
Tropomyosin-Related Kinase Fusions in Gastrointestinal Stromal Tumors

 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Treatment
2.3. KIT and PDGFRA Analysis
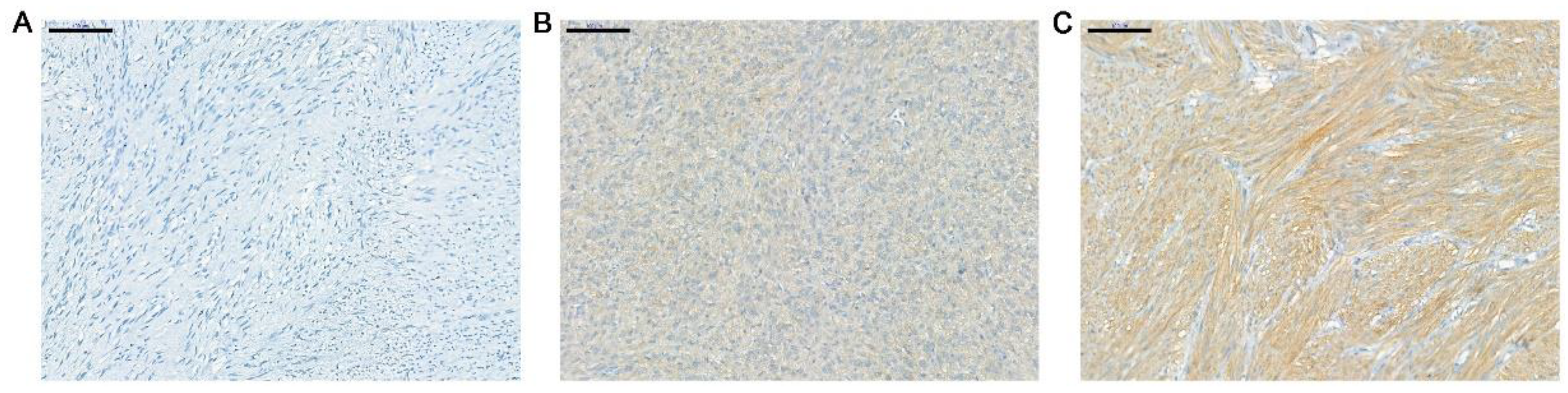
2.4. IHC for TRK Expression
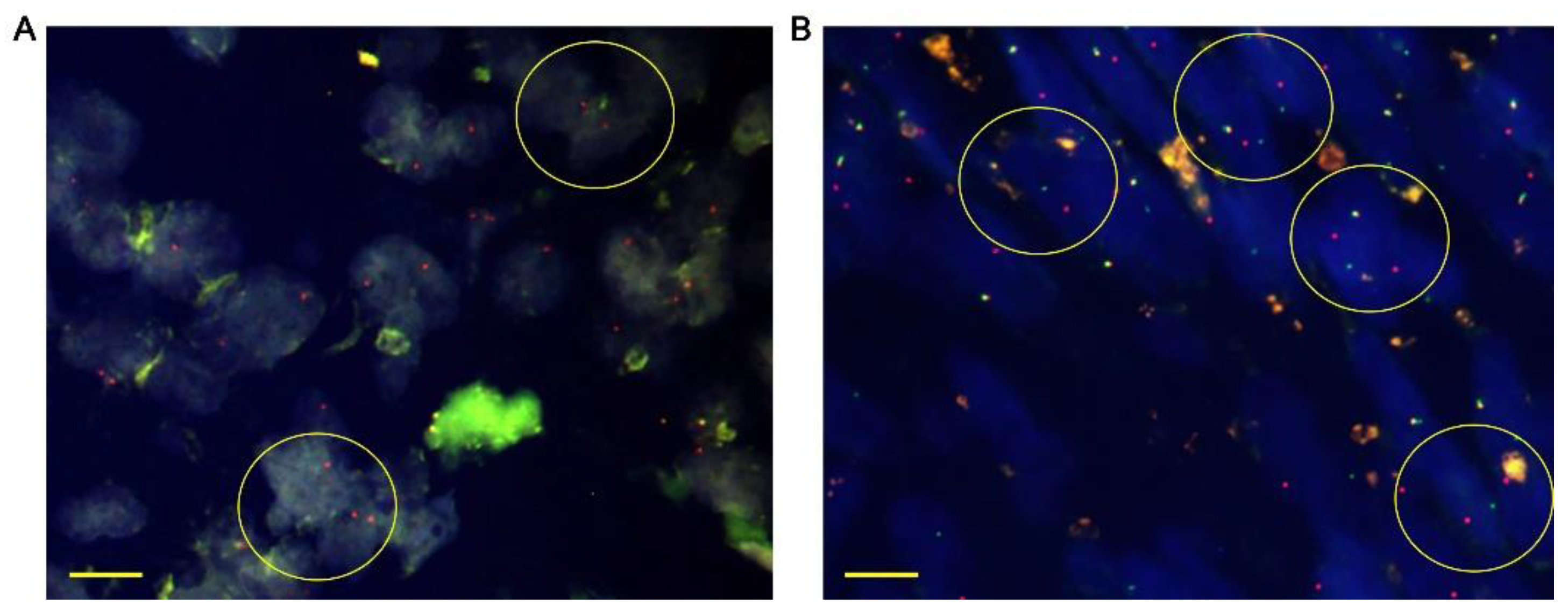
2.5. FISH
3. Results
3.1. Patient Characteristics and Treatment
3.2. TRK Expression in KIT WT GISTs
3.3. NTRK Fusion Analyses
3.4. Characteristics of the Five Patients Harboring NTRK Fusions
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Corless, C.L. Gastrointestinal stromal tumors: What do we know now? Mod. Pathol. 2014, 27 (Suppl. S1), S1–S16. [Google Scholar] [CrossRef] [PubMed]
- Ducimetiere, F.; Lurkin, A.; Ranchere-Vince, D.; Decouvelaere, A.V.; Peoch, M.; Istier, L.; Chalabreysse, P.; Muller, C.; Alberti, L.; Bringuier, P.P.; et al. Incidence of sarcoma histotypes and molecular subtypes in a prospective epidemiological study with central pathology review and molecular testing. PLoS ONE 2011, 6, e20294. [Google Scholar] [CrossRef] [PubMed]
- Von Mehren, M.; Joensuu, H. Gastrointestinal stromal tumors. J. Clin. Oncol. 2018, 36, 136–143. [Google Scholar] [CrossRef] [PubMed]
- Corless, C.L.; Fletcher, J.A.; Heinrich, M.C. Biology of gastrointestinal stromal tumors. J. Clin. Oncol. 2004, 22, 3813–3825. [Google Scholar] [CrossRef]
- Brcic, I.; Argyropoulos, A.; Liegl-Atzwanger, B. Update on Molecular Genetics of Gastrointestinal Stromal Tumors. Diagnostics 2021, 11, 194. [Google Scholar] [CrossRef]
- Von Mehren, M.; Randall, R.L.; Benjamin, R.S.; Boles, S.; Bui, M.M.; Ganjoo, K.N.; George, S.; Gonzalez, R.J.; Heslin, M.J.; Kane, J.M.; et al. Soft tissue sarcoma, version 2.2018, NCCN clinical practice guidelines in oncology. J. Natl. Compr. Cancer Netw. 2018, 16, 536–563. [Google Scholar] [CrossRef]
- Kheder, E.S.; Hong, D.S. Emerging Targeted Therapy for Tumors with NTRK Fusion Proteins. Clin. Cancer Res. 2018, 24, 5807–5814. [Google Scholar] [CrossRef]
- Brenca, M.; Rossi, S.; Polano, M.; Gasparotto, D.; Zanatta, L.; Racanelli, D.; Valori, L.; Lamon, S.; Dei Tos, A.P.; Maestro, R. Transcriptome sequencing identifies ETV6-NTRK3 as a gene fusion involved in GIST. J. Pathol. 2016, 238, 543–549. [Google Scholar] [CrossRef]
