
Investigating the Role of CTCs with Stem/EMT-like Features in Metastatic Breast Cancer Patients Treated with Eribulin Mesylate

 ,
, 


Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Treatment
2.2. Enrichment of CTCs
2.3. Immunofluorescence (IF)
2.4. Detection and Phenotypic Analysis of CTCs
2.5. Statistical Analysis
3. Results
3.1. Patient and Disease Characteristics
3.2. Detection and Monitoring of CTCs during Eribulin Treatment and on Disease Progression
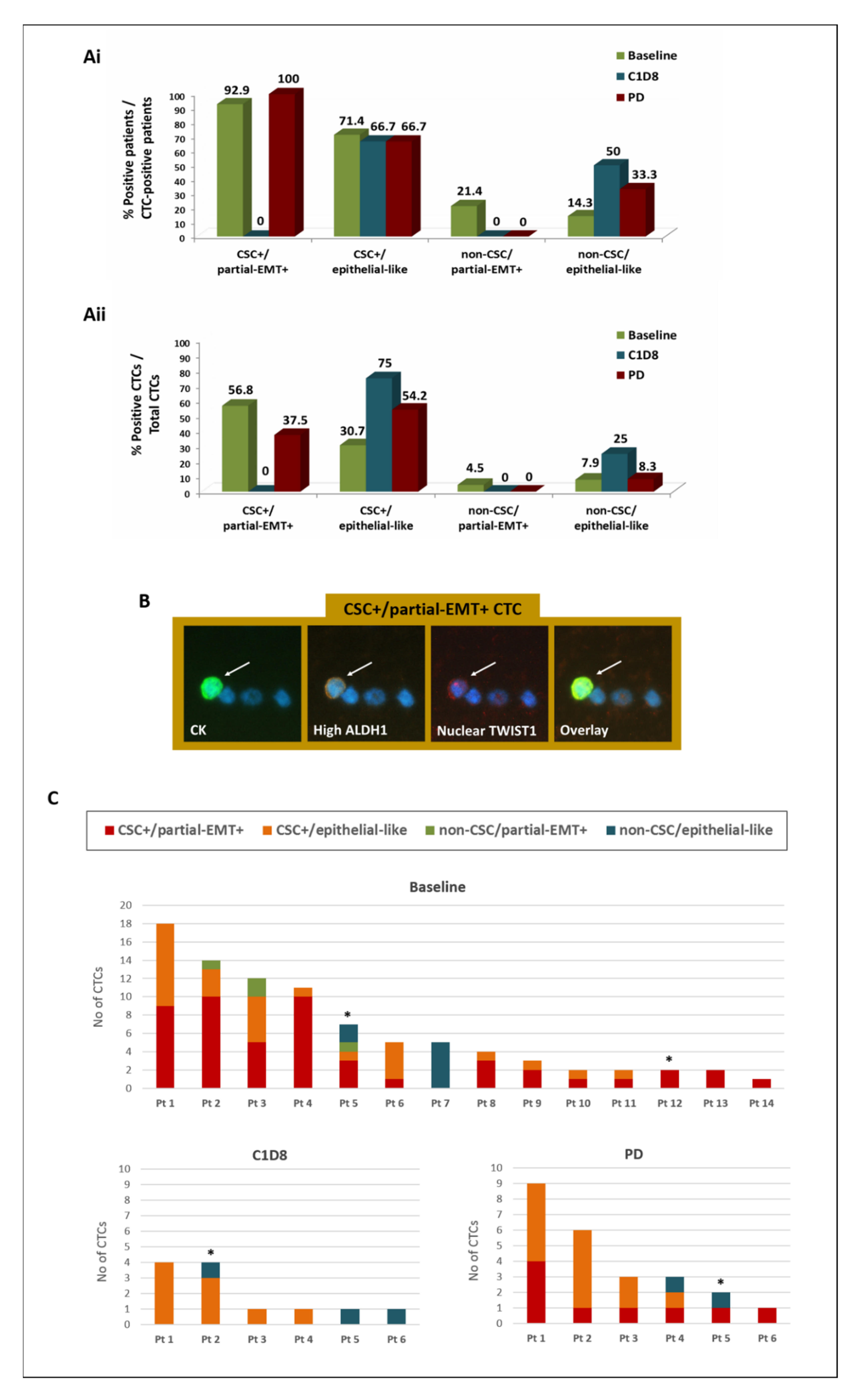
3.3. Phenotypic Analysis of CTCs during Eribulin Treatment and on Disease Progression
3.4. Clinical Relevance of the Detection and the CSC/Partial-EMT Phenotype of CTCs in BC Patients Treated with Eribulin Mesylate
3.4.1. Correlation with Patient and Disease Characteristics
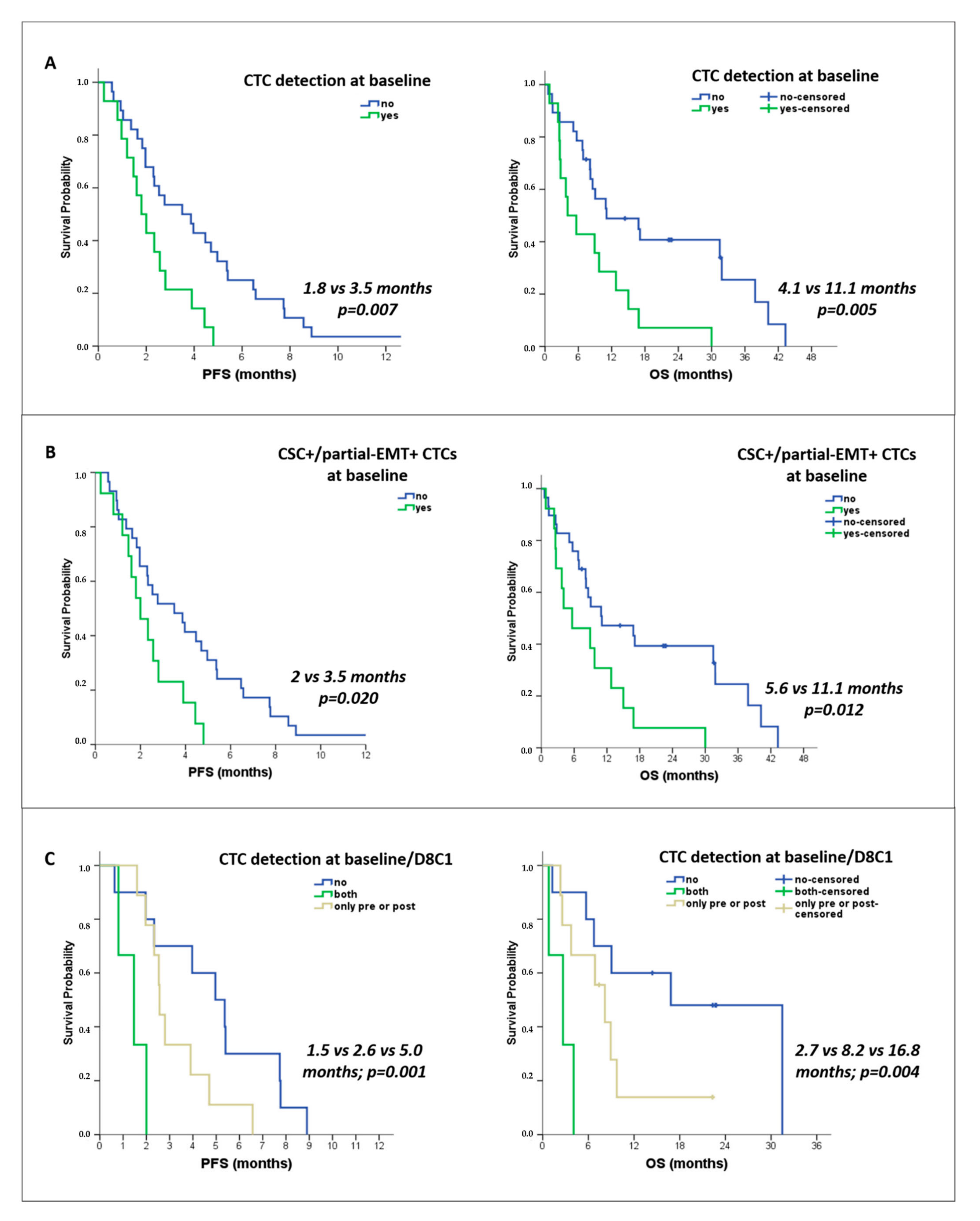
3.4.2. Correlation with Survival
3.4.3. Assessment of the Risk of Disease Progression and Death
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Dillekas, H.; Rogers, M.S.; Straume, O. Are 90% of deaths from cancer caused by metastases? Cancer Med. 2019, 8, 5574–5576. [Google Scholar] [CrossRef] [PubMed]
- Castro-Giner, F.; Aceto, N. Tracking cancer progression: From circulating tumor cells to metastasis. Genome Med. 2020, 12, 31. [Google Scholar] [CrossRef] [PubMed]
- Cristofanilli, M.; Pierga, J.Y.; Reuben, J.; Rademaker, A.; Davis, A.A.; Peeters, D.J.; Fehm, T.; Nole, F.; Gisbert-Criado, R.; Mavroudis, D.; et al. The clinical use of circulating tumor cells (CTCs) enumeration for staging of metastatic breast cancer (MBC): International expert consensus paper. Crit. Rev. Oncol. Hematol. 2019, 134, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Larsson, A.M.; Jansson, S.; Bendahl, P.O.; Levin Tykjaer Jorgensen, C.; Loman, N.; Graffman, C.; Lundgren, L.; Aaltonen, K.; Ryden, L. Longitudinal enumeration and cluster evaluation of circulating tumor cells improve prognostication for patients with newly diagnosed metastatic breast cancer in a prospective observational trial. Breast Cancer Res. 2018, 20, 48. [Google Scholar] [CrossRef] [PubMed]
- Bidard, F.C.; Jacot, W.; Kiavue, N.; Dureau, S.; Kadi, A.; Brain, E.; Bachelot, T.; Bourgeois, H.; Goncalves, A.; Ladoire, S.; et al. Efficacy of Circulating Tumor Cell Count-Driven vs Clinician-Driven First-line Therapy Choice in Hormone Receptor-Positive, ERBB2-Negative Metastatic Breast Cancer: The STIC CTC Randomized Clinical Trial. JAMA Oncol. 2021, 7, 34–41. [Google Scholar] [CrossRef] [PubMed]
- Baccelli, I.; Schneeweiss, A.; Riethdorf, S.; Stenzinger, A.; Schillert, A.; Vogel, V.; Klein, C.; Saini, M.; Bauerle, T.; Wallwiener, M.; et al. Identification of a population of blood circulating tumor cells from breast cancer patients that initiates metastasis in a xenograft assay. Nat. Biotechnol. 2013, 31, 539–544. [Google Scholar] [CrossRef] [PubMed]
