Use of Thiazide Diuretics and Risk of All Types of Skin Cancers: An Updated Systematic Review and Meta-Analysis

 , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Systematic Literature Search
2.2. Study Selection Criteria and Outcomes
2.3. Study Selection, Data Collection, and Risk of Bias Evaluation
2.4. Approach to Evidence Synthesis
2.5. Subgroup and Sensitivity Analyses
2.6. Judging the Strength of Evidence
3. Results
3.1. Evidence Identified from the Search
3.2. Overview of Study Characteristics
3.3. Finding from Meta-Analysis
3.4. Subgroup and Sensitivity Analyses
3.5. Evidence Certainty
4. Discussion
4.1. Strengths and Limitations
4.2. Implications for Practice and Future Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wang, Y.R.; Alexander, G.C.; Stafford, R.S. Outpatient hypertension treatment, treatment intensification, and control in Western Europe and the United States. Arch. Intern. Med. 2007, 167, 141–147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McNally, R.J.; Morselli, F.; Farukh, B.; Chowienczyk, P.J.; Faconti, L. A review of the prescribing trend of thiazide-type and thiazide-like diuretics in hypertension: A UK perspective. Br. J. Clin. Pharm. 2019, 85, 2707–2713. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E., Jr.; Collins, K.J.; Dennison Himmelfarb, C.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2018, 71, e127–e248. [Google Scholar] [CrossRef] [PubMed]
- Copland, E.; Canoy, D.; Nazarzadeh, M.; Bidel, Z.; Ramakrishnan, R.; Woodward, M.; Chalmers, J.; Teo, K.K.; Pepine, C.J.; Davis, B.R.; et al. Anti-hypertensive treatment and risk of cancer: An individual participant data meta-analysis. Lancet Oncol. 2021, 22, 558–570. [Google Scholar] [CrossRef]
- Guy, G.P., Jr.; Machlin, S.R.; Ekwueme, D.U.; Yabroff, K.R. Prevalence and costs of skin cancer treatment in the U.S., 2002-2006 and 2007-2011. Am. J. Prev. Med. 2015, 48, 183–187. [Google Scholar] [CrossRef] [Green Version]
- Kreutz, R.; Algharably, E.A.H.; Douros, A. Reviewing the effects of thiazide and thiazide-like diuretics as photosensitizing drugs on the risk of skin cancer. J. Hypertens 2019, 37, 1950–1958. [Google Scholar] [CrossRef]
- U.S. Food and Drug Administration. FDA approves label changes to hydrochlorothiazide to describe small risk of non-melanoma skin cancer. Available online: https://www.fda.gov/drugs/drug-safety-and-availability/fda-approves-label-changes-hydrochlorothiazide-describe-small-risk-non-melanoma-skin-cancer (accessed on 8 January 2022).
- Gandini, S.; Palli, D.; Spadola, G.; Bendinelli, B.; Cocorocchio, E.; Stanganelli, I.; Miligi, L.; Masala, G.; Caini, S. Anti-hypertensive drugs and skin cancer risk: A review of the literature and meta-analysis. Crit. Rev. Oncol. Hematol. 2018, 122, 1–9. [Google Scholar] [CrossRef]
- Tang, H.; Fu, S.; Zhai, S.; Song, Y.; Asgari, M.M.; Han, J. Use of anti-hypertensive drugs and risk of keratinocyte carcinoma: A meta-analysis of observational studies. Pharm. Drug Saf. 2018, 27, 279–288. [Google Scholar] [CrossRef]
- Tang, H.; Fu, S.; Zhai, S.; Song, Y.; Han, J. Use of Antihypertensive Drugs and Risk of Malignant Melanoma: A Meta-analysis of Observational Studies. Drug Saf. 2018, 41, 161–169. [Google Scholar] [CrossRef]
- Bendinelli, B.; Masala, G.; Garamella, G.; Palli, D.; Caini, S. Do Thiazide Diuretics Increase the Risk of Skin Cancer? A Critical Review of the Scientific Evidence and Updated Meta-Analysis. Curr. Cardiol. Rep. 2019, 21, 92. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of observational studies in epidemiology: A proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wells, G.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 8 January 2022).
