
Monocarboxylate Transporters 1 and 4 and Prognosis in Small Bowel Neuroendocrine Tumors

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Data Collection
2.2. Immunohistochemical Staining
2.3. Immunostaining Assessment
2.4. Statistical Analysis
3. Results
3.1. Patients
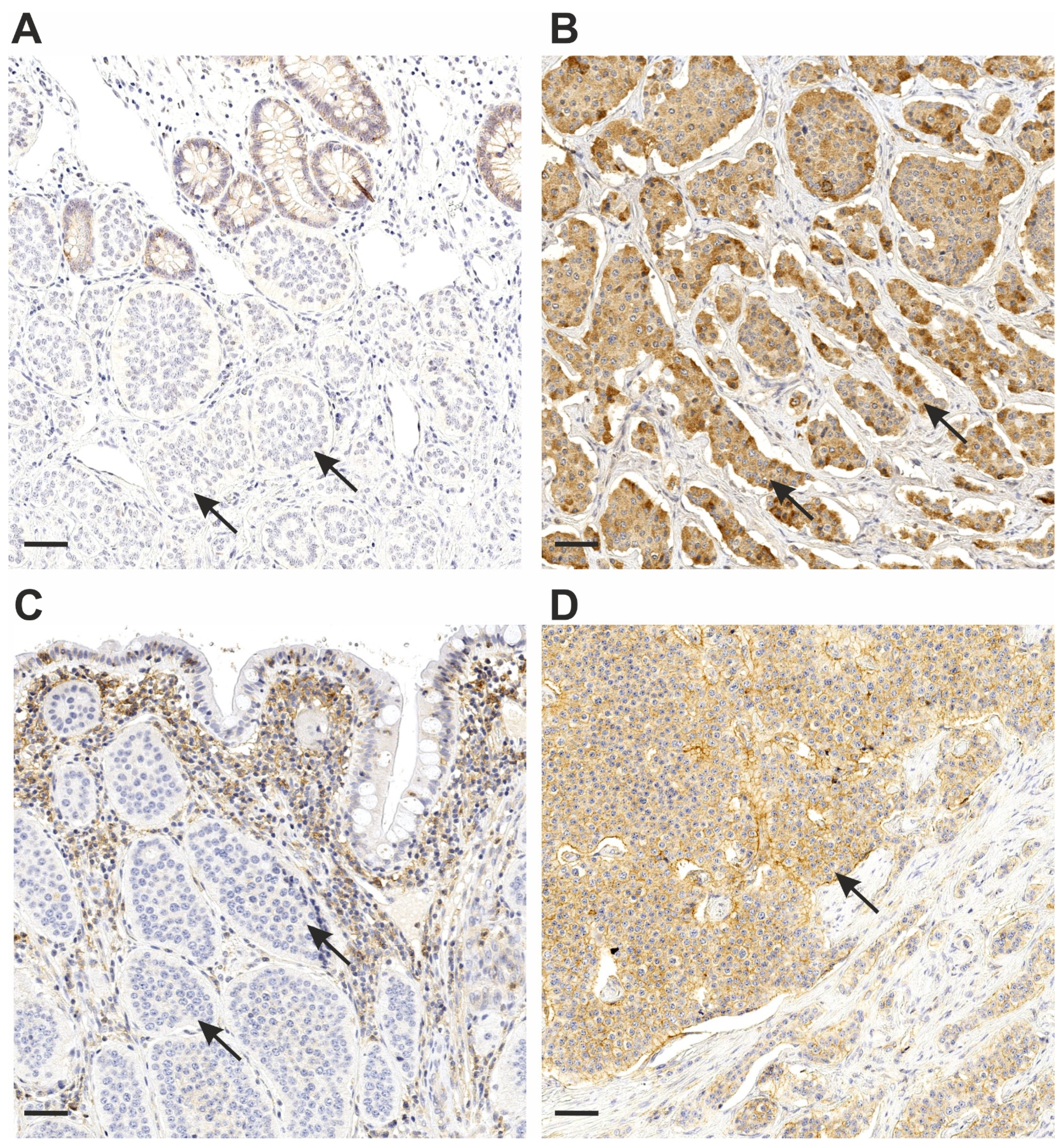
3.2. MCT1 and MCT4 Staining
3.3. MCT1 and MCT4 Association with Clinicopathological Variables
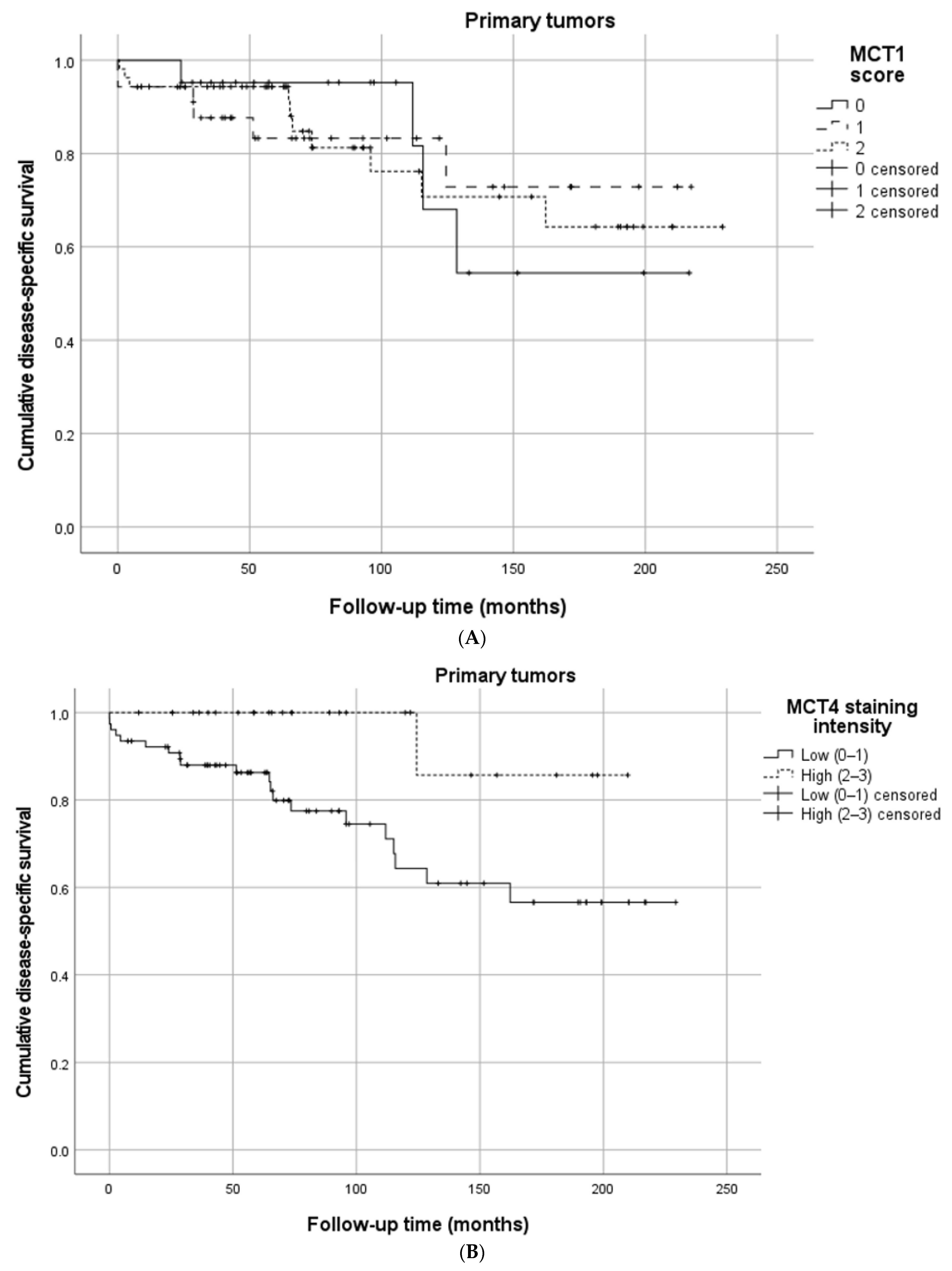
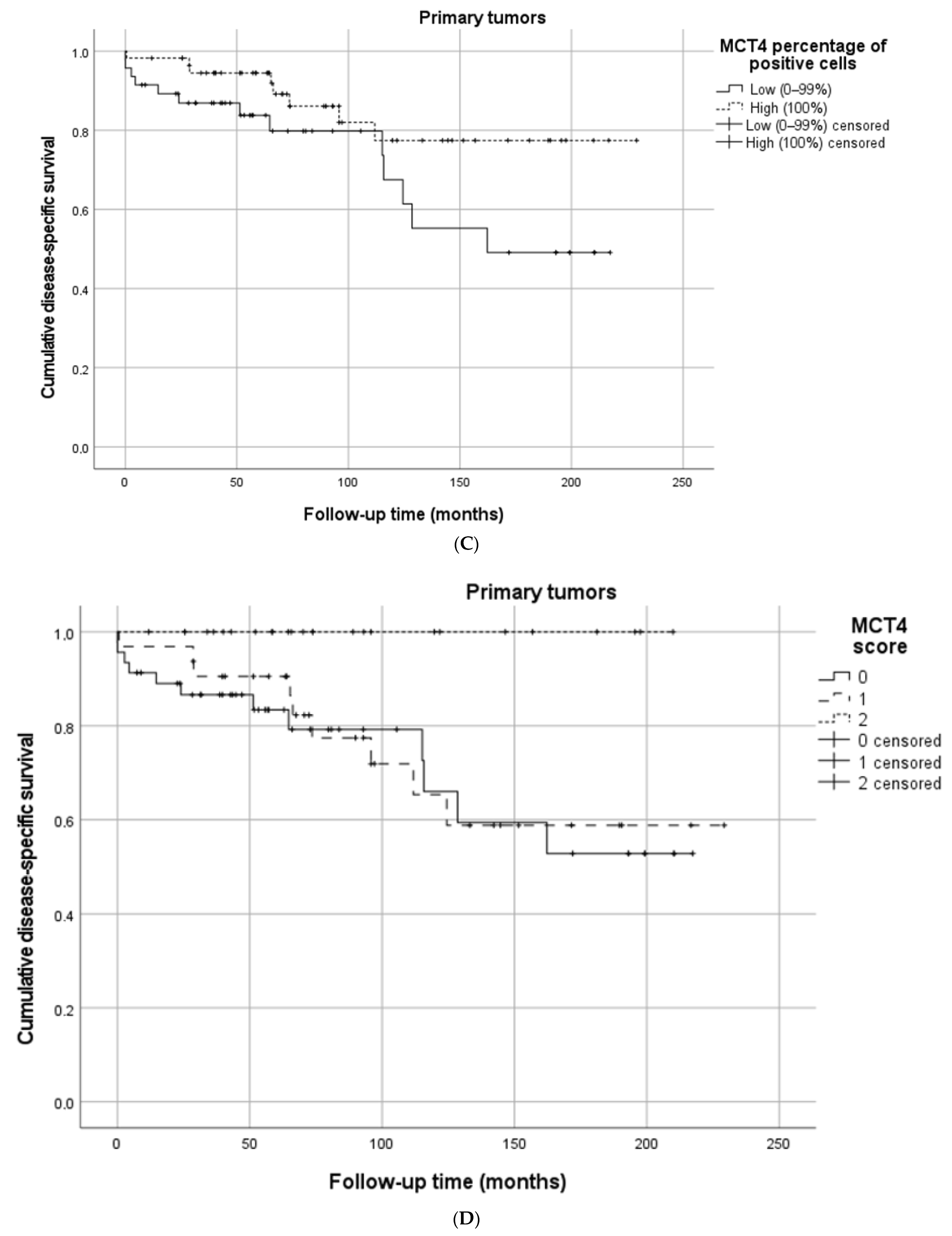
3.4. MCT1, MCT4, and Survival
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fernandez, C.J.; Agarwal, M.; Pottakkat, B.; Haroon, N.N.; George, A.S.; Pappachan, J.M. Gastroenteropancreatic neuroendocrine neoplasms: A clinical snapshot. World J. Gastrointest. Surg. 2021, 13, 231–255. [Google Scholar] [CrossRef] [PubMed]
- Yao, J.C.; Hassan, M.; Phan, A.; Dagohoy, C.; Leary, C.; Mares, J.E.; Abdalla, E.K.; Fleming, J.B.; Vauthey, J.N.; Rashid, A.; et al. One hundred years after “carcinoid”: Epidemiology of and prognostic factors for neuroendocrine tumors in 35,825 cases in the United States. J. Clin. Oncol. 2008, 26, 3063–3072. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dasari, A.; Shen, C.; Halperin, D.; Zhao, B.; Zhou, S.; Xu, Y.; Shih, T.; Yao, J.C. Trends in the incidence, prevalence, and survival outcomes in patients with neuroendocrine tumors in the United States. JAMA Oncol. 2017, 3, 1335–1342. [Google Scholar] [CrossRef] [PubMed]
- Van Der Zwan, J.M.; Trama, A.; Otter, R.; Larrañaga, N.; Tavilla, A.; Marcos-Gragera, R.; Dei Tos, A.P.; Baudin, E.; Poston, G.; Links, T.; et al. Rare neuroendocrine tumours: Results of the surveillance of rare cancers in Europe project. Eur. J. Cancer 2013, 49, 2565–2578. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.Y.; Lee, I.; Chang, W.J.; Ahn, S.M.; Lim, S.H.; Kim, H.S.; Yoo, K.H.; Jung, K.S.; Song, H.-N.; Cho, J.H.; et al. MCT4 as a potential therapeutic target for metastatic gastric cancer with peritoneal carcinomatosis. Oncotarget 2016, 7, 43492–43503. [Google Scholar] [CrossRef] [Green Version]
- Huhta, H.; Helminen, O.; Palomäki, S.; Kauppila, J.H.; Saarnio, J.; Lehenkari, P.P.; Karttunen, T.J. Intratumoral lactate metabolism in Barrett’s esophagus and adenocarcinoma. Oncotarget 2017, 8, 22894–22902. [Google Scholar] [CrossRef] [Green Version]
