
Acute Impact of Cancer Treatment on Head and Neck Cancer Patients: FIT4TREATMENT

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
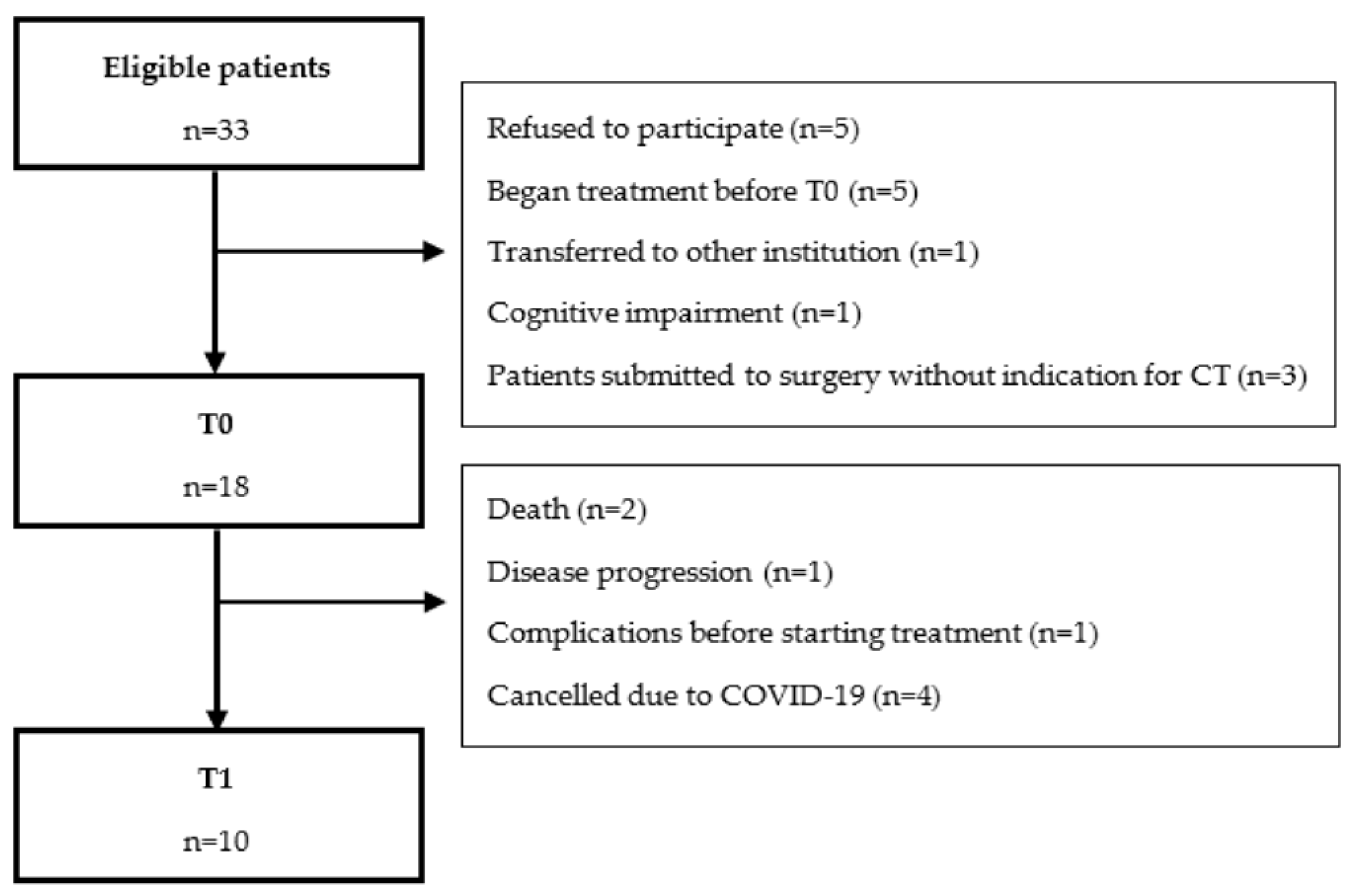
2.1. Study Population
2.2. Design
2.3. Endpoints
2.3.1. Health-Related Quality of Life
2.3.2. Nutritional Status and Body Composition
2.3.3. Physical Function
2.3.4. Dysphagia
2.3.5. Cognitive Function
2.3.6. Exercise Training Preferences
2.4. Statistical Analysis
3. Results
3.1. Baseline Characterization
3.1.1. Health-Related Quality of Life
3.1.2. Physical Function
3.1.3. Nutritional Status and Body Composition
3.1.4. Cognitive Function
3.1.5. Dysphagia
3.1.6. Exercise Preferences
3.2. Acute Effects of Radical Chemoradiotherapy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Licitra, L.; Karamouzis, M.V. ESMO Essentials for Clinicians Head Neck Cancers; ESMO Press: Lugano, Switzerland, 2017. [Google Scholar]
- Khleif, S.N.; Rixe, O.; Skeel, R.T. Carcinomas of the Head and Neck. In Skeel’s Handbook of Cancer Therapy, 9th ed.; Kluwer, W., Ed.; Lippincot Williams & Wilkins: Philadelphia, PA, USA, 2016. [Google Scholar]
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology Head and Neck Cancers (version 2.2021). Available online: http://www.nccn.org/professionals/physician_gls/pdf/head-and-neck.pdf (accessed on 6 September 2021).