- Nochaiwong, S.; Ruengorn, C.; Awiphan, R.; Koyratkoson, K.; Chaisai, C.; Noppakun, K.; Chongruksut, W.; Thavorn, K. The association between proton pump inhibitor use and the risk of adverse kidney outcomes: A systematic review and meta-analysis. Nephrol. Dial. Transpl. 2018, 33, 331–342. [Google Scholar] [CrossRef] [Green Version]
- Nochaiwong, S.; Ruengorn, C.; Awiphan, R.; Chai-Adisaksopha, C.; Tantraworasin, A.; Phosuya, C.; Kanjanarat, P.; Chongruksut, W.; Sood, M.M.; Thavorn, K. Use of serotonin reuptake inhibitor antidepressants and the risk of bleeding complications in patients on anticoagulant or antiplatelet agents: A systematic review and meta-analysis. Ann. Med. 2022, 54, 80–97. [Google Scholar] [CrossRef]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Riley, R.D.; Higgins, J.P.; Deeks, J.J. Interpretation of random effects meta-analyses. BMJ 2011, 342, d549. [Google Scholar] [CrossRef] [Green Version]
- VanderWeele, T.J.; Ding, P. Sensitivity Analysis in Observational Research: Introducing the E-Value. Ann. Intern. Med. 2017, 167, 268–274. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Borenstein, M.; Higgins, J.P.; Hedges, L.V.; Rothstein, H.R. Basics of meta-analysis: I(2) is not an absolute measure of heterogeneity. Res. Synth. Methods 2017, 8, 5–18. [Google Scholar] [CrossRef] [Green Version]
- Begg, C.B.; Mazumdar, M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994, 50, 1088–1101. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [Green Version]
- Duval, S.; Tweedie, R. Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Balshem, H.; Helfand, M.; Schünemann, H.J.; Oxman, A.D.; Kunz, R.; Brozek, J.; Vist, G.E.; Falck-Ytter, Y.; Meerpohl, J.; Norris, S.; et al. GRADE guidelines: 3. Rating the quality of evidence. J. Clin. Epidemiol. 2011, 64, 401–406. [Google Scholar] [CrossRef] [PubMed]
- Berkman, N.D.; Lohr, K.N.; Ansari, M.T.; Balk, E.M.; Kane, R.; McDonagh, M.; Morton, S.C.; Viswanathan, M.; Bass, E.B.; Butler, M.; et al. Grading the strength of a body of evidence when assessing health care interventions: An EPC update. J. Clin. Epidemiol. 2015, 68, 1312–1324. [Google Scholar] [CrossRef]
- Chen, H.; Cohen, P.; Chen, S. How big is a big odds ratio? Interpreting the magnitudes of odds ratios in epidemiological studies. Commun. Stat.-Simul. Comput. 2010, 39, 860–864. [Google Scholar] [CrossRef]
- Westerdahl, J.; Olsson, H.; Måsbäck, A.; Ingvar, C.; Jonsson, N. Risk of malignant melanoma in relation to drug intake, alcohol, smoking and hormonal factors. Br. J. Cancer 1996, 73, 1126–1131. [Google Scholar] [CrossRef]
- Jensen, A.; Thomsen, H.F.; Engebjerg, M.C.; Olesen, A.B.; Sørensen, H.T.; Karagas, M.R. Use of photosensitising diuretics and risk of skin cancer: A population-based case-control study. Br. J. Cancer 2008, 99, 1522–1528. [Google Scholar] [CrossRef] [Green Version]
- Kaae, J.; Boyd, H.A.; Hansen, A.V.; Wulf, H.C.; Wohlfahrt, J.; Melbye, M. Photosensitizing medication use and risk of skin cancer. Cancer Epidemiol. Biomark. Prev. 2010, 19, 2942–2949. [Google Scholar] [CrossRef] [Green Version]
- Ruiter, R.; Visser, L.E.; Eijgelsheim, M.; Rodenburg, E.M.; Hofman, A.; Coebergh, J.W.; Nijsten, T.; Stricker, B.H. High-ceiling diuretics are associated with an increased risk of basal cell carcinoma in a population-based follow-up study. Eur. J. Cancer 2010, 46, 2467–2472. [Google Scholar] [CrossRef]
- De Vries, E.; Trakatelli, M.; Kalabalikis, D.; Ferrandiz, L.; Ruiz-de-Casas, A.; Moreno-Ramirez, D.; Sotiriadis, D.; Ioannides, D.; Aquilina, S.; Apap, C.; et al. Known and potential new risk factors for skin cancer in European populations: A multicentre case-control study. Br. J. Derm. 2012, 167 (Suppl. S2), 1–13. [Google Scholar] [CrossRef] [PubMed]
