related non-Hodgkin lymphoma treated with rituximab plus infusional EPOCH (AMC-034 Trial). Clin. Cancer Res. 2016, 22, 328–336. [Google Scholar] [CrossRef] [Green Version]
- Martínez, L.E.; Lensing, S.Y.; Chang, D.; Magpantay, L.I.; Misuyasu, R.; Ambinder, R.F.; Sparano, J.A.; Martínez-Maza, O.; Epeldegui, M. Immune activation and microbial translocation as prognostic biomarkers for AIDS-related non-Hodgkin lymphoma in the AMC-034 study. Clin. Cancer Res. 2021, 27. [Google Scholar] [CrossRef]
- Treml, L.S.; Quinn, W.J.; Treml, J.F.; Scholz, J.L.; Cancro, M.P. Manipulating B cell homeostasis: A key component in the advancement of targeted strategies. Arch. Immunol. Ther. Exp. 2008, 56, 153–164. [Google Scholar] [CrossRef] [Green Version]
- Zhao, Y.; Uduman, M.; Siu, J.H.Y.; Tull, T.J.; Sanderson, J.D.; Wu, Y.-C.B.; Zhou, J.Q.; Petrov, N.; Ellis, R.; Todd, K.; et al. Spatiotemporal segregation of human marginal zone and memory B cell populations in lymphoid tissue. Nat. Commun. 2018, 9, 3857. [Google Scholar] [CrossRef]
- Weisel, N.M.; Weisel, F.J.; Farber, D.L.; Borghesi, L.A.; Shen, Y.; Ma, W.; Luning Prak, E.T.; Shlomchik, M.J. Comprehensive analyses of B-cell compartments across the human body reveal novel subsets and a gut-resident memory phenotype. Blood 2020, 136, 2774–2785. [Google Scholar] [CrossRef] [PubMed]
- Perez-Andres, M.; Paiva, B.; Nieto, W.G.; Caraux, A.; Schmitz, A.; Almeida, J.; Vogt, R.F.; Marti, G.E.; Rawstron, A.C.; Van Zelm, M.C.; et al. Human peripheral blood B-cell compartments: A crossroad in B-cell traffic. Cytom. B Clin. Cytom. 2010, 78 (Suppl. S1), S47–S60. [Google Scholar] [CrossRef]
- Good, K.L.; Avery, D.T.; Tangye, S.G. Resting human memory B cells are intrinsically programmed for enhanced survival and responsiveness to diverse stimuli compared to naive B cells. J. Immunol. Baltim. 2009, 182, 890–901. [Google Scholar] [CrossRef] [Green Version]
- Klein, U.; Rajewsky, K.; Küppers, R. Human immunoglobulin (Ig)M+IgD+ peripheral blood b cells expressing the cd27 cell surface antigen carry somatically mutated variable region genes: CD27 as a general marker for somatically mutated (memory) B Cells. J. Exp. Med. 1998, 188, 1679–1689. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zubler, R.H. Naive and memory B cells in T-cell-dependent and t-independent responses. Springer Semin. Immunopathol. 2001, 23, 405–419. [Google Scholar] [CrossRef] [PubMed]
- Widney, D.; Gundapp, G.; Said, J.W.; van der Meijden, M.; Bonavida, B.; Demidem, A.; Trevisan, C.; Taylor, J.; Detels, R.; Martínez-Maza, O. Aberrant expression of CD27 and Soluble CD27 (SCD27) in HIV infection and in AIDS-associated lymphoma. Clin. Immunol. 1999, 93, 114–123. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Patients with Pre-Diagnosis Samples (n = 7) | Patients with a 24-Month Immunological Follow-Up (n = 38) | ||
