
Clinical Characteristics and Predictive Outcomes of Recurrent Nasopharyngeal Carcinoma—A Lingering Pitfall of the Long Latency

 ,
, 
 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Recruitment
2.2. Salvage Treatment
2.3. Statistical Analysis
3. Results
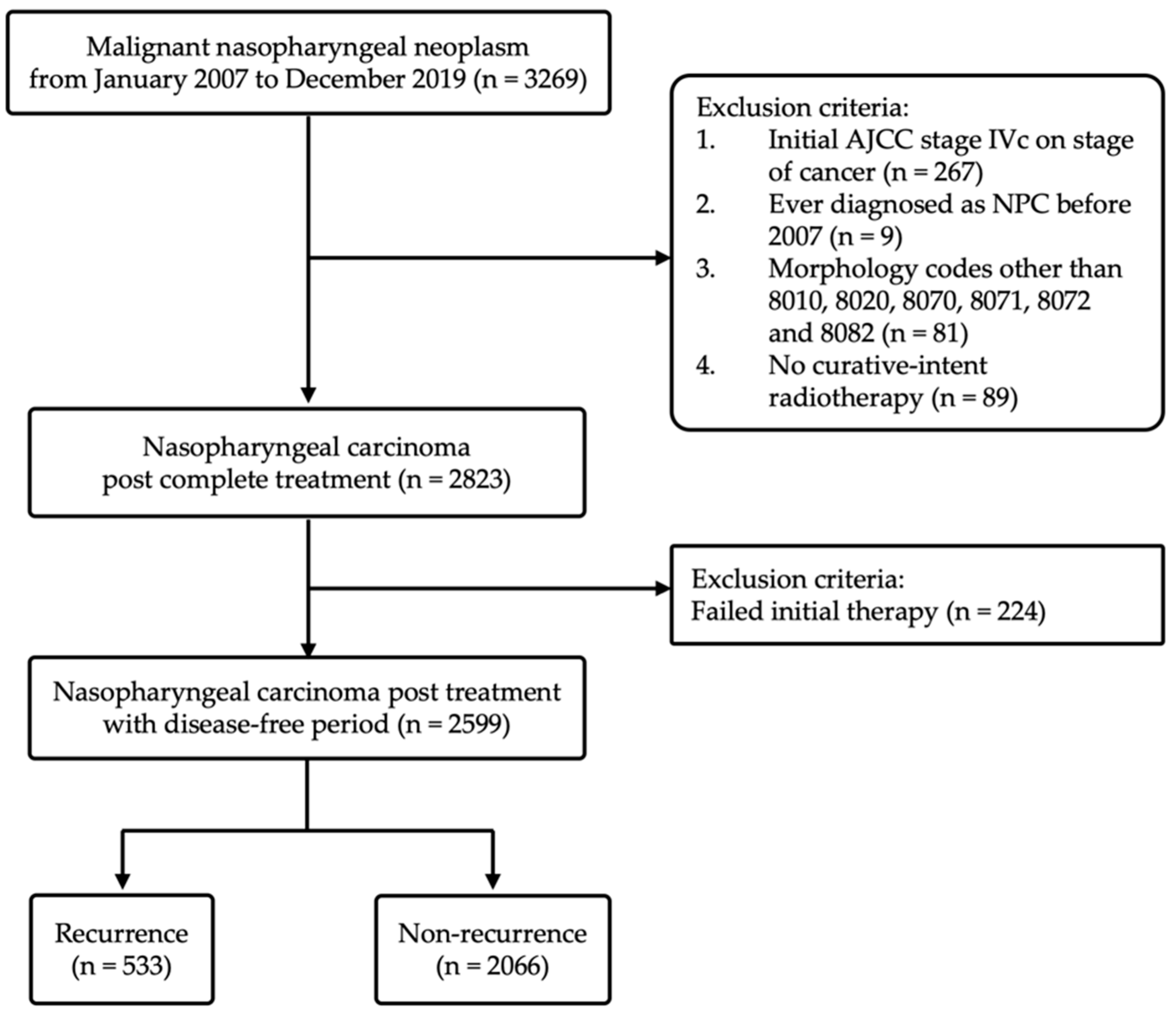
3.1. Study Population
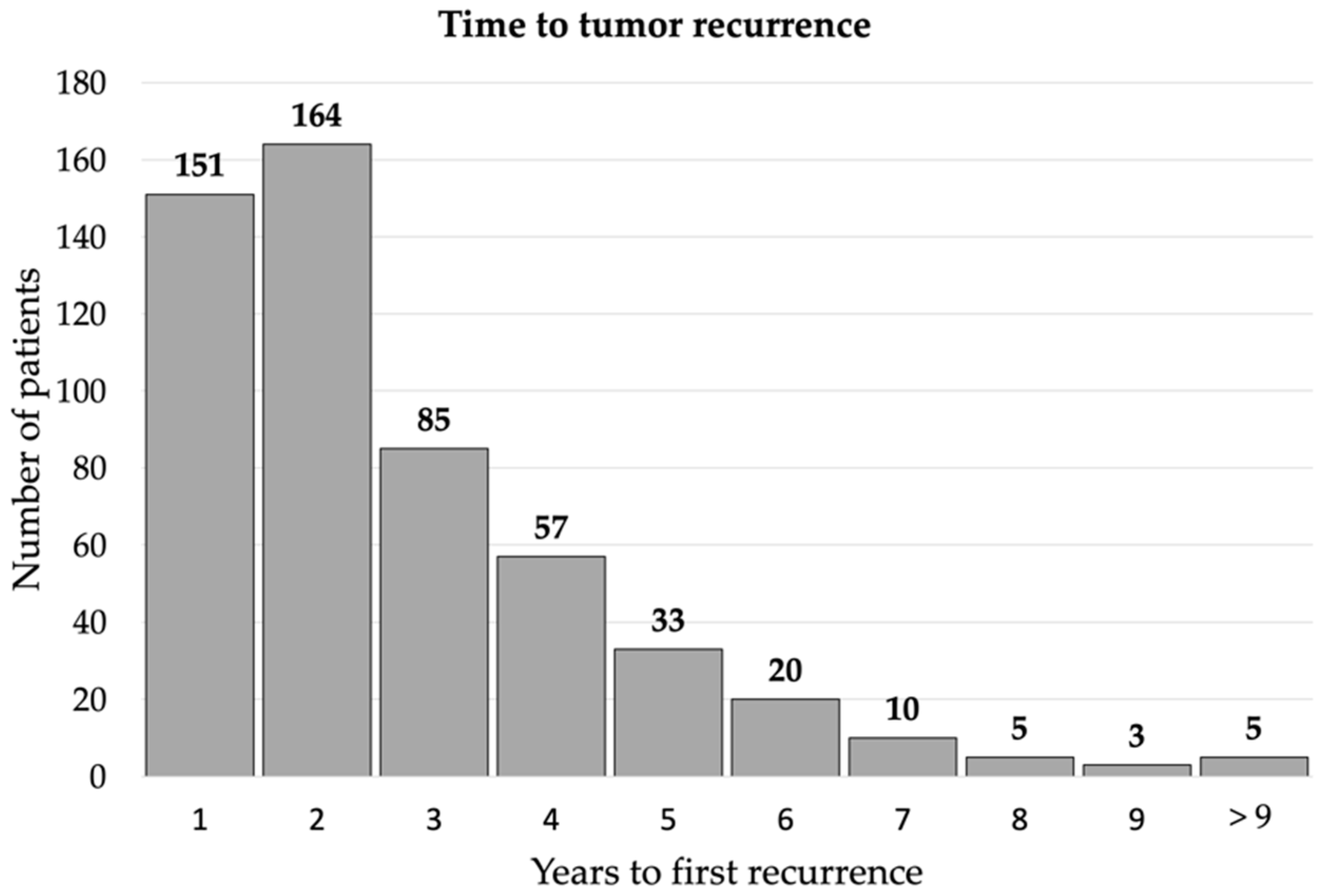
3.2. Clinical Characteristics and Time Distribution of Recurrent NPC
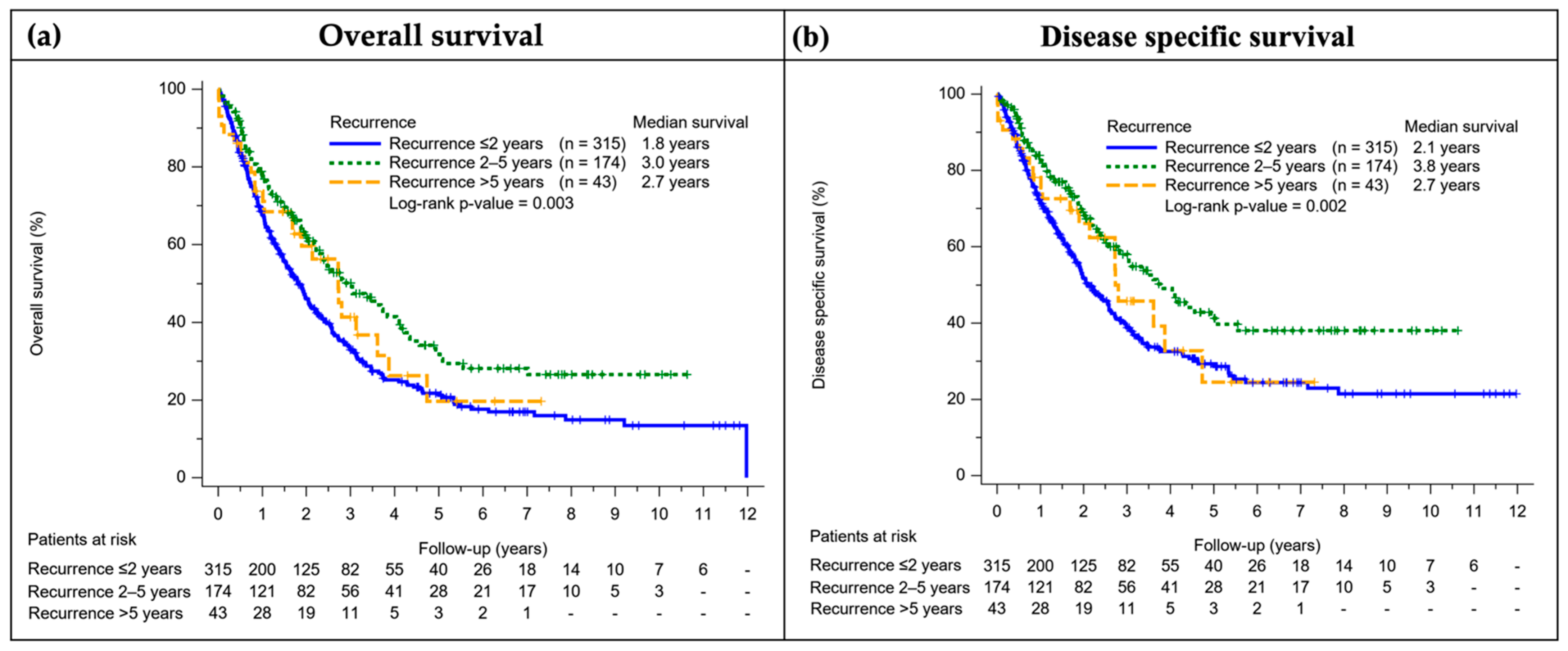
3.3. Survival Outcome of Patients with Recurrent NPC
3.4. The Long-Latent Recurrence NPC Group
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chen, Y.P.; Chan, A.T.C.; Le, Q.T.; Blanchard, P.; Sun, Y.; Ma, J. Nasopharyngeal carcinoma. Lancet 2019, 394, 64–80. [Google Scholar] [CrossRef]
- Chua, M.L.K.; Wee, J.T.S.; Hui, E.P.; Chan, A.T.C. Nasopharyngeal carcinoma. Lancet 2016, 387, 1012–1024. [Google Scholar] [CrossRef]
- Lee, A.W.; Ma, B.B.; Ng, W.T.; Chan, A.T. Management of Nasopharyngeal Carcinoma: Current Practice and Future Perspective. J. Clin. Oncol. 2015, 33, 3356–3364. [Google Scholar] [CrossRef]
- Pisani, P.; Airoldi, M.; Allais, A.; Aluffi Valletti, P.; Battista, M.; Benazzo, M.; Briatore, R.; Cacciola, S.; Cocuzza, S.; Colombo, A.; et al. Metastatic disease in head & neck oncology. Acta Otorhinolaryngol. Ital. 2020, 40, S1–S86. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.; Su, S.; Chen, C.; Han, F.; Zhao, C.; Xiao, W.; Deng, X.; Huang, S.; Lin, C.; Lu, T. Long-term outcomes of intensity-modulated radiotherapy for 868 patients with nasopharyngeal carcinoma: An analysis of survival and treatment toxicities. Radiother. Oncol. 2014, 110, 398–403. [Google Scholar] [CrossRef] [PubMed]
- Niu, X.; Xue, F.; Liu, P.; Hu, C.; He, X. Long-term outcomes of nasopharyngeal carcinoma patients with T1-2 stage in intensity-modulated radiotherapy era. Int. J. Med. Sci. 2022, 19, 267–273. [Google Scholar] [CrossRef]
- Montero, P.H.; Patel, S.G. Cancer of the oral cavity. Surg. Oncol. Clin. N. Am. 2015, 24, 491–508. [Google Scholar] [CrossRef] [Green Version]
- Price, J.M.; West, C.M.; Mistry, H.B.; Betts, G.; Bishop, P.; Kennedy, J.; Dixon, L.; Homer, J.J.; Garcez, K.P.; Lee, L.W.; et al. Improved survival prediction for oropharyngeal cancer beyond TNMv8. Oral Oncol. 2021, 115, 105140. [Google Scholar] [CrossRef]
- Li, J.X.; Lu, T.X.; Huang, Y.; Han, F. Clinical characteristics of recurrent nasopharyngeal carcinoma in high-incidence area. Sci. World J. 2012, 2012, 719754. [Google Scholar] [CrossRef] [Green Version]
- Han, F.; Zhao, C.; Huang, S.M.; Lu, L.X.; Huang, Y.; Deng, X.W.; Mai, W.Y.; Teh, B.S.; Butler, E.B.; Lu, T.X. Long-term outcomes and prognostic factors of re-irradiation for locally recurrent nasopharyngeal carcinoma using intensity-modulated radiotherapy. Clin. Oncol. 2012, 24, 569–576. [Google Scholar] [CrossRef]
- Colaco, R.J.; Betts, G.; Donne, A.; Swindell, R.; Yap, B.K.; Sykes, A.J.; Slevin, N.J.; Homer, J.J.; Lee, L.W. Nasopharyngeal carcinoma: A retrospective review of demographics, treatment and patient outcome in a single centre. Clin. Oncol. 2013, 25, 171–177. [Google Scholar] [CrossRef]
- Chen, S.; Yang, D.; Liao, X.; Lu, Y.; Yu, B.; Xu, M.; Bin, Y.; Zhou, P.; Yang, Z.; Liu, K.; et al. Failure Patterns of Recurrence and Metastasis After Intensity-Modulated Radiotherapy in Patients With Nasopharyngeal Carcinoma: Results of a Multicentric Clinical Study. Front. Oncol. 2021, 11, 693199. [Google Scholar] [CrossRef]
