
No Geographical Inequalities in Survival for Sarcoma Patients in France: A Reference Networks’ Outcome?

 , , , , , , , , and
, , , , , , , , and  add
Show full author list
add
Show full author list
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. National Sarcoma Networks Databases
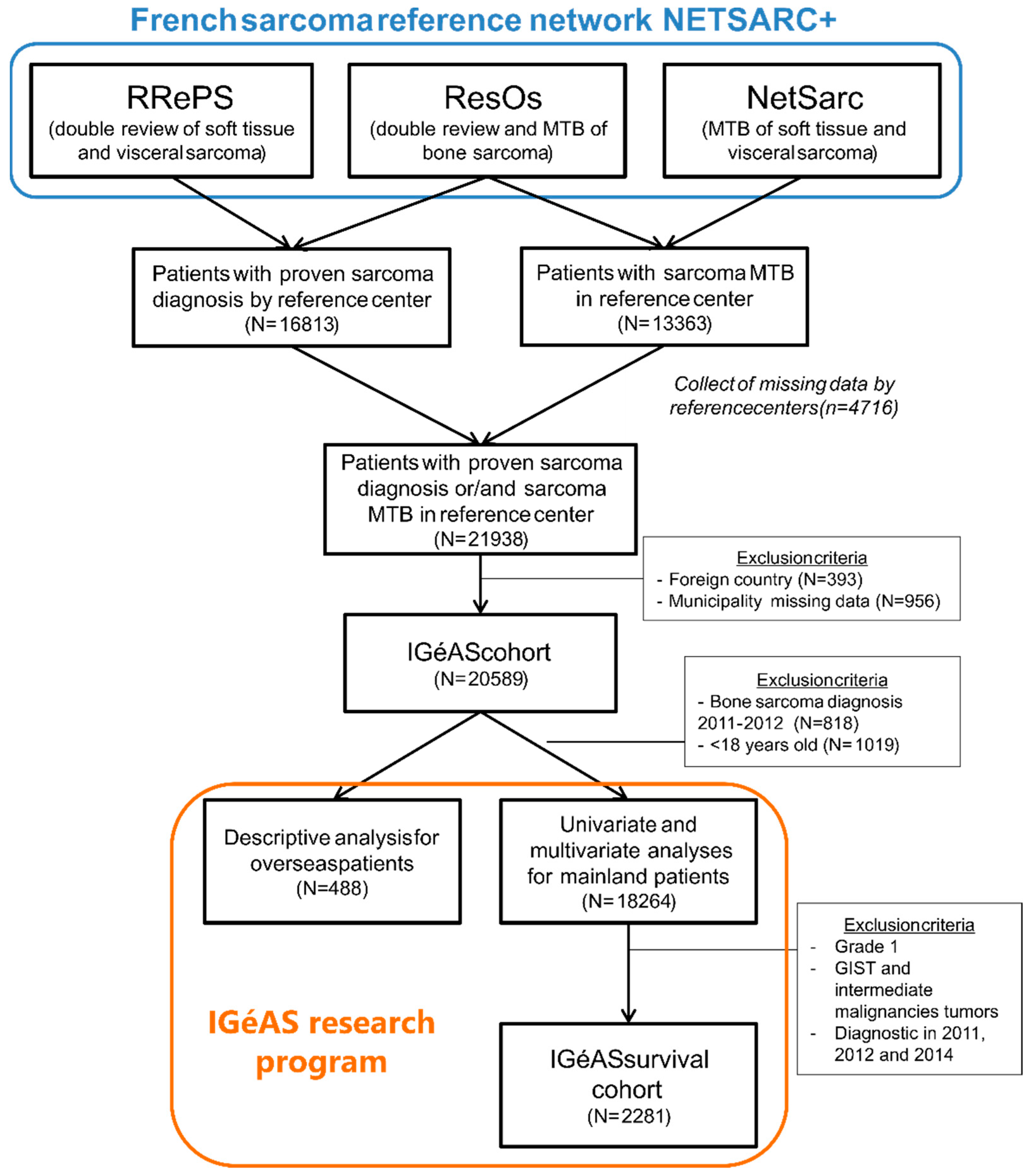
2.2. Constitution of the IGéAS Survival Cohort
- -
- Patient living in France at time of diagnosis;
- -
- Diagnosis of sarcoma/GIST/desmoid tumor/intermediate malignant tumor between 1 January 2011 and 31 December 2014;
- -
- Patient who benefiting from a review or a sarcoma MTB discussion in reference center belonging to the NETSARC+ network.