- Halestrap, A.P. The SLC16 gene family—Structure, role and regulation in health and disease. Mol. Aspects Med. 2013, 34, 337–349. [Google Scholar] [CrossRef]
- Halestrap, A.P. The monocarboxylate transporter family—Structure and functional characterization. IUBMB Life 2012, 64, 1–9. [Google Scholar] [CrossRef]
- Wang, C.; Wen, Z.; Xie, J.; Zhao, Y.; Zhao, L.; Zhang, S.; Liu, Y.; Xue, Y.; Shi, M. MACC1 mediates chemotherapy sensitivity of 5-FU and cisplatin via regulating MCT1 expression in gastric cancer. Biochem. Biophys. Res. Commun. 2017, 485, 665–671. [Google Scholar] [CrossRef]
- Puri, S.; Juvale, K. Monocarboxylate transporter 1 and 4 inhibitors as potential therapeutics for treating solid tumours: A review with structure-activity relationship insights. Eur. J. Med. Chem. 2020, 199, 112393. [Google Scholar] [CrossRef]
- Payen, V.L.; Mina, E.; Van Hée, V.F.; Porporato, P.E.; Sonveaux, P. Monocarboxylate transporters in cancer. Mol. Metab. 2020, 33, 48. [Google Scholar] [CrossRef] [PubMed]
- Eskuri, M.; Kemi, N.; Kauppila, J.H. Monocarboxylate Transporters 1 and 4 and MTCO1 in Gastric Cancer. Cancers 2021, 13, 2142. [Google Scholar] [CrossRef] [PubMed]
- Izumi, H.; Takahashi, M.; Uramoto, H.; Nakayama, Y.; Oyama, T.; Wang, K.Y.; Sasaguri, Y.; Nishizawa, S.; Kohno, K. Monocarboxylate transporters 1 and 4 are involved in the invasion activity of human lung cancer cells. Cancer Sci. 2011, 102, 1007–1013. [Google Scholar] [CrossRef] [PubMed]
- Abe, Y.; Nakayama, Y.; Katsuki, T.; Inoue, Y.; Minagawa, N.; Torigoe, T.; Higure, A.; Sako, T.; Nagata, N.; Hirata, K. The prognostic significance of the expression of monocarboxylate transporter 4 in patients with right- or left-sided colorectal cancer. Asia Pac. J. Clin. Oncol. 2019, 15, e49–e55. [Google Scholar] [CrossRef]
- Allen, E.; Miéville, P.; Warren, C.M.; Saghafinia, S.; Li, L.; Peng, M.W.; Hanahan, D. Metabolic Symbiosis Enables Adaptive Resistance to Anti-angiogenic Therapy that Is Dependent on mTOR Signaling. Cell Rep. 2016, 15, 1144. [Google Scholar] [CrossRef] [Green Version]