- Friedman, G.D.; Asgari, M.M.; Warton, E.M.; Chan, J.; Habel, L.A. Anti-hypertensive drugs and lip cancer in non-Hispanic whites. Arch. Intern. Med. 2012, 172, 1246–1251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Traianou, A.; Ulrich, M.; Apalla, Z.; De Vries, E.; Bakirtzi, K.; Kalabalikis, D.; Ferrandiz, L.; Ruiz-de-Casas, A.; Moreno-Ramirez, D.; Sotiriadis, D.; et al. Risk factors for actinic keratosis in eight European centres: A case-control study. Br. J. Derm. 2012, 167 (Suppl. S2), 36–42. [Google Scholar] [CrossRef] [PubMed]
- Robinson, S.N.; Zens, M.S.; Perry, A.E.; Spencer, S.K.; Duell, E.J.; Karagas, M.R. Photosensitizing agents and the risk of non-melanoma skin cancer: A population-based case-control study. J. Investig. Derm. 2013, 133, 1950–1955. [Google Scholar] [CrossRef] [Green Version]
- Schmidt, S.A.; Schmidt, M.; Mehnert, F.; Lemeshow, S.; Sørensen, H.T. Use of antihypertensive drugs and risk of skin cancer. J Eur. Acad. Derm. Venereol. 2015, 29, 1545–1554. [Google Scholar] [CrossRef]
- Nardone, B.; Majewski, S.; Kim, A.S.; Kiguradze, T.; Martinez-Escala, E.M.; Friedland, R.; Amin, A.; Laumann, A.E.; Edwards, B.J.; Rademaker, A.W.; et al. Melanoma and Non-Melanoma Skin Cancer Associated with Angiotensin-Converting-Enzyme Inhibitors, Angiotensin-Receptor Blockers and Thiazides: A Matched Cohort Study. Drug. Saf. 2017, 40, 249–255. [Google Scholar] [CrossRef]
- Pottegård, A.; Hallas, J.; Olesen, M.; Svendsen, M.T.; Habel, L.A.; Friedman, G.D.; Friis, S. Hydrochlorothiazide use is strongly associated with risk of lip cancer. J. Intern. Med. 2017, 282, 322–331. [Google Scholar] [CrossRef]
- Pedersen, S.A.; Gaist, D.; Schmidt, S.A.J.; Hölmich, L.R.; Friis, S.; Pottegård, A. Hydrochlorothiazide use and risk of non-melanoma skin cancer: A nationwide case-control study from Denmark. J. Am. Acad. Derm. 2018, 78, 673–681. [Google Scholar] [CrossRef] [Green Version]
- Pottegård, A.; Pedersen, S.A.; Schmidt, S.A.J.; Hölmich, L.R.; Friis, S.; Gaist, D. Association of Hydrochlorothiazide Use and Risk of Malignant Melanoma. JAMA Intern. Med. 2018, 178, 1120–1122. [Google Scholar] [CrossRef] [Green Version]
- Su, K.A.; Habel, L.A.; Achacoso, N.S.; Friedman, G.D.; Asgari, M.M. Photosensitizing anti-hypertensive drug use and risk of cutaneous squamous cell carcinoma. Br. J. Derm. 2018, 179, 1088–1094. [Google Scholar] [CrossRef]
- Pedersen, S.A.; Johannesdottir Schmidt, S.A.; Hölmich, L.R.; Friis, S.; Pottegård, A.; Gaist, D. Hydrochlorothiazide use and risk for Merkel cell carcinoma and malignant adnexal skin tumors: A nationwide case-control study. J. Am. Acad. Derm. 2019, 80, 460–465.e469. [Google Scholar] [CrossRef] [PubMed]
- Pottegård, A.; Pedersen, S.A.; Schmidt, S.A.J.; Lee, C.N.; Hsu, C.K.; Liao, T.C.; Shao, S.C.; Lai, E.C. Use of hydrochlorothiazide and risk of skin cancer: A nationwide Taiwanese case-control study. Br. J. Cancer 2019, 121, 973–978. [Google Scholar] [CrossRef]
- Daniels, B.; Pearson, S.A.; Vajdic, C.M.; Pottegård, A.; Buckley, N.A.; Zoega, H. Risk of squamous cell carcinoma of the lip and cutaneous melanoma in older Australians using hydrochlorothiazide: A population-based case-control study. Basic Clin. Pharm. Toxicol. 2020, 127, 320–328. [Google Scholar] [CrossRef]
- Lee, S.M.; Kim, K.; Yoon, J.; Park, S.K.; Moon, S.; Lee, S.E.; Oh, J.; Yoo, S.; Kim, K.I.; Yoon, H.J.; et al. Association between Use of Hydrochlorothiazide and Nonmelanoma Skin Cancer: Common Data Model Cohort Study in Asian Population. J. Clin. Med. 2020, 9, 2910. [Google Scholar] [CrossRef] [PubMed]
- Letellier, T.; Le Borgne, F.; Kerleau, C.; Gaultier, A.; Dantal, J.; Ville, S. Association between Use of Hydrochlorothiazide and Risk of Keratinocyte Cancers in Kidney Transplant Recipients. Clin. J. Am. Soc. Nephrol. 2020, 15, 1804–1813. [Google Scholar] [CrossRef] [PubMed]
- Morales, D.R.; Pacurariu, A.; Slattery, J.; Kurz, X. Association between hydrochlorothiazide exposure and different incident skin, lip and oral cavity cancers: A series of population-based nested case-control studies. Br. J. Clin. Pharm. 2020, 86, 1336–1345. [Google Scholar] [CrossRef] [Green Version]