- Machiels, J.P.; Rene Leemans, C.; Golusinski, W.; Grau, C.; Licitra, L.; Gregoire, V. Squamous cell carcinoma of the oral cavity, larynx, oropharynx and hypopharynx: EHNS-ESMO-ESTRO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2020, 31, 1462–1475. [Google Scholar] [CrossRef] [PubMed]
- Kantarjian, H.M.; Wolff, R.A. Section V—Head and Neck Cancer. In The MD Anderson Manual of Medical Oncology; McGraw Hill: New York, NY, USA, 2016. [Google Scholar]
- Argiris, A.; Karamouzis, M.V.; Raben, D.; Ferris, R.L. Head and neck cancer. Lancet 2008, 371, 1695–1709. [Google Scholar] [CrossRef]
- Capozzi, L.C.; Lau, H.; Reimer, R.A.; McNeely, M.; Giese-Davis, J.; Culos-Reed, S.N. Exercise and nutrition for head and neck cancer patients: A patient oriented, clinic-supported randomized controlled trial. BMC Cancer 2012, 12, 446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michaelsen, S.H.; Grønhøj, C.; Michaelsen, J.H.; Friborg, J.; von Buchwald, C. Quality of life in survivors of oropharyngeal cancer: A systematic review and meta-analysis of 1366 patients. Eur. J. Cancer 2017, 78, 91–102. [Google Scholar] [CrossRef]
- Guan, J.; Zhang, Y.; Li, Q.; Zhang, Y.; Li, L.; Chen, M.; Xiao, N.; Chen, L. A meta-analysis of weekly cisplatin versus three weekly cisplatin chemotherapy plus concurrent radiotherapy (CRT) for advanced head and neck cancer (HNC). Oncotarget 2016, 7, 70185–70193. [Google Scholar] [CrossRef] [Green Version]
- Citak, E.; Tulek, Z.; Uzel, O. Nutritional status in patients with head and neck cancer undergoing radiotherapy: A longitudinal study. Support. Care Cancer 2018, 27, 239–247. [Google Scholar] [CrossRef]
- Anbumani, S.; Lohith, A.S.G.; Somarat, B.R.B. Impact of Concurrent Chemoradiation on Quality of Life in Locally Advanced Head and Neck Cancers. Int. Clin. Pathol. J. 2017, 4, 4–11. [Google Scholar] [CrossRef] [Green Version]
- Gerritsen, J.K.W.; Vincent, A.J.P.E. Exercise improves quality of life in patients with cancer: A systematic review and meta-analysis of randomised controlled trials. Br. J. Sports Med. 2015, 50, 796–803. [Google Scholar] [CrossRef]
- Zhao, S.G.; Alexander, N.B.; Djuric, Z.; Zhou, J.; Tao, Y.; Schipper, M.; Feng, F.Y.; Eisbruch, A.; Worden, F.P.; Strath, S.J.; et al. Maintaining physical activity during head and neck cancer treatment: Results of a pilot controlled trial. Head Neck 2016, 38, E1086–E1096. [Google Scholar] [CrossRef] [Green Version]
- Samuel, S.R.; Maiya, A.G.; Fernandes, D.J.; Guddattu, V.; Saxena, P.U.P.; Kurian, J.R.; Lin, P.J.; Mustian, K.M. Effectiveness of exercise-based rehabilitation on functional capacity and quality of life in head and neck cancer patients receiving chemo-radiotherapy. Support. Care Cancer 2019, 27, 3913–3920. [Google Scholar] [CrossRef]
- Lin, K.Y.; Cheng, H.C.; Yen, C.J.; Hung, C.H.; Huang, Y.T.; Yang, H.L.; Cheng, W.T.; Tsai, K.L. Effects of Exercise in Patients Undergoing Chemotherapy for Head and Neck Cancer: A Pilot Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2021, 18, 1291. [Google Scholar] [CrossRef] [PubMed]