- Shibue, T.; Weinberg, R.A. EMT, CSCs, and drug resistance: The mechanistic link and clinical implications. Nat. Rev. Clin. Oncol. 2017, 14, 611–629. [Google Scholar] [CrossRef]
- Yu, M.; Bardia, A.; Wittner, B.S.; Stott, S.L.; Smas, M.E.; Ting, D.T.; Isakoff, S.J.; Ciciliano, J.C.; Wells, M.N.; Shah, A.M.; et al. Circulating breast tumor cells exhibit dynamic changes in epithelial and mesenchymal composition. Science 2013, 339, 580–584. [Google Scholar] [CrossRef] [PubMed]
- Theodoropoulos, P.A.; Polioudaki, H.; Agelaki, S.; Kallergi, G.; Saridaki, Z.; Mavroudis, D.; Georgoulias, V. Circulating tumor cells with a putative stem cell phenotype in peripheral blood of patients with breast cancer. Cancer Lett. 2010, 288, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Papadaki, M.A.; Kallergi, G.; Zafeiriou, Z.; Manouras, L.; Theodoropoulos, P.A.; Mavroudis, D.; Georgoulias, V.; Agelaki, S. Co-expression of putative stemness and epithelial-to-mesenchymal transition markers on single circulating tumour cells from patients with early and metastatic breast cancer. BMC Cancer 2014, 14, 651. [Google Scholar] [CrossRef] [PubMed]
- Papadaki, M.A.; Aggouraki, D.; Vetsika, E.K.; Xenidis, N.; Kallergi, G.; Kotsakis, A.; Georgoulias, V. Epithelial-to-mesenchymal Transition Heterogeneity of Circulating Tumor Cells and Their Correlation with MDSCs and Tregs in HER2-negative Metastatic Breast Cancer Patients. Anticancer Res. 2021, 41, 661–670. [Google Scholar] [CrossRef] [PubMed]
- Kallergi, G.; Papadaki, M.A.; Politaki, E.; Mavroudis, D.; Georgoulias, V.; Agelaki, S. Epithelial to mesenchymal transition markers expressed in circulating tumour cells of early and metastatic breast cancer patients. Breast Cancer Res. 2011, 13, R59. [Google Scholar] [CrossRef] [PubMed]
- Papadaki, M.A.; Stoupis, G.; Theodoropoulos, P.A.; Mavroudis, D.; Georgoulias, V.; Agelaki, S. Circulating Tumor Cells with Stemness and Epithelial-to-Mesenchymal Transition Features Are Chemoresistant and Predictive of Poor Outcome in Metastatic Breast Cancer. Mol. Cancer Ther. 2019, 18, 437–447. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, T.; Ozawa, Y.; Kimura, T.; Sato, Y.; Kuznetsov, G.; Xu, S.; Uesugi, M.; Agoulnik, S.; Taylor, N.; Funahashi, Y.; et al. Eribulin mesilate suppresses experimental metastasis of breast cancer cells by reversing phenotype from epithelial-mesenchymal transition (EMT) to mesenchymal-epithelial transition (MET) states. Br. J. Cancer 2014, 110, 1497–1505. [Google Scholar] [CrossRef]
- Kurebayashi, J.; Kanomata, N.; Yamashita, T.; Shimo, T.; Moriya, T. Antitumor and anticancer stem cell activities of eribulin mesylate and antiestrogens in breast cancer cells. Breast Cancer 2016, 23, 425–436. [Google Scholar] [CrossRef] [PubMed]