- Yao, Z.; Zhang, B.; Huang, J.; Shi, L.; Cheng, B. Radiation-induced acute injury of intensity-modulated radiotherapy versus three-dimensional conformal radiotherapy in induction chemotherapy followed by concurrent chemoradiotherapy for locoregionally advanced nasopharyngeal carcinoma: A prospective cohort study. Sci. Rep. 2021, 11, 7693. [Google Scholar] [CrossRef] [PubMed]
- Meccariello, G.; Bianchi, G.; Calpona, S.; Parisi, E.; Cammaroto, G.; Iannella, G.; Sgarzani, R.; Montevecchi, F.; De Vito, A.; Capaccio, P.; et al. Trans oral robotic surgery versus definitive chemoradiotherapy for oropharyngeal cancer: 10-year institutional experience. Oral Oncol. 2020, 110, 104889. [Google Scholar] [CrossRef] [PubMed]
- Newton, E.; Valenzuela, D.; Foley, J.; Thamboo, A.; Prisman, E. Outcomes for the treatment of locoregional recurrent nasopharyngeal cancer: Systematic review and pooled analysis. Head Neck 2021, 43, 3979–3995. [Google Scholar] [CrossRef]
- Kong, L.; Lu, J.J. Reirradiation of locally recurrent nasopharyngeal cancer: History, advances, and promises for the future. Chin. Clin. Oncol. 2016, 5, 26. [Google Scholar] [CrossRef]
- Zhan, Y.; Fan, S. Multiple Mechanisms Involving in Radioresistance of Nasopharyngeal Carcinoma. J. Cancer 2020, 11, 4193–4204. [Google Scholar] [CrossRef]
- Xiao, J.; He, X. Involvement of Non-Coding RNAs in Chemo- and Radioresistance of Nasopharyngeal Carcinoma. Cancer Manag. Res. 2021, 13, 8781–8794. [Google Scholar] [CrossRef]
- Zhang, L.; Zhu, Y.-X.; Wang, Y.; Huang, C.-P.; Wu, Y.; Ji, Q.-H. Salvage Surgery for Neck Residue or Recurrence of Nasopharyngeal Carcinoma: A 10-Year Experience. Ann. Surg. Oncol. 2011, 18, 233–238. [Google Scholar] [CrossRef] [Green Version]
- Wei, W.I.; Kwong, D.L. Recurrent nasopharyngeal carcinoma: Surgical salvage vs. additional chemoradiation. Curr. Opin. Otolaryngol. Head Neck Surg. 2011, 19, 82–86. [Google Scholar] [CrossRef]
- Feng, Y.; Dai, Z.; Yan, R.; Li, F.; Zhong, X.; Ye, H.; Chen, C.; Fan, S.; Qing, C.; Pan, Y.; et al. Outcomes of Recurrent Nasopharyngeal Carcinoma Patients Treated With Salvage Surgery: A Meta-Analysis. Front. Oncol. 2021, 11, 720418. [Google Scholar] [CrossRef]
- Liu, Y.P.; Wen, Y.H.; Tang, J.; Wei, Y.; You, R.; Zhu, X.L.; Li, J.; Chen, L.; Ling, L.; Zhang, N.; et al. Endoscopic surgery compared with intensity-modulated radiotherapy in resectable locally recurrent nasopharyngeal carcinoma: A multicentre, open-label, randomised, controlled, phase 3 trial. Lancet Oncol. 2021, 22, 381–390. [Google Scholar] [CrossRef]
- Thamboo, A.; Patel, V.S.; Hwang, P.H. 5-year outcomes of salvage endoscopic nasopharyngectomy for recurrent nasopharyngeal carcinoma. J. Otolaryngol. Head Neck Surg. 2021, 50, 12. [Google Scholar] [CrossRef]
- Li, G.; Wang, J.; Tang, H.; Han, R.; Zhao, Y.; Wang, X.; Zhou, H. Comparing endoscopic surgeries with open surgeries in terms of effectiveness and safety in salvaging residual or recurrent nasopharyngeal cancer: Systematic review and meta-analysis. Head Neck 2020, 42, 3415–3426. [Google Scholar] [CrossRef]