|---|---|---|---|
| Age (years) | |||
| Median | 42 | 43 | |
| IQR | 39–53 | 38–47 | |
| Gender | |||
| M | 7 | 33 | |
| F | 0 | 5 | |
| Lymphoma stage | |||
| I-II | 0 | 8 | |
| III-IV | 7 | 30 | |
| Histology | |||
| Nodular Sclerosis | 1 (14.3) | 3 (7.9) | |
| Mixed Cellularity | 4 (57.1) | 27 (71.1) | |
| Lymphocyte Predominance | 0 (0.0) | 1 (2.6) | |
| Not categorized | 2 (28.6) | 7 (18.4) | |
| Immunological Markers | |||
| IL10 (pg/mL) | |||
| Median | 20.3 | 32.2 | |
| IQR | 17.5–157.1 | 14.5–75.4 | |
| IL6 (pg/mL) | |||
| Median | 60.5 | 27.7 | |
| IQR | 6.8–266.4 | 8.1–60.5 | |
| BAFF (pg/mL) | |||
| Median | 2075.1 | 2024.2 | |
| IQR | 585.1–4381.0 | 913.7–4288.9 | |
| CD4+ T-cells (Cells/μL of blood) | |||
| Median | 465 | 380 | |
| IQR | 127–596 | 144–483 | |
| CD8+ T-cells (Cells/μL of blood) | |||
| Median | 692 | 544 | |
| IQR | 410–1806 | 394–784 | |
| CD19+ B-cells (Cells/μL of blood) | |||
| Median | 161 | 56 | |
| IQR | 26–196 | 16–153 | |
| CD3+CD4+ T-cells (Cells/μL of blood) | |||
| Median | 487 | 267 | |
| IQR | 234–579 | 125–510 | |
| CD3+CD8+ T-cells (Cells/μL of blood) | |||
| Median | 788 | 496 | |
| IQR | 427–1357 | 325–788 | |
| CD56+CD16+ NK-cells (Cells/μL of blood) | |||
| Median | 160 | 127 | |
| IQR | 105–256 | 76–177 |
| Populations | p-Values * | |||
|---|---|---|---|---|
| cHL Patients (n = 14) | Controls (n = 14) | |||
| Age | 0.0006 | |||
| Median | 46 | 51 | ||
| IQR | 41–52 | 44–55 | ||
| Sex | 1 | |||
| M | 12 | 12 | ||
| F | 2 | 2 | ||
| HIV viral Load (copies/mL) | 1 | |||
| ≤200 | 13 | 12 | ||
| >200 | 1 | 2 | ||
| Serum Markers | ||||
| IgG levels (g/L) | 0.31 | |||
| Median | 13.2 | 13.3 | ||
| IQR | 12.1–16.5 | 10.1–15.6 | ||
| n | 14 | 14 | ||
| IgA levels (g/L) | 0.19 | |||
| Median | 3.2 | 2.2 | ||
| IQR | 1.6–4.0 | 1.7–2.6 | ||
| n | 14 | 14 | ||
| IgM levels (g/L) | 0.49 | |||
| Median | 0.8 | 0.6 | ||
| IQR | 0.5–1.1 | 0.4–1.0 | ||
| n | 14 | 14 | ||
| IL10 (pg/mL) | <0.0001 | |||
| Median | 22.4 | 4.5 | ||
| IQR | 11.2–54.4 | 3.9–7.5 | ||
| n | 14 | 14 | ||
| IL6 (pg/mL) | 0.002 | |||
| Median | 23.5 | 2.1 | ||
| IQR | 5.2–128.7 | 0.9–9 | ||
| n | 14 | 14 | ||
| BAFF (pg/mL) | <0.0001 | |||
| Median | 898.9 | 398.8 | ||
| IQR | 720.2–1790.3 | 323.2–445.4 | ||
| n | 14 | 14 | ||
| Lymphocytic subpopulations | ||||
| CD45+ Lymphocytes | 0.63 | |||
| (cells/μL) | Median | 1488 | 1629 | |
| IQR | 966–2570 | 1203–2086 | ||
| n | 14 | 14 | ||
| CD3+CD4+ T-cells | 0.39 | |||
| (cells/μL) | Median | 498.5 | 417.5 | |
| IQR | 328–579 | 386–558 | ||
| n | 14 | 14 | ||
| CD3+CD8+ T-cells | 0.33 | |||
| (cells/μL) | Median | 616.5 | 646.5 | |
| IQR | 415–1208 | 431–741 | ||
| n | 14 | 14 | ||
| CD19+ B-cells | 0.91 | |||