- Cortes, J.; O’Shaughnessy, J.; Loesch, D.; Blum, J.L.; Vahdat, L.T.; Petrakova, K.; Chollet, P.; Manikas, A.; Dieras, V.; Delozier, T.; et al. Eribulin monotherapy versus treatment of physician’s choice in patients with metastatic breast cancer (EMBRACE): A phase 3 open-label randomised study. Lancet 2011, 377, 914–923. [Google Scholar] [CrossRef]
- Kaufman, P.A.; Awada, A.; Twelves, C.; Yelle, L.; Perez, E.A.; Velikova, G.; Olivo, M.S.; He, Y.; Dutcus, C.E.; Cortes, J. Phase III open-label randomized study of eribulin mesylate versus capecitabine in patients with locally advanced or metastatic breast cancer previously treated with an anthracycline and a taxane. J. Clin. Oncol. 2015, 33, 594–601. [Google Scholar] [CrossRef]
- Twelves, C.; Cortes, J.; Vahdat, L.; Olivo, M.; He, Y.; Kaufman, P.A.; Awada, A. Efficacy of eribulin in women with metastatic breast cancer: A pooled analysis of two phase 3 studies. Breast Cancer Res. Treat. 2014, 148, 553–561. [Google Scholar] [CrossRef] [PubMed]
- Aogi, K.; Watanabe, K.; Kitada, M.; Sangai, T.; Ohtani, S.; Aruga, T.; Kawagichi, H.; Fujisawa, T.; Maeda, S.; Morimoto, T.; et al. Clinical usefulness of eribulin as first- or second-line chemotherapy for recurrent HER2-negative breast cancer: A randomized phase II study (JBCRG-19). Int. J. Clin. Oncol. 2021, 26, 1229–1236. [Google Scholar] [CrossRef] [PubMed]
- Gris-Oliver, A.; Ibrahim, Y.H.; Rivas, M.A.; Garcia-Garcia, C.; Sanchez-Guixe, M.; Ruiz-Pace, F.; Viaplana, C.; Perez-Garcia, J.M.; Llombart-Cussac, A.; Grueso, J.; et al. PI3K activation promotes resistance to eribulin in HER2-negative breast cancer. Br. J. Cancer 2021, 124, 1581–1591. [Google Scholar] [CrossRef] [PubMed]
- Teng, X.; Hayashida, T.; Murata, T.; Nagayama, A.; Seki, T.; Takahashi, M.; Kitagawa, Y. A transposon screen identifies enhancement of NF-kappaB pathway as a mechanism of resistance to eribulin. Breast Cancer 2021, 28, 884–895. [Google Scholar] [CrossRef]
- Papadaki, M.A.; Koutsopoulos, A.V.; Tsoulfas, P.G.; Lagoudaki, E.; Aggouraki, D.; Monastirioti, A.; Koutoulaki, C.; Apostolopoulou, C.A.; Merodoulaki, A.C.; Papadaki, C.; et al. Clinical Relevance of Immune Checkpoints on Circulating Tumor Cells in Breast Cancer. Cancers 2020, 12, 376. [Google Scholar] [CrossRef]
- Papadaki, M.A.; Monastirioti, A.; Apostolopoulou, C.A.; Aggouraki, D.; Papadaki, C.; Michaelidou, K.; Vassilakopoulou, M.; Alexakou, K.; Mavroudis, D.; Agelaki, S. TLR4 and pSTAT3 Expression on Circulating Tumor Cells (CTCs) and Immune Cells in the Peripheral Blood of Breast Cancer Patients: Prognostic Implications. Cancers 2022, 14, 1053. [Google Scholar] [CrossRef]