- Shi, E.; Chmielecki, J.; Tang, C.M.; Wang, K.; Heinrich, M.C.; Kang, G.; Corless, C.L.; Hong, D.; Fero, K.E.; Murphy, J.D.; et al. FGFR1 and NTRK3 actionable alterations in “Wild-Type” gastrointestinal stromal tumors. J. Transl. Med. 2016, 14, 339. [Google Scholar] [CrossRef]
- Drilon, A.; Laetsch, T.W.; Kummar, S.; DuBois, S.G.; Lassen, U.N.; Demetri, G.D.; Nathenson, M.; Doebele, R.C.; Farago, A.F.; Pappo, A.S.; et al. Efficacy of Larotrectinib in TRK Fusion-Positive Cancers in Adults and Children. N. Engl. J. Med. 2018, 378, 731–739. [Google Scholar] [CrossRef]
- Doebele, R.C.; Drilon, A.; Paz-Ares, L.; Siena, S.; Shaw, A.T.; Farago, A.F.; Blakely, C.M.; Seto, T.; Cho, B.C.; Tosi, D.; et al. Entrectinib in patients with advanced or metastatic NTRK fusion-positive solid tumours: Integrated analysis of three phase 1–2 trials. Lancet Oncol. 2020, 21, 271–282. [Google Scholar] [CrossRef]
- Tang, Z.; Wang, L.; Tang, G.; Medeiros, L.J. Fluorescence in Situ Hybridization (FISH) for Detecting Anaplastic Lymphoma Kinase (ALK) Rearrangement in Lung Cancer: Clinically Relevant Technical Aspects. Int. J. Mol. Sci. 2019, 20, 3939. [Google Scholar] [CrossRef] [PubMed]
- Lange, A.M.; Lo, H.W. Inhibiting TRK Proteins in Clinical Cancer Therapy. Cancers 2018, 10, 105. [Google Scholar] [CrossRef]
- Pulciani, S.; Santos, E.; Lauver, A.V.; Long, L.K.; Aaronson, S.A.; Barbacid, M. Oncogenes in solid human tumours. Nature 1982, 300, 539–542. [Google Scholar] [CrossRef] [PubMed]
- Vaishnavi, A.; Capelletti, M.; Le, A.T.; Kako, S.; Butaney, M.; Ercan, D.; Mahale, S.; Davies, K.D.; Aisner, D.L.; Pilling, A.B.; et al. Oncogenic and drug-sensitive NTRK1 rearrangements in lung cancer. Nat. Med. 2013, 19, 1469–1472. [Google Scholar] [CrossRef]
- Greco, A.; Miranda, C.; Pierotti, M.A. Rearrangements of NTRK1 gene in papillary thyroid carcinoma. Mol. Cell. Endocrinol. 2010, 321, 44–49. [Google Scholar] [CrossRef]
- Sartore-Bianchi, A.; Ardini, E.; Bosotti, R.; Amatu, A.; Valtorta, E.; Somaschini, A.; Raddrizzani, L.; Palmeri, L.; Banfi, P.; Bonazzina, E.; et al. Sensitivity to Entrectinib Associated With a Novel LMNA-NTRK1 Gene Fusion in Metastatic Colorectal Cancer. J. Natl. Cancer Inst. 2016, 108. [Google Scholar] [CrossRef]
- Tognon, C.; Knezevich, S.R.; Huntsman, D.; Roskelley, C.D.; Melnyk, N.; Mathers, J.A.; Becker, L.; Carneiro, F.; MacPherson, N.; Horsman, D.; et al. Expression of the ETV6-NTRK3 gene fusion as a primary event in human secretory breast carcinoma. Cancer Cell 2002, 2, 367–376. [Google Scholar] [CrossRef]