- Park, E.; Lee, Y.; Jue, M.S. Hydrochlorothiazide use and the risk of skin cancer in patients with hypertensive disorder: A nationwide retrospective cohort study from Korea. Korean J. Intern. Med. 2020, 35, 917–928. [Google Scholar] [CrossRef] [Green Version]
- Adalsteinsson, J.A.; Muzumdar, S.; Waldman, R.; Hu, C.; Wu, R.; Ratner, D.; Ungar, J.; Silverberg, J.I.; Olafsdottir, G.H.; Kristjansson, A.K.; et al. Association between hydrochlorothiazide and the risk of in situ and invasive squamous cell skin carcinoma and basal cell carcinoma: A population-based case-control study. J. Am. Acad. Derm. 2021, 84, 669–675. [Google Scholar] [CrossRef]
- De Haan-Du, J.; Landman, G.W.D.; Groenier, K.H.; Vissers, P.A.J.; Louwman, M.W.J.; Kleefstra, N.; de Bock, G.H. The Risk of Cutaneous Squamous Cell Carcinoma Among Patients with Type 2 Diabetes Receiving Hydrochlorothiazide: A Cohort Study. Cancer Epidemiol. Biomark. Prev. 2021, 30, 2114–2121. [Google Scholar] [CrossRef]
- Drucker, A.M.; Hollestein, L.; Na, Y.; Weinstock, M.A.; Li, W.Q.; Abdel-Qadir, H.; Chan, A.W. Association between anti-hypertensive medications and risk of skin cancer in people older than 65 years: A population-based study. CMAJ 2021, 193, E508–E516. [Google Scholar] [CrossRef]
- Eworuke, E.; Haug, N.; Bradley, M.; Cosgrove, A.; Zhang, T.; Dee, E.C.; Adimadhyam, S.; Petrone, A.; Lee, H.; Woodworth, T.; et al. Risk of Nonmelanoma Skin Cancer in Association With Use of Hydrochlorothiazide-Containing Products in the United States. JNCI Cancer Spectr. 2021, 5, pkab009. [Google Scholar] [CrossRef] [PubMed]
- Habel, L.A.; Achacoso, N.; Fireman, B.; Pedersen, S.A.; Pottegård, A. Hydrochlorothiazide and risk of melanoma subtypes. Pharm. Drug Saf. 2021, 30, 1396–1401. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.C.; Kim, Y.C.; Choi, J.W. Use of hydrochlorothiazide and risk of non-melanoma skin cancer in Koreans: A retrospective cohort study using administrative healthcare data. Clin. Exp. Derm. 2021, 46, 680–686. [Google Scholar] [CrossRef] [PubMed]
- León-Muñoz, L.M.; Duarte-Salles, T.; Llorente, A.; Díaz, Y.; Puente, D.; Pottegård, A.; Montero-Corominas, D.; Huerta, C. Use of hydrochlorothiazide and risk of skin cancer in a large nested case-control study in Spain. Pharm. Drug Saf. 2021, 30, 1269–1278. [Google Scholar] [CrossRef]
- Rouette, J.; Yin, H.; Pottegård, A.; Nirantharakumar, K.; Azoulay, L. Use of Hydrochlorothiazide and Risk of Melanoma and Nonmelanoma Skin Cancer. Drug Saf. 2021, 44, 245–254. [Google Scholar] [CrossRef]
- Schneider, R.; Reinau, D.; Stoffel, S.; Jick, S.S.; Meier, C.R.; Spoendlin, J. Risk of skin cancer in new users of thiazides and thiazide-like diuretics: A cohort study using an active comparator group. Br. J. Derm. 2021, 185, 343–352. [Google Scholar] [CrossRef]
- Shaw, F.M.; Li, W.; Weinstock, M.A. Antihypertensive medications and risk of keratinocyte carcinoma. J. Investig. Derm. 2018, 138, S51. [Google Scholar] [CrossRef]
- Yeon, B.; Suh, A.; Choi, E.; Kim, B.; Han, S.Y.; Chung, S.Y. Assessing the risk of non-melanoma skin cancer associated with hydrochlorothiazide use in hypertensive patients: A nested case-control study in Korea. Pharm. Drug Saf. 2020, 29, 461–462. [Google Scholar] [CrossRef]
- International Agency for Research on Cancer (IARC). Some Drugs and Herbal Products. IARC Monographs on the Evaluation of Carcinogenic Risks to Humans; WHO Press: Geneva, Switzerland, 2016; Volume 108. [Google Scholar]
- Lopes, F.; Sleiman, M.G.; Sebastian, K.; Bogucka, R.; Jacobs, E.A.; Adamson, A.S. UV Exposure and the Risk of Cutaneous Melanoma in Skin of Color: A Systematic Review. JAMA Dermatol. 2021, 157, 213–219. [Google Scholar] [CrossRef]