| (cells/μL) | Median | 165 | 170.5 | |
| IQR | 87–210 | 125–222 | ||
| n | 14 | 14 | ||
| %CD27−IgD+ CD19+ naive B-cells | 0.0005 | |||
| Median | 76.2 | 53.1 | ||
| IQR | 64.7–89.1 | 38.3–62.2 | ||
| n | 12 | 12 | ||
| %CD27+IgD+ in CD19+ marginal zone-type B-cells | 0.62 | |||
| Median | 5.5 | 11.5 | ||
| IQR | 4.1–20.5 | 5.6–14.1 | ||
| n | 12 | 12 | ||
| %CD27+IgD− in CD19+ memory B-cells | 0.0005 | |||
| Median | 6.7 | 25.2 | ||
| IQR | 1.8–11.5 | 20.5–32.2 | ||
| n | 12 | 12 | ||
| CD56+CD16+ NK-cells | 0.17 | |||
| (cells/μL) | Median | 143.5 | 247.5 | |
| IQR | 81–258 | 125–406 | ||
| n | 14 | 14 | ||
| Population | p-Value * | |||
|---|---|---|---|---|
| Ann Arbor I-II (n = 18) | Ann Arbor III-IV (n = 26) | |||
| Serum Markers | ||||
| IL10 (pg/mL) | 0.002 | |||
| Median | 11.0 | 31.4 | ||
| IQR | 6.7–26.8 | 16.6–69.1 | ||
| n | 18 | 26 | ||
| IL6 (pg/mL) | 0.03 | |||
| Median | 5.1 | 23.9 | ||
| IQR | 2.7–30.9 | 10.8–60.4 | ||
| n | 18 | 26 | ||
| BAFF (pg/mL) | 0.01 | |||
| Median | 777.1 | 1039.6 | ||
| IQR | 471.1–1180.9 | 913.7–2338.0 | ||
| n | 18 | 26 | ||
| IgG levels (g/L) | 0.11 | |||
| Median | 12.1 | 16.2 | ||
| IQR | 10.75–16.5 | 12.8–18.8 | ||
| n | 16 | 24 | ||
| IgA levels (g/L) | 0.94 | |||
| Median | 3.0 | 2.6 | ||
| IQR | 1.9–3.7 | 1.8–3.7 | ||
| n | 16 | 24 | ||
| IgM levels (g/L) | 0.76 | |||
| Median | 0.8 | 0.7 | ||
| IQR | 0.7–1.0 | 0.4–1.2 | ||
| n | 16 | 24 | ||
| Lymphocytic subpopulations | ||||
| CD3+CD4+ T-cells | 0.50 | |||
| (cells/μL) | Median | 509 | 462 | |
| IQR | 380–581 | 349–623 | ||
| n | 18 | 26 | ||
| CD3+CD8+ T-cells | 0.71 | |||
| (cells/μL) | Median | 614 | 672 | |
| IQR | 514–891 | 394–797 | ||
| n | 18 | 26 | ||
| CD19+ | 0.30 | |||
| (cells/μL) | Median | 137 | 83 | |
| IQR | 49–222 | 42–167 | ||
| n | 16 | 25 | ||
| % CD27−IgD+ naive B-cells | 0.06 | |||
| in CD19+ | Median | 66.0 | 84 | |
| IQR | 48.6–82.2 | 67.1–92.4 | ||
| n | 13 | 21 | ||
| % CD27+IgD+ marginal zone-type | 0.10 | |||
| B-cells in CD19+ | Median | 14.4 | 4.01 | |
| IQR | 3.0–21.1 | 2.3–7.6 | ||
| n | 13 | 21 | ||
| % CD27+IgD− memory | 0.21 | |||
| B-cells in CD19+ | Median | 10.6 | 5.9 | |
| IQR | 6.8–19.9 | 2.1–5.9 | ||
| n | 13 | 21 | ||
| CD56+CD16+ NK-cells | ||||
| (cells/μL) | Median | 151 | 129 | 0.45 |
| IQR | 82–270 | 80–167 | ||
| n | 16 | 25 | ||
| At cHL Diagnosis (n = 38) | At 24 Months (n = 38) | p-Value * | ||
|---|---|---|---|---|
| Serum Markers | ||||
| IL10 (pg/mL) | <0.0001 | |||
| Median | 36.4 | 7.2 | ||
| IQR | 17.5–75.4 | 4.2–13.0 | ||
| n | 37 | 37 | ||
| IL6 (pg/mL) | 0.0002 | |||
| Median | 28.0 | 4.1 | ||
| IQR | 8.1–60.5 | 1.9–14.4 | ||
| n | 37 | 37 | ||
| BAFF (pg/mL) | <0.0001 | |||
| Median | 2043.8 | 527.0 | ||
| IQR | 932.2–4288.9 | 390.8–674.6 | ||
| n | 37 | 37 | ||