- Hiltunen, N.; Väyrynen, J.P.; Böhm, J.; Helminen, O. CD3+, CD8+, CD4+ and FOXP3+ T Cells in the Immune Microenvironment of Small Bowel Neuroendocrine Tumors. Diseases 2021, 9, 42. [Google Scholar] [CrossRef]
- Amin, M.B.; Edge, S.; Greene, F.; Byrd, D.R.; Brookland, R.K.; Washington, M.K.; Gershenwald, J.E.; Compton, C.C.; Hess, K.R.; Sullivan, D.C.; et al. AJCC Cancer Staging Manual, 8th ed.; Springer: New York, NY, USA, 2017. [Google Scholar]
- Nagtegaal, I.D.; Odze, R.D.; Klimstra, D.; Paradis, V.; Rugge, M.; Schirmacher, P.; Washington, K.M.; Carneiro, F.; Cree, I.A. The 2019 WHO classification of tumours of the digestive system. Histopathology 2020, 76, 182–188. [Google Scholar] [CrossRef] [Green Version]
- Andersen, S.; Solstad, Ø.; Donnem, T.; Eilertsen, M.; Nordby, Y.; Ness, N.; Richardsen, E.; Busund, L.-T.; Bremnes, R.M. Organized metabolic crime in prostate cancer: The coexpression of MCT1 in tumor and MCT4 in stroma is an independent prognosticator for biochemical failure. Urol. Oncol. Semin. Orig. Investig. 2015, 33, 338.e9–338.e17. [Google Scholar] [CrossRef]
- Pavel, M.; Öberg, K.; Falconi, M.; Krenning, E.P.; Sundin, A.; Perren, A.; Berruti, A. Gastroenteropancreatic neuroendocrine neoplasms: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2020, 31, 844–860. [Google Scholar] [CrossRef]
- Modlin, I.M.; Gustafsson, B.I.; Pavel, M.; Svejda, B.; Lawrence, B.; Kidd, M. A Nomogram to Assess Small-Intestinal Neuroendocrine Tumor (‘Carcinoid’) Survival. Neuroendocrinology 2010, 92, 143–157. [Google Scholar] [CrossRef]
- Kelly, S.; Aalberg, J.; Agathis, A.; Phillips, K.; Haile, S.; Haines, K.; Kang Kim, M.; Divino, C.M. Predicting Survival of Small Intestine Neuroendocrine Tumors: Experience from a Major Referral Center. Pancreas 2019, 48, 514–518. [Google Scholar] [CrossRef] [PubMed]
- Clift, A.K.; Faiz, O.; Goldin, R.; Martin, J.; Wasan, H.; Liedke, M.-O.; Schloericke, E.; Malczewska, A.; Rindi, G.; Kidd, M.; et al. Predicting the survival of patients with small bowel neuroendocrine tumours: Comparison of 3 systems. Endocr. Connect. 2017, 6, 71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levy, S.; van Veenendaal, L.M.; Korse, C.M.; Breekveldt, E.C.H.; Verbeek, W.H.M.; Vriens, M.R.; Kuhlmann, K.F.D.; van den Berg, J.G.; Valk, G.D.; Tesselaar, M.E.T. Survival in Patients with Neuroendocrine Tumours of the Small Intestine: Nomogram Validation and Predictors of Survival. J. Clin. Med. 2020, 9, 2502. [Google Scholar] [CrossRef] [PubMed]