- Papadaki, M.A.; Sotiriou, A.I.; Vasilopoulou, C.; Filika, M.; Aggouraki, D.; Tsoulfas, P.G.; Apostolopoulou, C.A.; Rounis, K.; Mavroudis, D.; Agelaki, S. Optimization of the Enrichment of Circulating Tumor Cells for Downstream Phenotypic Analysis in Patients with Non-Small Cell Lung Cancer Treated with Anti-PD-1 Immunotherapy. Cancers 2020, 12, 1556. [Google Scholar] [CrossRef]
- Kashiwagi, S.; Asano, Y.; Goto, W.; Takada, K.; Takahashi, K.; Hatano, T.; Tanaka, S.; Takashima, T.; Tomita, S.; Motomura, H.; et al. Mesenchymal-epithelial Transition and Tumor Vascular Remodeling in Eribulin Chemotherapy for Breast Cancer. Anticancer Res. 2018, 38, 401–410. [Google Scholar] [CrossRef]
- Horimoto, Y.; Tokuda, E.; Murakami, F.; Uomori, T.; Himuro, T.; Nakai, K.; Orihata, G.; Iijima, K.; Togo, S.; Shimizu, H.; et al. Analysis of circulating tumour cell and the epithelial mesenchymal transition (EMT) status during eribulin-based treatment in 22 patients with metastatic breast cancer: A pilot study. J. Transl. Med. 2018, 16, 287. [Google Scholar] [CrossRef]
- Ito, M.; Horimoto, Y.; Tokuda, E.; Murakami, F.; Uomori, T.; Himuro, T.; Nakai, K.; Orihata, G.; Iijima, K.; Saito, M. Impact of circulating tumour cells on survival of eribulin-treated patients with metastatic breast cancer. Med. Oncol. 2019, 36, 89. [Google Scholar] [CrossRef]
- Polioudaki, H.; Mala, A.; Gkimprixi, E.; Papadaki, M.A.; Chantziou, A.; Tzardi, M.; Mavroudis, D.; Agelaki, S.; Theodoropoulos, P.A. Epithelial/Mesenchymal Characteristics and PD-L1 Co-Expression in CTCs of Metastatic Breast Cancer Patients Treated with Eribulin: Correlation with Clinical Outcome. Cancers 2020, 12, 3735. [Google Scholar] [CrossRef]
- Rajput, S.; Guo, Z.; Li, S.; Ma, C.X. PI3K inhibition enhances the anti-tumor effect of eribulin in triple negative breast cancer. Oncotarget 2019, 10, 3667–3680. [Google Scholar] [CrossRef]
- Polyak, K.; Weinberg, R.A. Transitions between epithelial and mesenchymal states: Acquisition of malignant and stem cell traits. Nat. Rev. Cancer 2009, 9, 265–273. [Google Scholar] [CrossRef]
- Papadaki, M.A.; Messaritakis, I.; Fiste, O.; Souglakos, J.; Politaki, E.; Kotsakis, A.; Georgoulias, V.; Mavroudis, D.; Agelaki, S. Assessment of the Efficacy and Clinical Utility of Different Circulating Tumor Cell (CTC) Detection Assays in Patients with Chemotherapy-Naive Advanced or Metastatic Non-Small Cell Lung Cancer (NSCLC). Int. J. Mol. Sci. 2021, 22, 925. [Google Scholar] [CrossRef]
- Shishido, S.N.; Carlsson, A.; Nieva, J.; Bethel, K.; Hicks, J.B.; Bazhenova, L.; Kuhn, P. Circulating tumor cells as a response monitor in stage IV non-small cell lung cancer. J. Transl. Med. 2019, 17, 294. [Google Scholar] [CrossRef]
- Kiniwa, Y.; Nakamura, K.; Mikoshiba, A.; Ashida, A.; Akiyama, Y.; Morimoto, A.; Okuyama, R. Usefulness of monitoring circulating tumor cells as a therapeutic biomarker in melanoma with BRAF mutation. BMC Cancer 2021, 21, 287. [Google Scholar] [CrossRef]