2.3. Statistical Analysis
- -
- the GeoClasH classification distinguishing, through a K-means clustering, five types of French municipalities (metropolitan areas, precarious population districts, residential outskirts, agricultural and industrial plains, rural margins) from ten geographical scores measuring physical and social environments, as well as the spatial accessibility of health care [35];
- -
- the European Deprivation Index built by the ERISC platform (http://cancerspreventions.fr/inegalites-sociales/plateforme-2/, accessed on 24 May 2022) and based on ten social variables selected and weighted according to their association with individual data from the European Union Statistics on Income and Living Conditions survey [36];
- -
- the average travel time to the closest reference clinical center calculated with Odomatrix software [22].
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Factor Label | Events/N | Hazard Ratio (95% CI) | p-Value |
|---|---|---|---|
| GeoClasH Classification of municipalities | 0.6552 | ||
| Wealthy Metropolitan Areas | 139/440 | 1 | |
| Precarious Population Districts | 392/1122 | 1.03 (0.85–1.25) | |
| Residential Outskirts | 105/305 | 1.03 (0.80–1.33) | |
| Agricultural and Industrial Plains | 66/178 | 1.23 (0.91–1.65) | |
| Rural Margins | 35/107 | 0.94 (0.64–1.36) | |
| Age | <0.0001 | ||
| [0–15[ | 19/89 | 1 | |
| [15–18[ | 13/42 | 1.17 (0.57–2.37) | |
| [18–25[ | 35/95 | 1.99 (1.13–3.49) | |
| [25–50[ | 121/443 | 1.68 (1.03–2.76) | |
| [50–70[ | 282/795 | 2.67 (1.65–4.33) | |
| ≥70 | 267/688 | 4.38 (2.69–7.14) | |
| Sex | 0.0656 | ||
| Male | 407/1120 | 1 | |
| Female | 330/1032 | 0.87 (0.74–1.01) | |
| Type of tumor | 0.2041 | ||
| Bone | 115/364 | 1 | |
| Soft tissue | 494/1490 | 0.87 (0.48–1.56) | |
| Viscera | 128/298 | 1.25 (0.83–1.87) | |
| Depth | 0.7198 | ||
| Superficial | 70/297 | 1 | |
| Superficial and deep | 38/135 | 0.97 (0.64–1.46) | |
| Deep | 521/1395 | 1.13 (0.85–1.52) | |
| Missing | 108/325 | 1.07 (0.67–1.69) | |
| Size of tumor | <0.0001 | ||
| [0–50[ | 100/490 | 1 | |
| [50–100[ | 217/661 | 1.49 (1.16–1.92) | |
| ≥100 | 341/802 | 1.94 (1.51–2.50) | |
| Missing | 79/199 | 1.89 (1.37–2.60) | |
| Grade | <0.0001 | ||
| 2 | 164/637 | 1 | |
| 3 | 491/1215 | 1.78 (1.48–2.14) | |
| Missing | 82/300 | 1.20 (0.91–1.57) | |
| Internal trunk | 0.0752 | ||
| No | 558/1718 | 1 | |
| Yes | 179/434 | 1.54 (0.96–2.48) | |
| Metastatic at diagnosis | <0.0001 | ||
| No | 541/1817 | 1 | |
| Yes | 196/335 | 2.98 (2.50–3.56) |
References
- de Souza, J.A.; Hunt, B.; Asirwa, F.C.; Adebamowo, C.; Lopes, G. Global Health Equity: Cancer Care Outcome Disparities in High-, Middle-, and Low-Income Countries. J. Clin. Oncol. 2016, 34, 6–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaccarella, S.; Lortet-Tieulent, J.; Saracci, R.; Conway, D.; Straif, K.; Wild, C. Reducing Social Inequalities in Cancer: Evidence and Priorities for Research; International Agency for Research on Cancer: Lyon, France, 2019; ISBN 978-92-832-2223-1.