- Junttila, A.; Helminen, O.; Mrena, J.; Sihvo, E. Exercise capacity in the stair-climbing test predicts outcomes of operable esophageal cancer in minimally invasive era. Eur. J. Surg. Oncol. 2022, 48, 589–596. [Google Scholar] [CrossRef] [PubMed]
- Gatenby, R.A.; Gillies, R.J. Why do cancers have high aerobic glycolysis? Nat. Rev. Cancer 2004, 4, 891–899. [Google Scholar] [CrossRef]
- Swietach, P. What is pH regulation, and why do cancer cells need it? Cancer Metastasis Rev. 2019, 38, 5–15. [Google Scholar] [CrossRef] [Green Version]
- Warburg, O. On the origin of cancer cells. Science 1956, 123, 309–314. [Google Scholar] [CrossRef]
- Liberti, M.V.; Locasale, J.W. The Warburg Effect: How Does it Benefit Cancer Cells? Trends Biochem. Sci. 2016, 41, 211. [Google Scholar] [CrossRef] [Green Version]
- Pinheiro, C.; Albergaria, A.; Paredes, J.; Sousa, B.; Dufloth, R.; Vieira, D.; Schmitt, F.; Baltazar, F. Monocarboxylate transporter 1 is up-regulated in basal-like breast carcinoma. Histopathology 2010, 56, 860–867. [Google Scholar] [CrossRef]
- Koukourakis, M.I.; Giatromanolaki, A.; Bougioukas, G.; Sivridis, E. Lung cancer: An organized cellular and metabolic domain A Comparative Study of Metabolism Related Protein Expression in Cancer Cells and Tumor Associated Stroma. Cancer Biol. Ther. 2007, 6, 1476–1479. [Google Scholar] [CrossRef]
- Pinheiro, C.; Longatto-Filho, A.; Scapulatempo, C.; Ferreira, L.; Martins, S.; Pellerin, L.; Rodrigues, M.; Alves, V.A.F.; Schmitt, F.; Baltazar, F. Increased expression of monocarboxylate transporters 1, 2, and 4 in colorectal carcinomas. Virchows Arch. 2008, 452, 139–146. [Google Scholar] [CrossRef] [PubMed]
- Pértega-Gomes, N.; Vizcaíno, J.R.; Miranda-Gonçalves, V.; Pinheiro, C.; Silva, J.; Pereira, H.; Monteiro, P.; Henrique, R.M.; Reis, R.M.; Lopes, C.; et al. Monocarboxylate transporter 4 (MCT4) and CD147 overexpression is associated with poor prognosis in prostate cancer. BMC Cancer 2011, 11, 312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pavlides, S.; Whitaker-Menezes, D.; Castello-Cros, R.; Flomenberg, N.; Witkiewicz, A.K.; Frank, P.G.; Casimiro, M.C.; Wang, C.; Fortina, P.; Addya, S.; et al. Cell Cycle the reverse Warburg effect: Aerobic glycolysis in cancer associated fibroblasts and the tumor stroma. Cell Cycle 2009, 8, 3984–4001. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sonveaux, P.; Végran, F.; Schroeder, T.; Wergin, M.C.; Verrax, J.; Rabbani, Z.N.; De Saedeleer, C.J.; Kennedy, K.M.; Diepart, C.; Jordan, B.F.; et al. Targeting lactate-fueled respiration selectively kills hypoxic tumor cells in mice. J. Clin. Investig. 2008, 118, 3930–3942. [Google Scholar] [CrossRef] [Green Version]
- Végran, F.; Boidot, R.; Michiels, C.; Sonveaux, P.; Feron, O. Lactate influx through the endothelial cell monocarboxylate transporter MCT1 supports an NF-kB/IL-8 pathway that drives tumor angiogenesis. Cancer Res. 2011, 71, 2550–2560. [Google Scholar] [CrossRef] [Green Version]
- Sonveaux, P.; Copetti, T.; de Saedeleer, C.J.; Végran, F.; Verrax, J.; Kennedy, K.M.; Moon, E.J.; Dhup, S.; Danhier, P.; Frérart, F.; et al. Targeting the lactate transporter MCT1 in endothelial cells inhibits lactate-induced HIF-1 activation and tumor angiogenesis. PLoS ONE 2012, 7, e33418. [Google Scholar] [CrossRef]
- Doherty, J.R.; Cleveland, J.L. Targeting lactate metabolism for cancer therapeutics. J. Clin. Investig. 2013, 123, 3685. [Google Scholar] [CrossRef]
- Couvelard, A.; O’toole, D.; Turley, H.; Leek, R.; Sauvanet, A.; Degott, C.; Ruszniewski, P.; Belghiti, J.; Harris, A.L.; Gatter, K.; et al. Microvascular density and hypoxia-inducible factor pathway in pancreatic endocrine tumours: Negative correlation of microvascular density and VEGF expression with tumour progression. Br. J. Cancer 2005, 92, 94–101. [Google Scholar] [CrossRef]
- Terris, B.; Scoazec, J.Y.; Rubbia, L.; Bregeaud, L.; Pepper, M.S.; Ruszniewski, P.; Belghiti, J.; Fléjou, J.F.; Degott, C. Expression of vascular endothelial growth factor in digestive neuroendocrine tumours. Histopathology 1998, 32, 133–138. [Google Scholar] [CrossRef]
- Haugen, M.; Dammen, R.; Svejda, B.; Gustafsson, B.I.; Pfragner, R.; Modlin, I.; Kidd, M. Differential signal pathway activation and 5-HT function: The role of gut enterochromaffin cells as oxygen sensors. Am. J. Physiol.-Gastrointest. Liver Physiol. 2012, 303, G1164–G1173. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | MCT1 Score 0, n = 21 | MCT1 Score 1, n = 35 | MCT1 Score 2, n = 53 | P between Groups |