- Cabel, L.; Berger, F.; Cottu, P.; Loirat, D.; Rampanou, A.; Brain, E.; Cyrille, S.; Bourgeois, H.; Kiavue, N.; Deluche, E.; et al. Clinical utility of circulating tumour cell-based monitoring of late-line chemotherapy for metastatic breast cancer: The randomised CirCe01 trial. Br. J. Cancer 2021, 124, 1207–1213. [Google Scholar] [CrossRef]
- Agelaki, S.; Kalykaki, A.; Markomanolaki, H.; Papadaki, M.A.; Kallergi, G.; Hatzidaki, D.; Kalbakis, K.; Mavroudis, D.; Georgoulias, V. Efficacy of Lapatinib in Therapy-Resistant HER2-Positive Circulating Tumor Cells in Metastatic Breast Cancer. PLoS ONE 2015, 10, e0123683. [Google Scholar] [CrossRef]
- Meng, S.; Tripathy, D.; Frenkel, E.P.; Shete, S.; Naftalis, E.Z.; Huth, J.F.; Beitsch, P.D.; Leitch, M.; Hoover, S.; Euhus, D.; et al. Circulating tumor cells in patients with breast cancer dormancy. Clin. Cancer Res. 2004, 10, 8152–8162. [Google Scholar] [CrossRef]
- Kallergi, G.; Mavroudis, D.; Georgoulias, V.; Stournaras, C. Phosphorylation of FAK, PI-3K, and impaired actin organization in CK-positive micrometastatic breast cancer cells. Mol. Med. 2007, 13, 79–88. [Google Scholar] [CrossRef]
- Spiliotaki, M.; Mavroudis, D.; Kokotsaki, M.; Vetsika, E.K.; Stoupis, I.; Matikas, A.; Kallergi, G.; Georgoulias, V.; Agelaki, S. Expression of insulin-like growth factor-1 receptor in circulating tumor cells of patients with breast cancer is associated with patient outcomes. Mol. Oncol. 2018, 12, 21–32. [Google Scholar] [CrossRef]
- Kallergi, G.; Konstantinidis, G.; Markomanolaki, H.; Papadaki, M.A.; Mavroudis, D.; Stournaras, C.; Georgoulias, V.; Agelaki, S. Apoptotic circulating tumor cells in early and metastatic breast cancer patients. Mol. Cancer Ther. 2013, 12, 1886–1895. [Google Scholar] [CrossRef]
- Kallergi, G.; Markomanolaki, H.; Giannoukaraki, V.; Papadaki, M.A.; Strati, A.; Lianidou, E.S.; Georgoulias, V.; Mavroudis, D.; Agelaki, S. Hypoxia-inducible factor-1alpha and vascular endothelial growth factor expression in circulating tumor cells of breast cancer patients. Breast Cancer Res. 2009, 11, R84. [Google Scholar] [CrossRef]
- Tolaney, S.M.; Barroso-Sousa, R.; Keenan, T.; Li, T.; Trippa, L.; Vaz-Luis, I.; Wulf, G.; Spring, L.; Sinclair, N.F.; Andrews, C.; et al. Effect of Eribulin With or Without Pembrolizumab on Progression-Free Survival for Patients With Hormone Receptor-Positive, ERBB2-Negative Metastatic Breast Cancer: A Randomized Clinical Trial. JAMA Oncol. 2020, 6, 1598–1605. [Google Scholar] [CrossRef]
- Keenan, T.E.; Guerriero, J.L.; Barroso-Sousa, R.; Li, T.; O’Meara, T.; Giobbie-Hurder, A.; Tayob, N.; Hu, J.; Severgnini, M.; Agudo, J.; et al. Molecular correlates of response to eribulin and pembrolizumab in hormone receptor-positive metastatic breast cancer. Nat. Commun. 2021, 12, 5563. [Google Scholar] [CrossRef]