- Menvielle, G.; Kulhánová, I.; Mackenbach, J.P. Assessing the Impact of a Public Health Intervention to Reduce Social Inequalities in Cancer. In Reducing Social Inequalities in Cancer: Evidence and Priorities for Research; International Agency for Research on Cancer: Lyon, France, 2019. [Google Scholar]
- Boyle, P.; Smans, M. Atlas of Cancer Mortality in the European Union and the European Economic Area 1993–1997; IARC Scientific Publications: Lyon, France, 2008; ISBN 978-92-832-2159-3. ISSN 0300-5038. [Google Scholar]
- Bennett, J.E.; Li, G.; Foreman, K.; Best, N.; Kontis, V.; Pearson, C.; Hambly, P.; Ezzati, M. The Future of Life Expectancy and Life Expectancy Inequalities in England and Wales: Bayesian Spatiotemporal Forecasting. Lancet 2015, 386, 163–170. [Google Scholar] [CrossRef] [Green Version]
- Dwyer-Lindgren, L.; Bertozzi-Villa, A.; Stubbs, R.W.; Morozoff, C.; Mackenbach, J.P.; van Lenthe, F.J.; Mokdad, A.H.; Murray, C.J.L. Inequalities in Life Expectancy Among US Counties, 1980 to 2014: Temporal Trends and Key Drivers. JAMA Intern. Med. 2017, 177, 1003–1011. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ezzati, M.; Friedman, A.B.; Kulkarni, S.C.; Murray, C.J.L. The Reversal of Fortunes: Trends in County Mortality and Cross-County Mortality Disparities in the United States. PLoS Med. 2008, 5, e66. [Google Scholar] [CrossRef]
- Cramb, S.M.; Mengersen, K.L.; Turrell, G.; Baade, P.D. Spatial Inequalities in Colorectal and Breast Cancer Survival: Premature Deaths and Associated Factors. Health Place 2012, 18, 1412–1421. [Google Scholar] [CrossRef] [Green Version]
- Stanbury, J.F.; Baade, P.D.; Yu, Y.; Yu, X.Q. Impact of Geographic Area Level on Measuring Socioeconomic Disparities in Cancer Survival in New South Wales, Australia: A Period Analysis. Cancer Epidemiol. 2016, 43, 56–62. [Google Scholar] [CrossRef]
- Baade, P.D.; Yu, X.Q.; Smith, D.P.; Dunn, J.; Chambers, S.K. Geographic Disparities in Prostate Cancer Outcomes—Review of International Patterns. Asian Pac. J. Cancer Prev. 2015, 16, 1259–1275. [Google Scholar] [CrossRef] [Green Version]
- Baade, P.D.; Dasgupta, P.; Aitken, J.F.; Turrell, G. Geographic Remoteness, Area-Level Socioeconomic Disadvantage and Inequalities in Colorectal Cancer Survival in Queensland: A Multilevel Analysis. BMC Cancer 2013, 13, 493. [Google Scholar] [CrossRef] [Green Version]
- Dasgupta, P.; Baade, P.D.; Aitken, J.F.; Ralph, N.; Chambers, S.K.; Dunn, J. Geographical Variations in Prostate Cancer Outcomes: A Systematic Review of International Evidence. Front. Oncol. 2019, 9, 238. [Google Scholar] [CrossRef] [Green Version]
- Henry, K.A.; Niu, X.; Boscoe, F.P. Geographic Disparities in Colorectal Cancer Survival. Int. J. Health Geogr. 2009, 8, 48. [Google Scholar] [CrossRef] [Green Version]
- Johnson, A.M.; Hines, R.B.; Johnson, J.A.; Bayakly, A.R. Treatment and Survival Disparities in Lung Cancer: The Effect of Social Environment and Place of Residence. Lung Cancer 2014, 83, 401–407. [Google Scholar] [CrossRef] [PubMed]
- Onega, T.; Duell, E.J.; Shi, X.; Wang, D.; Demidenko, E.; Goodman, D. Geographic Access to Cancer Care in the U.S. Cancer 2008, 112, 909–918. [Google Scholar] [CrossRef] [PubMed]