- You, R.; Zou, X.; Wang, S.L.; Jiang, R.; Tang, L.Q.; Zhang, W.D.; Li, L.; Zhang, M.X.; Shen, G.P.; Guo, L.; et al. New surgical staging system for patients with recurrent nasopharyngeal carcinoma based on the AJCC/UICC rTNM classification system. Eur. J. Cancer 2015, 51, 1771–1779. [Google Scholar] [CrossRef]
- Tan, L.P.; Tan, G.W.; Sivanesan, V.M.; Goh, S.L.; Ng, X.J.; Lim, C.S.; Kim, W.R.; Mohidin, T.B.B.M.; Mohd Dali, N.S.; Ong, S.H.; et al. Systematic comparison of plasma EBV DNA, anti-EBV antibodies and miRNA levels for early detection and prognosis of nasopharyngeal carcinoma. Int. J. Cancer 2020, 146, 2336–2347. [Google Scholar] [CrossRef] [Green Version]
- King, A.D.; Woo, J.K.S.; Ai, Q.Y.; Mo, F.K.F.; So, T.Y.; Lam, W.K.J.; Tse, I.O.L.; Vlantis, A.C.; Yip, K.W.N.; Hui, E.P.; et al. Early Detection of Cancer: Evaluation of MR Imaging Grading Systems in Patients with Suspected Nasopharyngeal Carcinoma. Am. J. Neuroradiol. 2020, 41, 515–521. [Google Scholar] [CrossRef] [Green Version]
- Liu, Z.; Li, H.; Yu, K.J.; Xie, S.H.; King, A.D.; Ai, Q.H.; Chen, W.J.; Chen, X.X.; Lu, Z.J.; Tang, L.Q.; et al. Comparison of new magnetic resonance imaging grading system with conventional endoscopy for the early detection of nasopharyngeal carcinoma. Cancer 2021, 127, 3403–3412. [Google Scholar] [CrossRef] [PubMed]
- Kyto, E.; Haapio, E.; Minn, H.; Irjala, H. Critical review of the follow-up protocol for head and neck cancer patients. J. Laryngol. Otol. 2019, 133, 424–429. [Google Scholar] [CrossRef]
- Shaikh, H.; Karivedu, V.; Wise-Draper, T.M. Managing Recurrent Metastatic Head and Neck Cancer. Hematol. Oncol. Clin. N. Am. 2021, 35, 1009–1020. [Google Scholar] [CrossRef]
- Lester, S.E.; Wight, R.G. ‘When will I see you again?’ Using local recurrence data to develop a regimen for routine surveillance in post-treatment head and neck cancer patients. Clin. Otolaryngol. 2009, 34, 546–551. [Google Scholar] [CrossRef] [PubMed]
- Denaro, N.; Merlano, M.C.; Russi, E.G. Follow-up in Head and Neck Cancer: Do More Does It Mean Do Better? A Systematic Review and Our Proposal Based on Our Experience. Clin. Exp. Otorhinolaryngol. 2016, 9, 287–297. [Google Scholar] [CrossRef] [PubMed]
- Brennan, K.E.; Hall, S.F.; Owen, T.E.; Griffiths, R.J.; Peng, Y. Variation in routine follow-up care after curative treatment for head-and-neck cancer: A population-based study in Ontario. Curr. Oncol. 2018, 25, e120–e131. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Chen, F.P.; Chen, Y.P.; Chen, Y.; He, X.J.; Huang, X.D.; Zheng, Z.Q.; Zheng, W.H.; Liu, X.; Sun, Y.; et al. Clinical Characteristics and Prognostic Factors of Early and Late Recurrence After Definitive Radiotherapy for Nasopharyngeal Carcinoma. Front. Oncol. 2020, 10, 1469. [Google Scholar] [CrossRef]
- Lee, A.W.; Foo, W.; Law, S.C.; Poon, Y.F.; Sze, W.M.; KO, S.; Tung, S.Y.; Chappell, R.; Lau, W.H.; Ho, J.H. Recurrent nasopharyngeal carcinoma: The puzzles of long latency. Int. J. Radiat. Oncol. Biol. Phys. 1999, 44, 149–156. [Google Scholar] [CrossRef]
- Chan, K.C.A.; Woo, J.K.S.; King, A.; Zee, B.C.Y.; Lam, W.K.J.; Chan, S.L.; Chu, S.W.I.; Mak, C.; Tse, I.O.L.; Leung, S.Y.M.; et al. Analysis of Plasma Epstein–Barr Virus DNA to Screen for Nasopharyngeal Cancer. N. Engl. J. Med. 2017, 377, 513–522. [Google Scholar] [CrossRef] [PubMed]