|---|---|---|---|---|
| Sex | ||||
| Male, n (%) | 12 (57.1) | 21 (60.0) | 27 (50.9) | 0.689 |
| Age, median (IQR) years | 61 (56–69) | 66 (56–73) | 66 (56–73) | 0.866 |
| T-Class | 0.109 | |||
| T1–2, n (%) | 3 (14.3) | 9 (25.7) | 15 (28.3) | |
| T3, n (%) | 13 (61.9) | 17 (48.6) | 16 (30.2) | |
| T4, n (%) | 5 (23.8) | 9 (25.7) | 22 (41.5) | |
| N-Class | 0.530 | |||
| N0, n (%) | 3 (14.3) | 5 (14.3) | 12 (22.6) | |
| N1–2, n (%) | 18 (85.7) | 30 (85.7) | 41 (77.4) | |
| M-Class | 0.860 | |||
| M0, n (%) | 13 (61.9) | 24 (68.6) | 34 (64.2) | |
| M1, n (%) | 8 (38.1) | 11 (31.4) | 19 (35.8) | |
| Stage | 0.950 | |||
| I-II, n (%) | 2 (9.5) | 5 (14.3) | 5 (9.4) | |
| III, n (%) | 11 (52.4) | 19 (54.3) | 29 (54.7) | |
| IV, n (%) | 8 (38.1) | 11 (31.4) | 19 (35.8) | |
| Grade | ||||
| 1, n (%) | 17 (81.0) | 28 (80.0) | 40 (75.5) | 0.825 |
| 2, n (%) | 4 (19.0) | 7 (20.0) | 13 (24.5) | |
| Tumor location | 0.033 | |||
| Ileum, n (%) | 18 (85.7) | 32 (91.4) | 53 (100) | |
| Jejunum, n (%) | 3 (14.3) | 3 (8.6) | 0 | |
| Somatostatin analogue treatment | 0.391 | |||
| Yes, n (%) | 12 (57.1) | 16 (45.7) | 32 (60.4) | |
| Chemotherapy | 0.818 | |||
| No, n (%) | 16 (76.2) | 28 (80.0) | 45 (84.9) | |
| Preoperative, n (%) | 1 (4.8) | 2 (5.7) | 2 (3.8) | |
| Postoperative, n (%) | 4 (19.0) | 4 (11.4) | 4 (7.5) | |
| Multiple primary tumors | 0.403 | |||
| Yes, n (%) | 8 (40.0) | 8 (22.9) | 15 (28.8) | |
| P-CgA | ||||
| ≥3 nmol/L, n (%) | 16 (88.9) | 24 (85.7) | 43 (87.8) | 0.945 |
| Median (IQR) nmol/L | 8.5 (4.7–15.0) | 6.4 (3.6–13.5) | 4.8 (3.4–15.0) | 0.587 |
| dU-5-HIAA | ||||
| ≥42 µmol/L, n (%) | 10 (66.7) | 18 (69.2) | 21 (48.8) | 0.193 |
| Median (IQR) µmol/L | 56 (37–199) | 96 (27–149) | 40 (25–169) | 0.632 |
| Variables | MCT4 Score 0, n = 46 | MCT4 Score 1, n = 32 | MCT4 Score 2, n = 26 | P between Groups |
|---|---|---|---|---|
| Sex | ||||
| Male, n (%) | 28 (60.9) | 14 (43.8) | 14 (53.8) | 0.329 |
| Age, median (IQR) years | 62 (56–72) | 69 (56–75) | 65 (47–70) | 0.258 |
| T-Class | 0.713 | |||