- Onega, T.; Alford-Teaster, J.; Wang, F. Population-Based Geographic Access to Parent and Satellite National Cancer Institute Cancer Center Facilities. Cancer 2017, 123, 3305–3311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dejardin, O.; Jones, A.P.; Rachet, B.; Morris, E.; Bouvier, V.; Jooste, V.; Coombes, E.; Forman, D.; Bouvier, A.M.; Launoy, G. The Influence of Geographical Access to Health Care and Material Deprivation on Colorectal Cancer Survival: Evidence from France and England. Health Place 2014, 30, 36–44. [Google Scholar] [CrossRef] [Green Version]
- Murage, P.; Crawford, S.M.; Bachmann, M.; Jones, A. Geographical Disparities in Access to Cancer Management and Treatment Services in England. Health Place 2016, 42, 11–18. [Google Scholar] [CrossRef] [Green Version]
- Gentil, J.; Dabakuyo, T.S.; Ouedraogo, S.; Poillot, M.-L.; Dejardin, O.; Arveux, P. For Patients with Breast Cancer, Geographic and Social Disparities Are Independent Determinants of Access to Specialized Surgeons. A Eleven-Year Population-Based Multilevel Analysis. BMC Cancer 2012, 12, 351. [Google Scholar] [CrossRef]
- Blais, S.; Dejardin, O.; Boutreux, S.; Launoy, G. Social Determinants of Access to Reference Care Centres for Patients with Colorectal Cancer—A Multilevel Analysis. Eur. J. Cancer 2006, 42, 3041–3048. [Google Scholar] [CrossRef]
- Gatta, G.; van der Zwan, J.M.; Casali, P.G.; Siesling, S.; Dei Tos, A.P.; Kunkler, I.; Otter, R.; Licitra, L.; Mallone, S.; Tavilla, A.; et al. Rare Cancers Are Not so Rare: The Rare Cancer Burden in Europe. Eur. J. Cancer 2011, 47, 2493–2511. [Google Scholar] [CrossRef]
- Fayet, Y.; Coindre, J.-M.; Dalban, C.; Gouin, F.; De Pinieux, G.; Farsi, F.; Ducimetière, F.; Chemin-Airiau, C.; Jean-Denis, M.; Chabaud, S.; et al. Geographical Accessibility of the Sarcoma Referral Networks in France. Intermediate Results from the IGéAS Research Program. Int. J. Environ. Res. Public Health 2018, 15, 2204. [Google Scholar] [CrossRef] [Green Version]
- Frezza, A.M.; Trama, A.; Blay, J.-Y.; Casali, P.G. Networking in Rare Cancers: What Was Done, What’s Next. Eur. J. Surg. Oncol. 2019, 45, 16–18. [Google Scholar] [CrossRef]
- Sandrucci, S.; Gatta, G. Rare Cancers: A Network for Better Care. Eur. J. Surg. Oncol. 2019, 45, 1–2. [Google Scholar] [CrossRef]
- Casali, P.G. Rare Cancers: From Centralized Referral to Networking. Ann. Oncol. 2019, 30, 1037–1038. [Google Scholar] [CrossRef] [PubMed]
- de Pinieux, G.; Karanian-Philippe, M.; Le Loarer, F.; Le Guellec, S.; Chabaud, S.; Terrier, P.; Bouvier, C.; Battistella, M.; Neuville, A.; Robin, Y.-M.; et al. Nationwide Incidence of Sarcomas and Tumors of Intermediate Malignancy in France; Social Science Research Network: Rochester, NY, USA, 2020. [Google Scholar]