- Bishop, J.A.; Yonescu, R.; Batista, D.; Begum, S.; Eisele, D.W.; Westra, W.H. Utility of mammaglobin immunohistochemistry as a proxy marker for the ETV6-NTRK3 translocation in the diagnosis of salivary mammary analogue secretory carcinoma. Hum. Pathol. 2013, 44, 1982–1988. [Google Scholar] [CrossRef]
- Cocco, E.; Scaltriti, M.; Drilon, A. NTRK fusion-positive cancers and TRK inhibitor therapy. Nat. Rev. Clin. Oncol. 2018, 15, 731–747. [Google Scholar] [CrossRef]
- Vaishnavi, A.; Le, A.T.; Doebele, R.C. TRKing down an old oncogene in a new era of targeted therapy. Cancer Discov. 2015, 5, 25–34. [Google Scholar] [CrossRef] [PubMed]
- Hong, D.S.; DuBois, S.G.; Kummar, S.; Farago, A.F.; Albert, C.M.; Rohrberg, K.S.; van Tilburg, C.M.; Nagasubramanian, R.; Berlin, J.D.; Federman, N.; et al. Larotrectinib in patients with TRK fusion-positive solid tumours: A pooled analysis of three phase 1/2 clinical trials. Lancet Oncol. 2020, 21, 531–540. [Google Scholar] [CrossRef]
- Marchio, C.; Scaltriti, M.; Ladanyi, M.; Iafrate, A.J.; Bibeau, F.; Dietel, M.; Hechtman, J.F.; Troiani, T.; Lopez-Rios, F.; Douillard, J.Y.; et al. ESMO recommendations on the standard methods to detect NTRK fusions in daily practice and clinical research. Ann. Oncol. 2019, 30, 1417–1427. [Google Scholar] [CrossRef] [PubMed]
- Solomon, J.P.; Benayed, R.; Hechtman, J.F.; Ladanyi, M. Identifying patients with NTRK fusion cancer. Ann. Oncol. 2019, 30 (Suppl. S8), viii16–viii22. [Google Scholar] [CrossRef]
- Penault-Llorca, F.; Rudzinski, E.R.; Sepulveda, A.R. Testing algorithm for identification of patients with TRK fusion cancer. J. Clin. Pathol. 2019, 72, 460–467. [Google Scholar] [CrossRef]
- Chiang, S.; Cotzia, P.; Hyman, D.M.; Drilon, A.; Tap, W.D.; Zhang, L.; Hechtman, J.F.; Frosina, D.; Jungbluth, A.A.; Murali, R. NTRK fusions define a novel uterine sarcoma subtype with features of fibrosarcoma. Am. J. Surg. Pathol. 2018, 42, 791. [Google Scholar] [CrossRef]
- Lezcano, C.; Shoushtari, A.N.; Ariyan, C.; Hollmann, T.J.; Busam, K.J. Primary and metastatic melanoma with NTRK-Fusions. Am. J. Surg. Pathol. 2018, 42, 1052. [Google Scholar] [CrossRef]