- Yeh, S.-A.; Hwang, T.-Z.; Wang, C.-C.; Yang, C.-C.; Lien, C.-F.; Wang, C.-C.; Hsu, T.-Y.; Hsu, R.-F.; Shih, Y.-C.; Huang, Y.-C.; et al. Outcomes of patients with nasopharyngeal carcinoma treated with intensity-modulated radiotherapy. J. Radiat. Res. 2021, 62, 438–447. [Google Scholar] [CrossRef] [PubMed]
- NCCN. NCCN Guidelines Version 2.2022 Head and Neck Cancers; National Comprehensive Cancer Network: Plymouth Meeting, PA, USA, 2022. [Google Scholar]
- Luo, M.S.; Huang, G.J.; Liu, H.B. Oncologic outcomes of IMRT versus CRT for nasopharyngeal carcinoma: A meta-analysis. Medicine 2019, 98, e15951. [Google Scholar] [CrossRef]
- Forster, J.C.; Douglass, M.J.J.; Harriss-Phillips, W.M.; Bezak, E. Simulation of head and neck cancer oxygenation and doubling time in a 4D cellular model with angiogenesis. Sci. Rep. 2017, 7, 11037. [Google Scholar] [CrossRef] [Green Version]
- Jensen, A.R.; Nellemann, H.M.; Overgaard, J. Tumor progression in waiting time for radiotherapy in head and neck cancer. Radiother. Oncol. 2007, 84, 5–10. [Google Scholar] [CrossRef]
- Murphy, C.T.; Devarajan, K.; Wang, L.S.; Mehra, R.; Ridge, J.A.; Fundakowski, C.; Galloway, T.J. Pre-treatment tumor-specific growth rate as a temporal biomarker that predicts treatment failure and improves risk stratification for oropharyngeal cancer. Oral Oncol. 2015, 51, 1034–1040. [Google Scholar] [CrossRef]
- Ho, A.C.; Lee, V.H.; To, V.S.; Kwong, D.L.; Wei, W.I. Natural course and tumor doubling time of nasopharyngeal carcinoma. A study of 15 patients. Oral Oncol. 2011, 47, 742–746. [Google Scholar] [CrossRef]
- Nicholls, J.; Sham, J.; Ng, M.H.; Choy, D. In-situ carcinoma adjacent to recurrent nasopharyngeal carcinoma. Evidence of a new growth? Pathol. Res. Pract. 1993, 189, 1067–1070. [Google Scholar] [CrossRef]
- Campion, N.J.; Ally, M.; Jank, B.J.; Ahmed, J.; Alusi, G. The molecular march of primary and recurrent nasopharyngeal carcinoma. Oncogene 2021, 40, 1757–1774. [Google Scholar] [CrossRef]
- Ruben, J.D.; Smith, R.; Lancaster, C.M.; Haynes, M.; Jones, P.; Panettieri, V. Constituent components of out-of-field scatter dose for 18-MV intensity modulated radiation therapy versus 3-dimensional conformal radiation therapy: A comparison with 6-MV and implications for carcinogenesis. Int. J. Radiat. Oncol. Biol. Phys. 2014, 90, 645–653. [Google Scholar] [CrossRef]
- Chan, J.Y.W.; To, V.S.H.; Wong, S.T.S.; Wei, W.I. Radiation-induced squamous cell carcinoma of the nasopharynx after radiotherapy for nasopharyngeal carcinoma. Head Neck 2014, 36, 772–775. [Google Scholar] [CrossRef]
- Chan, J.Y.W.; Wong, S.T.S.; Lau, G.I.S.K.; Wei, W.I. Postradiation sarcoma after radiotherapy for nasopharyngeal carcinoma. Laryngoscope 2012, 122, 2695–2699. [Google Scholar] [CrossRef]
- Echchikhi, Y.; Loughlimi, H.; Touil, A.; Kebdani, T.; Benjaafar, N. Radiation-induced osteosarcoma of the skull base after radiation therapy in a patient with nasopharyngeal carcinoma: A case report and review of the literature. J. Med. Case Rep. 2016, 10, 334. [Google Scholar] [CrossRef] [Green Version]
- Chan, J.Y.; Wei, W.I. Critical appraisal of maxillary swing approach for nasopharyngeal carcinoma. Expert Opin. Targets 2012, 16 (Suppl. 1), S111–S117. [Google Scholar] [CrossRef]
- Xu, T.; Tang, J.; Gu, M.; Liu, L.; Wei, W.; Yang, H. Recurrent Nasopharyngeal Carcinoma: A Clinical Dilemma and Challenge. Curr. Oncol. 2013, 20, 406–419. [Google Scholar] [CrossRef] [Green Version]