- Amadeo, B.; Penel, N.; Coindre, J.-M.; Ray-Coquard, I.; Ligier, K.; Delafosse, P.; Bouvier, A.-M.; Plouvier, S.; Gallet, J.; Lacourt, A.; et al. Incidence and Time Trends of Sarcoma (2000–2013): Results from the French Network of Cancer Registries (FRANCIM). BMC Cancer 2020, 20, 190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lurkin, A.; Ducimetière, F.; Vince, D.R.; Decouvelaere, A.-V.; Cellier, D.; Gilly, F.N.; Salameire, D.; Biron, P.; de Laroche, G.; Blay, J.Y.; et al. Epidemiological Evaluation of Concordance between Initial Diagnosis and Central Pathology Review in a Comprehensive and Prospective Series of Sarcoma Patients in the Rhone-Alpes Region. BMC Cancer 2010, 10, 150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Derbel, O.; Heudel, P.E.; Cropet, C.; Meeus, P.; Vaz, G.; Biron, P.; Cassier, P.; Decouvelaere, A.-V.; Ranchere-Vince, D.; Collard, O.; et al. Survival Impact of Centralization and Clinical Guidelines for Soft Tissue Sarcoma (A Prospective and Exhaustive Population-Based Cohort). PLoS ONE 2017, 12, e0158406. [Google Scholar] [CrossRef] [PubMed]
- Ray-Coquard, I.; Thiesse, P.; Ranchère-Vince, D.; Chauvin, F.; Bobin, J.-Y.; Sunyach, M.-P.; Carret, J.-P.; Mongodin, B.; Marec-Bérard, P.; Philip, T.; et al. Conformity to Clinical Practice Guidelines, Multidisciplinary Management and Outcome of Treatment for Soft Tissue Sarcomas. Ann. Oncol. 2004, 15, 307–315. [Google Scholar] [CrossRef]
- Blay, J.-Y.; Honoré, C.; Stoeckle, E.; Meeus, P.; Jafari, M.; Gouin, F.; Anract, P.; Ferron, G.; Rochwerger, A.; Ropars, M.; et al. Surgery in Reference Centers Improves Survival of Sarcoma Patients: A Nationwide Study. Ann. Oncol. 2019, 30, 1143–1153. [Google Scholar] [CrossRef]
- Blay, J.-Y.; Soibinet, P.; Penel, N.; Bompas, E.; Duffaud, F.; Stoeckle, E.; Mir, O.; Adam, J.; Chevreau, C.; Bonvalot, S.; et al. Improved Survival Using Specialized Multidisciplinary Board in Sarcoma Patients. Ann. Oncol. 2017, 28, 2852–2859. [Google Scholar] [CrossRef]
- Casali, P.G.; Abecassis, N.; Aro, H.T.; Bauer, S.; Biagini, R.; Bielack, S.; Bonvalot, S.; Boukovinas, I.; Bovee, J.V.M.G.; Brodowicz, T.; et al. Soft Tissue and Visceral Sarcomas: ESMO-EURACAN Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up. Ann. Oncol. 2018, 29, iv51–iv67. [Google Scholar] [CrossRef]
- Fayet, Y.; Tétreau, R.; Honoré, C.; Le Nail, L.-R.; Dalban, C.; Gouin, F.; Causeret, S.; Piperno-Neumann, S.; Mathoulin-Pelissier, S.; Karanian, M.; et al. Determinants of the Access to Remote Specialised Services Provided by National Sarcoma Reference Centres. BMC Cancer 2021, 21, 631. [Google Scholar] [CrossRef]
- Fayet, Y.; Praud, D.; Fervers, B.; Ray-Coquard, I.; Blay, J.-Y.; Ducimetiere, F.; Fagherazzi, G.; Faure, E. Beyond the Map: Evidencing the Spatial Dimension of Health Inequalities. Int. J. Health Geogr. 2020, 19, 46. [Google Scholar] [CrossRef] [PubMed]
- Pornet, C.; Delpierre, C.; Dejardin, O.; Grosclaude, P.; Launay, L.; Guittet, L.; Lang, T.; Launoy, G. Construction of an Adaptable European Transnational Ecological Deprivation Index: The French Version. J. Epidemiol. Community Health 2012, 66, 982–989. [Google Scholar] [CrossRef] [PubMed]
- Diessner, B.J.; Weigel, B.J.; Murugan, P.; Zhang, L.; Poynter, J.N.; Spector, L.G. Associations of Socioeconomic Status, Public vs Private Insurance, and Race/Ethnicity With Metastatic Sarcoma at Diagnosis. JAMA Netw. Open 2020, 3, e2011087. [Google Scholar] [CrossRef] [PubMed]