| IgG levels (g/L) | <0.0001 | |||
| Median | 14.1 | 11.8 | ||
| IQR | 11.3–18.0 | 10.0–12.9 | ||
| n | 37 | 37 | ||
| IgA levels (g/L) | ||||
| Median | 2.9 | 2.5 | 0.0003 | |
| IQR | 1.6–4.3 | 1.7–3.0 | ||
| n | 37 | 37 | ||
| IgM levels (g/L) | 0.03 | |||
| Median | 0.6 | 0.5 | ||
| IQR | 0.4–1.1 | 0.4–0.8 | ||
| n | 37 | 37 | ||
| Lymphocytic subpopulations | ||||
| CD3+CD4+ T-cells | <0.0001 | |||
| (cells/μL) | Median | 267 | 490 | |
| IQR | 125–510 | 330–681 | ||
| n | 38 | 38 | ||
| CD3+CD8+ T-cells | 0.01 | |||
| (cells/μL) | Median | 496 | 787 | |
| IQR | 325–788 | 575–1027 | ||
| n | 38 | 38 | ||
| CD19+ B-cells | <0.0001 | |||
| (cells/μL) | Median | 56 | 302 | |
| IQR | 16–153 | 247–362 | ||
| n | 38 | 38 | ||
| %CD27−IgD+ in CD19+ naive B-cells | <0.0001 | |||
| Median | 78.4 | 89.6 | ||
| IQR | 66.0–86.7 | 84.9–93.7 | ||
| n | 31 | 31 | ||
| %CD27+IgD+ in CD19+ marginal zone-type B-cells | <0.0001 | |||
| Median | 5.1 | 2.3 | ||
| IQR | 3.0–10.7 | 1.1–3.4 | ||
| n | 31 | 31 | ||
| %CD27+IgD− in CD19+ memory B-cells | 0.01 | |||
| Median | 6.9 | 4.8 | ||
| IQR | 2.4–11.7 | 3.2–8.1 | ||
| n | 31 | 31 | ||
| CD56+CD16+ NK-cells | <0.0001 | |||
| (cells/μL) | Median | 127 | 202 | |
| IQR | 76–177 | 106–302 | ||
| n | 38 | 38 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lievin, R.; Hendel-Chavez, H.; Baldé, A.; Lancar, R.; Algarte-Génin, M.; Krzysiek, R.; Costagliola, D.; Assoumou, L.; Taoufik, Y.; Besson, C. Increased Production of B-Cell Activating Cytokines and Altered Peripheral B-Cell Subset Distribution during HIV-Related Classical Hodgkin Lymphoma. Cancers 2022, 14, 128. https://doi.org/10.3390/cancers14010128
Lievin R, Hendel-Chavez H, Baldé A, Lancar R, Algarte-Génin M, Krzysiek R, Costagliola D, Assoumou L, Taoufik Y, Besson C. Increased Production of B-Cell Activating Cytokines and Altered Peripheral B-Cell Subset Distribution during HIV-Related Classical Hodgkin Lymphoma. Cancers. 2022; 14(1):128. https://doi.org/10.3390/cancers14010128
Chicago/Turabian StyleLievin, Raphael, Houria Hendel-Chavez, Aliou Baldé, Rémi Lancar, Michèle Algarte-Génin, Roman Krzysiek, Dominique Costagliola, Lambert Assoumou, Yassine Taoufik, and Caroline Besson. 2022. "Increased Production of B-Cell Activating Cytokines and Altered Peripheral B-Cell Subset Distribution during HIV-Related Classical Hodgkin Lymphoma" Cancers 14, no. 1: 128. https://doi.org/10.3390/cancers14010128
APA StyleLievin, R., Hendel-Chavez, H., Baldé, A., Lancar, R., Algarte-Génin, M., Krzysiek, R., Costagliola, D., Assoumou, L., Taoufik, Y., & Besson, C. (2022). Increased Production of B-Cell Activating Cytokines and Altered Peripheral B-Cell Subset Distribution during HIV-Related Classical Hodgkin Lymphoma. Cancers, 14(1), 128. https://doi.org/10.3390/cancers14010128