- Tolaney, S.M.; Kalinsky, K.; Kaklamani, V.G.; D’Adamo, D.R.; Aktan, G.; Tsai, M.L.; O’Regan, R.M.; Kaufman, P.A.; Wilks, S.T.; Andreopoulou, E.; et al. Eribulin Plus Pembrolizumab in Patients with Metastatic Triple-Negative Breast Cancer (ENHANCE 1): A Phase Ib/II Study. Clin. Cancer Res. 2021, 27, 3061–3068. [Google Scholar] [CrossRef]
- Pascual, T.; Oliveira, M.; Villagrasa, P.; Ortega, V.; Pare, L.; Bermejo, B.; Morales, S.; Amillano, K.; Lopez, R.; Galvan, P.; et al. Neoadjuvant eribulin in HER2-negative early-stage breast cancer (SOLTI-1007-NeoEribulin): A multicenter, two-cohort, non-randomized phase II trial. NPJ Breast Cancer 2021, 7, 145. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Patients (n = 42) | n (%) |
|---|---|
| Age (years), median (range) | 61 (34–78) |
| Performance Status (PS) | |
| 0–1 | 35 (83.3) |
| 2 | 7 (16.7) |
| Histology | |
| Ductal | 33 (78.6) |
| Lobular | 5 (11.9) |
| Mixed | 2 (4.8) |
| Other | 2 (4.8) |
| Stage at diagnosis | |
| I–III | 33 (78.6) |
| IV | 9 (21.4) |
| Subtype | |
| HR+/HER2− | 22 (52.4) |
| Triple-negative | 13 (31) |
| HER2+ | 7 (16.7) |
| Prior chemotherapy for metastatic disease a | |
| Taxane-based | 18 (42.9) |
| Anthracycline-based | 1 (2.4) |
| Taxane/Anthracycline -based | 16 (38.1) |
| Other | 4 (9.5) |
| None | 3 (7.1) |
| Organs affected | |
| Bones | 27 (64.3) |
| Liver | 25 (59.5) |
| Lung | 20 (47.6) |
| Brain | 6 (14.3) |
| Lymph nodes | 15 (35.7) |
| Skin | 7 (16.7) |
| Line of Eribulin treatment | |
| 1–2 | 13 (31) |
| >2 | 29 (69) |
| Response to eribulin treatment at first evaluation | |
| Partial response | 4 (9.5) |
| Stable disease | 11 (26.2) |
| Progressive disease | 20 (47.6) |
| Non-evaluable | 7 (16.7) |
| Disease status at the end of treatment | |
| Partial response | 1 (2.4) |
| Stable disease | 10 (23.8) |
| Progressive disease | 24 (57.1) |
| Non-evaluable | 7 (16.7) |
| CTC Assessment | |||
|---|---|---|---|
| Patients | Baseline | C1D8 | PD |
| CTC-positive/total patients | 14/42 | 6/22 | 6/26 |
| Patient positivity | 33.3% | 27.3% | 23.1% |
| CTC counts | |||
| Sum (range) | 88 (1–18) | 12 (1–4) | 24 (1–9) |
| Mean no of CTCs | 6.29 | 2.00 | 4.00 |
| Progression-Free Survival (PFS). | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| Covariates | HR (95% CI) | p Value | HR (95% CI) | p Value |
| Age (below vs. above average, 60 years) | 1.738 (0.906–3.331) | 0.096 | ||
| Performance status (2 vs. 0–1) | 2.080 (0.889–4.865) | 0.091 | ||
| Stage at diagnosis (IV vs. I–III) | 1.563 (0.716–3.411) | 0.262 | ||
| Tumor subtype | ||||
| Hormone receptor+/HER2− | reference | reference | ||
| HER2+ | 1.894 (0.778–4.614) | 0.159 | 1.894 (0.778–4.614) | 0.159 |
| Triple-negative | 2.538 (1.086–5.936) | 0.032 * | 2.538 (1.086–5.936) | 0.032 * |
| Metastatic sites (yes vs. no) | ||||