- Westermann, C.; Weller, J.; Pedroso, F.; Canner, J.; Pratilas, C.A.; Rhee, D.S. Socioeconomic and Health Care Coverage Disparities in Children, Adolescents, and Young Adults with Sarcoma. Pediatr. Blood Cancer 2020, 67, e28708. [Google Scholar] [CrossRef]
- Cheung, M.R.; Kang, J.; Ouyang, D.; Yeung, V. Socio-Economic Factors Affect the Outcome of Soft Tissue Sarcoma: An Analysis of SEER Data. Asian Pac. J. Cancer Prev. 2014, 15, 25–28. [Google Scholar] [CrossRef] [Green Version]
- Miller, B.J.; Gao, Y.; Duchman, K.R. Socioeconomic Measures Influence Survival in Osteosarcoma: An Analysis of the National Cancer Data Base. Cancer Epidemiol. 2017, 49, 112–117. [Google Scholar] [CrossRef]
- Brennan, B.; Stiller, C.; Grimer, R.; Dennis, N.; Broggio, J.; Francis, M. Outcome and the Effect of Age and Socioeconomic Status in 1318 Patients with Synovial Sarcoma in the English National Cancer Registry: 1985–2009. Clin. Sarcoma Res. 2016, 6, 18. [Google Scholar] [CrossRef] [Green Version]
- Raedkjaer, M.; Maretty-Kongstad, K.; Baad-Hansen, T.; Safwat, A.; Mørk Petersen, M.; Keller, J.; Vedsted, P. The Association between Socioeconomic Position and Tumour Size, Grade, Stage, and Mortality in Danish Sarcoma Patients—A National, Observational Study from 2000 to 2013. Acta Oncol. 2020, 59, 127–133. [Google Scholar] [CrossRef]
- Tron, L.; Belot, A.; Fauvernier, M.; Remontet, L.; Bossard, N.; Launay, L.; Bryere, J.; Monnereau, A.; Dejardin, O.; Launoy, G. Socioeconomic Environment and Disparities in Cancer Survival for 19 Solid Tumor Sites: An Analysis of the French Network of Cancer Registries (FRANCIM) Data. Int. J. Cancer 2019, 144, 1262–1274. [Google Scholar] [CrossRef] [Green Version]
- Eastman, B.M.; Hippe, D.S.; Wootton, L.S.; Nyflot, M.J.; Thompson, M.J.; Pollack, S.M.; Kim, E.; Spraker, M.B. Socio-Economic Factors Do Not Affect Overall Survival in Soft Tissue Sarcoma When Patients Treated at a Single High-Volume Center. BMC Cancer 2021, 21, 620. [Google Scholar] [CrossRef]
- Thomas, A.A.; Gallagher, P.; O’Céilleachair, A.; Pearce, A.; Sharp, L.; Molcho, M. Distance from Treating Hospital and Colorectal Cancer Survivors’ Quality of Life: A Gendered Analysis. Support. Care Cancer 2015, 23, 741–751. [Google Scholar] [CrossRef] [PubMed]
- Penel, N.; Coindre, J.-M.; Bonvalot, S.; Italiano, A.; Neuville, A.; Le Cesne, A.; Terrier, P.; Ray-Coquard, I.; Ranchere-Vince, D.; Robin, Y.-M.; et al. Management of Desmoid Tumours: A Nationwide Survey of Labelled Reference Centre Networks in France. Eur. J. Cancer 2016, 58, 90–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perrier, L.; Rascle, P.; Morelle, M.; Toulmonde, M.; Ranchere Vince, D.; Le Cesne, A.; Terrier, P.; Neuville, A.; Meeus, P.; Farsi, F.; et al. The Cost-Saving Effect of Centralized Histological Reviews with Soft Tissue and Visceral Sarcomas, GIST, and Desmoid Tumors: The Experiences of the Pathologists of the French Sarcoma Group. PLoS ONE 2018, 13, e0193330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonvalot, S.; Gaignard, E.; Stoeckle, E.; Meeus, P.; Decanter, G.; Carrere, S.; Honore, C.; Delhorme, J.B.; Fau, M.; Tzanis, D.; et al. Survival Benefit of the Surgical Management of Retroperitoneal Sarcoma in a Reference Center: A Nationwide Study of the French Sarcoma Group from the NetSarc Database. Ann. Surg. Oncol. 2019, 26, 2286–2293. [Google Scholar] [CrossRef] [PubMed]