- Lergenmuller, S.; Ghiasvand, R.; Robsahm, T.E.; Green, A.C.; Lund, E.; Rueegg, C.S.; Veierød, M.B. Association of Lifetime Indoor Tanning and Subsequent Risk of Cutaneous Squamous Cell Carcinoma. JAMA Dermatol. 2019, 155, 1350–1357. [Google Scholar] [CrossRef] [Green Version]
- An, S.; Kim, K.; Moon, S.; Ko, K.P.; Kim, I.; Lee, J.E.; Park, S.K. Indoor Tanning and the Risk of Overall and Early-Onset Melanoma and Non-Melanoma Skin Cancer: Systematic Review and Meta-Analysis. Cancers 2021, 13, 5940. [Google Scholar] [CrossRef] [PubMed]
- Xiang, F.; Lucas, R.; Hales, S.; Neale, R. Incidence of non-melanoma skin cancer in relation to ambient UV radiation in white populations, 1978–2012: Empirical relationships. JAMA Dermatol. 2014, 150, 1063–1071. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author (year) | Country | Study Design | Total Sample Size | Study Population | Database | Study Period | Age in Years, Mean ± SD | Female Sex, No. (%) | Definition of Thiazide Diuretics Exposure | Outcomes Reported: Skin Cancer |
|---|---|---|---|---|---|---|---|---|---|---|
| Westerdahl et al. (1996) [29] | Sweden | Nested case-control | 908 | Participants in the South Swedish Healthcare region | Regional cancer registry | 1 July 1988–30 June 1990 | Range: 15–75 (NS) | NR | Self-reported: used prescribed thiazide diuretics > 1 month continuously | MM |
| Jensen et al. (2008) [30] | Denmark | Nested case-control | BCC cohort, 29,820; SCC cohort, 5645; MM cohort, 5050 | Adult Danish residents in North Jutland country | EHRs linkage with cancer registry | 1989–2003 | BCC cohort, median 69; SCC cohort, median 77; MM cohort, median 59 | NR | Thiazide/Thiazide-like-users (bendroflumethiazide, indapamide, HCTZ): any prescriptions filled, >1 year, and >5 years before the index date | BCC, SCC, MM |
| Kaae et al. (2010) [31] | Denmark | Retrospective cohort | 4,761,749 | Danish residents | EHRs linkage with cancer registry | 1995–2006 | ≥15 (NS) | NR | Bendroflumethiazide users: filled at least 1 prescription | BCC, SCC, MCC, MM |
| Ruiter et al. (2010) [32] | Netherlands | Prospective cohort | 10,692 | Adult participants in the Rotterdam cohort (mainly Caucasians) | Rotterdam Study I and II; National registry of histo- and cytopathology | 1 April 1991–31 December 2007 | 69.0 (9.7) | 6404 (59.9) | Thiazide diuretics-users (chlorthalidone and thiazides in combination with other drugs) | BCC |
| de Vries et al. (2012) [33] | International | Case-control | 2521 | Hospital-based adult European populations in Finland, Germany, Greece, Italy, Malta, Poland, Scotland, and Spain | EPIDERM consortium, partly self-administered and partly completed by dermatologists | NR | 67.1 (12.1) | 1464 (58.1) | Thiazide diuretics-users (self-reported) | BCC, SCC, MM |
| Friedman et al. (2012) [34] | USA | Case-control | 23,616 | Adult non-Hispanic whites in the San Francisco Bay area and central valley of California | EHRs linkage with cancer registry—SEER program | 1 August 1994–29 February 2008 | 67.2 (8.8) | 6243 (26.4) | HCTZ-users | Lip cancer |
| Traianou et al. (2012) [35] | International | Case-control | 1029 | Hospital-based adult European populations in Finland, Germany, Greece, Italy, Malta, Poland, Scotland, and Spain | EPIDERM consortium, partly self-administered and partly completed by dermatologists | NR | 65.4 (9.7) | 382 (37.1) | Thiazide diuretics-users (self-reported) | Actinic keratosis |
| Robinson et al. (2013) [36] | USA | Nested case-control | Whole cohort, 5072; SCC cohort, 3505 | Adult residents of New Hampshire, speak English | Part of New Hampshire Skin Cancer Study | July 1993–June 2009 | ≤60, 2285 (45.1%); 61–70, 1846 (36.4%); >70, 941 (18.6%) | 2213 (43.6) | HCTZ-users (self-reported) | SCC |