- van der Laan, H.P.; Van den Bosch, L.; Schuit, E.; Steenbakkers, R.; van der Schaaf, A.; Langendijk, J.A. Impact of radiation-induced toxicities on quality of life of patients treated for head and neck cancer. Radiother. Oncol. 2021, 160, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Rogers, L.Q.; Anton, P.M.; Fogleman, A.; Hopkins-Price, P.; Verhulst, S.; Rao, K.; Malone, J.; Robbs, R.; Courneya, K.S.; Nanavati, P.; et al. Pilot, randomized trial of resistance exercise during radiation therapy for head and neck cancer. Head Neck 2013, 35, 1178–1188. [Google Scholar] [CrossRef] [PubMed]
- Lonbro, S.; Dalgas, U.; Primdahl, H.; Johansen, J.; Nielsen, J.L.; Aagaard, P.; Hermann, A.P.; Overgaard, J.; Overgaard, K. Progressive resistance training rebuilds lean body mass in head and neck cancer patients after radiotherapy—results from the randomized DAHANCA 25B trial. Radiother. Oncol. 2013, 108, 314–319. [Google Scholar] [CrossRef]
- van Rijn-Dekker, M.I.; van den Bosch, L.; van den Hoek, J.G.M.; Bijl, H.P.; van Aken, E.S.M.; van der Hoorn, A.; Oosting, S.F.; Halmos, G.B.; Witjes, M.J.H.; van der Laan, H.P.; et al. Impact of sarcopenia on survival and late toxicity in head and neck cancer patients treated with radiotherapy. Radiother. Oncol. 2020, 147, 103–110. [Google Scholar] [CrossRef]
- Surov, A.; Pech, M.; Gessner, D.; Mikusko, M.; Fischer, T.; Alter, M.; Wienke, A. Low skeletal muscle mass is a predictor of treatment related toxicity in oncologic patients. A meta-analysis. Clin. Nutr. 2021, 40, 5298–5310. [Google Scholar] [CrossRef]
- O’Doherty, A.F.; West, M.; Jack, S.; Grocott, M.P. Preoperative aerobic exercise training in elective intra-cavity surgery: A systematic review. Br. J. Anaesth. 2013, 110, 679–689. [Google Scholar] [CrossRef] [Green Version]
- Pais-Ribeiro, J.; Pinto, C.; Santos, C. Validation study of the portuguese version of the QLC-C30-V.3. Psicol. Saúde Doença 2008, 1, 89–102. [Google Scholar]
- Singer, S.; Amdal, C.D.; Hammerlid, E.; Tomaszewska, I.M.; Castro Silva, J.; Mehanna, H.; Santos, M.; Inhestern, J.; Brannan, C.; Yarom, N.; et al. International validation of the revised European Organisation for Research and Treatment of Cancer Head and Neck Cancer Module, the EORTC QLQ-HN43: Phase IV. Head Neck 2019, 41, 1725–1737. [Google Scholar] [CrossRef]
- Campos, J.A.D.B.; do Prado, C.D. Cross-cultural adaptation of the Portuguese version of the patient-generated subjective global assessment. Nutr. Hosp. 2012, 27, 583–589. [Google Scholar] [CrossRef]
- Bauer, J.; Capra, S.; Ferguson, M. Use of the scored Patient-Generated Subjective Global Assessment (PG-SGA) as a nutrition assessment tool in patients with cancer. Eur. J. Clin. Nutr. 2002, 56, 779–785. [Google Scholar] [CrossRef] [PubMed]
- Ottery, F.D. Definition of Standardized Nutriotional Assessment and Interventional Pathways in Oncology. Nutrition 1996, 12, S15–S19. [Google Scholar] [CrossRef]
- American Thoracic Society. ATS Statement: Guidelines for the Six-Minute Walk Test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [Google Scholar] [CrossRef] [PubMed]