- Suarez, C.; Rodrigo, J.P.; Rinaldo, A.; Langendijk, J.A.; Shaha, A.R.; Ferlito, A. Current treatment options for recurrent nasopharyngeal cancer. Eur. Arch. Otorhinolaryngol. 2010, 267, 1811–1824. [Google Scholar] [CrossRef] [Green Version]
- Siti-Azrin, A.H.; Norsa'adah, B.; Naing, N.N. Prognostic factors of nasopharyngeal carcinoma patients in a tertiary referral hospital: A retrospective cohort study. BMC Res. Notes 2017, 10, 705. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yeung, D.C.M.; Yeung, Z.; Wong, E.W.Y.; Vlantis, A.C.; Chan, J.Y.K. Neck lymph node status on survival of regionally recurrent or persistent nasopharyngeal carcinoma. Sci. Rep. 2020, 10, 5622. [Google Scholar] [CrossRef] [Green Version]
- Chen, M.K.; Lai, J.C.; Chang, C.C.; Liu, M.T. Minimally invasive endoscopic nasopharyngectomy in the treatment of recurrent T1-2a nasopharyngeal carcinoma. Laryngoscope 2007, 117, 894–896. [Google Scholar] [CrossRef]
- Li, J.X.; Huang, S.M.; Jiang, X.H.; Ouyang, B.; Han, F.; Liu, S.; Wen, B.X.; Lu, T.X. Local failure patterns for patients with nasopharyngeal carcinoma after intensity-modulated radiotherapy. Radiat. Oncol. 2014, 9, 87. [Google Scholar] [CrossRef] [Green Version]
- King, A.D.; Woo, J.K.S.; Ai, Q.Y.; Chan, J.S.M.; Lam, W.K.J.; Tse, I.O.L.; Bhatia, K.S.; Zee, B.C.Y.; Hui, E.P.; Ma, B.B.Y.; et al. Complementary roles of MRI and endoscopic examination in the early detection of nasopharyngeal carcinoma. Ann. Oncol. 2019, 30, 977–982. [Google Scholar] [CrossRef] [PubMed]
- King, A.D.; Vlantis, A.C.; Yuen, T.W.; Law, B.K.; Bhatia, K.S.; Zee, B.C.; Woo, J.K.; Chan, A.T.; Chan, K.C.; Ahuja, A.T. Detection of Nasopharyngeal Carcinoma by MR Imaging: Diagnostic Accuracy of MRI Compared with Endoscopy and Endoscopic Biopsy Based on Long-Term Follow-Up. AJNR Am. J. Neuroradiol. 2015, 36, 2380–2385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- King, A.D.; Vlantis, A.C.; Bhatia, K.S.; Zee, B.C.; Woo, J.K.; Tse, G.M.; Chan, A.T.; Ahuja, A.T. Primary nasopharyngeal carcinoma: Diagnostic accuracy of MR imaging versus that of endoscopy and endoscopic biopsy. Radiology 2011, 258, 531–537. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.C.; Lee, J.C.; Huang, W.Y.; Juan, C.J.; Jen, Y.M.; Lin, L.F. Image-based diagnosis of residual or recurrent nasopharyngeal carcinoma may be a phantom tumor phenomenon. Medicine 2021, 100, e24555. [Google Scholar] [CrossRef] [PubMed]
- Chan, K.C.A.; Hung, E.C.W.; Woo, J.K.S.; Chan, P.K.S.; Leung, S.-F.; Lai, F.P.T.; Cheng, A.S.M.; Yeung, S.W.; Chan, Y.W.; Tsui, T.K.C.; et al. Early detection of nasopharyngeal carcinoma by plasma Epstein-Barr virus DNA analysis in a surveillance program. Cancer 2013, 119, 1838–1844. [Google Scholar] [CrossRef]
- He, S.S.; Wang, Y.; Yang, Y.Y.; Niu, S.Q.; Zhu, M.Y.; Lu, L.X.; Chen, Y. Circulating Plasma Epstein-Barr Virus DNA Load During the Follow-up Periods Predicts Recurrence and Metastasis in Nasopharyngeal Carcinoma. Cancer J. 2022, 28, 85–92. [Google Scholar] [CrossRef]