| Brain | 2.570 (1.032–6.399) | 0.043 * | 2.868 (1.132–7.264) | 0.026 * |
| Liver | 1.394 (0.741–2.626) | 0.483 | ||
| Lung | 1.008 (0.544–1.870) | 0.651 | ||
| Bones | 1.153 (0.589–2.257) | 0.679 | ||
| Lymph nodes | 0.786 (0.403–1.536) | 0.482 | ||
| Skin | 1.059 (0.463–2.422) | 0.891 | ||
| Line of eribulin treatment (>2 vs. 1–2) | 0.902 (0.465–1.748) | 0.759 | ||
| CTC assessmenta | ||||
| All CTC detection at baseline (yes vs. no) | 2.565 (1.254–5.248) | 0.010 * | 2.034 (0.927–4.461) | 0.076 |
| CSC+/partial-EMT+ CTCs at baseline (yes vs. no) | 2.297 (1.118–4.722) | 0.024 * | 1.784 (0.812–3.921) | 0.150 |
| Overall Survival (OS) | Univariate Analysis | Multivariate Analysis | ||
| Covariates | HR (95% CI) | p value | HR (95% CI) | p value |
| Age (below vs. above average, 60 years) | 1.116 (0.567–2.198) | 0.750 | ||
| Performance status (2 vs. 0–1) | 2.540 (1.019–6.332) | 0.045 * | ||
| Stage at diagnosis (IV vs. I–III) | 0.608 (0.233–1.587) | 0.309 | ||
| Tumor Subtype | ||||
| Hormone receptor+/HER2− | reference | |||
| HER2+ | 0.671 (0.223–2.020) | 0.478 | ||
| Triple-negative | 1.729 (0.831–3.598) | 0.143 | ||
| Metastatic sites (yes vs. no) | ||||
| Brain | 5.854 (2.096–16.354) | 0.001 * | 11.100 (3.550–34.711) | 0.000 * |
| Liver | 1.124 (0.543–2.327) | 0.754 | ||
| Lung | 0.909 (0.463–1.786) | 0.783 | ||
| Bones | 1.735 (0.836–3.603) | 0.139 | ||
| Lymph nodes | 0.752 (0.368–1.539) | 0.436 | ||
| Skin | 4.339 (1.716–10.969) | 0.002 * | 8.331 (2.888–24.030) | 0.000 * |
| Line of eribulin treatment (>2 vs. 1–2) | 4.116 (0.493–34.392) | 0.191 | ||
| CTC assessmenta | ||||
| All CTC detection at baseline (yes vs. no) | 2.727 (1.315–5.656) | 0.007 * | 3.779 (1.737–8.222) | 0.001 * |
| CSC+/partial-EMT+ CTCs at baseline (yes vs. no) | 2.467 (1.187–5.128) | 0.016 * | 3.714 (1.684–8.191) | 0.001 * |
| Progression-Free Survival (PFS) | Univariate Analysis | |||
|---|---|---|---|---|
| Covariates | HR (95% CI) | p Value | ||
| Age (below vs. above average, 60 years) | 1.818 (0.735–4.496) | 0.196 | ||
| Performance status (2 vs. 0–1) | 1.819 (0.503–6.579) | 0.362 | ||
| Stage at diagnosis (IV vs. I–III) | 1.832 (0.623–5.391) | 0.272 | ||
| Tumor subtype | ||||
| Hormone receptor+/HER2− | reference | |||
| HER2+ | 1.142 (0.311–4.186) | 0.842 | ||
| Triple-negative | 2.613 (0.909–7.516) | 0.075 | ||
| Metastatic sites (yes vs. no) | ||||
| Brain | 2.418 (0.751–7.787) | 0.139 | ||
| Liver | 1.045 (0.430–2.539) | 0.923 | ||
| Lung | 1.064 (0.450–2.515) | 0.888 | ||
| Bones | 1.265 (0.502–3.189) | 0.618 | ||
| Lymph nodes | 0.793 (0.326–1.929) | 0.609 | ||
| Skin | 1.155 (0.413–3.235) | 0.783 | ||
| Line of eribulin treatment (>2 vs. 1–2) | 1.463 (0.487–4.399) | 0.498 | ||
| CTC assessment | ||||
| CTC detection at baseline (yes vs. no) | 4.460 (1.422–13.987) | 0.010 * | ||