- Queirós, A.; Moreira, S.; Silva, A.; Costa, R.; Lains, J. Contributo para a Adaptação e Validação da Eat Assessment Tool (EAT-10) e da Functional Oral Intake Scale (FOIS). Rev. Soc. Port. De Med. Física E Reabil. 2013, 24, 25–30. [Google Scholar]
- Duro, D.; Simoes, M.R.; Ponciano, E.; Santana, I. Validation studies of the Portuguese experimental version of the Montreal Cognitive Assessment (MoCA): Confirmatory factor analysis. J. Neurol. 2010, 257, 728–734. [Google Scholar] [CrossRef]
- Rogers, S.N.; Waylen, A.E.; Thomas, S.; Penfold, C.; Pring, M.; Waterboer, T.; Pawlita, M.; Hurley, K.; Ness, A.R. Quality of life, cognitive, physical and emotional function at diagnosis predicts head and neck cancer survival: Analysis of cases from the Head and Neck 5000 study. Eur. Arch. Oto-Rhino-Laryngol. 2020, 277, 1515–1523. [Google Scholar] [CrossRef] [Green Version]
- Siddiqui, F.; Pajak, T.F.; Watkins-Bruner, D.; Konski, A.A.; Coyne, J.C.; Gwede, C.K.; Garden, A.S.; Spencer, S.A.; Jones, C.; Movsas, B. Pretreatment quality of life predicts for locoregional control in head and neck cancer patients: A radiation therapy oncology group analysis. Int. J. Radiat. Oncol. Biol. Phys. 2008, 70, 353–360. [Google Scholar] [CrossRef]
- van Nieuwenhuizen, A.J.; Buffart, L.M.; Brug, J.; Leemans, C.R.; Verdonck-de Leeuw, I.M. The association between health related quality of life and survival in patients with head and neck cancer: A systematic review. Oral Oncol. 2015, 51, 1–11. [Google Scholar] [CrossRef]
- Yang, C.J.; Roh, J.L.; Kim, M.J.; Lee, S.W.; Kim, S.B.; Choi, S.H.; Nam, S.Y.; Kim, S.Y. Pretreatment quality of life as a prognostic factor for early survival and functional outcomes in patients with head and neck cancer. Qual. Life Res. 2016, 25, 165–174. [Google Scholar] [CrossRef]
- Ribeiro, I.P.; Lopes, T.; Pedro, N.; Barroso, L.; Costa, R.; Carreira, I.M.; Ribeiro, F. Should sitting time be a treatment target in head and neck cancer patients receiving curative treatment? Oral Oncol. 2022, 124, 105418. [Google Scholar] [CrossRef]
- Connor, N.P.; Cohen, S.B.; Kammer, R.E.; Sullivan, P.A.; Brewer, K.A.; Hong, T.S.; Chappell, R.J.; Harari, P.M. Impact of conventional radiotherapy on health-related quality of life and critical functions of the head and neck. Int. J. Radiat. Oncol. Biol. Phys. 2006, 65, 1051–1062. [Google Scholar] [CrossRef] [PubMed]
- Majid, A.; Sayeed, B.Z.; Khan, M.; Lakhani, M.; Saleem, M.M.; Rajani, H.; Ramesh, P.; Hashmani, N.; Zia, M.; Abid, H.; et al. Assessment and Improvement of Quality of Life in Patients Undergoing Treatment for Head and Neck Cancer. Cureus 2017, 9, e1215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karimi, A.M.; Gairola, M.; Ahlawat, P.; Tandon, S.; Pal, M.; Sachdeva, N.; Sharief, M.I.; Dobriyal, K. Health-related quality of life assessment for head-and-neck cancer patients during and at 3 months after radiotherapy—A prospective, analytical questionnaire-based study. Natl. J. Maxillofac. Surg. 2019, 10, 134–140. [Google Scholar] [CrossRef] [PubMed]