| Schmidt et al. (2015) [37] | Denmark | Nested case-control | Whole cohort, 254,927; BCC cohort, 18,902; SCC cohort, 25,053; MM cohort, 40,253 | Adult Danish residents in northern Denmark | EHRs linkage with cancer registry | 1991–2010 | <60, 86,892 (34.1%); 60–69, 62,721 (24.6%); 70–79, 59,680 (23.4%); ≥80, 45,634 (17.9%) | 125,419 (49.2) | Thiazides diuretics-users (bendroflumethiazide, hydroflumethiazide, HCTZ, chlorothiazide) | BCC, SCC, MM |
| Nardone et al. (2017) [38] | USA | Retrospective cohort | 60,664 | Adult participants receiving treatment through Northwestern University healthcare affiliates | Northwestern Medicine Enterprise Data Warehouse | January 2004–December 2014 | <60, 29,791 (49.1%); 60–69, 15,412 (25.4%); 70–79, 10,129 (16.7%); 80–89, 5306 (8.7%) | 38,315 (63.2) | Thiazide diuretics-users (NS) | BCC, SCC, MM |
| Pottegård et al. (2017) [39] | Denmark | Nested case-control | 63,700 | Adults Danish residents | EHRs linkage with cancer registry | 1 January 2004–31 December 2012 | 72.0 (11.9) | 20,775 (32.6) | HCTZ-users | Lip cancer |
| Pedersen et al. (2018) [40] | Denmark | Nested case-control | BCC cohort, 1502436; SCC cohort, 181091 | Adults Danish residents | EHRs linkage with cancer registry | 1 January 2004–31 December 2012 | BCC cohort, 66.3 (14.1); SCC cohort, 76.7 (12.6) | 792,333 (52.7) | HCTZ-users | BCC, SCC |
| Pottegård et al. (2018) [41] | Denmark | Nested case-control | 212,003 | Adults Danish residents | EHRs linkage with cancer registry | 1 January 2004–31 December 2015 | Range:18–90 | NR | HCTZ-users | MM |
| Su et al. (2018) [42] | USA | Retrospective cohort | 28,357 | Adult non-Hispanic white patients with hypertension in a closed healthcare system | Based on KPNC’s Research Program in Genes and Environmental Health | 1 January 2002–31 December 2012 | 69.1 (10.6) | 15,975 (56.3) | Thiazide-users | SCC (in situ or invasive) |
| Pedersen et al. (2019) [43] | Denmark | Nested case-control | MCC cohort, 1954; MAST cohort, 2752 | Adult Danish residents | EHRs linkage with cancer registry | 1 January 2004–31 December 2015 | MCC cohort, 78.6 (11.9); MAST cohort, 71.0 (13.4) | MCC cohort, 1156 (59.2); MAST cohort, 1449 (52.6) | HCTZ-users | MCC, MAST |
| Pottegård et al. (2019) [44] | Taiwan | Nested case-control | 319,902 | Adult Taiwanese residents | NHIRD, Nationwide Taiwanese claims database | 1 January 2008–31 December 2015 | 67.3 (20.0) | 156,211 (48.8) | HCTZ-users | Non-melanoma skin cancer (lip and non-lip), MM |
| Daniels et al. (2020) [45] | Australia | Nested case-control | Lip cancer cohort, 911; MM cohort, 13,105 | Elderly patients aged ≥65 years within a population of veterans residing in New South Wales | EHRs linkage with cancer registry | 1 January 2004–31 December 2015 | Lip cancer cohort, 78.3 (4.5); MM cohort, 80.7 (3.7) | Lip cancer cohort, 386 (42.4); MM cohort, 4263 (32.5) | HCTZ-users | Lip cancer (SCC), MM |
| Lee et al. (2020) [46] | Korea | Retrospective cohort | 299,198 | Adult patients aged 20–80 years | Three-academic center hospital-Based | 1 January 2004–28 February 2018 | 59.7 (13.8) | 157,655 (52.7) | HCTZ-users | Non-melanoma skin cancer (NS), MM |
| Letellier et al. (2020) [47] | France | Retrospective cohort | 2496 | Adult patients undergoing kidney, pancreas, or combined kidney-pancreas transplantation with graft functioned ≥ 3 months) | Single-center at university hospital | 1 January 2000–31 December 2017 | 49.0 (14.0) | 958 (38.4) | HCTZ-users | BCC, SCC |
| Morales et al. (2020) [48] | UK | Nested case-control | BCC cohort, 1,870,800; SCC cohort, 158,754; lip cancer cohort, 71,207; oral cavity cancer cohort, 73,844; MM cohort, 234,885 | Population-based: adults aged ≥ 18 years | THIN database | 1 January 1999–1 May 2016 | SCC cohort, 74.8 (11.5); BCC cohort, 68.3 (13.6); lip cancer cohort, 63.8 (13.6); oral cavity cohort, 61.5 (13.2); MM cohort, 58.2 (16.4) | SCC cohort, 63,315 (39.9); BCC cohort, 913,647 (48.8); lip cancer cohort, 23,939 (33.6); oral cavity cancer cohort: 24,675 (33.4); MM cohort: 133,665 (56.9) | HCTZ-users | BCC, SCC, lip cancer, oral cavity cancer, MM |