- Liang, F.Y.; Sun, W.; Han, P.; Lu, X.; Lian, Y.N.; Huang, X.M. Detecting plasma Epstein-Barr virus DNA to diagnose postradiation nasopharyngeal skull base lesions in nasopharyngeal carcinoma patients: A prospective study. Chin. J. Cancer 2012, 31, 142–149. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.Y.; Wei, X.L.; Ren, C.; Zhang, Y.; Hu, Y.F.; Li, J.Y.; Chen, J.L.; Wang, Y.Q.; Han, F.; Wang, F.H. Association of Plasma Epstein-Barr Virus DNA With Outcomes for Patients With Recurrent or Metastatic Nasopharyngeal Carcinoma Receiving Anti-Programmed Cell Death 1 Immunotherapy. JAMA Netw. Open 2022, 5, e220587. [Google Scholar] [CrossRef]
- Tsai, M.S.; Lin, M.H.; Lee, C.P.; Yang, Y.H.; Chen, W.C.; Chang, G.H.; Tsai, Y.T.; Chen, P.C.; Tsai, Y.H. Chang Gung Research Database: A multi-institutional database consisting of original medical records. Biomed. J. 2017, 40, 263–269. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | Recurrence (n = 533) | Non-Recurrence (n = 2066) | p-Value |
|---|---|---|---|
| Age (Mean ± SD, Years) (n = 2599) | 50.2 ± 12.1 | 49.9 ± 12.2 | 0.512 |
| Sex (n = 2599) | 0.004 | ||
| Male | 426 (79.9%) | 1526 (73.9%) | |
| Female | 107 (20.1%) | 540 (26.1%) | |
| Clinical T classification (n = 2599) | <0.001 | ||
| 1, 2 | 232 (43.5%) | 1183 (57.3%) | |
| 3, 4 | 301 (56.5%) | 883 (42.7%) | |
| Clinical N classification (n = 2599) | <0.001 | ||
| 0 | 47 (8.8%) | 365 (17.7%) | |
| 1, 2, 3 | 486 (91.2%) | 1701 (82.3%) | |
| Clinical AJCC stage (n = 2599) | <0.001 | ||
| 1, 2 | 86 (16.1%) | 738 (35.7%) | |
| 3, 4 | 447 (83.9%) | 1328 (64.3%) | |
| Death (n = 2599) | 354 (66.4%) | 243 (11.8%) | <0.001 |
| Diabetes mellitus (n = 2599) | 20 (3.8%) | 108 (5.2%) | 0.161 |
| Hypertension (n = 2599) | 40 (7.5%) | 190 (9.2%) | 0.220 |
| Prolonged RT duration (n = 2599) | <0.001 | ||
| No | 368 (69.0%) | 1629 (78.8%) | |
| Yes | 165 (31.0%) | 437 (21.2%) | |
| Treatment protocol (n = 2599) | <0.001 | ||
| RT alone | 35 (6.6%) | 287 (13.9%) | |
| CCRT | 451 (84.6%) | 1572 (76.1%) | |
| Induction CT + CCRT | 47 (8.8%) | 207 (10.0%) | |
| WHO type (n = 2599) | <0.001 | ||
| Keratinizing squamous cell carcinoma | 57 (10.7%) | 174 (8.4%) | |
| Non-keratinizing carcinoma, differentiated | 300 (56.3%) | 1387 (67.1%) | |
| Non-keratinizing carcinoma, undifferentiated | 176 (33.0%) | 505 (24.4%) | |
| Recurrence type (n = 2599) | |||
| Local | 174 (32.6%) | - | |
| Regional | 122 (22.9%) | - | |
| Distal | 237 (44.5%) | - |
| Overall (n = 2599) | ||||
|---|---|---|---|---|
| Variables | Crude OR (95% C.I.) | p-Value | Adjusted OR (95% C.I.) | p-Value |
| Age (Mean ± SD) (years) (n = 2599) | 1.00 (0.99, 1.01) | 0.512 | 1.01 (1.00, 1.01) | 0.148 |
| Sex (n = 2599) | ||||
| Male | 1.41 (1.12, 1.78) | 0.004 | 1.35 (1.07, 1.72) | 0.013 |
| Female | 1.00 | 1.00 | ||
| AJCC (n = 2599) | ||||
| 1, 2 | 1.00 | 1.00 | ||
| 3, 4 | 2.89 (2.25, 3.70) | <0.001 | 2.64 (2.04, 3.42) | <0.001 |
| Diabetes mellitus (n = 2599) | ||||
| No | 1.00 | 1.00 | ||
| Yes | 0.71 (0.43, 1.15) | 0.163 | 0.78 (0.45, 1.34) | 0.362 |
| Hypertension (n = 2599) | ||||
| No | 1.00 | 1.00 | ||
| Yes | 0.80 (0.56, 1.14) | 0.221 | 0.90 (0.60, 1.35) | 0.602 |
| Prolonged RT duration (n = 2599) | ||||
| No | 1.00 | 1.00 | ||
| Yes | 1.67 (1.35, 2.07) | <0.001 | 1.52 (1.22, 1.89) | <0.001 |
| Treatment protocol (n = 2599) | ||||
| RT alone | 0.54 (0.33, 0.86) | 0.010 | 0.78 (0.48, 1.29) | 0.336 |
| CCRT | 1.26 (0.91, 1.76) | 0.169 | 1.27 (0.90, 1.78) | 0.177 |
| Induction CT + CCRT | 1.00 | 1.00 | ||
| WHO type (n = 2599) | ||||
| Keratinizing squamous cell carcinoma | 1.00 | 1.00 | ||