- Klein, J.; Livergant, J.; Ringash, J. Health related quality of life in head and neck cancer treated with radiation therapy with or without chemotherapy: A systematic review. Oral Oncol. 2014, 50, 254–262. [Google Scholar] [CrossRef] [PubMed]
- So, W.K.; Chan, R.J.; Chan, D.N.; Hughes, B.G.; Chair, S.Y.; Choi, K.C.; Chan, C.W. Quality-of-life among head and neck cancer survivors at one year after treatment—A systematic review. Eur. J. Cancer 2012, 48, 2391–2408. [Google Scholar] [CrossRef]
- Jereczek-Fossa, B.A.; Santoro, L.; Alterio, D.; Franchi, B.; Fiore, M.R.; Fossati, P.; Kowalczyk, A.; Canino, P.; Ansarin, M.; Orecchia, R. Fatigue during head-and-neck radiotherapy: Prospective study on 117 consecutive patients. Int. J. Radiat. Oncol. Biol. Phys. 2007, 68, 403–415. [Google Scholar] [CrossRef]
- Williams, A.M.; Lindholm, J.; Cook, D.; Siddiqui, F.; Ghanem, T.A.; Chang, S.S. Association Between Cognitive Function and Quality of Life in Patients With Head and Neck Cancer. JAMA Otolaryngol. Head Neck Surg. 2017, 143, 1228–1235. [Google Scholar] [CrossRef]
- Meyers, C.A.; Hess, K.R.; Yung, W.K.A.; Levin, V.A. Cognitive Function as a Predictor of Survival in Patients with Recurrent Malignant Glioma. J. Clin. Oncol. 2000, 18, 646. [Google Scholar] [CrossRef]
- Zer, A.; Pond, G.R.; Razak, A.R.A.; Tirona, K.; Gan, H.K.; Chen, E.X.; O’Sullivan, B.; Waldron, J.; Goldstein, D.P.; Weinreb, I.; et al. Association of Neurocognitive Deficits with Radiotherapy or Chemoradiotherapy for Patients with Head and Neck Cancer. JAMA Otolaryngol. Head Neck Surg. 2018, 144, 71–79. [Google Scholar] [CrossRef] [Green Version]
- Hopkinson, N.S.; Nickol, A.H.; Payne, J.; Hawe, E.; Man, W.D.; Moxham, J.; Montgomery, H.; Polkey, M.I. Angiotensin converting enzyme genotype and strength in chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2004, 170, 395–399. [Google Scholar] [CrossRef]
- Rogers, L.Q.; Courneya, K.S.; Carter, S.J.; Anton, P.M.; Verhulst, S.; Vicari, S.K.; Robbs, R.S.; McAuley, E. Effects of a multicomponent physical activity behavior change intervention on breast cancer survivor health status outcomes in a randomized controlled trial. Breast Cancer Res. Treat. 2016, 159, 283–291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Douma, J.A.J.; Verdonck-de Leeuw, I.M.; Leemans, C.R.; Jansen, F.; Langendijk, J.A.; Baatenburg de Jong, R.J.; Terhaard, C.H.J.; Takes, R.P.; Chinapaw, M.J.; Altenburg, T.M.; et al. Demographic, clinical and lifestyle-related correlates of accelerometer assessed physical activity and fitness in newly diagnosed patients with head and neck cancer. Acta. Oncol. 2020, 59, 342–350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baxi, S.S.; Schwitzer, E.; Jones, L.W. A review of weight loss and sarcopenia in patients with head and neck cancer treated with chemoradiation. Cancers Head Neck 2016, 1, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Findlay, M.; White, K.; Stapleton, N.; Bauer, J. Is sarcopenia a predictor of prognosis for patients undergoing radiotherapy for head and neck cancer? A meta-analysis. Clin. Nutr. 2021, 40, 1711–1718. [Google Scholar] [CrossRef]