- Smith, D.; Thomson, K.; Bambra, C.; Todd, A. The Breast Cancer Paradox: A Systematic Review of the Association between Area-Level Deprivation and Breast Cancer Screening Uptake in Europe. Cancer Epidemiol. 2019, 60, 77–85. [Google Scholar] [CrossRef] [PubMed]
- Peretti-Watel, P.; L’Haridon, O.; Seror, V. Time Preferences, Socioeconomic Status and Smokers’ Behaviour, Attitudes and Risk Awareness. Eur. J. Public Health 2013, 23, 783–788. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alvegård, T.; Sundby Hall, K.; Bauer, H.; Rydholm, A. The Scandinavian Sarcoma Group: 30 Years’ Experience. Acta Orthop. Suppl. 2009, 80, 1–104. [Google Scholar] [CrossRef]
- Benson, C.; Judson, I. Role of Expert Centres in the Management of Sarcomas—A UK Perspective. Eur. J. Cancer 2014, 50, 1951–1956. [Google Scholar] [CrossRef]
- Mastrangelo, G.; Coindre, J.-M.; Ducimetière, F.; Dei Tos, A.P.; Fadda, E.; Blay, J.-Y.; Buja, A.; Fedeli, U.; Cegolon, L.; Frasson, A.; et al. Incidence of Soft Tissue Sarcoma and beyond: A Population-Based Prospective Study in 3 European Regions. Cancer 2012, 118, 5339–5448. [Google Scholar] [CrossRef]


| Factor Label | Univariable (N = 2281) | Multivariable (N = 2152) | ||||
|---|---|---|---|---|---|---|
| Deaths/N | Hazard Ratio (95% CI) | p-Value | Deaths/N | Hazard Ratio (95% CI) | p-Value | |
| Sex | 0.0363 | 0.0477 | ||||
| Male | 429/1188 | 1 | 407/1120 | 1 | ||
| Female | 352/1093 | 0.86 (0.75–0.99) | 330/1032 | 0.86 (0.74–1.00) | ||
| Age | <0.0001 | <0.0001 | ||||
| [0–15[ | 21/97 | 1 | 19/89 | 1 | ||
| [15–18[ | 13/43 | 1.19 (0.60–2.37) | 13/42 | 1.18 (0.58–2.40) | ||
| [18–25[ | 36/97 | 1.88 (1.10–3.23) | 35/95 | 2.00 (1.14–3.50) | ||
| [25–50[ | 124/464 | 1.27 (0.80–2.02) | 121/443 | 1.67 (1.02–2.73) | ||
| [50–70[ | 298/838 | 1.98 (1.27–3.09) | 282/795 | 2.64 (1.63–4.27) | ||
| ≥70 | 289/742 | 2.83 (1.82–4.41) | 267/688 | 4.29 (2.64–6.97) | ||
| Type of tumor | 0.0007 | 0.0119 | ||||
| Bone | 121/384 | 1 | 115/364 | 1 | ||
| Soft tissue | 526/1573 | 1.21 (0.99–1.48) | 494/1490 | 0.96 (0.76–1.21) | ||
| Viscera | 134/324 | 1.60 (1.25–2.05) | 128/298 | 1.33 (1.01–1.75) | ||
| Depth of tumor | 0.0008 | |||||
| Superficial | 76/321 | 1 | ||||
| Superficial and deep | 42/144 | 1.19 (0.81–1.73) | ||||
| Deep | 548/1470 | 1.51 (1.18–1.91) | ||||
| Missing | 115/346 | 1.15 (0.86–1.54) | ||||
| Size of tumor | <0.0001 | <0.0001 | ||||
| [0–50[ | 104/513 | 1 | 100/490 | 1 | ||
| [50–100[ | 227/687 | 1.61 (1.28–2.04) | 217/661 | 1.46 (1.15–1.86) | ||
| ≥100 | 350/831 | 2.30 (1.84–2.86) | 341/802 | 1.89 (1.50–2.38) | ||
| Missing | 100/250 | 2.91 (2.21–3.83) | 79/199 | 1.88 (1.38–2.56) | ||
| Grade | <0.0001 | <0.0001 | ||||
| 2 | 176/677 | 1 | 164/637 | 1 | ||
| 3 | 515/1280 | 1.66 (1.40–1.97) | 491/1215 | 1.78 (1.48–2.14) | ||
| Missing | 90/324 | 1.22 (0.95–1.58) | 82/300 | 1.21 (0.93–1.59) | ||
| Lower limb | 0.0671 | |||||
| No | 641/1835 | 1 | ||||