| Park et al. (2020) [49] | Korea | Retrospective cohort | 3,565,952 | Population-based: adult patients aged ≥ 18 years with a first diagnosis of primary hypertension | Health Insurance Review and Assessment Service claims database | 1 January 2007–30 June 2017 | 55.5 (12.8) | 1,519,379 (47.8) | HCTZ-users | Non-melanoma skin cancer (NS), MM |
| Adalsteinsson et al. (2021) [50] | Iceland | Case-control | BCC cohort, 51,992; SCC in situ cohort, 13,128; invasive SCC cohort, 11,389 | Population-based: all Icelandic population | EHRs linkage with cancer registry | 2003–2017 | BCC cohort, 68.0 (17.1); SCC in situ cohort 76.0 (12.6); invasive SCC: 78.2 (11.1) | BCC cohort, 29,982 (57.7); SCC in situ cohort, 8335 (63.5); invasive SCC cohort: 5559 (48.8) | HCTZ-users | BCC, SCC in situ, invasive SCC |
| de Haan-Du et al. (2021) [51] | Netherlands | Prospective cohort | 70,494 | Adult type 2 diabetes patients | EHRs linkage with cancer registry | 1998–2019 | 66.5 (12.1) | 34,949 (49.6) | HCTZ-users | SCC |
| Drucker et al. (2021) [52] | Canada | Retrospective cohort | 262,575 | Population-based: elderly aged ≥ 65 years | Linked administrative health data from Ontario | 1 January 1998–31 December 2017 | 70.7 (5.9) | 165,723 (63.1) | New users of thiazides: chlorthalidone, HCTZ, indapamide, metolazone | BCC, SCC, MM |
| Eworuke et al. (2021) [53] | USA | Retrospective cohort | 10,422,642 | Adults participants | US FDA Sentinel System (17 health plans) | 1 January 2000–31 August 2018 | 60.7 (NS) | 5,503,155 (52.8) | New users of any HCTZ-containing products | BCC, SCC |
| Habel et al. (2021) [54] | USA | Nested case-control | 273,957 | Adults non-Hispanic White participants | KPNC, an integrated healthcare system | 1 January 1996–30 June 2014 | <60, 112,049 (40.9%); 60–69, 67,788 (24.7%); ≥70, 94,120 (34.4%) | 116,750 (42.6) | HCTZ-users | MM |
| Kim et al. (2021) [55] | Korea | Retrospective cohort | 124,486 | Adult participants randomly selected from 91% of people in the country | Korean National Health Insurance Service National Sample Cohort | 2002–2013 | <60, 65,214 (52.4%); 60–69, 32,762 (26.3%); ≥70, 26,510 (21.3%) | 64,774 (52.0) | HCTZ-users (cumulative dose of ≥2500 mg) | Non-melanoma skin cancer (NS) |
| León-Muñoz et al. (2021) [56]: SIDIAP cohort | Spain | Nested case-control | Nonmelanoma cohort, 814,100; MM cohort, 88,078 | Population-based: adults aged ≥ 18 years | SIDIAP, prospective database in primary care (Catalonia region) | 2007–2017 | Nonmelanoma cohort, 73.0 (14.1); MM cohort, 59.8 (19.3) | Nonmelanoma cohort, 431,643 (53.0); MM cohort, 49,181 (55.8) | HCTZ-users | Non-melanoma skin cancer (NS), MM |
| León-Muñoz et al. (2021) [56]: BIFAP cohort | Spain | Nested case-control | Nonmelanoma cohort, 341,693; MM cohort, 51271 | Population-based: adults aged ≥ 18 years | BIFAP, prospective database in primary care (different Spanish regions) | 2007–2017 | Nonmelanoma cohort, 72.7 (14.1); MM cohort, 60.7 (18.5) | Nonmelanoma cohort, 176,418 (51.6); MM cohort, 28,633 (55.8) | HCTZ-users | BCC, SCC, MM |
| Rouette et al. (2021) [57] | UK | Retrospective cohort | 41,026 | Population-based: adults aged ≥ 18 years | CPRD, primary care and linked data | 1 January 1988–31 March 2018 | 61.1 (14.9) | 24,292 (59.2) | New users of HCTZ | BCC, SCC, MM |
| Schneider et al. (2021) [58] | UK | Retrospective cohort | 546,417 | Population-based: adults aged 18–85 years | CPRD, primary care and linked data | 1 January 1998–31 December 2017 | 61.6 (13.4) | 344,079 (63.0) | New users of thiazides and thiazide-like diuretics | BCC, SCC, MM |
| Skin Cancer | No. of Included Studies (Sample Size) | OR (95% CI) | p-Value | E-Values for | 95% Prediction Interval | Heterogeneity | Strength of Evidence (Evidence-Based Conclusion) | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Point Estimate | CI Limit | Q Statistic | p-Value | I2 Index (95% CI) | τ2 | ||||||