- Pedruzzi, P.A.G.; Kowalski, L.P.; Nishimoto, I.N.; Oliveira, B.V.; Tironi, F.; Ramos, G.H.A. Analysis of Prognostic Factors in Patients with Oropharyngeal Squamous Cell Carcinoma Treated with Radiotherapy Alone or in Combination with Systemic Chemotherapy. Arch. Otolaryngol.–Head Neck Surg. 2008, 134, 1196–1204. [Google Scholar] [CrossRef] [Green Version]
- Langius, J.A.; Zandbergen, M.C.; Eerenstein, S.E.; van Tulder, M.W.; Leemans, C.R.; Kramer, M.H.; Weijs, P.J. Effect of nutritional interventions on nutritional status, quality of life and mortality in patients with head and neck cancer receiving (chemo)radiotherapy: A systematic review. Clin. Nutr. 2013, 32, 671–678. [Google Scholar] [CrossRef]
- Elting, L.S.; Cooksley, C.D.; Chambers, M.S.; Garden, A.S. Risk, outcomes, and costs of radiation-induced oral mucositis among patients with head-and-neck malignancies. Int. J. Radiat. Oncol. Biol. Phys. 2007, 68, 1110–1120. [Google Scholar] [CrossRef]
- Zhao, J.Z.; Zheng, H.; Li, L.Y.; Zhang, L.Y.; Zhao, Y.; Jiang, N. Predictors for Weight Loss in Head and Neck Cancer Patients Undergoing Radiotherapy: A Systematic Review. Cancer Nurs. 2015, 38, E37–E45. [Google Scholar] [CrossRef]
- Cheney, D.M.; Siddiqui, M.T.; Litts, J.K.; Kuhn, M.A.; Belafsky, P.C. The Ability of the 10-Item Eating Assessment Tool (EAT-10) to Predict Aspiration Risk in Persons with Dysphagia. Ann. Otol. Rhinol. Laryngol. 2015, 124, 351–354. [Google Scholar] [CrossRef]
- Ishii, R.; Kato, K.; Ohkoshi, A.; Sato, T.; Hirano, A.; Ogawa, T.; Katori, Y. Simultaneous evaluation of symptoms, swallowing functions, and patient-reported swallowing difficulties and their correlations with ingestion status during definitive chemoradiotherapy for oropharyngeal and hypopharyngeal cancer. Support. Care Cancer 2021, 29, 955–964. [Google Scholar] [CrossRef]
- Chauhan, N.S.; Samuel, S.R.; Meenar, N.; Saxena, P.P.; Keogh, J.W.L. Sarcopenia in male patients with head and neck cancer receiving chemoradiotherapy: A longitudinal pilot study. PeerJ 2020, 8, e8617. [Google Scholar] [CrossRef] [PubMed]
- Samuel, S.R.; Maiya, G.A.; Babu, A.S.; Vidyasagar, M.S. Effect of exercise training on functional capacity & quality of life in head & neck cancer patients receiving chemoradiotherapy. Indian J. Med. Res. 2013, 137, 515–520. [Google Scholar] [PubMed]
- Yen, C.J.; Hung, C.H.; Kao, C.L.; Tsai, W.M.; Chan, S.H.; Cheng, H.C.; Jheng, W.T.; Lu, Y.J.; Tsai, K.L. Multimodal exercise ameliorates exercise responses and body composition in head and neck cancer patients receiving chemotherapy. Support. Care Cancer 2019, 27, 4687–4695. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Total |
|---|---|
| Age in years—median (IQR) | 53.3 (51.8–65.5) |
| Gender, male—n (%) | 18 (100) |
ECOG-PS—n (%)
| 7 (38.9) 11 (61.1) |
Marital status—n (%)
| 5 (27.8) 13 (72.2) |
Education—n (%)
| 9 (50.0) 9 (50.0) |
Employment—n (%)
| 8 (44.4) 5 (27.8) 5 (27.8) |
Smoking status—n (%)
| 8 (44.4) 10 (55.6) |
Alcohol status—n (%)