| Yes | 136/439 | 0.84 (0.70–1.01) | ||||
| Upper limb | 0.0153 | |||||
| No | 732/2095 | 1 | ||||
| Yes | 45/179 | 0.69 (0.51–0.93) | ||||
| Trunk wall | 0.7757 | |||||
| No | 674/1968 | 1 | ||||
| Yes | 103/306 | 0.97 (0.79–1.19) | ||||
| Head and neck | 0.1194 | |||||
| No | 731/2099 | 1 | ||||
| Yes | 46/175 | 0.79 (0.59–1.06) | ||||
| Internal trunk | <0.0001 | <0.0001 | ||||
| No | 588/1815 | 1 | 558/1718 | 1 | ||
| Yes | 189/459 | 1.46 (1.24–1.72) | 179/434 | 1.49 (1.23–1.80) | ||
| Metastatic at diagnostic | <0.0001 | <0.0001 | ||||
| No | 542/1819 | 1 | 541/1817 | 1 | ||
| Yes | 199/340 | 2.95 (2.50–3.47) | 196/335 | 2.98 (2.50–3.56) | ||
| GeoClasH classification of municipalities | 0.2455 | |||||
| Wealthy metropolitan areas | 148/468 | 1 | ||||
| Precarious population districts | 414/1188 | 1.23 (1.02–1.48) | ||||
| Residential outskirts | 108/321 | 1.20 (0.93–1.54) | ||||
| Agricultural and industrial plains | 72/193 | 1.30 (0.98–1.72) | ||||
| Rural margins | 39/111 | 1.23 (0.86–1.75) | ||||
| European Deprivation Index (quintiles) | 0.8172 | |||||
| ≤−1.4 (least deprived) | 159/462 | 1 | ||||
| ]−1.4; 1.7] | 174/468 | 1.10 (0.89–1.37) | ||||
| ]1.7; 5.5] | 160/457 | 1.05 (0.84–1.31) | ||||
| ]5.5; 8.8] | 145/452 | 0.97 (0.77–1.21) | ||||
| >8.8 (most deprived) | 143/442 | 1.02 (0.82–1.28) | ||||
| Travel time to the closest clinical sarcoma reference center (in minutes, quintiles) | 0.8190 | |||||
| ≤30 | 158/467 | 1 | ||||
| ]30; 56] | 153/440 | 0.97 (0.78–1.21) | ||||
| ]56; 78.5] | 163/451 | 1.09 (0.87–1.35) | ||||
| ]78.5; 102] | 147/467 | 0.96 (0.77–1.20) | ||||
| >102 | 160/456 | 1.02 (0.82–1.27) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fayet, Y.; Chevreau, C.; Decanter, G.; Dalban, C.; Meeus, P.; Carrère, S.; Haddag-Miliani, L.; Le Loarer, F.; Causeret, S.; Orbach, D.; et al. No Geographical Inequalities in Survival for Sarcoma Patients in France: A Reference Networks’ Outcome? Cancers 2022, 14, 2620. https://doi.org/10.3390/cancers14112620
Fayet Y, Chevreau C, Decanter G, Dalban C, Meeus P, Carrère S, Haddag-Miliani L, Le Loarer F, Causeret S, Orbach D, et al. No Geographical Inequalities in Survival for Sarcoma Patients in France: A Reference Networks’ Outcome? Cancers. 2022; 14(11):2620. https://doi.org/10.3390/cancers14112620
Chicago/Turabian StyleFayet, Yohan, Christine Chevreau, Gauthier Decanter, Cécile Dalban, Pierre Meeus, Sébastien Carrère, Leila Haddag-Miliani, François Le Loarer, Sylvain Causeret, Daniel Orbach, and et al. 2022. "No Geographical Inequalities in Survival for Sarcoma Patients in France: A Reference Networks’ Outcome?" Cancers 14, no. 11: 2620. https://doi.org/10.3390/cancers14112620
APA StyleFayet, Y., Chevreau, C., Decanter, G., Dalban, C., Meeus, P., Carrère, S., Haddag-Miliani, L., Le Loarer, F., Causeret, S., Orbach, D., Kind, M., Le Nail, L. -R., Ferron, G., Labrosse, H., Chaigneau, L., Bertucci, F., Ruzic, J. -C., Le Brun Ly, V., Farsi, F., ... Blay, J. -Y. (2022). No Geographical Inequalities in Survival for Sarcoma Patients in France: A Reference Networks’ Outcome? Cancers, 14(11), 2620. https://doi.org/10.3390/cancers14112620