| Non-keratinizing carcinoma, differentiated | 0.66 (0.48, 0.91) | 0.012 | 0.70 (0.50, 0.98) | 0.038 |
| Non-keratinizing carcinoma, undifferentiated | 1.06 (0.75, 1.50) | 0.724 | 1.13 (0.79, 1.61) | 0.508 |
| Variables | Recurrence ≤ 2 Years (n = 315) | Recurrence 2–5 Years (n = 175) | Recurrence > 5 Years (n = 43) | p-Value |
|---|---|---|---|---|
| Age (Mean ± SD) (years) (n = 533) | 50.4 ± 12.1 | 50.1 ± 12.3 | 49.5 ± 12.1 | 0.896 |
| Sex (n = 533) | 0.962 | |||
| Male | 253 (80.3%) | 139 (79.4%) | 34 (79.1%) | |
| Female | 62 (19.7%) | 36 (20.6%) | 9 (20.9%) | |
| T (n = 533) | 0.002 | |||
| 1, 2 | 118 (37.5%) | 88 (50.3%) | 26 (60.5%) | |
| 3, 4 | 197 (62.5%) | 87 (49.7%) | 17 (39.5%) | |
| N (n = 533) | 0.013 | |||
| 0 | 23 (7.3%) | 15 (8.6%) | 9 (20.9%) | |
| 1, 2, 3 | 292 (92.7%) | 160 (91.4%) | 34 (79.1%) | |
| AJCC (n = 533) | 0.001 | |||
| 1, 2 | 37 (11.7%) | 36 (20.6%) | 13 (30.2%) | |
| 3, 4 | 278 (88.3%) | 139 (79.4%) | 30 (69.8%) | |
| Death (n = 533) | 232 (73.7%) | 97 (55.4%) | 25 (58.1%) | <0.001 |
| Diabetes mellitus (n = 533) | 12 (3.8%) | 5 (2.9%) | 3 (7.0%) | 0.443 |
| Hypertension (n = 533) | 24 (7.6%) | 12 (6.9%) | 4 (9.3%) | 0.856 |
| Prolonged RT duration (n = 533) | 0.972 | |||
| No | 218 (69.2%) | 121 (69.1%) | 29 (67.4%) | |
| Yes | 97 (30.8%) | 54 (30.9%) | 14 (32.6%) | |
| Treatment protocol (n = 533) | 0.432 | |||
| RT alone | 17 (5.4%) | 13 (7.4%) | 5 (11.6%) | |
| CCRT | 271 (86.0%) | 147 (84.0%) | 33 (76.7%) | |
| Induction CT + CCRT | 27 (8.6%) | 15 (8.6%) | 5 (11.6%) | |
| WHO type (n = 533) | 0.980 | |||
| Keratinizing squamous cell carcinoma | 34 (10.8%) | 19 (10.9%) | 4 (9.3%) | |
| Non-keratinizing carcinoma, differentiated | 179 (56.8%) | 98 (56.0%) | 23 (53.5%) | |
| Non-keratinizing carcinoma, undifferentiated | 102 (32.4%) | 58 (33.1%) | 16 (37.2%) | |
| Recurrence type (n = 533) | <0.001 | |||
| Local | 96 (30.5%) | 58 (33.1%) | 20 (46.5%) | |
| Regional | 56 (17.8%) | 55 (31.4%) | 11 (25.6%) | |
| Distal | 163 (51.7%) | 62 (35.4%) | 12 (27.9%) | |
| Salvage surgery (n = 533) | 0.527 | |||
| No | 270 (85.7%) | 144 (82.3%) | 35 (81.4%) | |
| Yes | 45 (14.3%) | 31 (17.7%) | 8 (18.6%) |
| Variables | Univariable HR (95% C.I.) | p-Value | Multivariable HR (95% C.I.) | p-Value |
|---|---|---|---|---|
| Age (years) | 1.03 (1.02, 1.04) | <0.001 | 1.03 (1.02, 1.04) | <0.001 |
| Sex | ||||
| Male | 0.97 (0.75, 1.27) | 0.847 | 1.01 (0.77, 1.33) | 0.929 |
| Female | 1.00 | 1.00 | ||
| AJCC | ||||
| 1, 2 | 1.00 | 1.00 | ||
| 3, 4 | 1.56 (1.14, 2.12) | 0.005 | 1.46 (1.04, 2.04) | 0.027 |
| Diabetes mellitus | ||||
| No | 1.00 | 1.00 | ||
| Yes | 1.82 (1.10, 3.00) | 0.020 | 1.41 (0.81, 2.46) | 0.225 |
| Hypertension | ||||
| No | 1.00 | 1.00 | ||
| Yes | 1.34 (0.92, 1.96) | 0.129 | 0.92 (0.60, 1.40) | 0.690 |
| Prolonged RT duration | ||||
| No | 1.00 | 1.00 | ||
| Yes | 1.30 (1.05, 1.62) | 0.017 | 1.16 (0.93, 1.46) | 0.190 |
| Treatment protocol | ||||
| CCRT | 1.00 | 1.00 | ||
| RT alone | 1.38 (0.92, 2.05) | 0.118 | 1.38 (0.89, 2.13) | 0.149 |
| WHO type | ||||
| Keratinizing squamous cell carcinoma | 1.00 | 1.00 | ||
| Non-keratinizing carcinoma, differentiated | 0.91 (0.64, 1.30) | 0.617 | 0.81 (0.57, 1.16) | 0.247 |
| Non-keratinizing carcinoma, undifferentiated | 0.97 (0.68, 1.39) | 0.868 | 0.93 (0.65, 1.35) | 0.719 |
| Recurrence | ||||
| Recurrence ≤ 2 years | 1.00 | 1.00 | ||