| 1 (5.6) 7 (38.9) 10 (55.6) |
Primary tumour location—n (%)
| 2 (11.1) 7 (38.9) 9 (50.0) |
Stage—n (%)
| 1 (5.6) 12 (66.7) 5 (27.8) |
Treatment—n (%)
| 2 (11.1) 5 (27.8) 9 (50.0) 2 (11.1) |
| Characteristic | Total | |
|---|---|---|
| Median | IQR | |
| HRQoL—EORTC QLQ-C30 (score) | ||
| Global health status | 70.8 | 50.0–83.3 |
| Functional scales | ||
| Physical functioning | 86.7 | 73.3–100 |
| Emotional functioning | 75.0 | 66.7–85.4 |
| Cognitive functioning | 91.7 | 83.3–100 |
| Social functioning | 100 | 66.7–100 |
| Symptom scales | ||
| Fatigue | 11.1 | 8.3–33.3 |
| Pain | 16.7 | 12.5–50.0 |
| Insomnia | 33.3 | 0–41.7 |
| Appetite loss | 0 | 0–33.3 |
| Financial difficulties | 16.7 | 0–66.7 |
| HRQoL—EORTC QLQ-HN43 (score) | ||
| Swallowing | 20.8 | 0–50.0 |
| Dry mouth and sticky saliva | 25.0 | 0–33.3 |
| Body image | 5.6 | 0–22.2 |
| Fear of progression | 16.7 | 16.7–66.7 |
| Physical function | ||
| 6 min walk test (meters) | 434 | 399–533.8 |
| 30 s sit-to-stand test (repetitions) | 13.5 | 12.0–15.5 |
| Isometric handgrip strength (kgf) | ||
| Dominant hand | 38.0 | 34.7–44.0 |
| Nondominant hand | 37.1 | 33.7–41.3 |
| Isometric quadriceps strength (kgf) | ||
| Dominant limb | 31.7 | 20.7–36.5 |
| Nondominant limb | 30.5 | 20.9–35.6 |
| Nutritional status and body composition * | ||
| Body mass index (kg/m2) | 21.9 | 18.0–25.1 |
| Global Assessment PG-SGA (score) | 12.0 | 7.0–16.0 |
| Cognitive function | ||
| MoCA (points) | 23 | 20.8–26.3 |
| Dysphagia * | ||
| EAT-10 total score (points) | 7.5 | 1.8–22.3 |
| FOIS score (points) | 5.0 | 5.0–6.0 |
| N | Baseline T0 | Post-Treatment T1 | p-Value | Effect Size | |
|---|---|---|---|---|---|
| HRQoL—EORTC QLQ-C30 (score) – median (IQR) | |||||
| Global health status | 7 | 75 (66.7–83.3) | 50 (33.3–66.7) | 0.014 1 | 0.657 |
| Functional scales | 7 | ||||
| Physical functioning | 86.7 (60–100) | 80 (73.3–86.7) | 0.684 | 0.109 | |
| Emotional functioning | 75 (66.7–83.3) | 77.8 (58.3–83.3) | 1.000 | 0.000 | |
| Cognitive functioning | 100 (83.3–100) | 100 (83.3–100) | 0.414 | 0.218 | |
| Social functioning | 100 (100–100) | 66.7 (66.7–100) | 0.046 1 | 0.567 | |
| Symptom scales | 7 | ||||
| Fatigue | 11.1 (0–33.3) | 44.4 (33.3–77.8) | 0.026 1 | 0.595 | |
| Pain | 16.7 (16.7–33.3) | 33.3 (33.3–50) | 0.038 1 | 0.553 | |
| Insomnia | 0 (0–33.3) | 66.7 (0–66.7) | 0.063 | 0.496 | |
| Appetite loss | 0 (0–0) | 0 (0–33.3) | 0.157 | 0.378 | |
| Financial difficulties | 33.3 (0–66.7) | 66.7 (0–100) | 0.414 | 0.218 | |
| HRQoL—EORTC QLQ-HN43 (score) – median (IQR) | |||||
| Swallowing | 6 | 29.2 (0–52.1) | 66.7 (25–72.9) | 0.043 1 | 0.584 |
| Dry mouth and sticky saliva | 6 | 0 (0–33.3) | 66.7 (45.8–87.5) | 0.041 1 | 0.589 |
| Body image | 7 | 0 (0–11.1) | 11.1 (0–55.6) | 0.109 | 0.429 |
| Fear of progression | 7 | 16.7 (16.7–66.7) | 33.3 (16.6–33.3) | 0.785 | 0.073 |
| Physical function – median (IQR) | |||||
| 6MWT (meters) | 7 | 486 (412–533) | 422 (362–510) | 0.236 | 0.317 |
| 30 second sit-to-stand test (reps) | 6 | 13 (12–17) | 14 (12–17) | 0.833 | 0.061 |