| Primary Outcomes | |||||||||||
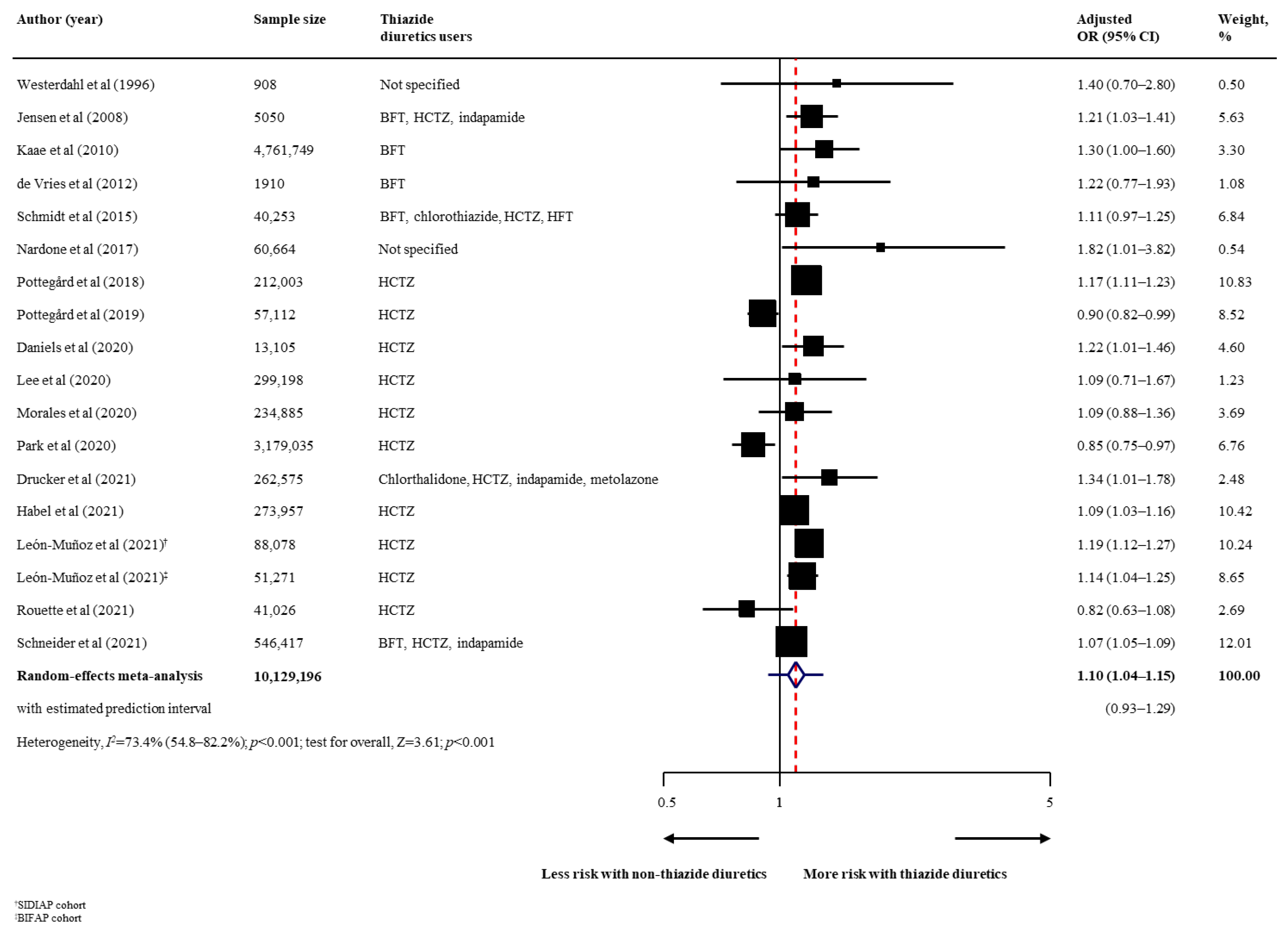
| Malignant melanoma: All subtype | 17 (n = 10,129,196) | 1.10 (1.04–1.15) | <0.001 | 1.420 | 1.255 | 0.93–129 | 63.94 | <0.001 | 73.4% (54.8–82.2) | 0.005 | Very low (very small harmful) |
| Malignant melanoma: Superficial spreading melanoma | 3 (n = 221,624) | 1.18 (1.05–1.33) | 0.006 | 1.643 | 1.279 | 0.35–4.02 | 4.32 | 0.115 | 53.7% (0.0–85.3) | 0.006 | Very low (very small harmful) |
| Malignant melanoma: Nodular melanoma | 3 (n = 36,631) | 1.23 (1.08–1.40) | 0.001 | 1.760 | 1.383 | 0.54–2.79 | 1.66 | 0.435 | 0.0% (0.0–72.9) | <0.001 | Very low (very small harmful) |
| Malignant melanoma: Lentigo maligna melanoma | 3 (n = 21,407) | 1.33 (1.08–1.65) | 0.008 | 2.001 | 1.365 | 0.18–10.09 | 3.17 | 0.205 | 36.9% (0.0–81.7) | 0.013 | Very low (very small harmful) |
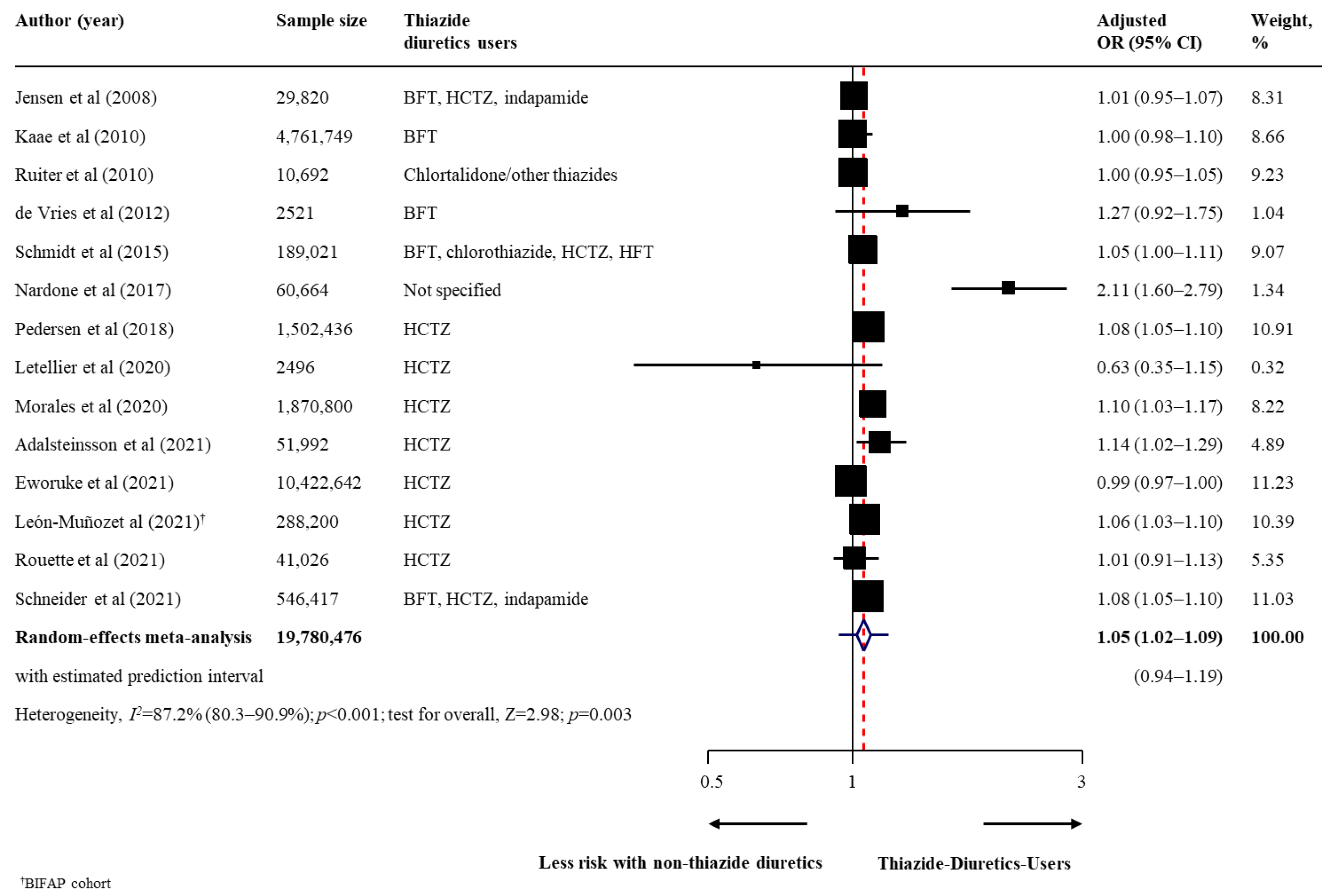
| Non-melanoma skin cancer: BCC | 14 (n = 19,780,476) | 1.05 (1.02–1.09) | 0.003 | 1.293 | 1.153 | 0.94–1.19 | 101.43 | <0.001 | 87.2% (80.3–90.9) | 0.003 | Very low (very small harmful) |
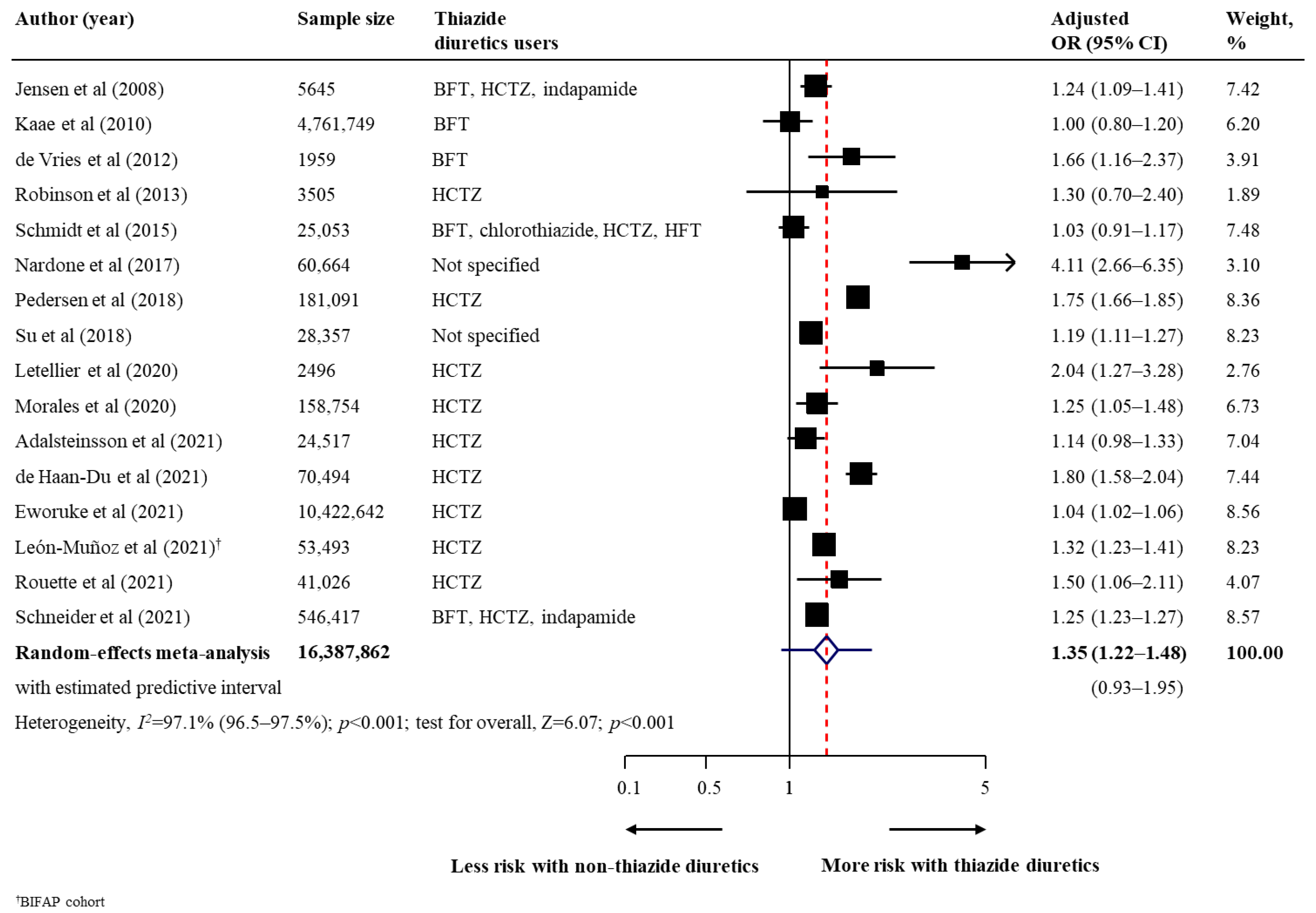
| Non-melanoma skin cancer: SCC | 16 (n = 16,387,862) | 1.35 (1.22–1.48) | <0.001 | 2.026 | 1.743 | 0.93–1.95 | 511.45 | <0.001 | 97.1% (96.5–97.5) | 0.028 | Very low (very small harmful) |
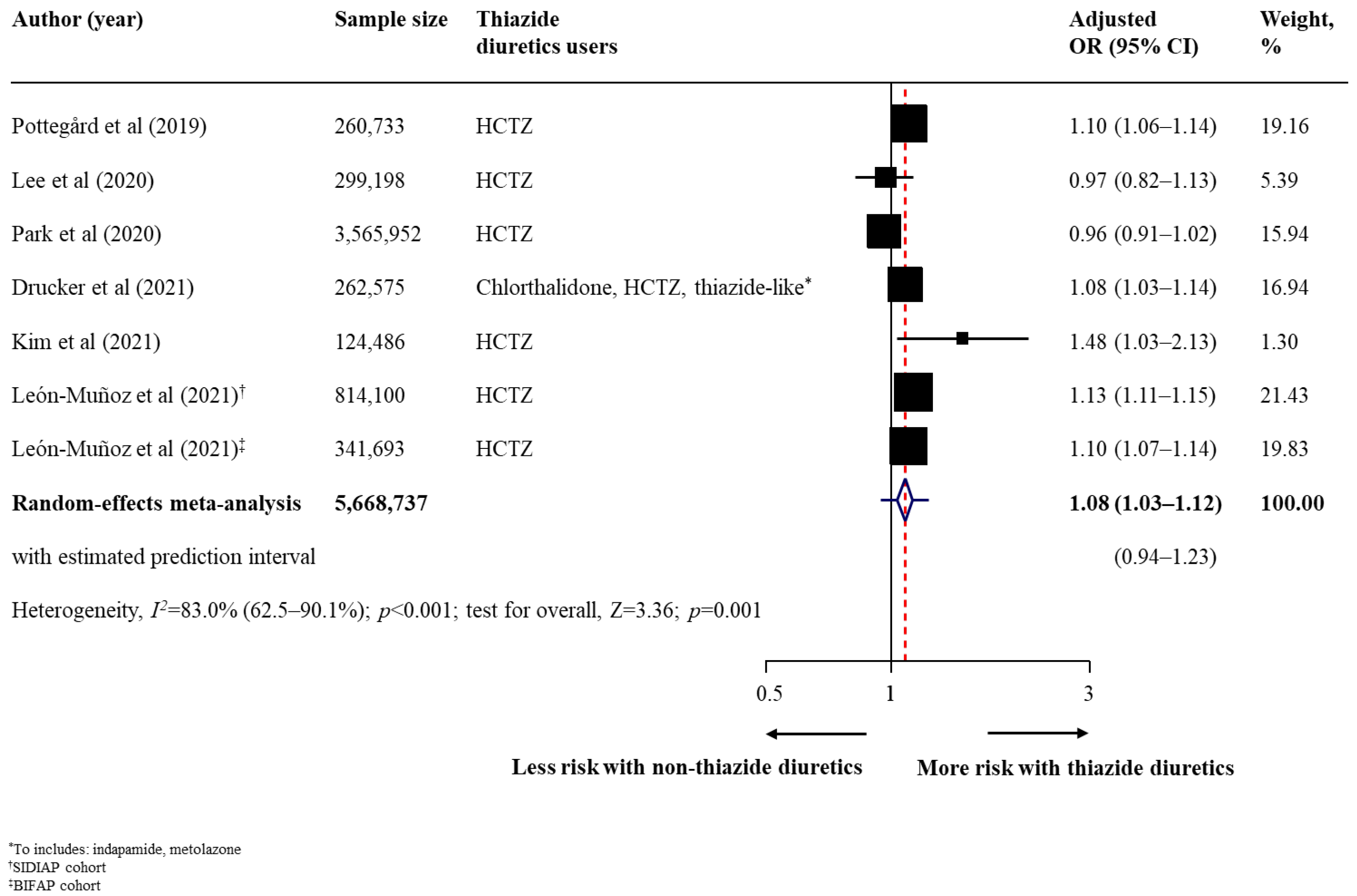
| Non-melanoma skin cancer: Unspecified | 6 (n = 5,668,737) | 1.08 (1.03–1.12) | 0.001 | 1.362 | 1.210 | 0.94–1.23 | 35.38 | <0.001 | 83.0% (62.5–90.1) | 0.002 | Very low (very small harmful) |
| Secondary Outcomes | |||||||||||
| Lip cancer | 5 (n = 161,491) | 1.92 (1.52–2.42) | <0.001 | 3.249 | 2.409 | 0.97–3.81 | 8.25 | 0.083 | 51.5% (0.0–80.3) | 0.032 | Very low (small harmful) |
| MCC | 2 (n = 4,763,703) | 0.98 (0.57–1.65) | 0.924 | 1.165 | 1.000 | NA | 0.12 | 0.732 | 0.0% (NA) | <0.001 | Insufficient data (NA) |
| MAST | 1 (n = 2752) | 1.40 (0.86–2.29) | 0.179 | 2.148 | 1.000 | NA | NA | NA | NA | NA | Insufficient data (NA) |
| Oral cavity cancer | 1 (n = 73,844) | 0.90 (0.60–1.36) | 0.614 | 1.462 | 1.000 | NA | NA | NA | NA | NA | Insufficient data (NA) |
| Actinic keratosis | 1 (n = 1029) | 3.18 (1.93–5.25) | <0.001 | 5.813 | 3.270 | NA | NA | NA | NA | NA | Insufficient data (NA) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nochaiwong, S.; Chuamanochan, M.; Ruengorn, C.; Noppakun, K.; Awiphan, R.; Phosuya, C.; Tovanabutra, N.; Chiewchanvit, S.; Sood, M.M.; Hutton, B.; et al. Use of Thiazide Diuretics and Risk of All Types of Skin Cancers: An Updated Systematic Review and Meta-Analysis. Cancers 2022, 14, 2566. https://doi.org/10.3390/cancers14102566
Nochaiwong S, Chuamanochan M, Ruengorn C, Noppakun K, Awiphan R, Phosuya C, Tovanabutra N, Chiewchanvit S, Sood MM, Hutton B, et al. Use of Thiazide Diuretics and Risk of All Types of Skin Cancers: An Updated Systematic Review and Meta-Analysis. Cancers. 2022; 14(10):2566. https://doi.org/10.3390/cancers14102566
Chicago/Turabian StyleNochaiwong, Surapon, Mati Chuamanochan, Chidchanok Ruengorn, Kajohnsak Noppakun, Ratanaporn Awiphan, Chabaphai Phosuya, Napatra Tovanabutra, Siri Chiewchanvit, Manish M. Sood, Brian Hutton, and et al. 2022. "Use of Thiazide Diuretics and Risk of All Types of Skin Cancers: An Updated Systematic Review and Meta-Analysis" Cancers 14, no. 10: 2566. https://doi.org/10.3390/cancers14102566
APA StyleNochaiwong, S., Chuamanochan, M., Ruengorn, C., Noppakun, K., Awiphan, R., Phosuya, C., Tovanabutra, N., Chiewchanvit, S., Sood, M. M., Hutton, B., Thavorn, K., & Knoll, G. A. (2022). Use of Thiazide Diuretics and Risk of All Types of Skin Cancers: An Updated Systematic Review and Meta-Analysis. Cancers, 14(10), 2566. https://doi.org/10.3390/cancers14102566