- Milione, M.; Ardini, E.; Christiansen, J.; Valtorta, E.; Veronese, S.; Bosotti, R.; Pellegrinelli, A.; Testi, A.; Pietrantonio, F.; Fucà, G. Identification and characterization of a novel SCYL3-NTRK1 rearrangement in a colorectal cancer patient. Oncotarget 2017, 8, 55353. [Google Scholar] [CrossRef]
- Castillon, M.; Kammerer-Jacquet, S.F.; Cariou, M.; Costa, S.; Conq, G.; Samaison, L.; Douet-Guilbert, N.; Marcorelles, P.; Doucet, L.; Uguen, A. Fluorescent In Situ Hybridization Must be Preferred to pan-TRK Immunohistochemistry to Diagnose NTRK3-rearranged Fastrointestinal Stromal Tumors (GIST). Appl. Immunohistochem. Mol. Morphol. 2021, 29, 626–634. [Google Scholar] [CrossRef]
- Atiq, M.A.; Davis, J.L.; Hornick, J.L.; Dickson, B.C.; Fletcher, C.D.M.; Fletcher, J.A.; Folpe, A.L.; Mariño-Enríquez, A. Mesenchymal tumors of the gastrointestinal tract with NTRK rearrangements: A clinicopathological, immunophenotypic, and molecular study of eight cases, emphasizing their distinction from gastrointestinal stromal tumor (GIST). Mod. Pathol. 2021, 34, 95–103. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Total (n = 31) N (%) | NTRK Fusion (n = 5) | NTRK Wild Type (n = 26) | p-Value |
|---|---|---|---|---|
| Age | ||||
| Median (range) | 56 (33–92) | 61 (33–92) | 53 (37–84) | 0.163 |
| Sex | - | - | - | 1000 |
| Male | 14 (45.2) | 2 (40.0) | 12 (46.2) | - |
| Female | 17 (54.8) | 3 (60.0) | 14 (53.8) | - |
| Tumor size (cm) | - | - | - | - |
| Median ± SD | 8.2 ± 5.3 | 3.9 ± 6.5 | 6.0 ± 5.2 | 0.410 |
| Tumor location | - | - | - | 0.028 |
| Abdominal wall | 1 (0.3) | 0 (0.0) | 1 (3.8) | - |
| Stomach | 14 (45.1) | 1 (20.0) | 14 (53.8) | - |
| Small bowel | 11 (35.4) | 2 (40.0) | 6 (23.1) | - |
| Descending colon | 1 (0.3) | 0 (0.0) | 1 (3.8) | - |
| Rectum | 4 (12.9) | 2 (40.0) | 4 (15.4) | - |
| Tumor size, groups (cm) ◇ | - | - | - | 1000 |
| ≤5 | 14 (50.0) | 3 (60.0) | 11 (47.8) | - |
| >5 | 14 (50.0) | 2 (40.0) | 12 (52.2) | -- |
| Mitotic rate ◐ (no. of mitoses/50 HPFs *) | -- | 0.711 | ||
| ≤5 | 11 (50.0) | 2 (40.0) | 12 (52.2) | - |
| >5 | 16 (50.0) | 3 (60.0) | 10 (43.5) | - |
| Disease status | - | - | - | 0.859 |
| No evidence of disease | 21 (67.7) | 5 (100.0) | 16 (61.5) | - |
| on anticancer treatment | 3 (9.7) | 0 (0.0) | 3 (11.5) | - |
| Unknown | 3 (9.7) | 0 (0.0) | 3 (11.5) | - |
| Dead | 4 (12.9) | 0 (0.0) | 4 (15.4) | - |
| Risk of metastasis ◈ | - | - | - | 0.253 |