| CTC detection at baseline and C1D8 | ||||
| Negative | reference | |||
| Positive in one time point | 2.731 (0.995–7.498) | 0.051 | ||
| Positive in both time points | 9.545 (1.556–58.189) | 0.014 * | ||
| Overall Survival (OS) | Univariate Analysis | Multivariate Analysis | ||
| Covariates | HR (95% CI) | p value | HR (95% CI) | p value |
| Age (below vs. above average, 60 years) | 3.173 (1.045–9.637) | 0.042 * | ||
| Performance status (2 vs. 0–1) | 1.038 (0.233–4.626) | 0.961 | ||
| Stage at diagnosis (IV vs. I–III) | 0.963 (0.268–3.465) | 0.954 | ||
| Tumor subtype | ||||
| Hormone receptor+/HER2− | reference | |||
| HER2+ | 0.345 (0.042–2.838) | 0.163 | ||
| Triple-negative | 1.729 (0.831–3.598) | 0.092 | ||
| Metastatic sites (yes vs. no) | ||||
| Brain | 3.787 (1.058–13.557) | 0.041 * | 3.888 (1.050–14.399) | 0.042 * |
| Liver | 2.074 (0.742–5.802) | 0.164 | ||
| Lung | 0.897 (0.318–2.530) | 0.838 | ||
| Bones | 3.237 (0.998–10.502) | 0.050 | ||
| Lymph nodes | 0.990 (0.357–2.748) | 0.985 | ||
| Skin | 2.893 (0.934–8.955) | 0.065 | ||
| Line of eribulin treatment (>2 vs. 1–2) | 1.023 (0.324–3.226) | 0.969 | ||
| CTC assessmenta | ||||
| CTC detection at baseline (yes vs. no) | 5.109 (1.716–15.210) | 0.003 * | 5.222 (1.723–15.828) | 0.003 * |
| CTC detection at baseline and C1D8 | ||||
| Negative | reference | reference | ||
| Positive in one time point | 2.805 (0.888–8.859) | 0.079 | 2.675 (0.840–8.518) | 0.096 |
| Positive in both time points | 7.579 (1.207–47.603) | 0.031 * | 4.355 (0.595–31.880) | 0.147 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Papadaki, M.A.; Mala, A.; Merodoulaki, A.C.; Vassilakopoulou, M.; Mavroudis, D.; Agelaki, S. Investigating the Role of CTCs with Stem/EMT-like Features in Metastatic Breast Cancer Patients Treated with Eribulin Mesylate. Cancers 2022, 14, 3903. https://doi.org/10.3390/cancers14163903
Papadaki MA, Mala A, Merodoulaki AC, Vassilakopoulou M, Mavroudis D, Agelaki S. Investigating the Role of CTCs with Stem/EMT-like Features in Metastatic Breast Cancer Patients Treated with Eribulin Mesylate. Cancers. 2022; 14(16):3903. https://doi.org/10.3390/cancers14163903
Chicago/Turabian StylePapadaki, Maria A., Anastasia Mala, Aikaterini C. Merodoulaki, Maria Vassilakopoulou, Dimitrios Mavroudis, and Sofia Agelaki. 2022. "Investigating the Role of CTCs with Stem/EMT-like Features in Metastatic Breast Cancer Patients Treated with Eribulin Mesylate" Cancers 14, no. 16: 3903. https://doi.org/10.3390/cancers14163903
APA StylePapadaki, M. A., Mala, A., Merodoulaki, A. C., Vassilakopoulou, M., Mavroudis, D., & Agelaki, S. (2022). Investigating the Role of CTCs with Stem/EMT-like Features in Metastatic Breast Cancer Patients Treated with Eribulin Mesylate. Cancers, 14(16), 3903. https://doi.org/10.3390/cancers14163903