| Recurrence 2–5 years | 0.66 (0.52, 0.84) | 0.001 | 0.69 (0.54, 0.88) | 0.003 |
| Recurrence > 5 years | 0.82 (0.54, 1.24) | 0.344 | 0.91 (0.59, 1.39) | 0.665 |
| Recurrence type | ||||
| Local | 1.00 | 1.00 | ||
| Regional | 0.70 (0.51, 0.95) | 0.023 | 0.72 (0.52, 0.99) | 0.046 |
| Distal | 1.45 (1.14, 1.83) | 0.002 | 1.05 (0.81, 1.34) | 0.725 |
| Salvage surgery | ||||
| No | 1.00 | 1.00 | ||
| Yes | 0.30 (0.21, 0.44) | <0.001 | 0.38 (0.25, 0.57) | <0.001 |
| Variables | Dead (n = 25) | Alive (n = 18) | p-Value |
|---|---|---|---|
| Age (Mean ± SD) (years) when recurrence (n = 43) | 58.5 ± 11.3 | 54.6 ± 13.3 | 0.304 |
| Sex (n = 43) | 0.712 | ||
| Male | 19 (76.0%) | 15 (83.3%) | |
| Female | 6 (24.0%) | 3 (16.7%) | |
| T classification when recurrence (n = 43) | 0.003 | ||
| 0 | 5 (20.0%) | 11 (61.1%) | |
| 1, 2 | 7 (28.0%) | 6 (33.3%) | |
| 3, 4 | 13 (52.0%) | 1 (5.69%) | |
| N classification when recurrence (n = 43) | 0.158 | ||
| 0 | 19 (76.0%) | 10 (55.6%) | |
| 1, 2, 3 | 6 (24.0%) | 8 (44.4%) | |
| AJCC stage when recurrence (n = 43) | 0.006 | ||
| 1, 2 | 4 (16.0%) | 10 (55.6%) | |
| 3, 4 | 21 (84.0%) | 8 (44.4%) | |
| Prolonged RT duration (n = 43) | 0.059 | ||
| No | 14 (56.0%) | 15 (83.3%) | |
| Yes | 11 (44.0%) | 3 (16.7%) | |
| WHO type when recurrence (n = 43) | 0.311 | ||
| Keratinizing squamous cell carcinoma | 1 (4%) | 2 (33.3%) | |
| Non-keratinizing carcinoma, differentiated | 7 (28.0%) | 4 (22.2%) | |
| Non-keratinizing carcinoma, undifferentiated | 9 (36.0%) | 10 (66.7%) | |
| Others | 8 (32.0%) | 2 (11.1%) | |
| Recurrent type (n = 43) | 0.036 | ||
| Local | 15 (60.0%) | 5 (27.8%) | |
| Regional | 3 (12.0%) | 8 (44.4%) | |
| Distal | 7 (28.0%) | 5 (27.8%) | |
| Salvage surgery (n = 43) | 0.247 | ||
| No | 22 (88.0%) | 13 (72.2%) | |
| Yes | 3 (12.0%) | 5 (27.8%) | |
| Symptomatic (n = 43) | 0.014 | ||
| Yes | 17 (68.0%) | 5 (27.8%) | |
| No | 8 (32.0%) | 13 (72.2%) | |
| Prolonged follow-up interval (>6 months) (n = 43) | 0.163 | ||
| Yes | 9 (36.0%) | 3 (16.7%) | |
| Nos | 16 (64.0%) | 15 (83.3%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Y.-H.; Luo, S.-D.; Wu, S.-C.; Wu, C.-N.; Chiu, T.-J.; Wang, Y.-M.; Yang, Y.-H.; Chen, W.-C. Clinical Characteristics and Predictive Outcomes of Recurrent Nasopharyngeal Carcinoma—A Lingering Pitfall of the Long Latency. Cancers 2022, 14, 3795. https://doi.org/10.3390/cancers14153795
Chen Y-H, Luo S-D, Wu S-C, Wu C-N, Chiu T-J, Wang Y-M, Yang Y-H, Chen W-C. Clinical Characteristics and Predictive Outcomes of Recurrent Nasopharyngeal Carcinoma—A Lingering Pitfall of the Long Latency. Cancers. 2022; 14(15):3795. https://doi.org/10.3390/cancers14153795
Chicago/Turabian StyleChen, Yung-Hsuan, Sheng-Dean Luo, Shao-Chun Wu, Ching-Nung Wu, Tai-Jan Chiu, Yu-Ming Wang, Yao-Hsu Yang, and Wei-Chih Chen. 2022. "Clinical Characteristics and Predictive Outcomes of Recurrent Nasopharyngeal Carcinoma—A Lingering Pitfall of the Long Latency" Cancers 14, no. 15: 3795. https://doi.org/10.3390/cancers14153795
APA StyleChen, Y. -H., Luo, S. -D., Wu, S. -C., Wu, C. -N., Chiu, T. -J., Wang, Y. -M., Yang, Y. -H., & Chen, W. -C. (2022). Clinical Characteristics and Predictive Outcomes of Recurrent Nasopharyngeal Carcinoma—A Lingering Pitfall of the Long Latency. Cancers, 14(15), 3795. https://doi.org/10.3390/cancers14153795