| Isometric handgrip strength (kgf) | |||||
| Dominant hand | 7 | 39.7 (35.0–50.0) | 35.0 (31.7–39.3) | 0.018 1 | 0.632 |
| Nondominant hand | 7 | 37.2 (33.6–42.5) | 33.9 (34.3–41.2) | 0.043 1 | 0.542 |
| Isometric quadriceps strength (kgf) | |||||
| Dominant limb | 7 | 33.8 (26.3–36.5) | 28.7 (25.7–31.4) | 0.176 | 0.361 |
| Nondominant limb | 7 | 30.8 (22.4–37.0) | 26.2 (19.3–33.4) | 0.237 | 0.316 |
| Nutritional status and body composition | |||||
| BMI (kg/m2) – median (IQR) | 7 | 24.2 (18.1–25.6) | 20.6 (18.6–22.7) | 0.028 1 | 0.587 |
| Body fat (%) – median (IQR) | 6 | 21.1 (11.3–26.4) | 15.3 (11.8–20.3) | 0.046 1 | 0.575 |
| Fat-free mass (kg) – n (%) | 6 | 51.8 (46.0–55.5) | 49.0 (44.1–52) | 0.046 1 | 0.575 |
| Global Assessment PG-SGA | 6 | ||||
| A. Well nourished | 3 (50%) | 0 (0%) | 0.549 | ||
| B. Moderately malnourished or suspected malnutrition | 2 (33.3%) | 1 (16.7%) | |||
| C. Severely malnourished | 1 (16.7%) | 5 (83.3%) | |||
| PG-SGA total score (points) | 6 | 7 (3–13) | 18 (15–23) | 0.028 1 | 0.635 |
| Dysphagia | |||||
| EAT-10 total score (points) – median (IQR) | 7 | 7 (0–11) | 31 (21–40) | 0.027 1 | 0.590 |
| FOIS score – n (%) | 7 | ||||
| Nothing by mouth | 1 (14.3%) | 2 (28.6%) | 0.203 | ||
| Tube dependent with minimal attempts of food or liquid | 0 (0%) | 1 (14.3%) | |||
| Total oral diet with multiple consistencies, but requiring special preparation or compensations | 2 (28.6%) | 1 (14.3%) | |||
| Total oral diet with multiple consistencies without special preparation, but with specific food limitations | 2 (28.6%) | 2 (28.6%) | |||
| Total oral diet with no restrictions | 2 (28.6%) | 1 (14.3%) | |||
| FOIS total score (points) | 6 | 6 (5–7) | 4 (1–5) | 0.041 1 | 0.545 |
| Cognitive function | |||||
| MoCA (points) – median (IQR) | 7 | 26 (20–27) | 23 (20–26) | 0.167 | 0.369 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leão, I.; Garcia, C.; Antunes, P.; Campolargo, A.; Dias, I.; Coimbra, E.; Oliveira, P.; Zenha, H.; Costa, H.; Capela, A.; et al. Acute Impact of Cancer Treatment on Head and Neck Cancer Patients: FIT4TREATMENT. Cancers 2022, 14, 2698. https://doi.org/10.3390/cancers14112698
Leão I, Garcia C, Antunes P, Campolargo A, Dias I, Coimbra E, Oliveira P, Zenha H, Costa H, Capela A, et al. Acute Impact of Cancer Treatment on Head and Neck Cancer Patients: FIT4TREATMENT. Cancers. 2022; 14(11):2698. https://doi.org/10.3390/cancers14112698
Chicago/Turabian StyleLeão, Inês, Catarina Garcia, Pedro Antunes, Ana Campolargo, Isabel Dias, Edite Coimbra, Pedro Oliveira, Horácio Zenha, Horácio Costa, Andreia Capela, and et al. 2022. "Acute Impact of Cancer Treatment on Head and Neck Cancer Patients: FIT4TREATMENT" Cancers 14, no. 11: 2698. https://doi.org/10.3390/cancers14112698
APA StyleLeão, I., Garcia, C., Antunes, P., Campolargo, A., Dias, I., Coimbra, E., Oliveira, P., Zenha, H., Costa, H., Capela, A., Viamonte, S., Alves, A. J., & Joaquim, A. (2022). Acute Impact of Cancer Treatment on Head and Neck Cancer Patients: FIT4TREATMENT. Cancers, 14(11), 2698. https://doi.org/10.3390/cancers14112698