| T1–2, n (%) | 11 (23.9) | 7 (21.9) | 9 (34.6) | |
| T3, n (%) | 19 (41.3) | 16 (50.0) | 9 (34.6) | |
| T4, n (%) | 16 (34.8) | 9 (28.1) | 8 (30.8) | |
| N-Class | 0.308 | |||
| N0, n (%) | 10 (21.7) | 6 (18.8) | 2 (7.7) | |
| N1–2, n (%) | 36 (78.3) | 26 (81.3) | 24 (92.3) | |
| M-Class | 0.948 | |||
| M0, n (%) | 29 (63.0) | 19 (59.4) | 16 (61.5) | |
| M1, n (%) | 17 (37.0) | 13 (40.6) | 10 (38.5) | |
| Stage | 0.959 | |||
| I–II, n (%) | 6 (13.0) | 3 (9.4) | 2 (7.7) | |
| III, n (%) | 23 (50.0) | 16 (50.0) | 14 (53.8) | |
| IV, n (%) | 17 (37.0) | 13 (40.6) | 10 (38.5) | |
| Grade | ||||
| 1, n (%) | 35 (76.1) | 27 (84.4) | 18 (69.2) | 0.389 |
| 2, n (%) | 11 (23.9) | 5 (15.6) | 8 (30.8) | |
| Tumor location | 0.203 | |||
| Ileum, n (%) | 42 (91.3) | 32 (100) | 25 (96.2) | |
| Jejunum, n (%) | 4 (8.7) | 0 | 1 (3.8) | |
| Somatostatin analogue treatment | ||||
| Yes, n (%) | 24 (52.2) | 20 (62.5) | 16 (61.5) | 0.596 |
| Chemotherapy | 0.669 | |||
| No, n (%) | 35 (76.1) | 27 (84.4) | 24 (92.3) | |
| Preoperative, n (%) | 3 (6.5) | 1 (3.1) | 0 | |
| Postoperative, n (%) | 6 (13.0) | 3 (9.4) | 2 (7.7) | |
| Multiple primary tumors | ||||
| Yes, n (%) | 15 (33.3) | 1 (35.5) | 4 (15.4) | 0.187 |
| P-CgA | ||||
| ≥3 nmol/L, n (%) | 34 (91.9) | 25 (86.2) | 21 (84.0) | 0.609 |
| Median (IQR) nmol/L | 7.6 (4.1–39.5) | 5.0 (3.4–10.2) | 5.5 (3.3–12.0) | 0.209 |
| dU-5-HIAA | ||||
| ≥42 µmol/L, n (%) | 19 (59.4) | 15 (55.6) | 15 (68.2) | 0.658 |
| Median (IQR) µmol/L | 74 (32–266) | 44 (24–104) | 58 (27–222) | 0.258 |
| Disease-Specific Survival | No. of Patients | MCT1 Intensity, Low | MCT1 Intensity, High | p | |
|---|---|---|---|---|---|
| Primary tumors | 109 | 66.7% | 64.0% | 0.825 | |
| No. of patients | MCT1 percentage, low | MCT1 percentage, high | p | ||
| Primary tumors | 109 | 51.8% | 68.0% | 0.841 | |
| No. of patients | MCT1 score 0 | MCT1 score 1 | MCT1 score 2 | p | |
| Primary tumors | 109 | 54.4% | 72.9% | 64.3% | 0.999 |
| No. of patients | MCT4 intensity, low | MCT4 intensity, high | p | ||
| Primary tumors | 104 | 56.6% | 85.7% | 0.020 | |
| Lymph node metastases | 61 | 62.6% | 73.6% | 0.345 | |
| No. of patients | MCT4 percentage, low | MCT4 percentage, high | p | ||
| Primary tumors | 104 | 49.1% | 77.4% | 0.058 | |