| Low | 8 (25.8) | 1 (20.0) | 7 (26.9) | - |
| Intermediate | 3 (9.7) | 0 (0.0) | 3 (11.5) | - |
| High | 17 (54.8) | 4 (80.0) | 13 (50.0) | - |
| Not assessable | 3 (9.7) | 0 (0.0) | 3 (11.5) | - |
| Surgical treatment | - | - | - | 1000 |
| Yes | 28 (90.3) | 5 (100.0) | 23 (88.5) | - |
| No | 3 (9.7) | 0 (0.0) | 3 (11.5) | - |
| pan-TRK IHC | Intensity of Staining | H-Score | |||
|---|---|---|---|---|---|
| 0 | 1 | 2 | 3 | - | |
| Proportion of staining (%) | 20% | 80% | - | - | 80 |
| 20% | 80% | - | - | 80 | |
| 90% | - | 10% | - | 20 | |
| 70% | - | 30% | - | 60 | |
| 70% | - | 30% | - | 60 | |
| Patients (#1–#5) | #1 | #2 | #3 | #4 | #5 |
|---|---|---|---|---|---|
| Age (years) | 44 | 45 | 65 | 61 | 43 |
| Sex | F | M | F | F | M |
| Location | Rectum | Duodenum | Stomach | Jejunum | Rectum |
| Mitotic rate (no. of mitoses/50 HPFs * | 17 | 1 | 70 | 12 | 0 |
| Size (cm) | 2.8 | 1.7 | 17.0 | 3.9 | 11.0 |
| Surgery (yes or no) | yes | yes | yes | yes | yes |
| Follow-up period (years) | 11 | 6 | 8 | 4 | 3 |
| NTRK fusion by FISH | NRTK1 | NRTK3 | NRTK1 | NRTK1 | NTRK3 |
| Imatinib | No | No | Adjuvant | Adjuvant | No |
| Disease/survival status | DDP | NED | DDP | NED | NED |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.H.; Shin, S.-J.; Choe, E.-A.; Kim, J.; Hyung, W.J.; Kim, H.S.; Jung, M.; Beom, S.-H.; Kim, T.I.; Ahn, J.B.; et al. Tropomyosin-Related Kinase Fusions in Gastrointestinal Stromal Tumors. Cancers 2022, 14, 2659. https://doi.org/10.3390/cancers14112659
Lee JH, Shin S-J, Choe E-A, Kim J, Hyung WJ, Kim HS, Jung M, Beom S-H, Kim TI, Ahn JB, et al. Tropomyosin-Related Kinase Fusions in Gastrointestinal Stromal Tumors. Cancers. 2022; 14(11):2659. https://doi.org/10.3390/cancers14112659
Chicago/Turabian StyleLee, Ji Hyun, Su-Jin Shin, Eun-Ah Choe, Jungyoun Kim, Woo Jin Hyung, Hyo Song Kim, Minkyu Jung, Seung-Hoon Beom, Tae Il Kim, Joong Bae Ahn, and et al. 2022. "Tropomyosin-Related Kinase Fusions in Gastrointestinal Stromal Tumors" Cancers 14, no. 11: 2659. https://doi.org/10.3390/cancers14112659
APA StyleLee, J. H., Shin, S. -J., Choe, E. -A., Kim, J., Hyung, W. J., Kim, H. S., Jung, M., Beom, S. -H., Kim, T. I., Ahn, J. B., Chung, H. C., & Shin, S. J. (2022). Tropomyosin-Related Kinase Fusions in Gastrointestinal Stromal Tumors. Cancers, 14(11), 2659. https://doi.org/10.3390/cancers14112659