| Lymph node metastases | 61 | 71.1% | 65.1% | 0.856 | |
| No. of patients | MCT4 stroma, negative | MCT4 stroma, positive | p | ||
| Primary tumors | 104 | 65.7% | 51.9% | 0.469 | |
| Lymph node metastases | 61 | 65.7% | 75.6% | 0.659 | |
| No. of patients | MCT4 score 0 | MCT4 score 1 | MCT4 score 2 | p | |
| Primary tumors | 104 | 52.8% | 58.8% | 100% | 0.025 |
| Lymph node metastases | 61 | 70.0% | 56.5% | 73.4% | 0.678 |
| MCT4 Intensity | ||||
| Primary tumors | No. of patients | Low HR (95%CI) | High HR (95%CI) | |
| Crude | 104 | 1.00 (reference) | 0.13 (0.02–0.99) | |
| Adjusted | 104 | 1.00 (reference) | 0.19 (0.03–1.48) | |
| MCT4 percentage | ||||
| Primary tumors | No. of patients | Low, HR (95%CI) | High, HR (95%CI) | |
| Crude | 104 | 1.00 (reference) | 0.44 (0.18–1.05) | |
| Adjusted | 104 | 1.00 (reference) | 0.23 (0.09–0.61) | |
| MCT4 score | ||||
| Primary tumors | No. of patients | Score 0, HR (95%CI) | Score 1, HR (95%CI) | Score 2, HR (95%CI) |
| Crude | 104 | 1.00 (reference) | 0.87 (0.36–2.06) | 0.00 (0.00–0.00) |
| Adjusted | 104 | 1.00 (reference) | 0.41 (0.16–1.10) | 0.00 (0.00–0.00) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hiltunen, N.; Rintala, J.; Väyrynen, J.P.; Böhm, J.; Karttunen, T.J.; Huhta, H.; Helminen, O. Monocarboxylate Transporters 1 and 4 and Prognosis in Small Bowel Neuroendocrine Tumors. Cancers 2022, 14, 2552. https://doi.org/10.3390/cancers14102552
Hiltunen N, Rintala J, Väyrynen JP, Böhm J, Karttunen TJ, Huhta H, Helminen O. Monocarboxylate Transporters 1 and 4 and Prognosis in Small Bowel Neuroendocrine Tumors. Cancers. 2022; 14(10):2552. https://doi.org/10.3390/cancers14102552
Chicago/Turabian StyleHiltunen, Niko, Jukka Rintala, Juha P. Väyrynen, Jan Böhm, Tuomo J. Karttunen, Heikki Huhta, and Olli Helminen. 2022. "Monocarboxylate Transporters 1 and 4 and Prognosis in Small Bowel Neuroendocrine Tumors" Cancers 14, no. 10: 2552. https://doi.org/10.3390/cancers14102552
APA StyleHiltunen, N., Rintala, J., Väyrynen, J. P., Böhm, J., Karttunen, T. J., Huhta, H., & Helminen, O. (2022). Monocarboxylate Transporters 1 and 4 and Prognosis in Small Bowel Neuroendocrine Tumors. Cancers, 14(10), 2552. https://doi.org/10.3390/cancers14102552